
Abstract
Objective
To assess the factors influencing the type and timing of Alveolar Bone Grafting (ABG) among cleft centers throughout India. To examine the decision-making criteria for orthodontic treatment and the timing of ABG.
Design
Cross sectional survey
Method
This survey was based on a convenience-based sample selected from cleft teams across India. The survey was formulated using the SurveyMonkey platform and emailed to 40 cleft teams. The survey included questions on demographics, timing, surgical protocol, orthodontic protocol, radiograph prescription rate, assessment methods for the success of ABG and three scenarios for evaluating the timing of the bone graft. The Chi-squared test was performed to evaluate the difference in opinion between specialists. The inter-examiner reliability was assessed using Kappa statistics.
Results
Thirty-five units completed the questionnaire. Most units operate with 1-2 surgeons, with 42.9% of them treating cleft patients for under 5 years. Only 11.4% of centres routinely advised oblique occlusal radiographs for post-surgery evaluation, and 31.4% prescribed CBCT. However, 40% of cleft teams did not perform audits to evaluate the success of ABG, and less than 50% advised radiographs six months post-surgery. Around 26% of centres do not routinely provide orthodontic treatment pre-ABG. The inter-examiner reliability for case scenarios showed poor agreement between the clinicians.
Conclusion
The survey showed a serious lack of consensus in the ABG treatment among cleft teams in India and emphasises the need for standardised protocols for the treatment of children with cleft palate. There is an urgent need to develop core outcome set in cleft.
Introduction
One in 700 people worldwide are born with cleft lip and palate. 1 Despite the absence of national epidemiological data in India, it estimated that 28 000 to 35 000 babies are bone with cleft each year. 2 Importantly, only half the percentage of patients have access or visit cleft centers for treatment. 3 Children affected by this birth defect have a high burden of care due to the need for multiple specialties to manage their complex needs from birth through to adulthood.
An anterior bony defect requiring alveolar bone graft surgery is present in all cleft cases involving the alveolar process. The Alveolar Bone Graft surgery (ABG) is carried out primarily to close any residual oro-nasal fistula, improve facial aesthetics, allow eruption of permanent teeth through the defect filled by the bone graft, and to improve speech. Primary alveolar bone grafting is the earlier surgery performed between two to three years of the life of a child, this being the less popular counterpart than the widely followed secondary alveolar bone graft (SABG). SABG is generally performed between the ages of 8 to 11 years, at the time of two-thirds of root apex formation of the maxillary permanent canine.4–6 However, there is a huge variation on the ideal treatment age, pre-graft orthodontic treatment, investigations routinely undertaken pre and post graft, bone graft donor site, and the post graft follow up time points for patients requiring ABG surgery at cleft centres across the globe.
A previous survey on the practice of alveolar bone grafting in the United States showed a huge variation in the care provided between cleft teams. 7 On the contrary, the care provided in the UK showed much more consistent results, except for pre-graft orthodontic treatment. 8 It is important to point out that there are no such studies looking at the care provided for these patients in India.
The current study aims to evaluate the protocol followed for patients with cleft palate requiring an ABG and to identify any variation in protocols practiced within centres in India. The survey also aims to assess the decision-making criteria for orthodontic treatment prior to alveolar bone graft surgery.
Methods
This cross-sectional questionnaire-based survey was on a convenience based sample selected from cleft teams across India. The online survey poll was compiled using the Survey Monkey platform with 29 questions, of which, 28 were multiple choice or semi open ended and one was open ended question. The questions were taken from the previously used UK questionnaire 8 and modified to reflect the current Indian clinical set-up. The ethical approval was obtained from Sree Balaji Dental College Institutional Ethics Committee.
The online survey was then emailed to 40 cleft teams, both to surgeons and orthodontists, who treat cleft patients in their respective centers. A personal reminder was given when the teams visited the Indian Cleft conference in 2022. The teams were asked to complete the form as a group, but no checks were in place to oversee this. One from each center was returned and included in the analysis.
The survey was in English, as all clinicians had university education in English and had a sufficient level of English proficiency. The survey included questions on demographics, timing of ABG, surgical protocol, orthodontic protocol, radiograph prescription rate and assessment methods for success of ABG (supplementary Table 1). The last three questions were clinical scenarios where respondents were provided with intraoral photographs and panoramic radiograph to answer the questions. The cases were carefully selected to reflect different stages of canine root formation and permanent lateral incisor position (Supplementary Table 1).
Statistics
The responses were exported into an Excel spreadsheet and data was cleaned and checked independently and in duplicate by two authors (MP and BT). Any discrepancies were resolved with mutual discussion. Descriptive statistics were performed, and results reported as percentage and numbers. The Chi-squared test was performed to evaluate the difference in opinion between specialists. The significance was kept at 0.05. Kappa statistics was used to evaluate the inter examiner reliability.
Results
Thirty-five responses (n = 35) were received from 35 individual respective cleft care treatment centers, from various parts of India.
