
Abstract
Objective
To develop risk prediction models for preterm birth among infants with orofacial clefts.
Design
Data from the Texas Birth Defects Registry for infants with orofacial clefts born between 1999-2014 were used to develop preterm birth predictive models. Logistic regression was used to consider maternal and infant characteristics, and internal validation of the final model was performed using bootstrapping methods. The area under the curve (AUC) statistic was generated to assess model performance, and separate predictive models were built and validated for infants with cleft lip and cleft palate alone. Several secondary analyses were conducted among subgroups of interest.
Setting
State-wide, population-based Registry data.
Patients/Participants
6774 infants with orofacial clefts born in Texas between 1999-2014.
Main Outcome Measure(s)
Preterm birth among infants with orofacial clefts.
Results
The final predictive model performed modestly, with an optimism-corrected AUC of 0.67 among all infants with orofacial clefts. The optimism-corrected models for cleft lip (with or without cleft palate) and cleft palate alone had similar predictive capability, with AUCs of 0.66 and 0.67, respectively. Secondary analyses had similar results, but the model among infants with delivery prior to 32 weeks demonstrated higher optimism-corrected predictive capability (AUC = 0.74).
Conclusions
This study provides a first step towards predicting preterm birth risk among infants with orofacial clefts. Identifying pregnancies affected by orofacial clefts at the highest risk for preterm birth may lead to new avenues for improving outcomes among these infants.
Introduction
Cleft lip and/or palate are common orofacial malformations, collectively occurring in ∼1-2 per 1000 live births globally. 1 Infants with orofacial clefts often undergo surgical correction, usually involving multiple procedures, and can experience long-term medical consequences including abnormal or delayed speech, difficulty with feeding, dental abnormalities, and hearing loss.2–4 Orofacial clefts are also associated with increased infant mortality, 5 and long-term psychological effects are common for both affected individuals and their families. 6
Preterm birth, delivery prior to 37 weeks gestation, 7 occurs 2-3 times more frequently than among infants with orofacial clefts than in the general population.8,9 Because infants with clefts are more medically vulnerable than infants without orofacial clefts the consequences of preterm birth may be even more substantial among this group. 10 For example, one study reported that the majority of infants with isolated orofacial clefts who died during the first year of follow-up after birth had a prematurity-related cause of death. 11 However, there is currently a dearth of knowledge of the etiology of preterm birth among infants with orofacial clefts.
Preterm birth risk prediction models are used in the general population for the purpose of identifying infants at high risk for preterm birth.12,13 Potential benefits of screening tools include prenatal preterm birth risk stratification (eg, high risk vs. low risk) and the opportunity for improved delivery planning and coordination of care. For example, affected pregnancies identified as being at the highest risk for preterm birth may be candidates for prophylactic prenatal interventions such as routine cervical length assessment, therapies for threatened preterm labor or lung maturation, cervical cerclage, bed rest, or relocation near appropriate delivery facilities.14,15 Given the higher prevalence of preterm birth among infants with orofacial clefts and the additional medical complications they face, predictive models of preterm birth may be impactful tool for improving outcomes for infants with prenatally diagnosed clefts. Thus, in this analysis, we aimed to develop a predictive model of preterm birth for infants with orofacial clefts.
Methods
Study Subjects
Cases were identified by the Texas Birth Defect Registry (TBDR) among 1999-2014 deliveries (ie, the currently available dataset at the time the analyses were initiated). The TBDR is a state-wide, population-based surveillance program run by the Texas Department of State Health Services Birth Defects Epidemiology and Surveillance Branch. Active surveillance for birth defects is conducted through review of medical records at relevant healthcare facilities across the state by TBDR staff. Cases must have a monitored structural birth defect or chromosomal anomaly diagnosed within the first 12 months following birth to be included. Registry staff identify and document all defects present in cases using a six-digit Centers for Disease Control (CDC) modified British Pediatric Association (BPA) designation code.
