
Abstract
Sotos syndrome is a genetic disorder characterized by distinct craniofacial features, overgrowth in childhood, and impaired intellectual development. We herein report the successful orthodontic treatment of a 14-year-old boy with Sotos syndrome caused by a heterozygous mutation in the NSD1 gene. He showed severe hypodontia, impaction of the maxillary second molars and a skeletal Class III jaw-base relationship. Orthodontic management, including space control by protraction of the maxillary first molars and traction of the impacted molars, was performed using fixed appliances and miniscrews. As a result, acceptable occlusion was obtained without any discernible relapse 18 months postretention.
Introduction
Sotos syndrome is a neurologic disorder characterized by overgrowth from the prenatal stage through childhood with advanced bone age, impaired intellectual development, and distinctive craniofacial features, with an incidence of approximately 1/14,000.1,2 It may be accompanied by various complications, including cardiovascular, urogenital, ophthalmic malformations, seizures, scoliosis, and behavior problems.2,3
The distinct craniofacial appearance of the syndrome is characterized by a large skull, a long and narrow face, hypertelorism, downward-slanting eyes, acromegalic features, metopic protrusion and a pointed chin.1,2 Previous reports have described the characteristic craniofacial morphology of individuals with Sotos syndrome by analyzing cephalometrics, identifying retrusion of the maxilla and mandible, a long facial height, a large gonial angle, N-S-Gn angle and Ar-Go-Gn angle as being involved.4–6 In addition, a variety of dental-oral abnormalities have been reported, including hypodontia, excessive tooth wear, premature tooth eruption, enamel hypoplasia, talon caps, ectopic eruption, high palate, discoloration, crossbite and deep bite.3–5,7–9
Given these craniofacial and dental-oral manifestations in Sotos syndrome, orthodontic treatment is often needed to improve the oral health of such patients. When orthodontic treatment is performed in these patients, the orthodontist should make an individualized orthodontic treatment plan based on the dental and craniofacial characteristics associated with Sotos syndrome. However, there is still a lack of information regarding orthodontic treatment in such patients.10,11
Genetically, Sotos syndrome is typically caused by a heterozygous mutation in the NSD1 gene (mutation-type) or by a deletion in the 5q35 region including the genomic sequence in addition to the NSD1 gene (deletion -type). 1 There are ethnic differences in the frequency of these two genetic subtypes. According to Kurotaki et al., the deletion type was the most common cause of Sotos in the Japanese populations (52%), 12 whereas the mutation type (83%) was the most common cause in the non-Japanese populations. 2 Several studies have examined the genotype-phenotype relationship in Sotos syndrome, suggesting that the phenotypes differ between the two genetic subtypes.5,7,13 Thus, genetic information seems essential for better understanding the etiology of the craniofacial and dental-oral abnormalities in patients with Sotos syndrome and planning appropriate orthodontic treatment for those patients.
We herein report the successful orthodontic treatment of a Japanese boy with Sotos syndrome caused by mutations in the NSD1 gene (c.5020T > G, p.C1674G). The patient showed seven congenital missing teeth (all second premolars, the mandibular lateral incisors and the maxillary right first premolar), impaction of the maxillary second molars and a skeletal Class III jaw-base relationship. Orthodontic management, including protraction of the maxillary first molars to create alignment spaces of the maxillary second molars and traction of the maxillary second molars, was performed using fixed appliances and miniscrews. After 40 months of active treatment, acceptable occlusion was achieved. The present report aims to provide further information regarding the progress of orthodontic treatment for patients with Sotos syndrome.
Case History
A Japanese boy with Sotos syndrome (14 years and 8 months old) was referred to our department. He reported symptoms of mild tenderness of the maxillary second molars while chewing or biting food with his molars. At 1 year and 3 months old, he had been clinically diagnosed with Sotos syndrome at Osaka University Hospital. Whole-exome sequencing identified heterozygous mutations in the NSD 1 gene (c.5020T > G, p.C1674G) (Figure 1). He had mild intellectual disability, renal pelvis enlargement on the right side and hernia.
