
Abstract
Objective
Objective measurement of pre-operative severity is important to optimize evidence-based practices given that the wide spectrum of presentation likely influences outcomes. The purpose of this study was to determine the correlation of objective measures of form with a subjective standard of cleft severity.
Design
3D images were ranked according to severity of nasal deformity by 7 cleft surgeons so that the mean rank could be used as the severity standard.
Patients
45 patients with unilateral cleft lip and 5 normal control subjects.
Interventions
Each image was assessed using traditional anthropometric analysis, 3D landmark displacements, and shape-based analysis to produce 81 indices for each subject.
Main Outcome
The correlation of objective measurements with the clinical severity standard.
Results
Lateral deviation of subnasale from midline was the best predictor of severity (0.86). Other strongly-correlated anthropometric measurements included columellar angle, nostril width ratio, and lateral lip height ratio (0.72, 0.80, 0.79). Almost all shape-based measurements had tight correlation with the severity standard, however, dorsum deviation and point difference nasolabial symmetry were the most predictive (0.84, 0.82).
Conclusions
Quantitative measures of severity transcend cleft type and can be used to grade clinical severity. Lateral deviation of subnasale was the best measure of severity and may be used as a surrogate of uncoupled premaxillary growth; it should be recorded as an index of pre-operative severity with every cleft lip repair. The correlation of other measures evaluated clarify treatment priorities and could potentially be used to grade outcomes.
Introduction
Optimal treatment of the unilateral cleft lip nasal deformity (uCLND) remains a significant challenge. Persistent deformity is common, revisions are frequent, and practices rely heavily upon expert opinion.
Objective and quantifiable measurement of uCLND before and after treatment would facilitate evidence-based practices. By enabling evaluation of outcomes and identification of effective treatments, providers could improve care. The first step in doing so is to define severity because the spectrum of presentation varies widely from subtle blemishes to markedly twisted nasolabial form; the presentation likely influences the outcomes that can be achieved; and measuring post-operative form must consider varying combinations of residual deformity and iatrogenic changes.
Advances in 3D image analysis have allowed for novel methods to assess form that is specific to children with uCLND. In addition to traditional anthropometric analysis,1,2 3D displacements of landmarks can now be tracked, 3 and computer vision techniques have been used to leverage the rich 3D surface data to quantify various aspects of symmetry.4–6 Although an array of measurements for uCLND have been developed that are objective, quantitative, and based upon our understanding of embryologic processes, their clinical relevance needs to be assessed.
The purpose of this study was to determine the correlation of objective quantitative measures of 3D nasolabial form with a clinical qualitative consensus of uCLND severity. Those indices included traditional anthropometric analysis, 3D landmark displacements, and shape-based analysis of form.
The most relevant measures could provide insights into important aspects of the deformity, may be used as objective indices of severity without the need for clinical assessments, and could potentially be used as metrics in assessment of treatment outcomes.
Methods
This prospective study was approved by Institutional Review Board. All subjects (patients and surgeons) provided informed consent to participate.
Image Set
A previously established image-set of 45 infants with unrepaired unilateral cleft lip (that span the spectrum of presentation) and 5 age-matched controls 7 was studied. 3D stereophotographs were captured by a professional image technologist using the 3dMDCranial system (3dMD, Atlanta, GA). Images were processed by extracting the face within the image and normalizing to a standard facial frontal plane. 8
Subjective Assessment of Clinical Severity
For qualitative assessment, images were randomly distributed in a digital “shuffleboard” that allows raters to re-order the images into their desired sequence. The stereophotographs could be examined in detail allowing for zooming, panning, and rotation, of the face to any desired angle. The shuffleboard layout also facilitated side-by-side comparisons of images (Supplemental Digital Content 1). Raters were asked to place the subjects in order of worst-to-best nasal appearance. Seven experienced (mid-career) cleft surgeons were recruited from Canada and the United States. Two raters repeated their assessments after a 3-week washout period so that intra-rater reliability could be estimated. The mean rank score was considered the clinical consensus.
Objective Measurement
For quantitative assessment, each subject image was labeled with 44 anatomic landmarks using 3dMD Vultus (3dMD, Atlanta, GA) (Figure 1). Definitions for measurement have previously been described1,3–7 and are detailed in Supplemental Digital Content 2.
Traditional anthropometric analysis
Twenty-five standard and previously described nasolabial angles, dimensions, and ratios1,7 were calculated using the landmarks that were placed.