Demographics
All the respondents completing the questionnaire were involved in the management of cleft lip and palate patients. Of the 35 respondents (Table 1) who completed the questionnaire, 13 (37.1%) were cleft orthodontists, 7 (20%) were plastic surgeons and 15 (44.8%) were oral and maxillofacial surgeons. More than 71.4% (n = 25) respondents were male. In 43% (n = 15) of the centres, the surgeons had less than five years of experience treating cleft patients, 7 centres (20%) had clinicians with more than 20 years of experience in cleft care, and 7 centres (20%) had 10 to 15 years of experience (Table 1).
Demographics.
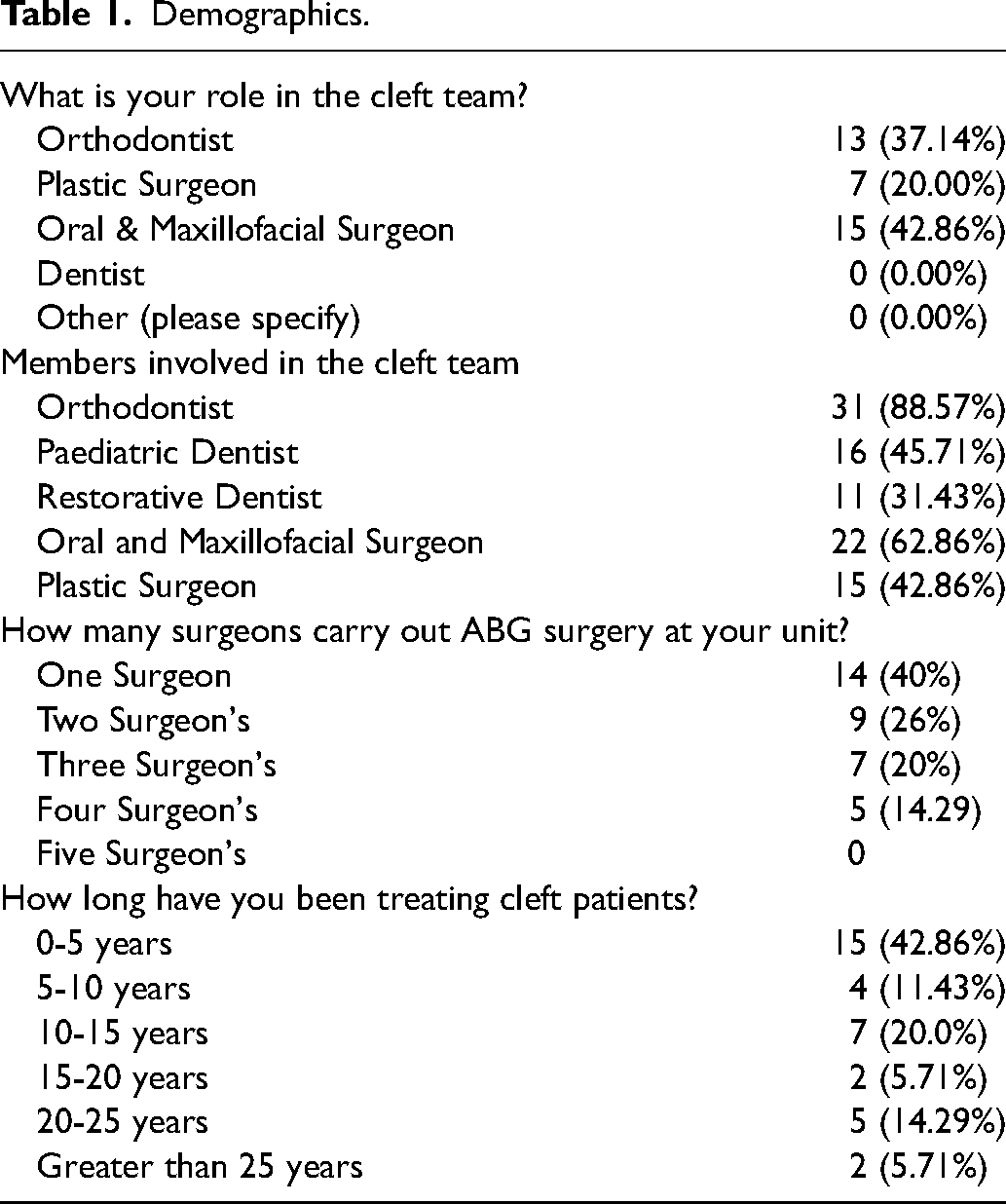
In their multidisciplinary teams, 88.6% had an orthodontist, 45.7% had a paediatric dentist and 31.4% had a restorative dentist in their team. All the teams either had an oral and maxillofacial surgeon or a plastic surgeon. Less than half (n = 14, 40%) of centres reported having a single surgeon performing ABG surgery, one fourth (n = 9, 26%) of centres had two surgeons, 20% (n = 7) had three surgeons, and five units reported having more than three surgeons carrying out ABGs.
Timing of Alveolar Bone Grafts
When asked whether the patients seen for ABG had their primary surgery at their centre, the response was mixed, with 71% (n = 25) of centres treating patients that were operated in their unit and 29% (n = 10) (Table 2) operating on patients having primary surgery mostly from other centres. When asked on the type of information provided to patients, majority of the centres reported providing verbal information (n = 29, 82.9%) and around half (n = 17, 48.6%) reported providing written information. A small proportion (n = 5, 14.3%) provided their patient information via a video, and 2 units (5.7%) provided no patient information (Table 2).