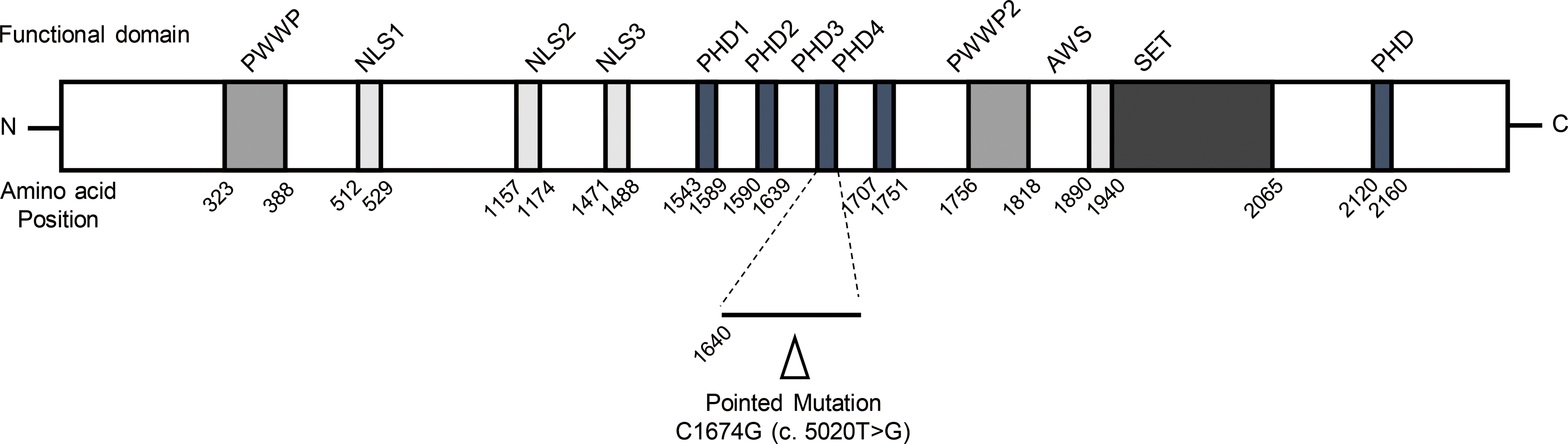
Schematic representation showing the genomic structure of NSD1 and location of the detected mutation. Filled boxes indicate the functional domains of NSD1. The arrowhead indicates the mutation detected in the present case. PWWP: proline-tryptophan-tryptophan-proline domain; NLS: nuclear localization signal; PHD: plant homeodomain domain; AWS: associated with SET domains; SET: Su (var)3–9, Enhancer-of-zeste, Trithorax domain.
At the orthodontic examination, the patient's bone height and weight were 173.9 cm (+1.23 standard deviation [SD]) and 60.7 kg (+0.58 SD), respectively. A distinct craniofacial appearance was shown, including a slightly protrusive forehead, a long and narrow face, hypertelorism, downward-slanting eyes and a pointed chin (Figure 2A). An intra-oral examination revealed a high palate, persistence of all deciduous second molars and deciduous maxillary right canine, mild crowding of the lower anterior teeth, excessive tooth wear at all first molars and caries at the deciduous maxillary second molars and the deciduous maxillary canine (Figure 2B). The maxillary second molars were unerupted, which resulted in the extrusion of the mandibular second molars. The molar relationships revealed a Class III relationship (Figure 2B). The maxillary dental arch was relatively narrow, and crossbite were seen at the deciduous maxillary right canine and the deciduous mandibular right second molar as well as the maxillary left first premolar and the deciduous mandibular left second molars (Figure 2B). Stainless-steel crowns had been placed on the deciduous mandibular second molars.

Pre-treatment records (age: 14 years and 8 months old). (A) Facial photographs; (B) intraoral photographs; (C) panoramic radiograph and hypodontia. The ○ symbol stands for congenitally missing permanent teeth; (D) three-dimensional reconstruction image showing the maxillary first and second molars; and (E) lateral cephalogram.
A panoramic radiograph confirmed that he had severe hypodontia, including seven congenital missing teeth from the second premolars, the mandibular lateral incisors, and the maxillary right first premolar, as well as impaction of the maxillary second molars (Figure 2C). Cone-beam computed tomography (CT) showed that the impacted maxillary second molars with cystic lesions were bilaterally located on the apical side at the distal root of the adjacent maxillary first molars. Distal root resorption of the maxillary first molars was also seen (Figure 2D). There were no adequate spaces in the lower dental arch for eruption of the maxillary second molars.