Infants with an orofacial cleft and no documented syndromic diagnosis were eligible for inclusion in our main analyses. This included cleft palate alone (CP) (BPA codes 749.000-749.090) and cleft lip with or without cleft palate (CLP) (BPA codes 749.100-749.220). We limited all analyses to singleton live born infants and excluded rare cases with co-occurring anencephaly, given the extremely high prevalence of preterm birth among infants with this defect. 8 Cases with a gestational age of <24 weeks were excluded due to expected difficulty in accurately classifying orofacial clefts prior to 24 weeks. 8
Relevant maternal and infant demographic data were provided by the TBDR through a combination of medical record data and routinely linked vital record data from the Center for Health Statistics at the Texas Department of State Health Services. Gestational age at birth for each infant was abstracted from vital record data. Approval for the study protocol was given by the Institutional Review Boards of UTHealth at Houston and the Texas Department of State Health Services. The requirement to obtain informed consent was waived for this project.
Statistical Methods
We used logistic regression to develop a predictive model of preterm birth. We first analyzed the aggregate group of infants with any cleft (CP or CLP) and then analyzed each of these two cleft groups separately. Thus, three separate models were developed, allowing for potential differences in predictors of preterm birth between the three groups. Potential predictors with data available from 1999-2014 included infant sex, presence of an additional major birth defect, maternal age, race/ethnicity, education, diabetes (inclusive of both gestational and pre-gestational diabetes), hypertension (inclusive of gestational and pre-gestational hypertension), tobacco smoking status, marital status, any prenatal care during the first trimester of pregnancy, short interpregnancy interval (<6 months), previous livebirth, designation of residence as urban or rural as defined by maternal county of residence at delivery based on the US Department of Agriculture Rural–Urban Continuum Codes (RUCC), 16 and residence in a county along the Texas-Mexico border. Variables with data available from 2005-2014 only included maternal pre-pregnancy body mass index (BMI), previous cesarean section, previous preterm birth, insurance payment type, and Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) enrollment, which provides resources for low-income pregnant women. The distributions of all potential predictors were tabulated for each phenotypic group. We used all eligible infants (eg, all with CP for the CP model) to create each initial predictive model and then implemented a bootstrapping technique 17 that has been used among preterm birth predictive models in the general population for model assessment and validation purposes 13 (described below).
To build each model, we conducted univariate unconditional logistic regression to determine the crude association between each potential predictor and preterm birth. All potential predictors with at least one category that was associated with preterm birth (Wald P-value < .05) were included in a preliminary multivariate model. To establish the final multivariable model, beginning with all covariates associated in univariate analyses, we iteratively removed variables in order of descending p-value until at least one category of each predictor in the multivariable model was associated with preterm birth (Wald P-value < .05). A receiver operating characteristic (ROC) curve was constructed for the final model, which we used to determine the area under the curve (AUC) and the corresponding 95% confidence interval.
The AUC serves as an indicator of the model's predictive ability in discriminating between those with preterm (<37 weeks gestation) versus full term (≥37 weeks gestation) delivery, with an AUC of 0.50 equating to a model predicting no better than chance. 18 An AUC ≥ 0.70 indicates that the model has an acceptable to excellent level of discrimination. 18 After calculating the AUC for the final model, we applied bootstrapping, as described by Lankham and Slaughter, to internally validate the model and generate an optimism-corrected AUC. 17 In essence, Lankham and Slaughter 17 proposed estimating optimism for AUC by calculating the average of the differences of the AUC of the original data model applied to each bootstrap sample and the AUC of the model fit uniquely to each bootstrap sample. The optimism corrected AUC may then be generated by subtracting this mean difference from the AUC of the original model fit to the original data. For our study, we first created 500 bootstrapped samples, randomly drawing with replacement from our original dataset. For each of the bootstrap samples, we computed two AUC's; one AUC was computed by simply applying the original model to each bootstrapped sample dataset, and a second was computed by applying the model fit from each bootstrap sample to the original data. Following this, we calculated the optimism as the average of the differences between the two AUC's computed for each bootstrap sample,17,19 which is a measure for estimating of the degree of overfitting of the model. Specifically, optimism is determined by measuring the difference between the observed or apparent discrimination ability of the model among the 500 bootstrapped samples (original model AUCs) and the actual or true discrimination ability of the model on each bootstrapped sample (AUC's from each bootstrap model applied to the original data).17,19 Finally, we calculated an optimism-corrected AUC for the final model by subtracting the optimism from the generated AUC when our model was fit to the original dataset. 17
Several secondary analyses were conducted, all of which followed the same model building and internal validation process. Main analyses were repeated after removing the small proportion of pregnancies for which no prenatal care was received. In order to estimate the impact of excluding syndromic cases, we additionally ran all of the main models among all cases (ie, those with and without syndromic diagnoses). Among all infants in the full group, we evaluated extremely to very preterm (prior to 32 weeks) infants compared to births at greater than or equal to 32 weeks gestational age. Small counts limited repetition of this secondary analysis in the separate phenotypic subgroups.