Timing of Alveolar Bone Grafting.
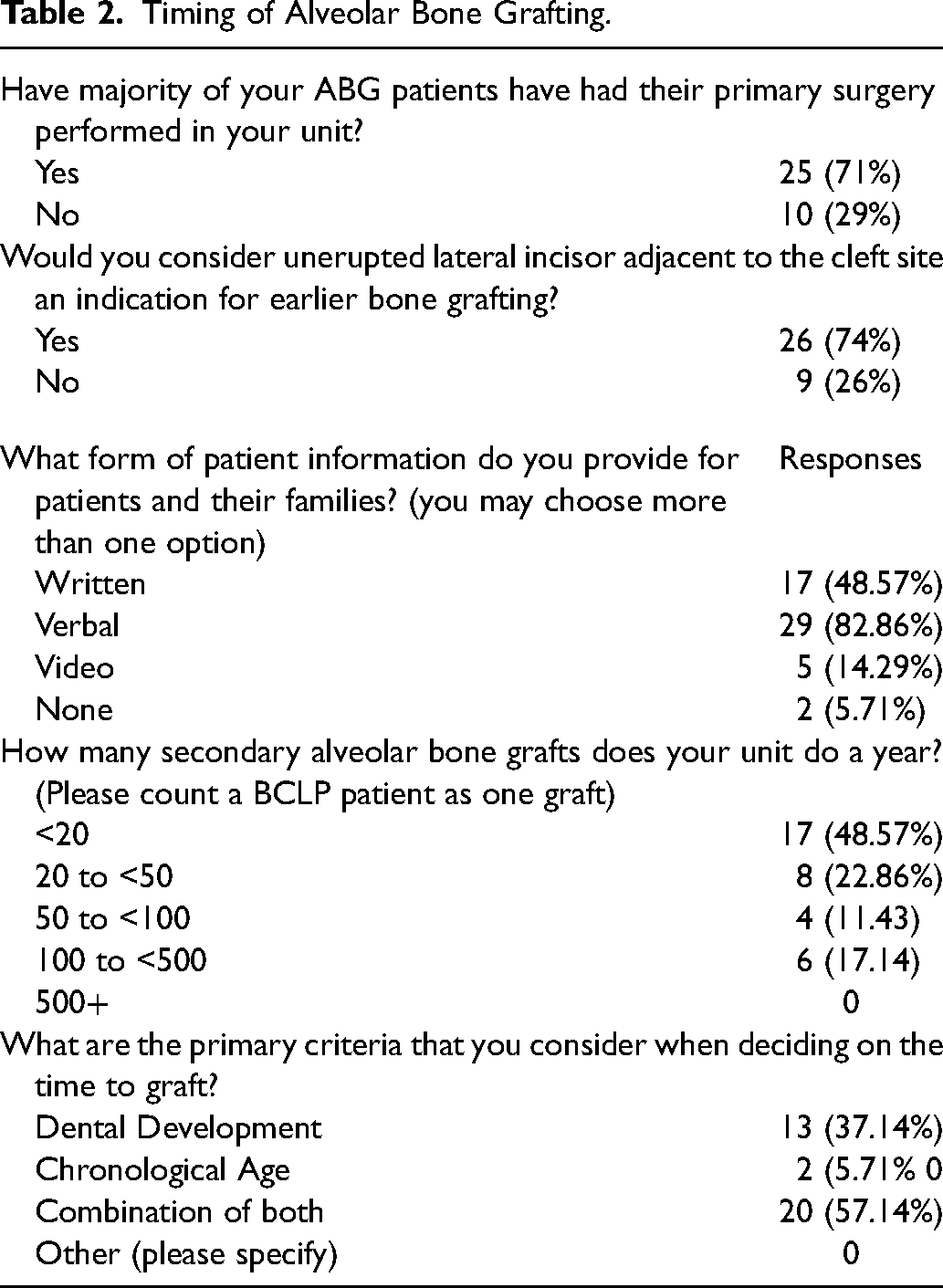
On the criteria considered for deciding on the timing for ABG, the majority of the centres (n = 20, 57.1%) reported a combination of dental development and chronological age, and the rest (n = 13, 37.1%) reported using dental developmental criteria alone (Table 2). When asked if “an unerupted lateral incisor adjacent to the cleft site an indication for earlier bone grafting?” 74% (n = 26) opting for ‘yes’ as an early indicator for bone grafting, while 26% (n = 9) reported not considering an unerupted lateral incisor to be an indicator for an early bone graft surgery (Table 2).
Radiographs Used Pre and Post ABG Surgery
For pre-operative radiographs, a routine orthopantomogram (OPG) was the widely preferred choice, with 85.7% (n = 30). Interestingly, Cone Beam Computer Tomography (CBCT) was a routine choice for pre-ABG surgery in 48.6% (n = 17) of centres (Table 3). Oblique occlusal and anterior occlusal were routinely used in 11.4% (n = 4) and 22.9% (n = 8) of centres, respectively. The least used radiographs were periapicals 5.7% (n = 2).