Compared to the Japanese norm, a lateral cephalometric analysis showed a retruded position (SNA angle: 72.7°, −2.7 SD) and a short anteroposterior length of the maxilla (Ptm-A/PP: 42.8 mm, −2.4 SD, Ptm-Ans/PP: 47.3 mm, −2.7 SD), which resulted in a skeletal Class III jaw-base relationship (ANB angle: −2.3°, −2.4 SD) (Figure 2E and Table 1). The N-S-Ba and gonion angle were large (N-S-Ba angle: 134.2°, 0.9 SD, gonion angle: 127.1°, 0.9 SD), which resulted in a high mandibular plane angle and excessive facial height (FMA angle: 30.9°, 1.3 SD). The maxillary incisors were normally inclined (U1 to SN angle: 104.9°, −0.2 SD), while the mandibular incisor was lingually inclined (IMPA angle: 80.1°, −2.4 SD). The overjet was large (overjet: 5.3 mm, 1.8 SD). In terms of tooth size, the lower incisors and lower canines were larger than the Japanese norms.
Lateral Cephalometric Measurements.
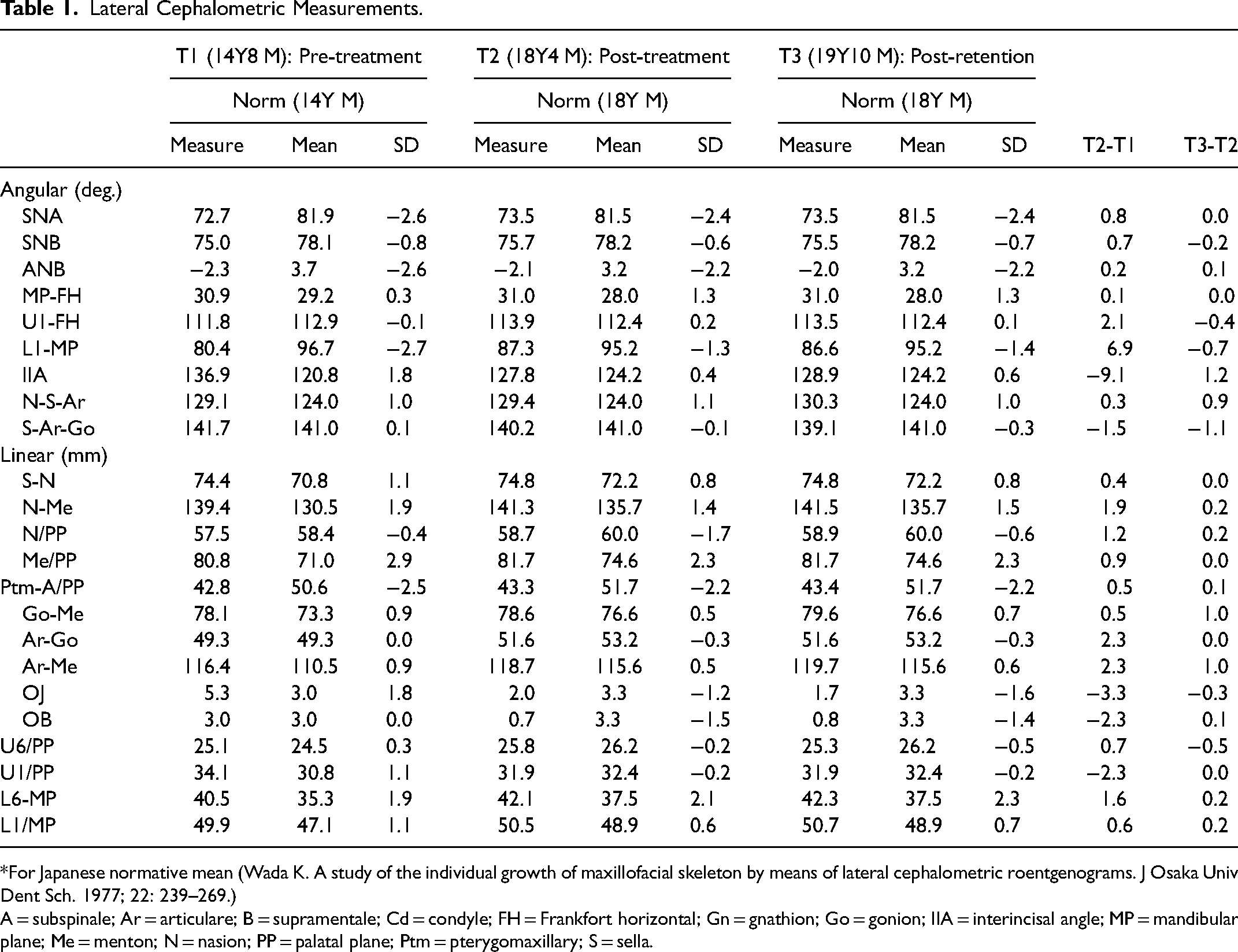
*For Japanese normative mean (Wada K. A study of the individual growth of maxillofacial skeleton by means of lateral cephalometric roentgenograms. J Osaka Univ Dent Sch. 1977; 22: 239–269.)