Next, we assessed whether adding predictors which only had data available beginning in 2005 improved the predictive ability of the model. Our model development process incorporated the variables only available beginning in 2005 by adding those variables associated in univariate analyses to the variables already in the three main predictive models (for the full group, CLP, and CP) and iteratively removed those that were no longer associated in the full model. All analyses were conducted using SAS software version 9.4 (SAS Institute, Cary, NC).
Results
Among liveborn, singleton births (96.8% of cases) included in the analysis, 6774 infants had a non-syndromic orofacial cleft, 1794 infants with CP and 4980 infants with CLP. Counts were tabulated for each potential predictor (Table 1). Cases were distributed in largely similar percentages within most of the variables available from 1999-2014 and 2005-2014 across the full group, infants with CLP, and infants with CP. Among all infants, maternal education, maternal race/ethnicity group, hypertension, diabetes, prenatal care, the presence of additional birth defects, maternal body mass index, previous Caesarean section, and previous preterm birth differed significantly between preterm and full term births (Table 1).
Characteristics of Mothers and Infants with Orofacial Clefts by Preterm Birth Status, Texas Birth Defects Registry 1999-2014 a .
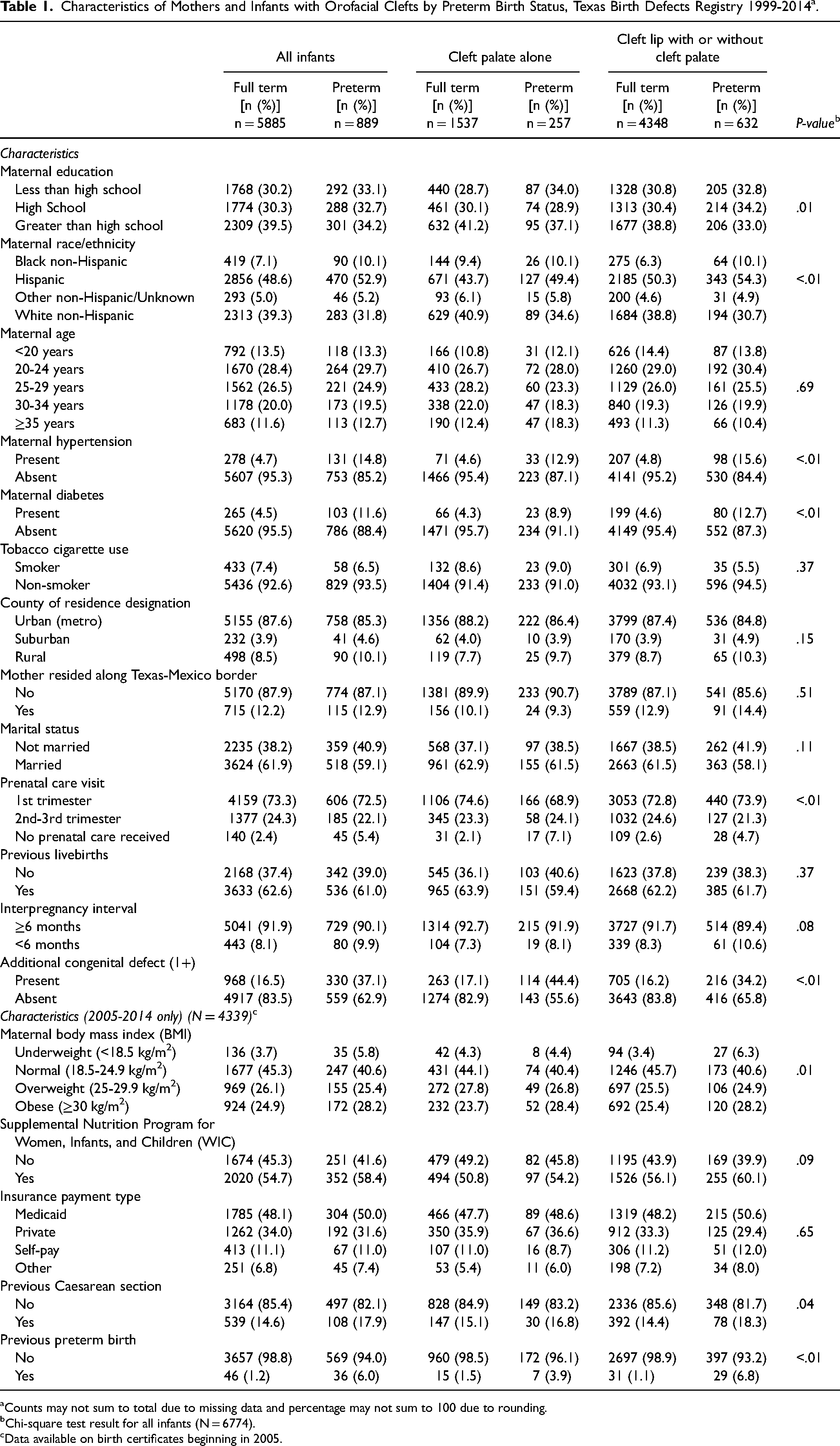
Counts may not sum to total due to missing data and percentage may not sum to 100 due to rounding.
Chi-square test result for all infants (N = 6774).
Data available on birth certificates beginning in 2005.
Adjusted odds ratio estimates are presented in Table 2 for all predictors retained in the final CLP + CP model, which included maternal education group, maternal race/ethnicity, hypertension, diabetes, and the presence of additional birth defects. The final model had an optimism-corrected AUC = 0.67 (Table 2). Table 2 also presents the final predictors in the CLP and CP models, respectively. Models differed across the two subgroups. Specifically, the CLP model included maternal race/ethnicity and diabetes, whereas maternal age group was retained in the CP model only. Both models demonstrated similar predictive ability (CLP optimism-corrected AUC = 0.66, CP optimism-corrected AUC = 0.67). Following removal of pregnancies in which no prenatal care was received (2.4%) in a secondary analysis (data not shown), results were very similar to those from the main results.
Adjusted Odds Ratios for Preterm Birth of Included Maternal and Infant Characteristics by Orofacial Phenotypic Group, 1999-2014 (N = 6774) a .