Radiographic Investigations and Audit Protocols.
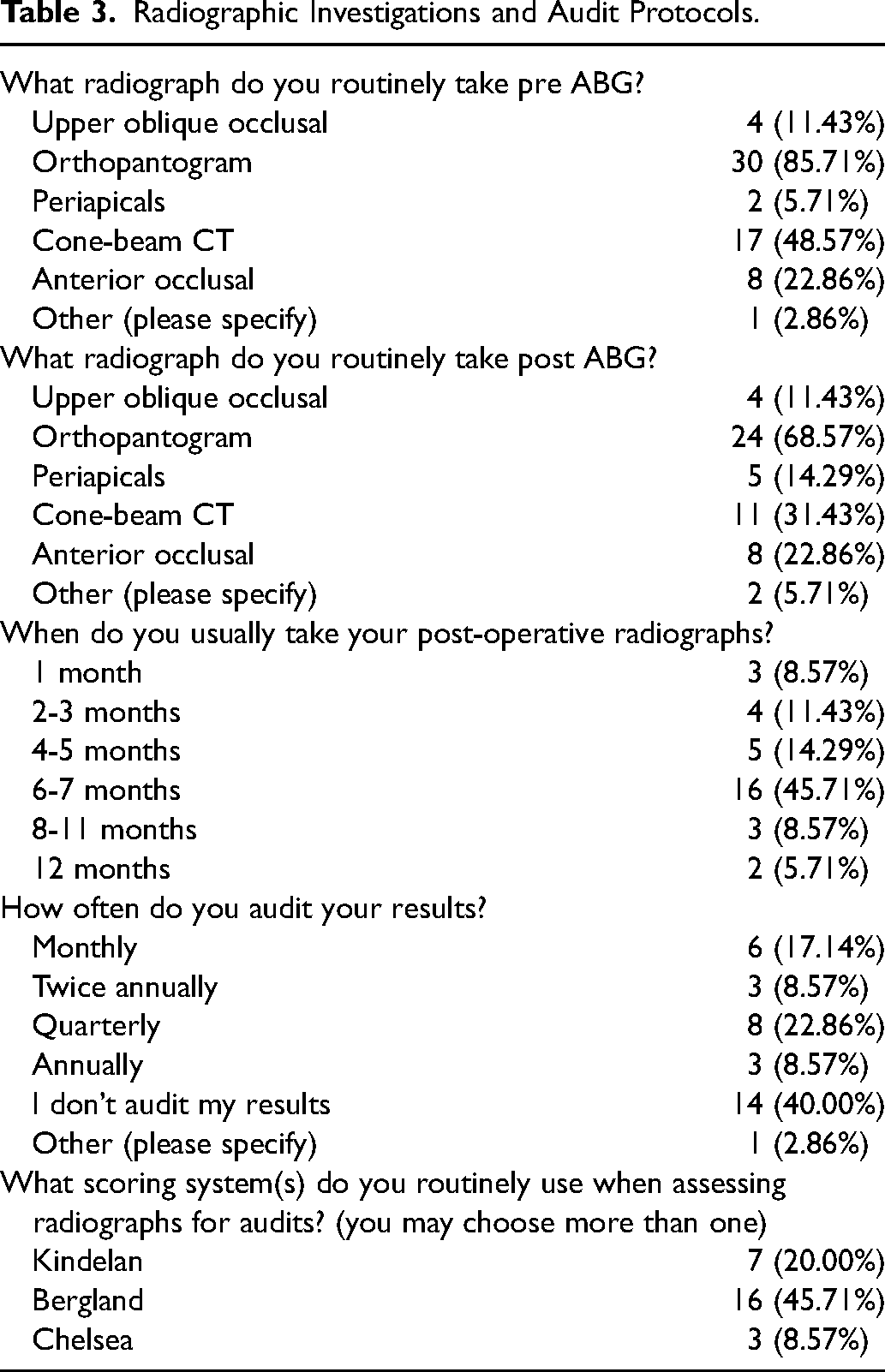
The results for postoperative radiographs routinely taken were similar to those for preoperative investigation with 68.6% (n = 24) routinely prescribing OPG radiographs, 31.4% (n = 11) prescribing CBCT radiographs, 11.4% (n = 4) prescribing oblique occlusals, 22.9% (n = 8) prescribing anterior occlusals, and 14.3% (n = 5) prescribing periapical radiographs (Table 3). Most of the respondents (n = 16, 46.7%) indicated that the post-operative radiographs were taken 6-7 months post ABG surgery. Fourteen percent (n = 5) reported taking radiographs at 4 to 5 months, 8.6% (n = 3) routinely took radiographs at one month post ABG and 14.3% (n = 5) reported taking radiographs at 8 months or after.