A = subspinale; Ar = articulare; B = supramentale; Cd = condyle; FH = Frankfort horizontal; Gn = gnathion; Go = gonion; IIA = interincisal angle; MP = mandibular plane; Me = menton; N = nasion; PP = palatal plane; Ptm = pterygomaxillary; S = sella.
Treatment Objectives
Given these findings, we diagnosed this patient with severe hypodontia, impaction of the maxillary second molars and a skeletal Class III jaw-base relationship. The treatment objectives were to achieve occlusion with acceptable intercuspation of the teeth and to maintain the facial profile.
The present case was therefore treated according to the following plan: (1) Extraction of both deciduous maxillary second molars and the deciduous right maxillary canine, (2) alignment of teeth with preadjusted edgewise appliances, (3) protraction of both maxillary first molars with miniscrews and a transpalatal arch (TPA), (4) exposure and traction of both maxillary second molars with a lingual arch, and (5) application of a prosthesis related to the absence of the right maxillary canine.
Alternatives
Regarding the impacted maxillary second molars, three treatment plans were planned for this patient through discussion with oral surgeons. For treatment plan A, the maxillary second molars would be extracted; for treatment plan B, the maxillary first molars would be extracted, followed by surgical exposure and orthodontic traction of the maxillary second molars; and for treatment plan C, the maxillary second molars would be exposed and aligned to the maxillary dental arch after protraction of the maxillary first molars. The advantages and disadvantages of all potential treatment plans were explained to the patient and his parents, and the patient and his parents ultimately choose treatment plan C. To idealize the skeletal proportions and provide the anterior occlusion with sufficient overjet, orthognathic surgery would have been more appropriate. However, the patient and his family expressed a desire to avoid orthognathic surgery.
Treatment Plan and Progress
After extraction of the deciduous maxillary second molars, a 0.022-inch slot preadjusted edgewise appliance and TPA were placed in the upper dental arch. Leveling and alignment of the upper dental arch were initiated with 0.014-inch nickel-titanium wires. Three months after leveling, 3 miniscrews (diameter, 1.4 mm; length, 6 mm; Dualtop autoscrews; Proceed Co., Ltd., Tokyo, Japan) were inserted as shown in Figure 3A. Under local anesthesia, two miniscrewes were inserted at the palatal side, and one miniscrew was inserted at the buccal side between the maxillary right lateral incisor and canine.