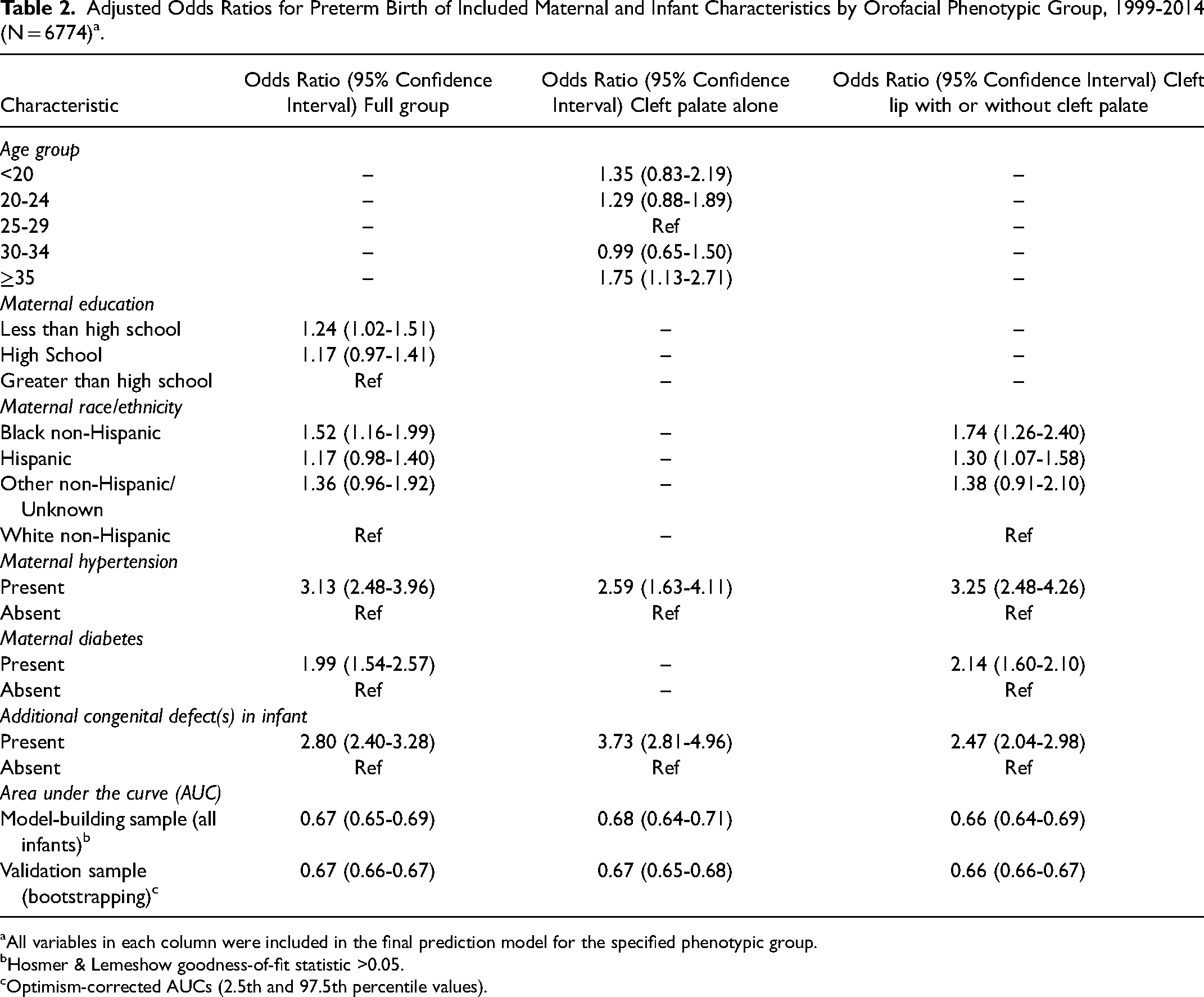
All variables in each column were included in the final prediction model for the specified phenotypic group.
Hosmer & Lemeshow goodness-of-fit statistic >0.05.
Optimism-corrected AUCs (2.5th and 97.5th percentile values).
In Table 3, we report a high optimism-corrected AUC for our secondary analysis of extremely-to-very preterm birth (<32 weeks) (AUC = 0.74). Following the addition of variables available from 2005-2014 to the predictive models (previous preterm birth and/or previous Caesarean section), optimism-corrected AUCs ranged from 0.67-0.70 across the respective models for infants with CLP + CP, infants with CLP, and infants with CP (Table 3). Adjusted odds ratio estimates for the secondary analyses are presented in supplementary tables (Supplementary Table 1-2). Results from the analyses of all cases, including cases with a syndromic diagnosis, demonstrated slightly improved, but overall similar AUC estimates compared to the main analyses (Supplementary Table 3).
Optimism-Corrected Area Under the Curve (AUC) Estimates for Secondary Analyses, by Orofacial Cleft Subgroup a .

Optimism-corrected AUCs (2.5th and 97.5th percentile values).
Counts for analytic group were not sufficient for secondary analyses.