When asked about routine audits to assess the outcome of ABG surgery, 40% (n = 14) reported not performing any audits, 22.9% (n = 8) performing quarterly, 8.6% (n = 3) annually and 8.6% (n = 3) six monthly. Seventeen percent of respondents (n = 6) reported carrying out audits monthly. The common scoring criteria used for assessing successful bone grafts were the Bergland index (n = 16, 45.7%), followed by Kindelan's index (n = 7, 20%), the Chelsea index (n = 3, 8.6%), and 12 (34.3%) centres did not use any scoring system (Table 3).
Surgical Protocol
All the respondents reported using the iliac crest as the donor site for ABG surgery. Following ABG surgery, hospitalisation time was split evenly at 34% for one and three nights (n = 12) and 32% (n = 11) for two nights. (Table 4).
Surgical and Orthodontic Protocol.
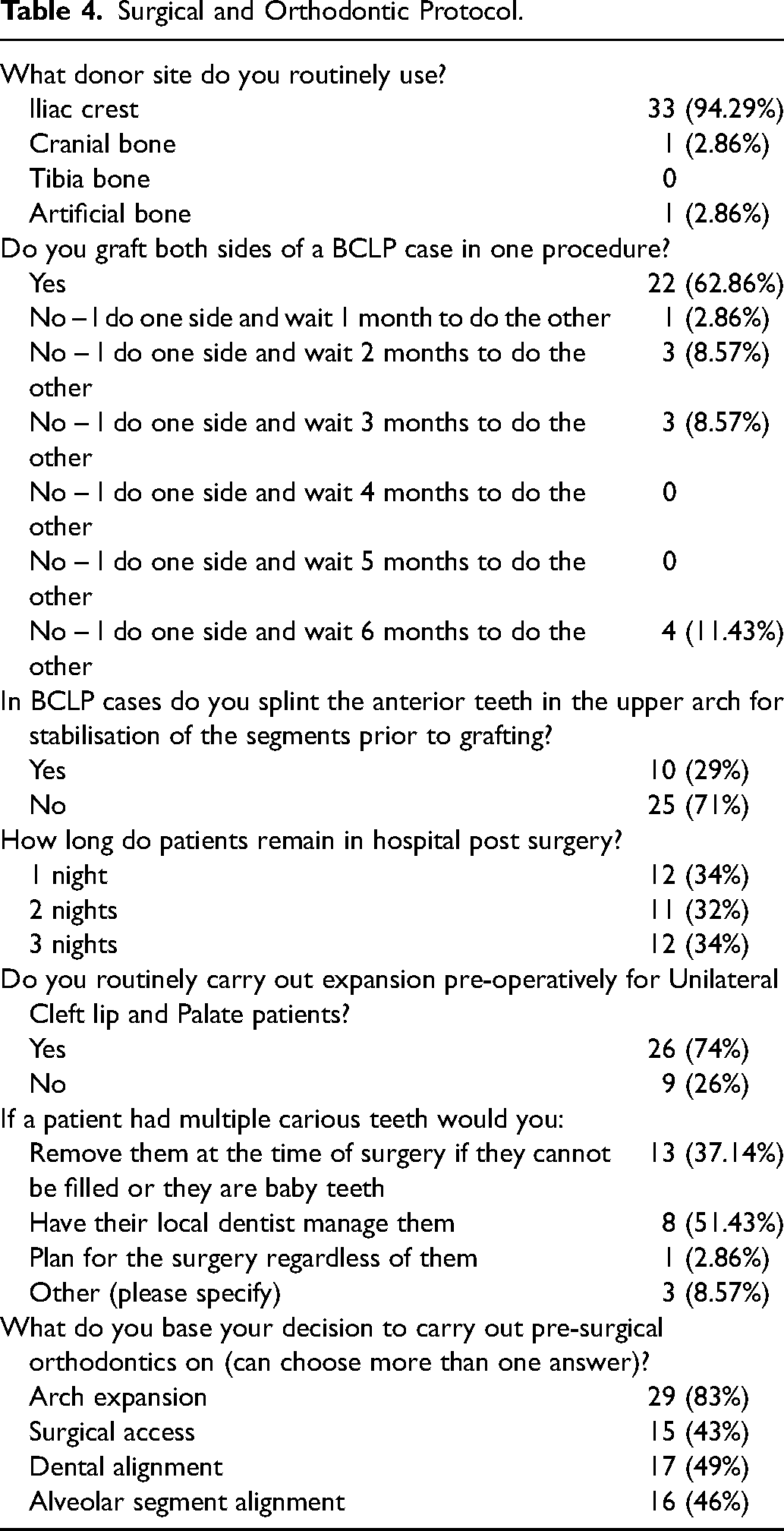
When asked about the timing of surgery (Table 4) for bilateral cleft palate patients, 62.9% (n = 22) reported performing surgery for right and left side simultaneously, 8.6% (n = 3) of centres reported performing one side and waiting for three months for the opposing side, while 11.4% (n = 4) reported waiting for six months between the two operations. In terms of protocols, 71% (n = 25) reported not splinting the upper anterior teeth in BCLP cases, and 29% (n = 10) respondents would splint the anterior teeth routinely prior to ABG surgery.
Orthodontic Treatment Protocol
When the respondents were asked whether they would routinely expand pre graft surgery, 74% (n = 26) reported they would, and 26% (n = 9) reported they would not routinely expand. Of those who reported not carrying out expansion routinely, they said on average they carried out pre-surgical orthodontics in 39% of cases (Table 4).