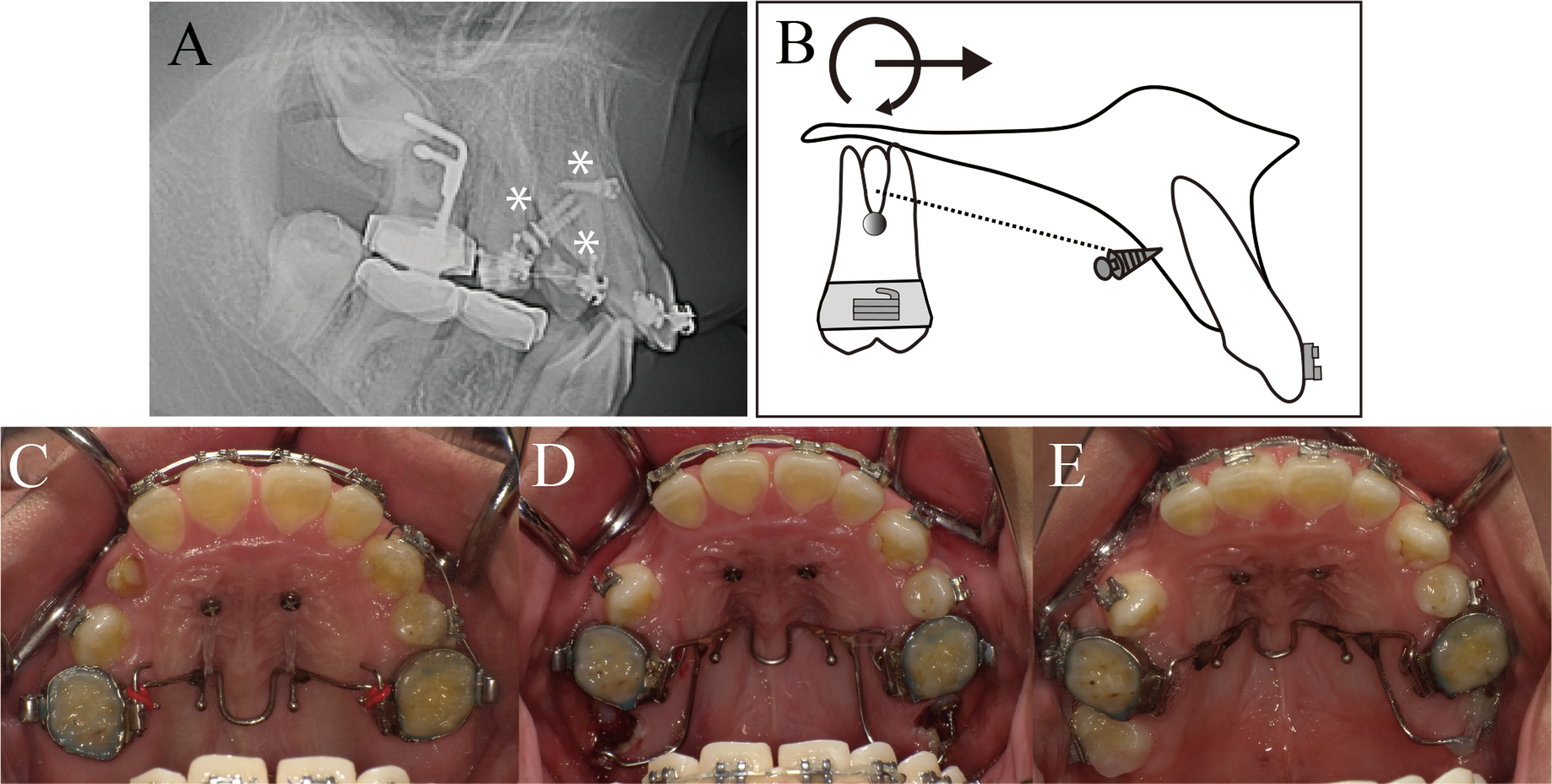
(A) the magnification of the lateral cephalogram showing the site of the miniscrew placement and the hook at the transpalatal arch. (B) Schematic representation showing the mechanics of protraction of the maxillary first molars. The ● symbol indicates the center of resistance, and the dotted line is the line of action of force, while the black line is the moment and force on the maxillary first molars. (C) Intraoral photographs during protraction of the maxillary first molars, (D) at the start of orthodontic traction of both maxillary second molars and (E) after orthodontic traction.
Three weeks after the insertion of the miniscrews, protraction of the maxillary first molars was started with the miniscrews and the hooks attached at the TPA (Figure 3A). The elastic modules were connected via the palatal miniscrews to the hook on the TPA (force, 150 g) above the line of action of the force passing to the center of resistance (Figure 3B). A 0.019 × 0.025-inch stainless steel wire was used as a working wire, and the maxillary first molars were protracted with sliding mechanics (Figure 3C).
Thirteen months after the start of loading, the spaces after extraction of the deciduous maxillary second molars were closed, which created adequate space for aligning the maxillary second molars. Surgical exposure and orthodontic traction of the maxillary second molars were then performed with a distal expansion lingual arch (Figure 3D).
Ten months after the start of traction, the maxillary second molars were aligned in the upper dental arch (Figure 3E). After traction of the maxillary second molars, the deciduous maxillary right canine was extracted, followed by protraction of the maxillary right canine using the elastic modules from the buccal miniscrew and the hook on the maxillary right canine.
Ten months later, the maxillary right canine had been brough adjacent to the maxillary lateral incisor. Leveling and alignment of the lower dental arch was then started 20 months after the start of leveling of the upper dental arch. A 0.022-inch slot preadjusted edgewise appliance and a lingual arch were used for the alignment of the lower dental arch and the intrusion of the mandibular second molars.
The total active treatment time was 40 months. After removal of the edgewise appliances, the bonded retainers were placed in both arches. A Begg type retainer was also used in the maxillary arch, but only at night.