3D landmark displacements
The vectors of 15 nasolabial landmarks were determined along x, y, and z axes to produce 45 vectors per image. The inter-endocanthion line defined the x-axis with its midpoint considered facial midline
9
and origin. Rotation was set by a 7.5° upward rotation from the endocanthion-tragal axis to define y (cranio-caudal) and z-(antero-posterior) axes as previously described.3,10
Surface shape-based analysis
Eleven indices were developed for assessment of cleft deformity using available computer-vision techniques. Technical details have been described.4–6 The regions and features of interest are summarized (Figure 1).
Nose and lipWith the oral commissures and the level of the inter-endocanthion line defining the nasolabial region, symmetry across the facial midline was measured by differences in points, surface curvatures, and the normal vectors to the surface (“Point”, “Radius”, and “Angle” difference).
4
NoseTo specifically assess the nose, facial recognition software was used to crop the nose from the mesh so that it could be sliced into coronal planes to define various depths, like a contour map. The aggregate differences in plane surface areas across the midline produced an index of nasal asymmetry known as “Depth area difference”.
5
Variation in form from normal was also calculated using “PCA reconstruction”, a computer science method of constructing a normal reference from a given image. The measured reconstruction error is an indication of how different a given nose is from the normal reference.
5
Upper noseTo specifically assess the upper nose, surface changes along transverse contour lines were used to detect the prominence of the dorsum so that deviation from the inter-endocanthion midline could be quantified as the “Dorsum deviation”.
6
“Nasal axis deviation” is a similar measure but utilizes landmarks identified by computer-based template mesh deformation and measures the deviation of the plane formed by nasion, pronasale, and subnasale from inter-endocanthion midline.
4
Lower noseTo specifically assess the lower nose, surface changes along transverse contour lines across the alar-tip region were used to isolate the nose from the cheeks so that the difference in the volume of the nose across midline could be quantified as the “Alar-tip volume ratio”.
6
“Alar-cheek definition” was calculated as the average difference in angles between ala and cheek surfaces throughout the junction of the alar and cheek subunits.
6
Several other measures were derived from dimensions calculated from landmarks identified by computer-based template mesh deformation.
4
“Nasal tip deviation” was the distance of the auto-landmarked pronasale from midline. “Columellar deviation” was the difference in angles between auto-landmarked pronasale, sunasale, and alare on each side of the nose.
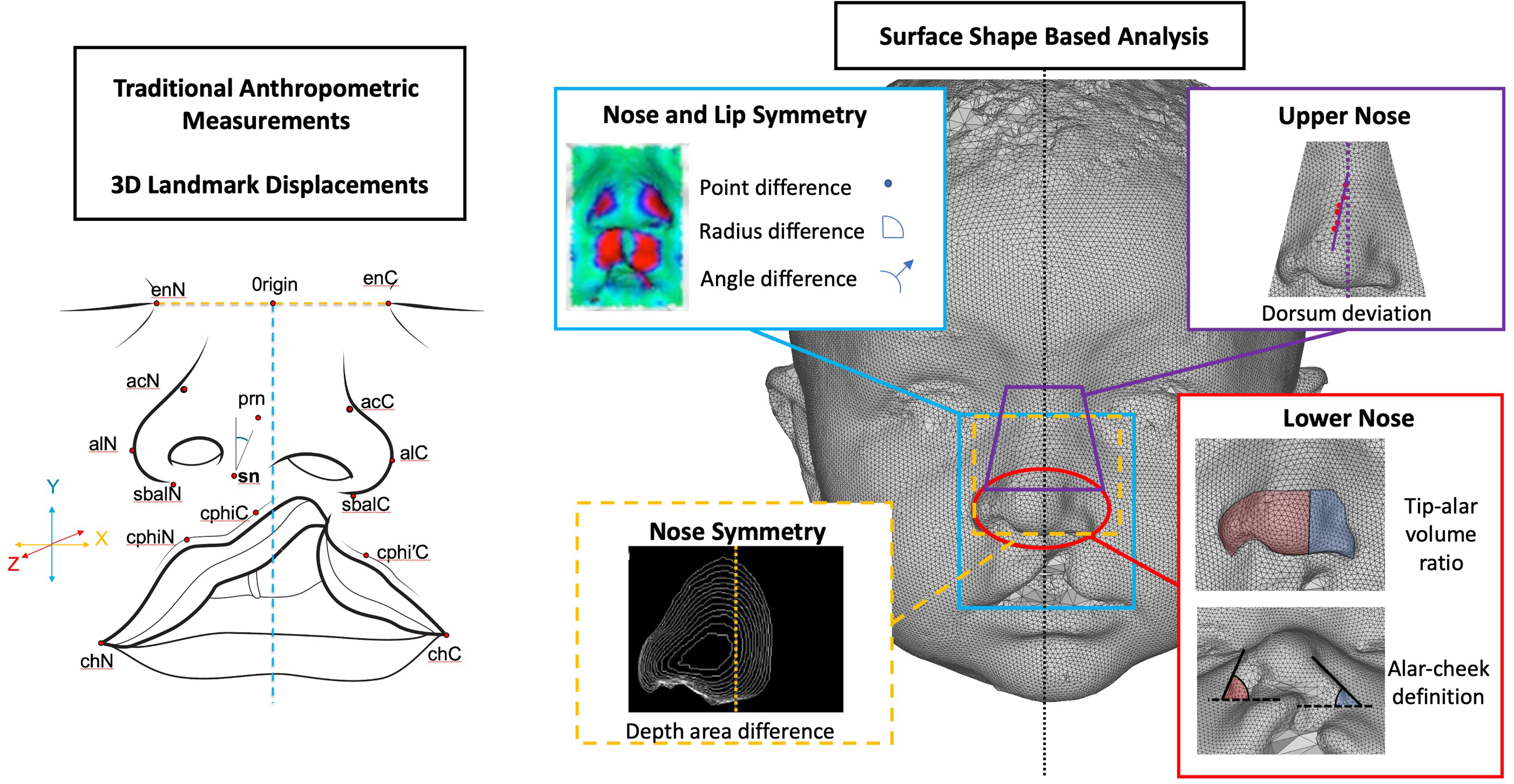
