
Abstract
Cases of severe bilateral Tessier 4 cleft with unilateral Tessier 3 cleft and additional involvement of the amniotic band syndrome are rarer. This case reports a very rare case of ABS with severe facial cleft. Postoperative progress was satisfactory and the patient achieved functional recovery. The patient underwent several miner reconstructive surgeries and appropriate surgical treatment is necessary to restore the patient's social life.
Introduction
Congenital anomalies in the cranio-maxillofacial region and cleft lip with or without palate (CL ± P) are widely known, with a reported incidence of approximately 9.92 per 10 000 live births. 1 However, clefts of the craniofacial region other than the CL ± P are extremely rare, with Kawamoto et al. reporting a rate of 1.43 per 100 000 live births. 2 Tessier's classification of facial clefts, excluding CL ± P, was published in 1976 and is now widely accepted. 3 In particular, the Tessier 4 cleft extends from the lips to the orbit and forms a complete cleft palate. Ocular abnormalities may also be present, and blindness may occur because of the inability to close the eyelids. The cause of such facial clefts is failure of fusion of the facial processes during the embryonic period, and the cleft type can be classified according to Tessier's classification, which indicates the site of fusion of the processes. Therefore, surgical procedures can be planned according to each cleft type.
Conversely, in amniotic band syndrome (ABS), the amnion of the placenta forms excessive cord-like material due to mechanical damage or other causes, which entangles the fetus and causes morphological abnormalities in all parts of the body, including the trunk, limb, and face. ABS can cause various abnormalities ranging from minor scarring to severe tissue deformities. Its incidence varies from 1 in 1200 to 1 in 15 000 live births. 4 They cause complex morphological abnormalities when occurring on the face.
Severe morphological abnormalities occur when the amniotic band is involved, making treatment even more difficult. However, these rare facial clefts are difficult to treat because no clearly defined treatment guidelines exist.
We present a case of amniotic band syndrome with a Tessier 3, 4 in which functional and aesthetic recovery was achieved.
Case
Family members of patients in this case were informed about the purpose, methods, expected benefits, questions to be asked, and confidentiality of data. The importance of publishing facial photographs was explained to the patient's family and consent was obtained.
A 2-year-old Indonesian female was referred to Dental Hospital, University of Padjadjaran, Bandung, Indonesia. No other body surface abnormalities were observed except for facial defects. Another medical examination regarding a defect in other organs or systemic conditions enabled us to describe it explicitly because of limited data. In the frontal view, bilateral complete facial clefts were observed. The right side shows a Tessier type 4 cleft with wide inferior palpebral coloboma and exposure of soft tissue below the eyeball. The lower eyelid lashes were slightly lateral. On the left side was a Tessier type 3 cleft with extensive loss of lower eyelid skin as on the right side. The left nostril base was absent and continuous with a facial cleft on the left side. The premaxillary bone was deviated to the right, nasal columella was tilted to the right, and base of the right ala base was positioned largely upward. Bilateral alveolar cleft and complete cleft palate were observed. It was unclear whether it was hyperterolism or not. (Figure 1a and b) In the lateral view, an amniotic band scar was observed on the surface from the lateral commissure to the temporal region. No exophthalmos was noted. (Figure 1c and d)

Clinical view of the patient. (A)The anterior facial view showed asymmetric bilateral oblique clefts of Tessier type 3 and 4 cleft extending from the superior vermilion through the alar grooves up to the inferior eyelids. (B)The inferior facial view showed a bilateral cleft lip with a bilateral alveolar cleft with a right rotated premaxilla and a cleft in the left nostril. (C, D) Left and right lateral views showing the orbicularis oculi muscle and the amniotic band extending from the orbital commissure to the temporal side.
Before surgery, the patient was referred to a pediatrician and an anesthesiologist to evaluate the general condition related to preparation for surgery under general anesthesia.
Landmarks and incision lines around the defect area were created using methylene blue. (Figure 2) The upper lip area was designed using the modified DeHaan's method, assuming a bilateral cleft lip surgery. In other words, the skin from the base of the right alar base to near the base of the nasal dorsum was removed as excess tissue (Figure 2b※), and a skin flap was created. Similarly, on the left and right sides, an incision line was drawn from the alar base toward the base of the nasal dorsum, and the lateral skin was excised as excess tissue. In addition, the buccal subcutaneous tissue was widely dissected to provide sufficient mobility and attract the tissue to the midline. For the formation of the lower eyelid, a cutback was added to the base of the nasal dorsum and inserted into the lower eyelid incision, including the severed lower eyelashes, to form the medial canthus. The skin in the area of the band scar was excised and sutured to create a lateral canthus. The upper and lower eyelids were sutured and kept closed for 1 week postoperatively, particularly as the skin was moved extensively for this procedure (Figure 3).