Results
The posttreatment facial photographs showed that the facial profile had been maintained (Figure 4A). The posttreatment oral photographs revealed that the spaces related to hypodontia of the maxillary second premolars were closed by mesialization of the maxillary first molars; the maxillary second molars were aligned in the upper dental arch, and a space for the prosthesis related to hypodontia of the right maxillary first premolar was created by mesialization of the right maxillary canine (Figure 4B). Occlusion with acceptable intercuspation of the teeth was achieved, although it was not ideal (Figure 4B and Table 1). The canines remained in Class III relationships with a small overjet and overbite, due to hypodontia of seven permanent teeth and a skeletal Class III jaw-base relationship. The panoramic radiograph showed proper root paralleling including the maxillary second molars without any further root resorption of the maxillary first molars (Figure 4C). A posttreatment cephalometric analysis showed little change in the skeletal variables (Figure 4D and Table 1). The Class III jaw-base relationship and mandibular plane angle were unchanged (ANB: 2.2°, FMA: 31.0°) (Figure 5, Table 1). The maxillary first molars were protracted by 5.0 mm without any lingual inclination of the maxillary (U1-FH: 113.9°). The inclination of the mandibular incisors was increased (FMIA: 61.7°, IMPA: 87.3°), which resulted in an acceptable interincisal angle (IIA: 127.8°) and a normative overjet (1.5 mm). The 18 months post-retention examinations showed stable occlusion and a good facial profile without any discernible relapse. An implant or a fixed partial denture could have been placed in the space for a prosthesis due to hypodontia of the maxillary right premolar. However, considering the patient and his family's preference, a dental restoration was not pursued. Instead, regular periodontal treatment was provided.

Post-active treatment records (age: 18 years and 4 months old). (A) Facial photographs; (B) intraoral photographs; (C) panoramic radiograph; (D) lateral cephalogram.
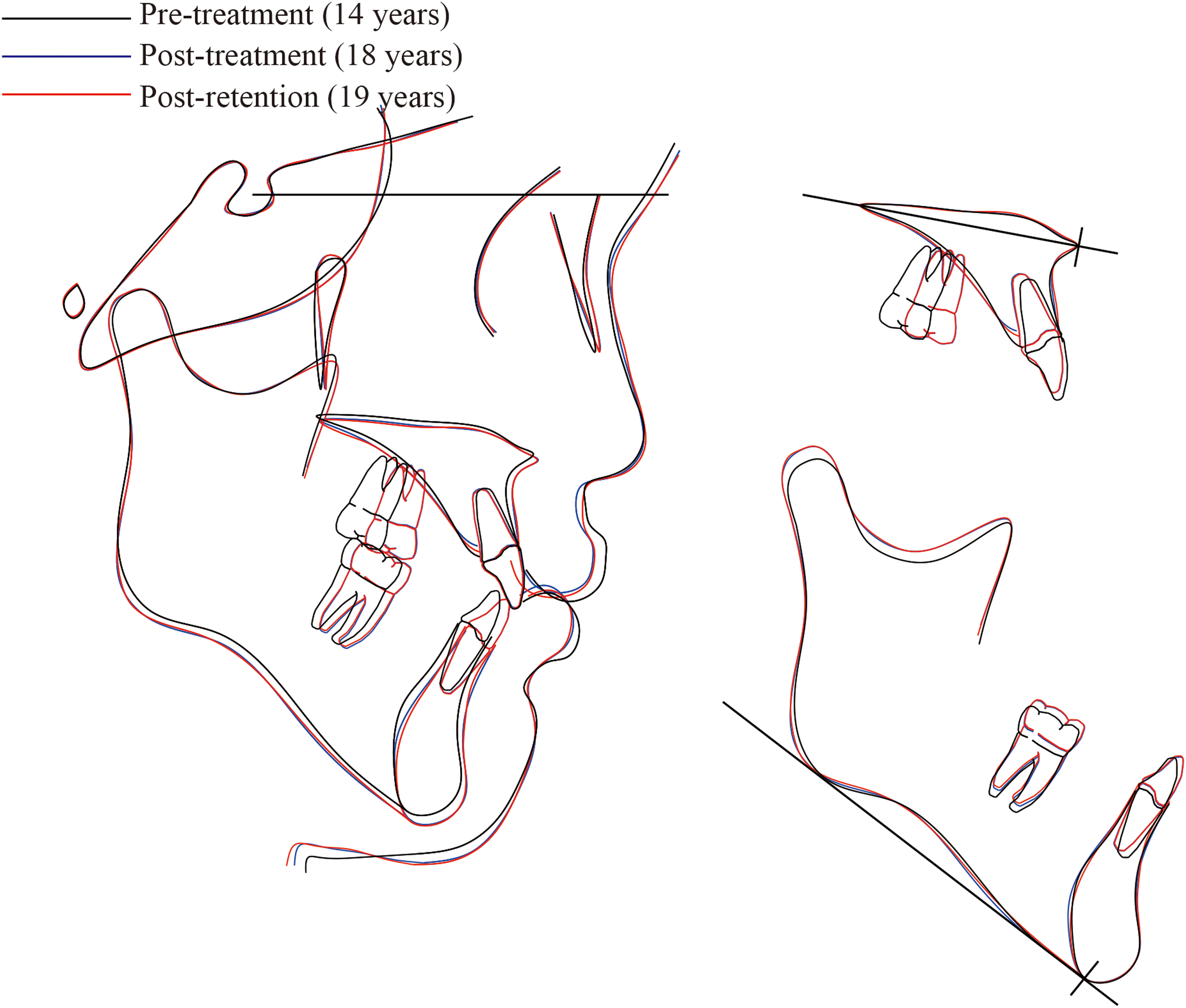
Superimposed lateral cephalometric tracings on the SN plane at the Sella, on the palatal plate at ANS, and on the mandibular plate at Me: pre-treatment (black line) and post-treatment (blue line), post-retention (red line). ANS, anterior nasal spine; Me, menton; N, nasion; PNS, posterior nasal spine; S, sella.
Discussion