When asked “What do you base your decision to carry out pre-surgical orthodontics on?”, this was a multi-select question with 83% (n = 29) reporting the need for arch expansion, 43% (n = 15) for surgical access, 49% (n-17) for alignment of teeth and 46% (n = 16) for alveolar segment alignment. In terms of caries management, 37.1% (n = 13) of respondents would remove carious teeth at the time of surgery, and 51.4% (n = 8) would refer them to their local dentist prior to surgery.
The most important clinical outcome of success as being eruption of permanent teeth in the line of cleft was ranked first by 62.9% (n = 22), 20% (n = 7) reported bony infill as their first choice, 11.4% (n = 4) reported no fistula post treatment as their first choice and 2.9% (n = 1) reported aesthetics as their first choice (Figure 1).
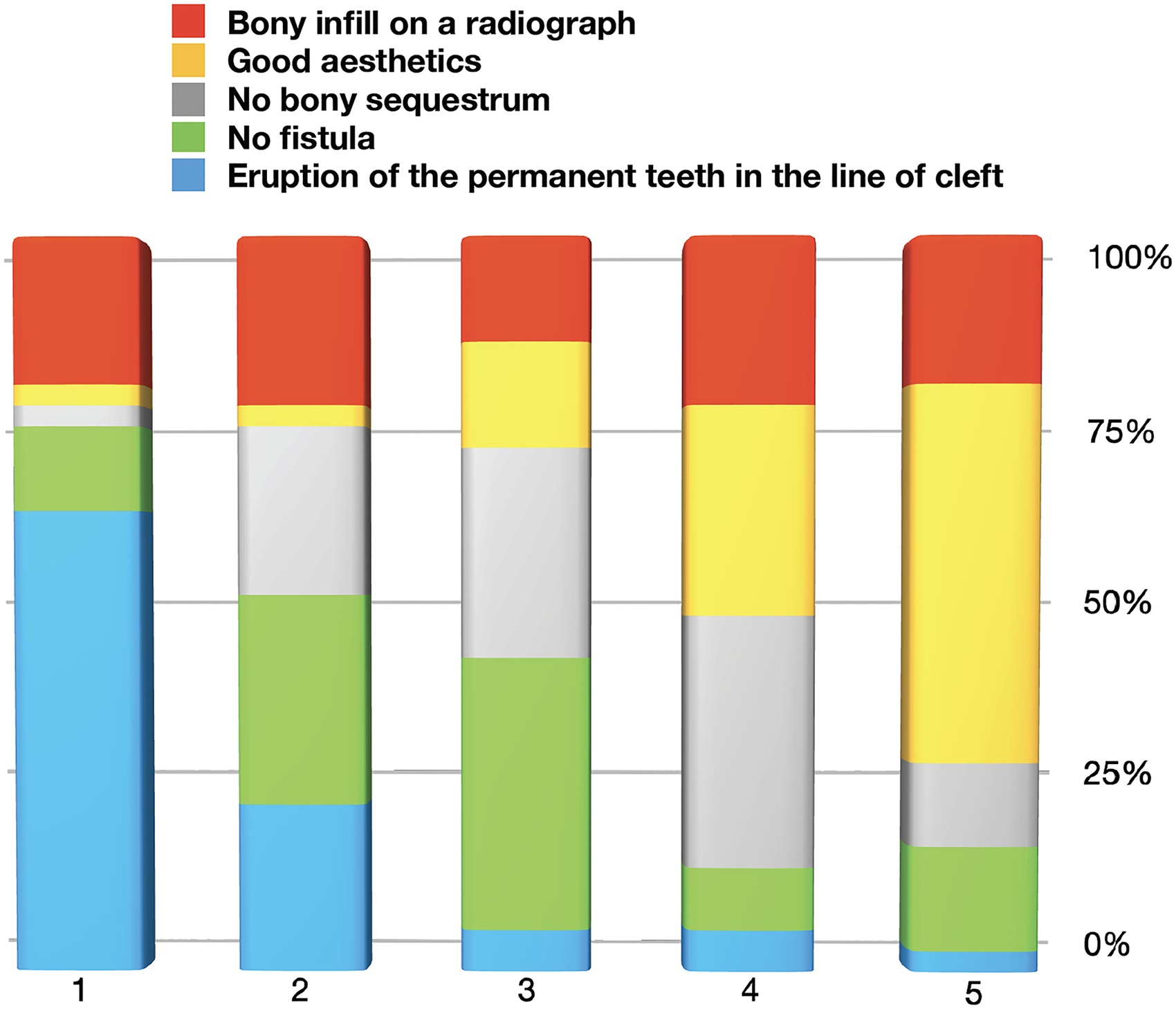
Answers to the question ‘what do you rate as the most important clinical outcome for success of ABG on a scale of 1 to 5 with 1 being most important and 5 being least important?’. The raters had to rank each outcome hierarchically from 1 to 5.