Objective measurements. (left) Traditional anthropometric analysis and 3D landmark displacements – Landmarks were placed on each image so that traditional anthropometric analysis could be performed (see the Supplemental Digital Content Table 1 for definitions). In order to track landmark displacements, images were normalized to inter-endocanthal midline and rotation (reverse Tanikawa rotation of 7.5 degree rotation from tr-sn line to define horizontal*) to define x, y, and z axes. Each landmark displacement was measured relative to the axis origin (mid endocanthion line) so that x, y, and z vector displacements for each landmark could be determined. * Tanikawa C, Takada K, van Aalst J, Trotman CA. Objective three-dimensional assessment of lip form in patients with repaired cleft lip. Cleft Palate Craniofac J. 2010;47:611–622. (right) Surface shape-based analysis of 3D images – Various methods to assess form were developed. Nose and lip symmetry could be quantified by point, radius, and surface normal angle differences. Nose symmetry could be quantified using depth maps to isolate the nose so that cumulative area differences across midline could be calculated. The upper nose was assessed using horizontal contour analysis to define the axis of greatest nasal dorsal prominence and its deviation from midline. The lower nose was assessed by comparing the difference in volume across midline and the difference in surface contours between cheek and ala. Other measurements were tested and have been previously described in the literature (but were not found to be as great in importance as these ones).
Analysis of Expert Rankings
For each of the image sets, individual inter-rater and intra-rater reliability was determined using Spearman's rank correlation (ρ, rho). Overall inter-rater reliability was estimated using Intra-class Correlation Coefficient. The individual rankings from surgeons were summed for each image to produce a rank sum score that would serve as the “gold standard”.
Analysis of Objective Measures
The correlation of objective measures with the subjective standard of severity was determined using Pearson correlation. Once objective measures with high correlation were determined, we performed multivariable linear regression analysis to determine which of the measures was the most predictive of the subjective severity. Outcome variable was surgeon rank sum score. A separate linear regression model was built for each set of measurements: anthropometric measurements, landmark displacements, surface shape-based analysis. Due to small sample size, five predictor variables from each set of objective measurements were used based on correlation analysis. All variables were centered and scaled prior to regression analysis. Model fits, correlation and regression coefficients and p-values were used to evaluate the effects. All analyses were run in R.
Results
Subjective Assessment of Clinical Severity
Inter-rater and intra-rater correlations were greater than 0.90 and intraclass correlation was 0.93 (P < .001) (Supplemental Digital Content Table 2). The mean severity rank could therefore be considered the consensus standard.