Among the dental-oral manifestations observed in patients with Sotos syndrome, hypodontia has been the most frequently reported.4,5,8,9 Hirai et al. described hypodontia as being exclusively seen in the second premolars, with no marked differences in the number of missing teeth between the deletion and mutation types. 5 According to Kotilainen et al., 9 premolar hypodontia was recognized as a common feature of Sotos syndrome with heterozygous mutations, including microdeletion and point mutations in the NSD1 gene. In that study, a patient with a microdeletion had the most severe phenotype of tooth agenesis, while the patients with missense mutations had a mild phenotype of tooth agenesis, suggesting that the severity of hypodontia increases with the pathogenicity of the aberration in NSD1. Considering these previous findings, dental management of hypodontia may be required in patients with Sotos syndrome.
Generally, three treatment options are considered for hypodontia, depending on factors such as crowding, the relationship of the jaws, the patient's preference and cooperation in orthodontic treatment.14,15 These treatment options include (1) preservation of the deciduous teeth, (2) space maintenance or redistribution of space for a prosthesis and (3) orthodontic space closure. In the present patient with mutation-type Sotos syndrome who showed severe hypodontia in all second premolars, the mandibular lateral incisors and the maxillary right first premolar, space control for hypodontia was selected. First, the deciduous mandibular second molars were preserved because of the mild crowding in the lower dental arch and the relatively good condition of the deciduous teeth. Second, the deciduous maxillary right canine was extracted due to caries, and space for a prosthesis related to the missing maxillary right first premolar was redistributed by protraction of the right maxillary canine. Finally, the space related to hypodontia of the maxillary second premolars was closed by protraction of the maxillary first molars to create space for aligning the impacted maxillary second molars.
However, the side effect of mesial tipping of the maxillary first molars during the protraction was of some concern, since it would worsen the root resorption of the maxillary first molars by making contact with the impacted neighbor teeth. Recently, effective techniques for achieving molar protraction using miniscrews have been able to prevent mesial tipping of molars during the protraction.16–18 Therefore, to prevent mesial tipping of the maxillary first molars during protraction in our case, we connected the elastic modules from the palatal miniscrews to the hook on the TPA with the line of action of the force passed above the resistance center of the maxillary first molars. The TPA was also used to prevent mesial rotation of the maxillary first molars during protraction. As a result, space closure was achieved, followed by traction of the impacted maxillary second molars without further root resorption of the maxillary first molars.