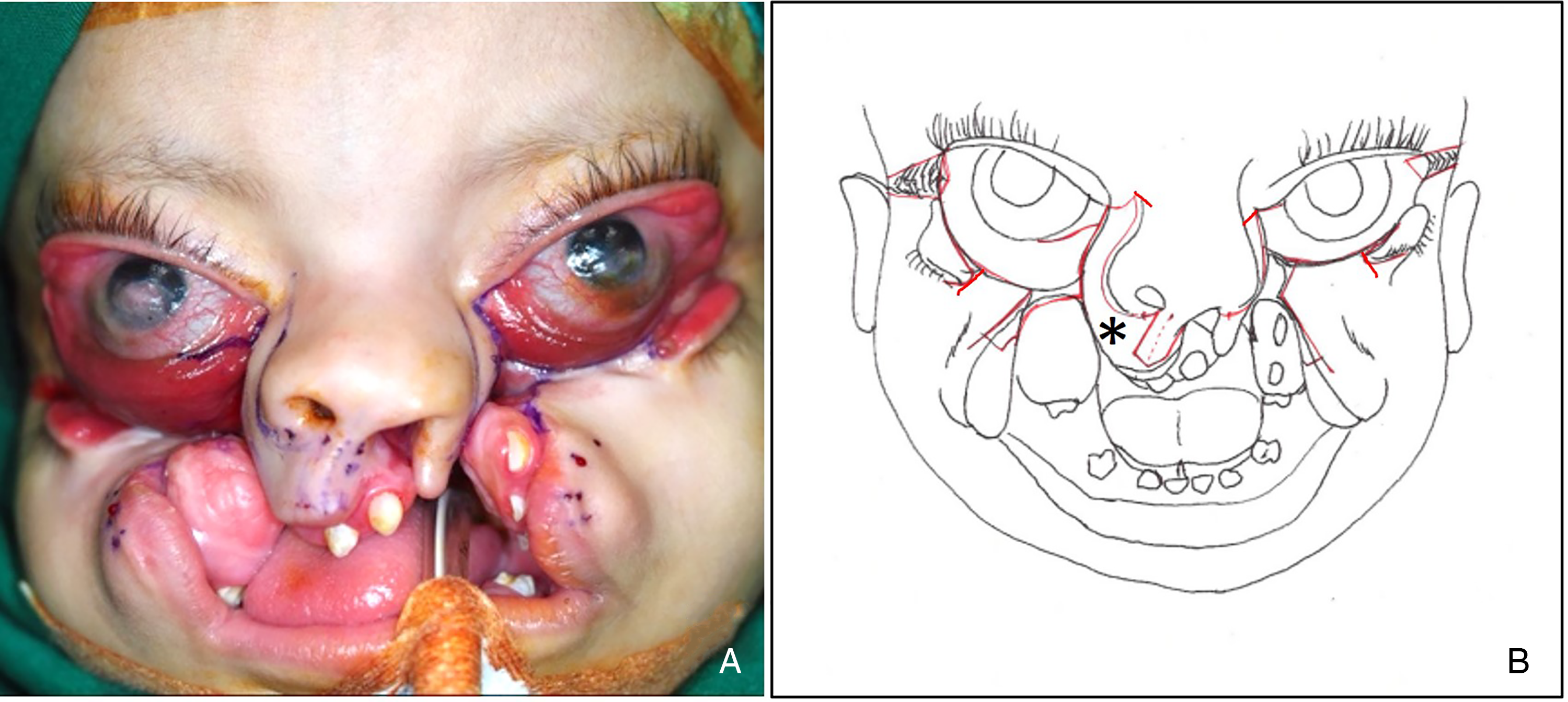
Setting the incision lines. (A) Incision line at the beginning of surgery. (B) Schema of the actual final incision line. The upper lip was designed using the modified DeHaan's method, in which the lateral skin from the base of the nasal ala to the base of the nasal dorsum was excised to form the cheek area (*). The medial canthus was formed by adding a cutback at the base of the nasal dorsum and inserting it into the lower eyelid incision.

(A) Anterior view after defect area was sealed by combination flap. (B, C) lateral view after defect closure.
On follow-up 4 months post-surgery, the patient revealed acceptable soft tissue healing and symmetrical facial contours. In addition, the orbicularis oris muscle functioned, which was confirmed when the patient cried or laughed. The ocular part revealed persistent ectropion of the eyelid, which required secondary correction. The following year, reconstructive surgery focusing on the eyelid area was performed. The patient is now 6 years old, has entered elementary school, and is attending school similar to a healthy child (Figure 4).

Post operated 4 years.