Clinical Scenarios
The agreement between centres for clinical scenarios on the timing of ABG is shown below (Figure 2):

Answers to the question ‘do you think, based on the ABOVE radiograph this patient is ready for their alveolar bone graft?’ (a) cleft on the left with canine root formation less than one-half, (b) cleft on the left with canine root formation two-thirds, (c) cleft on the right side with canine root formation nearly complete.
For scenario one, 61% (n = 17) of units agreed it was too early, 18% (n = 5) reported the patient was ready, 7% (n = 2) reported it was too late and 14% (n = 4) were unsure. A chi-square test for agreement amongst the respondents showed poor agreement (P = .12) between the respondents.
For scenario two, 66% (n = 19) thought the patient was ready for surgery, 14% (n = 4) thought it was too late, 17% (n = 5) thought they were unsure and 3% (n = 1) thought the case was too early for surgery. The chi-square test revealed a very good agreement between the respondents. P-value of P = .86 demonstrating very good agreement.
For scenario three, 55% (n = 16) of respondents thought this scenario was ready for surgery, 13% (n = 4) thought it was too late for this scenario to have surgery, 21% (n = 6) were unsure, and 21% (n = 6) of respondents said it was too early. For the final clinical scenario there was moderate agreement with a p-value of p = 0.47.
The opinions between orthodontists and surgeons did not show any statistically significant difference for all three scenarios (P = .12, .86 and .42 for scenarios 1, 2 & 3 respectively). The inter-examiner reliability results showed poor agreement between the clinicians (Kappa = 0.12).
Discussion
The results from this survey showed a huge variation amongst centres across India on the timing of bone graft, surgical and orthodontic treatment protocols, investigation methods and the type of outcome assessment methods. This is not surprising in cleft care and shows the urgent need for centralization and regularisation of cleft care in India.
A study published in 2022 9 highlighted the discrepancies in cleft care funding across India, with 87% of centres receiving funding via nongovernment organisations. More importantly, only 39% of centres were providing comprehensive cleft care. With only 68% of units having access to an orthodontist, it is evident that cleft orthodontic care in India is inconsistent, requiring an urgent need for more nationalised, coordinated care for our patients.
The present survey reported 88.6% of centres having an orthodontist, with the results not reflecting the current Indian scenario. 9 This is because only the centres providing comprehensive care were invited. However, two centres didn’t have an orthodontist, with orthodontic care being provided by dentists with a special interest in orthodontics. With regards to surgical care, 40% of centres had one surgeon and 26% of centres had two surgeons. A similar study in the UK reported 56% of centres having two surgeons, possibly due to the centralisation of services. 8
The type of patients being operated on is unique to India, as 29% of centres reported routinely operating on patients having their primary surgeries carried out at a different unit. Previous reports have shown that patients having primary surgeries at different centres had more complications and a more difficult ABG surgery. 10 However, there is a lack of data available on the success of ABG in India. The survey shows the average number of ABG surgeries performed in each unit is 36. The CSAG report from the UK reported that the minimum number of surgeries required from each centre should be at least 30. Similarly, in Germany, there is a minimum volume standard required to maintain quality. 11 This has been supported by numerous evidence from high quality studies and systematic reviews.12–14 The present survey showed that the Indian centres have a good volumes to maintain quality.
There is a huge variation between centres in the type of information provided for patients with only 48.6% providing written information. A previous study reported that a lack of information provided to patients by healthcare professionals led to confusion, increasingly vulnerable to misinformation, and an inability to combat stigma. 15 Additionally, it is shown that verbal information alone can lead to incomplete information being provided to patients and thereby poor compliance with treatment.16,17 This is especially important in the Indian context due to the language diversity that exists within the country. A recent study showed that immense language diversity and high patient volumes pose challenges in health care in India. 18
The present survey shows a lack of uniformity in assessing the post-operative results of ABGs, which is similar to the results from the US survey. 7 The variation in the types of radiographs being taken, which would impact the scoring system used, combined with the timing of the post-operative images being taken, makes it impossible to carry out inter centre audits. Additionally, 40% (n = 14) of centres in this study do not audit their results, making it challenging to assess how well a service is being provided. In the present survey, only 11.4% of the centres routinely advised oblique occlusal radiographs. This shows that the possibility of comparing their results with global standards would not be possible. This might also be the reason for not having any national data on the success of ABG in India. Although the use of CBCTs in nearly 50% of units pre-operatively and in 31.4% of units post-operatively demonstrates a greater appreciation of 3-D imaging over plain images, this significantly increases the radiation dose for paediatric patients. The survey shows an urgent need to establish core outcome measurement sets for cleft patients so national audits and comparable results can be made available. However, it is reassuring to know that the majority of respondents (68%, n = 23) felt the eruption of the permanent teeth in the line of the cleft as the most important clinical marker of success. This is good, as it could therefore be used as a nationally agreed clinical outcome measure for audit purposes.