Discussion
Our final predictive model yielded moderate discrimination for preterm birth among infants with orofacial clefts, performing comparably, if not slightly better, than models developed for predicting preterm birth using similar clinical and demographic variables in the general population (AUCs: 0.63-0.66).19,20 Most predictors in our models (eg, maternal race/ethnicity, hypertension, diabetes, prenatal care) overlap with variables included in predictive models of preterm birth among the general population, though our models included substantially fewer variables than those among the general population.19,20 However, we observed a strong association (OR 2.80, 95% CI [2.40-3.28]) among all infants between the presence of additional defects and preterm birth, which supports the notion that an orofacial clefts-specific preterm prediction model may be beneficial.
A notable result was the relatively high discrimination ability of our model specifically developed for extremely to very preterm birth infants (<32 weeks) (AUC = 0.74). This estimate falls squarely within the range that is considered to have clinical utility, which suggests that it may ultimately prove to be clinically useful. Overall, infants with lower gestational age experience poor survival and long-term outcomes (eg, cognitive)21,22 making risk stratification for extremely to very preterm birth especially relevant as a next step to appropriate intervention planning. Pending confirmation, future work might focus on understanding if fetuses with orofacial clefts predicted to be at high risk for extremely to very preterm birth may benefit from interventions.
More generally, all pregnancies diagnosed with an orofacial cleft may particularly benefit from preterm birth risk stratification tools, given the increased risk for preterm birth among affected infants and the increasing ability of prenatal diagnostics to detect these common defects.23,24 Overall, prenatal diagnoses are expected to increase for all subtypes in the future with expanded use of three-dimensional ultrasonography. 25 Our model may represent the first step in working towards a clinical risk stratification tool for predicting preterm birth risk among this vulnerable population, as discussed below.
Among all infants (n = 6774) and infants with CLP (n = 4980), maternal race/ethnicity was included in the final model. Specifically, non-Hispanic Black women had the largest magnitude of association for preterm birth (OR 1.53, 95% CI 1.16-2.00). Similar associations have been consistently reported for non-Hispanic Black women among prediction models for preterm birth in the general U.S. population.26,27 Multiple hypotheses have been proposed to explain how and why the association persists in the general population even when controlling for other factors. 28 For example, the March of Dimes examined 33 leading theories for the preterm birth disparity among Black women in the U.S. and found the most plausible reasons to include environmental hazards, epigenetic factors, chronic stress, hypertensive disorders, disadvantage of a lower-resource neighborhood, and the overall effects of chronic racism and health-related racism. 28 Our results suggest that increased risk of preterm birth is likely present among offspring of Black women with orofacial clefts as well.
Hypertensive disorders during pregnancy are a major predictor of preterm birth among the general population12,26,27,29 and hypertension was also a predictor of preterm birth in all of our models among infants with orofacial clefts. Although the exact mechanism leading to increased risk for preterm birth in the general population due to a pre-gestational or gestational hypertensive disorder is still unclear, disruptions from maternal inflammation or oxidative stress are likely involved. 30 Past work has described the negative effects of hypertension-related oxidative stress on pregnancy outcomes, including preterm birth. 31 Briefly, hypertensive disorders specific to pregnancy (ie, preeclampsia and gestational hypertension) have been linked with increased levels of oxidative stress which can subsequently resulting in decreased blood flow to the placenta (placental insufficiency) 32 a leading cause of preterm labor. 33 Additionally, poorly controlled hypertension and/or maternal or fetal complications due to hypertensive disorders during pregnancy can be an indication for preterm delivery. 34 Our results may suggest that mechanisms and procedures related to hypertensive disorders during pregnancy may play a role in preterm birth among infants with orofacial clefts. Screening tools for preterm birth, such as future iterations of the predictive model developed here, may lead to new opportunities to consider appropriate preterm birth prevention therapies. An example of this in action could be prevention of early onset of labor in some women with pregnancies identified as high-risk for preterm birth. 35 Further, some women predicted to have a high risk for extremely to very preterm birth specifically and who do not reside near a delivery center with appropriate critical care capacity may consider relocating nearer to an appropriate delivery facility earlier in pregnancy. Thus, confirmation and refinement of preterm birth predictive models among infants with orofacial cleft may one day help to facilitate improved clinical care. It is expected that this would ultimately translate to improved outcomes for these infants, though the effectiveness of preterm birth interventions among these infants is not well-understood. In the general population, even modest increases in gestational age have been associated with improved outcomes,22,36 and it seems likely that infants with orofacial clefts might experience similar benefits.