Discussion
Cases such as this are frequently attributed to failed mesodermal fusion during embryonic processes, although the exact cause of this case is unknown. The etiopathogenesis cited in these instances includes an immediate halt in development, neurovascular insufficiency or necrosis, and tears in the developing maxillary process. Additionally, literature indicates that these malformations may be caused by a combination of directly tethered tissue migration, such as amniotic bands, and increased local pressure, resulting in cellular ischemia.5,6 Appley et al. reported that an amniotic band causes a complex lateral or oblique cleft. 7 Owing to the rarity and variable presentation of this condition, developing a standardized diagnostic and treatment algorithm is challenging. 7 Each operation must be performed precisely to achieve the best functional and aesthetic results in the shortest amount of time to achieve a more presentable appearance. The cleft becomes more complicated as it involves multiple areas, including the nasal, ocular, sinus, palate, alveolus, and soft tissue components. Consequently, depending on the age at which these structures are presented and their maturation or growth patterns, multiple operations are frequently required to correct these defects. 8
According to Chen et al., the repair of soft tissue deficits in Tessier type 3 and 4 clefts is based on four fundamental components: medial canthoplasty, rotation of the medially based nasal flap with advancement of the laterally based cheek flap, repositioning of the facial muscles, and placement of surgical scars along the lines of the facial unit. 8 Kim et al. used a straight-line advance-release technique. 9 Chen et al. believed that minimal scarring, good skin color matching, and natural facial expression were the most critical factors determining an excellent aesthetic outcome following craniofacial cleft correction. The traditional approach, which uses the interdigitating Z-plasty technique, frequently results in suboptimal scarring. The concept of midface rotation advancement in conjunction with repositioning of the nasalis and facial expression muscles, as well as the placement of suture lines along the junction of the nasal and cheek facial subunits, must be applied to circumvent the aforementioned disadvantages. 8
Historically, multiple local cheek and nasal flaps have been used to correct Tessier types 3 and 4 clefts. Resnick and Kawamoto proposed that the soft tissue Tessier type 4 cleft be closed with cheek and nasal flaps. 10 In some cases, the use of a nasal flap is impossible because of a significant lateral nose defect. Alternatively, straight-line cleft closure may be used. However, the risk of fistula development, due to tissue tension, and deformation of cheek scars is relatively high. In the present case, the bilateral cleft lips were repaired using the commonly used technique of orbicularis oris reconstitution at the same time. Laterally, the cheek flaps were advanced medially upward and downward to reconstruct the medial canthi and close the peri-nasal cleavages. The facial expression muscles were sufficiently dissected and functionally repositioned to achieve natural facial expressions. We used a midface rotational advancement flap without Z-plasty to obtain face harmony and reduce scar formation. The surgical outcomes were satisfactory according to both functional and aesthetic parameters.
Inevitably, in such cases, other deformities, such as depressed nasal tip, midface hypoplasia, residual scars, bilateral alveolar clefts, and constricted dental arch, are present; therefore, treatments of these deformities will need to be addressed in stages as the patient grows and develops. Speech therapies, orthodontic treatment, distraction osteogenesis, and orthognathic surgery may be required in the future owing to the constricted dental arch. The timing and harvest sites of bone grafts vary among surgeons. Costochondral grafting, with its reduced capacity for resorption, appears to be an appropriate method for the reconstruction of nasal and orbital defects; however, the timing of bone grafting is controversial. Sari suggested that grafts should be performed simultaneously with primary closure. 11 Resnick and Kawamoto suggested that bone grafting is preferable before the age of 5 years, and if severe bony deficiency of the orbital floor causes significant dystopia of the globe, orbital floor reconstruction should be considered at an earlier age. 10 Nevertheless, another study reported that the value of bone graft before 5 years on the maxilla is uncertain. Bone resorption occurs over time, and secondary bone augmentation may be necessary. 12 We believe that bone grafting to her inferior orbital rims and zygomatic areas may improve her lower eyelid position, although there is some disagreement in the literature as to the best timing for bone grafting in these cases. On the other hand, in this case, appropriate soft tissue reconstruction protected the eye and accepted the functional and aesthetic outcome of the face. In addition, the patient lived in an isolated area with inadequate medical facilities and it was financially difficult for her to undergo multiple surgeries, including bone grafting. For such patients, surgical techniques should be chosen to reduce the number of operations as much as possible. Long-term observation of facial growth and visual and oral function will be required in the future.13,14
We based our assessment of her situation on a video sent by a local staff member. In the video, she did not wear any glasses. She was able to write letters with a pencil while reading the Indonesian language (alphabet) aloud in the textbook. The speech was clear and did not evince severe VPI. Therefore, we concluded that the patient achieved a level of visual acuity and articulatory control that would allow her to live her life in school. However, A limitation of this patient's treatment is that she was not treated by a multidisciplinary team, including an ophthalmologist, a pediatrician and a speech and language therapist. It is therefore difficult to assess the effectiveness of the treatment, as specialist vision testing by ophthalmologists and training by speech and language pathologist cannot be carried out. We are very concerned regarding the social and psychological development of the patient in the future. We believe that speech disorders and bullying problems due to facial scarring will be issues that she will face in the near future. However, we believe that surgery has made a great difference in the patient's life compared with her initial condition. We would like to further consider not only surgical but also social and educational support for patients such as her in the future.
Footnotes
Acknowledgements
I would like to thank Dr.Joji Nakama (Yaeyama Hospital, Okinawa, Japan) for his significant contribution to treating and photographing this case.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Family members of patients in this case were informed about the purpose, methods, expected benefits, questions to be asked, and confidentiality of data. The importance of publishing facial photographs was explained to the patient's family and consent was obtained. (The consent form was already uploaded as an additional document.)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.