In addition to hypodontia, various dental abnormalities were observed in the present case, including impaction of the maxillary second molars, high palate, crossbite, small dental arch of maxilla, deep bite, excessive overjet and excessive dental tooth wear, similar to previously reported findings.3–5,7–9 To provide preventive care for patients with Sotos syndrome at an appropriate timing, we recommend that dentists or orthodontists observe the dental-oral abnormalities of those patients regularly while taking panoramic radiographs. If ectopic eruption of the maxillary second molars in the present case had been detected earlier by observation with panoramic radiography, simple interceptive orthodontics, such as striping or extraction of the deciduous maxillary second molars, could have prevented impaction of the maxillary second molars and root resorption of the neighbor teeth.
In the craniofacial manifestation, patients with Sotos syndrome have a distinct craniofacial morphology with maxillary and mandibular retrusion and an excessive facial height.4,6,10 Hirai et al. 5 reported a tendency for maxillary retrusion to be found in Sotos syndrome of both the deletion type and mutation type, while mandibular retrusion is more frequent in deletion-type disease. To our knowledge, longitudinal studies on craniofacial growth in children with Sotos syndrome managed with or without orthodontic treatment are lacking. 11
In the present case, the maxilla was in a retruded position and small in size, whereas the mandible was in the normal position and large in size. This caused a skeletal Class III jaw relationship. A large gonial angle and N-S-Ba angle resulted in a high mandibular plane angle and excessive facial height. Although we were concerned about the direction and amount of mandibular growth in this patient during treatment due to the skeletal Class III relationship and large mandible size, the amount of mandible growth was small and proceeded in a straight-down direction, which largely maintained the skeletal variables in the anterior and vertical dimensions. During treatment, the changes in the maxillary incisor position were minimal, even though the maxillary molars were protracted. Our approach to space closure using miniscrews was also effective in maintaining the facial profile without any lingual inclinations of the maxillary incisors. The miniscrews helped manage the orthodontic treatment for this patient with Sotos Syndrome.
The present treatment was associated with several limitations. Firstly, the skeletal proportions were not corrected. Although orthognathic surgery would have been more appropriate to idealize the skeletal proportions, the patient and his family expressed a desire to avoid orthognathic surgery. Secondly, the final occlusion was not ideal, as the canines remained in Class III relationships with a small overjet and overbite. This difficulty arose due to tooth size discrepancy with hypodontia of the mandibular lateral incisors, the second premolars and the maxillary right first premolar. Achieving an ideal canine relationship was challenging in this case. The bilateral mandibular first premolars were substituted for the canines, and a canine guide was not provided. Furthermore, the resultant compromised anterior occlusion was in conjunction with a skeletal Class III jaw-base relationship. Orthognathic surgery would have provided more advantages in achieving an ideal anterior occlusion. One additional reason for the insufficient overjet and the heavy anterior fremitus was associated with the Bolton discrepancy, which resulted from the preservation of mandibular primary second molars that are wider than the subsequent premolars. If the stainless-steel crowns on the mandibular primary molars were replaced with premolar-sized crowns, it would create leeway space allowing for the retraction of the mandibular anterior teeth, potentially leading to a significant improvement in occlusion. However, the patient did not wish for the restoration of the mandibular primary molars.
Lastly, the treatment duration extended to 40 months. The main reason for this prolonged duration was the closure of spaces related to hypodontia and the alignment of impacted second molars, which required a considerable amount of time. It should be noted that if a treatment involving prosthetic intervention for the spaces related to hypodontia and extraction of the impacted teeth had been pursed, the treatment duration would have been shorter. Additionally, patients with Sotos syndrome commonly exhibit varying degrees of intellectual disabilities, which can present challenges in adapting to orthodontic treatment and maintaining proper oral hygiene. In such cases, avoiding prolonged orthodontic treatment may be advisable. Treatment duration varies depending on the orthodontic intervention. Therefore, it is important to thoroughly evaluate whether the orthodontic treatment option is justified in relation to the final outcome and alternative options on an individual basis. Careful diagnosis and treatment planning are required for managing malocclusion associated with Sotos syndrome.
Conclusions
We described the orthodontic management of a Japanese boy with Sotos syndrome caused by mutations in the NSD1 gene who showed severe hypodontia, impaction of the maxillary second molars, excessive overjet and a skeletal Class III jaw-base relationship. Traction of the impacted molars and space control by protraction of the maxillary molars were performed using miniscrews and fixed appliances. As a result, acceptable occlusion was achieved. Our results suggest that orthodontic treatment can help improve the oral health of people with Sotos syndrome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Informed consent was obtained from the patient and the mother for their anonymized information to be published in this article.