In our analyses, a key strength was the use of a large, diverse, population-based sample available through the TBDR. This large sample size allowed for sufficient numbers to examine several sub-groups and to specifically assess extremely to very preterm birth. Additionally, we focused on potential predictors that are typically available in birth defect registries, which may allow for comparable analyses from other states.
Limitations of the analysis include the inability to reliably distinguish between spontaneous and indicated preterm births as several of the key variables that could be used to classify preterm birth subtypes using a birth certificate-based algorithm 37 are under-reported on birth certificates (eg, <50% of PROM recorded)38,39 and these methods have not been validated among infants with birth defects. Information on certain predictors sometimes included in predictive models of preterm birth among the general population, such as variables ascertained in a clinical setting (eg, cervical measurements or maternal biomarkers) were also unavailable.40,41 However, our focus on readily available variables may have advantages (eg, implementation without the need to collect data that cannot be self-reported relatively early in pregnancy). It is also possible that diabetes and/or hypertension may have been underreported in our dataset, 42 which could potentially affect (likely reduce) the observed discriminatory ability of our model, though the specificities of these variables are high on vital records. 39 Future work using more sensitive approximations of diabetic and hypertensive status for patients would therefore likely improve upon the AUCs and predictive ability of the models developed here.
Variables in our final models (ie, hypertension and maternal race/ethnicity group) are well known contributors to the risk of preterm birth in the general population, as described above. Next step approaches may include formal comparison of analogous models between infants with versus without orofacial clefts. Additionally, risk prediction stands to improve substantially if other clinically relevant variables to preterm birth were taken into account in future work. For example, data collection like that performed by the National Birth Defect Prevention Study ascertains more detailed information on maternal exposures relevant to preterm birth such as maternal opioid use, dietary exposures (eg, nitrates), or environmental stressors during pregnancy.43–45
Finally, our work used traditional logistic regression approaches to create the reported models focused on main effect terms. Future work may benefit from methods that further account for complex interaction, such as traditional or machine-learning developed models, which are likely to provide more accurate predictions for a preterm birth. Alternative approaches include refined bootstrapping approaches, forest-based methods, or neural network-based methods, which have been used successfully to generate preterm birth prediction models in general population. 46
Despite these limitations, the discrimination ability of our models approaches or goes beyond minimal acceptable discrimination for clinical utility.
Conclusions
Our final predictive models, developed among infants with orofacial clefts, approached or achieved standard “clinical usefulness” thresholds. These results suggest that predictive models of preterm birth among infants with orofacial clefts have the potential to offer comparable clinical utility to analogous models developed among the general population. Future studies could lead to enhancement of the predictive ability of our models by incorporating additional maternal clinical variables or by utilizing a larger nationwide population dataset. By improving the risk discrimination of a model tailored to infants with orofacial clefts, we can aid in identifying higher-risk pregnancies within an already vulnerable population and identify targeted measures for improving outcomes in those susceptible to preterm birth.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231198945 - Supplemental material for Prediction of Preterm Birth among Infants with Orofacial Cleft Defects
Supplemental material, sj-docx-1-cpc-10.1177_10556656231198945 for Prediction of Preterm Birth among Infants with Orofacial Cleft Defects by Katherine L. Ludorf, Renata H. Benjamin, Mark A. Canfield, Michael D. Swartz and A. J. Agopian in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
The authors thank Matthew Rysavy, MD, PhD, from McGovern Medical School at the University of Texas Health Science Center at Houston for his review and feedback of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The protocol for this project was approved by Institutional Review Boards of the Texas Department of State Health Services and UTHealth.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (1R01HD093660-01A1) and in part by Title V Maternal and Child Health Block Grant with the Texas Department of State Health Services. The project sponsors had no active involvement in the project.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.