The clarity in using the iliac crest as the donor site amongst all of the respondents is very encouraging, with the literature demonstrating a low incidence of morbidity from this site. 19 However, unlike the UK system, 8 none of the operations were carried out as day-case procedures, with patients being hospitalised for 1-3 nights. It's logical to presume that this discrepancy would add to the cost of the procedure. For UCLP cases, 74% (n = 26) routinely expand cases prior to their ABG, with other reasons for pregraft orthodontics being dental alignment, segment alignment, and finally surgical access. There was a majority view on timing, with 74% (n = 26) of respondents considering the presence of a unerupted lateral incisor adjacent to the cleft site to be an indication for earlier grafting. This is also demonstrated by the results that 57.1% (n = 20) feel a combination of chronological age and dental development determines the time to graft, with 37.1% (n = 13) having the view that dental development alone is a more important indicator. This general consensus that dental development itself was a key factor demonstrates an overall uniformity in the views across cleft centres in terms of timing. The use of an orthopantogram (OPG) by 85.7% (n = 29) or CBCT by 48.6% (n = 17) would allow for the determination of the dental development and primarily the root formation of the maxillary canine in the line of the cleft, if present.
It is interesting that 62.9% (n = 22) were carrying out ABG surgeries on both sides at the same time. While the literature shows that the majority of the centres have a six month interval between the two sides for bilateral patients, there is no clear consensus in this area. 20 Hence, it is challenging to infer a conclusion on the best methods as there is limited published data on the best approach to ABG surgery for bilateral cleft patients.
There is a debate within cleft clinicians on the benefits of expansion prior to bone grafting, with the only real consensus being that it is needed for surgical access and to align the segments to aid closure of the wound with a watertight seal. These results from the present survey showed 83% (n = 29) reporting that orthodontics is primarily carried out for arch expansion, 43% (n = 15) reporting it is for surgical access, 49% (n-17) for alignment of teeth, and 46% (n = 16) for alveolar segment alignment. The results are in accordance with the survey from the United States which showed 85% provided pre ABG orthodontics for expansion and 58% for expansion, crossbite correction and 25% for expansion, crossbite correction and anterior segment alignment. 21 However, only 3% of orthodontists would not provide any treatment, compared to 26% in this survey. This is interesting, as although there is a serious lack of evidence, orthodontists in the US seem to provide more extensive care pre ABG compared to Indian orthodontists.
Another debated topic in the field of orthodontics is the use of outcome measures. In cleft ABG cases, the historical scoring is performed using radiographs, but with the advent of CBCTs, there is no validated scoring system for using them. Although there are studies reporting the use of CBCT to evaluate the success of ABG surgery, 22 we feel that a clinical outcome measure such as the eruption of a permanent tooth into the cleft site would be a logical outcome measure. The present survey results show 68% of respondents ranking this as their ideal measure of success.
This section on clinical scenarios provided interesting results, with around up to one-third (24%) of the clinicians unable to come to a conclusion in the timing of surgery. Additionally, the majority of the clinicians (55%) graded the case with 90% root formation as being ready for surgery, with only 14% agreeing that this is too late. It is globally agreed that the best timing for surgery is when the canine is half to two-thirds formed. More importantly, 10% reported that the case was too early for surgery. Although it is globally agreed that the best results are achieved when ABG is carried out when the canine is half to two-thirds formed, the success of ABG depends on various other factors, including the amount of grafted bone, the extent of grafted bone coverage with the masticatory mucosa, the sound gingival attachment level of adjacent teeth, and more importantly, the skill of the surgeons. It is clear from the results of this survey that there is a serious lack of consensus among clinicians from centres across India, with no consistent clinical care protocol across cleft teams. The survey provides clear justification for reorganising cleft care in India and developing national guidelines on treatment. Although it can be agreed that India is geographically and culturally diverse and it is difficult to establish one protocol for all approach, it is important that some basic care pathways and clinical protocols must be established to improve the quality of care we provide for our patients. Additionally, there is also a serious lack of high-quality studies in this area that can be used to inform clinicians on the best care pathway for patients requiring alveolar bone graft surgery.
Limitations
The study was carried out on 35 cleft teams across India, and this may not reflect the entire Indian scenario. However, the number of teams providing comprehensive care, with access to surgery, speech, dentistry, and orthodontics is limited, with the majority of teams providing one or two specialties. The other limitation is the use of a non-validated questionnaire. The questionnaire, although not validated, has been previously used in the UK and has been adapted to reflect the Indian scenario. It is important to point out that there is no validated questionnaire in this area of cleft care.
Conclusions
There is a serious lack of consensus on the alveolar bone graft treatment among cleft teams in India, emphasising the need for standardised protocols for the treatment of children with cleft palate.
There is an urgent need to develop core outcome sets and core outcome measurement instruments in cleft care.
Supplemental Material
sj-pdf-1-cpc-10.1177_10556656231201491 - Supplemental material for A Survey on Alveolar Bone Grafting in Indian Cleft Centers
Supplemental material, sj-pdf-1-cpc-10.1177_10556656231201491 for A Survey on Alveolar Bone Grafting in Indian Cleft Centers by Badri Thiruvenkatachari, Manoj Prathap, Preeti Jauhar, Panchali Batra, Preetham Shetty and Pramod Subash in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the Science & Engineering Research Board, a statutory body of Department of Science & Technology (DST), Government of India (grant number CRG/2021/006208).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.