Objective Measures
(1) Traditional anthropometric analysis (Table 1)
Cleft nostril width, nostril width ratio, and columellar angle strongly correlated with subjective clinical severity of the uCLND (0.86, 0.80, 0.72). The lateral lip height ratio was similar in correlation (0.79); although it is not a nasal dimension it may be an indication of overall cleft severity or hypoplasia. Notably the medial lip height ratio, a measure that is commonly thought of as an indication of cleft severity had a weaker correlation (0.41).
(2) 3D landmark displacements (Table 1)
Lateral deviation of subnasale (sn) from midline (“sn_x”) had the strongest correlation (0.86). Lateral deviation of prolabium (Mid Cupid's bow, cphiN, cphiC) and non-cleft alar base (sbalN) from midline were also significant (0.73, 0.71, 0.64; and 0.69). The lateral deviation of other nasal landmarks overlying the greater segment but further from the premaxilla (acN, prn) were also associated with the severity standard (0.51, 0.51).
Posterior retrusion (z-axis) of cleft side landmarks overlying the lesser segment (sbalC, acC) was also associated with the severity standard (0.64, 0.56).
Landmark displacements along the vertical y-axis tended to have little correlation.
(3) Surface shape-based analysis (Table 1)
“Point” and “radius” difference measures of nasolabial symmetry had strong correlation (0.84 and 0.77). “Dorsum deviation” also had strong correlation (0.82). Other surface shape-based measures of nasal symmetry (“Depth area difference” and “Alar-tip volume ratio”) and normality (“PCA reconstruction”) were also highly correlated (0.73, 0.71, 0.72).
Correlation of Objective Measurement with Consensus Severity.
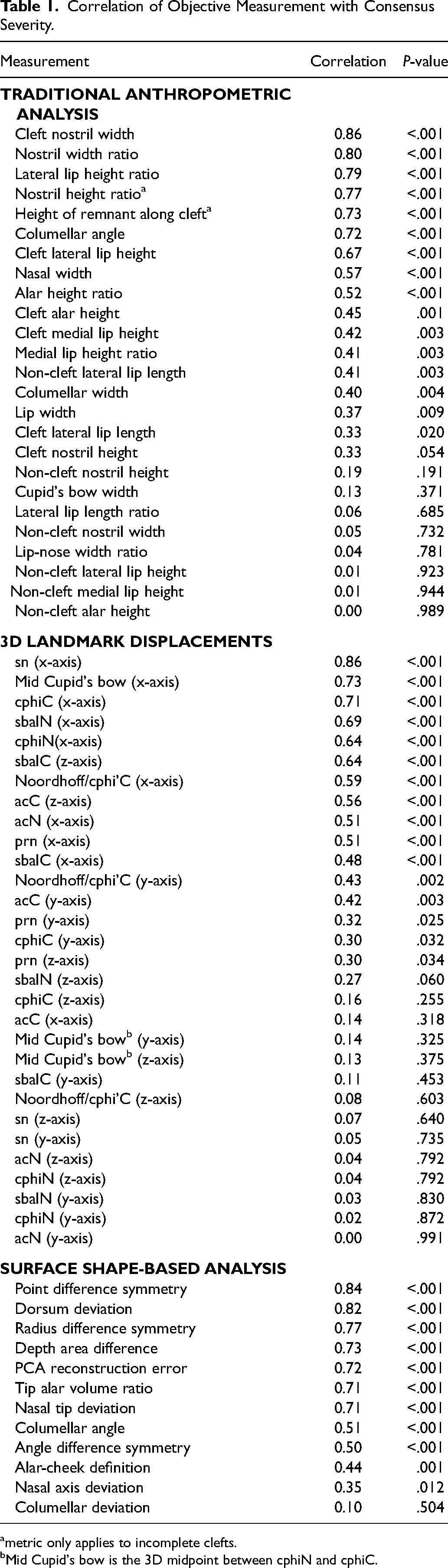
metric only applies to incomplete clefts.
Mid Cupid's bow is the 3D midpoint between cphiN and cphiC.
Multivariable Regression
Sn_x was the greatest predictor of clinical severity amongst landmark vectors, as well as anthropometric and shape-based measures, on multivariable regression analysis (Table 2).
Multivariate Analysis of Pre-Operative Objective Measures and Their Correlation with Subjective Rankings of Pre-Operative Severity.
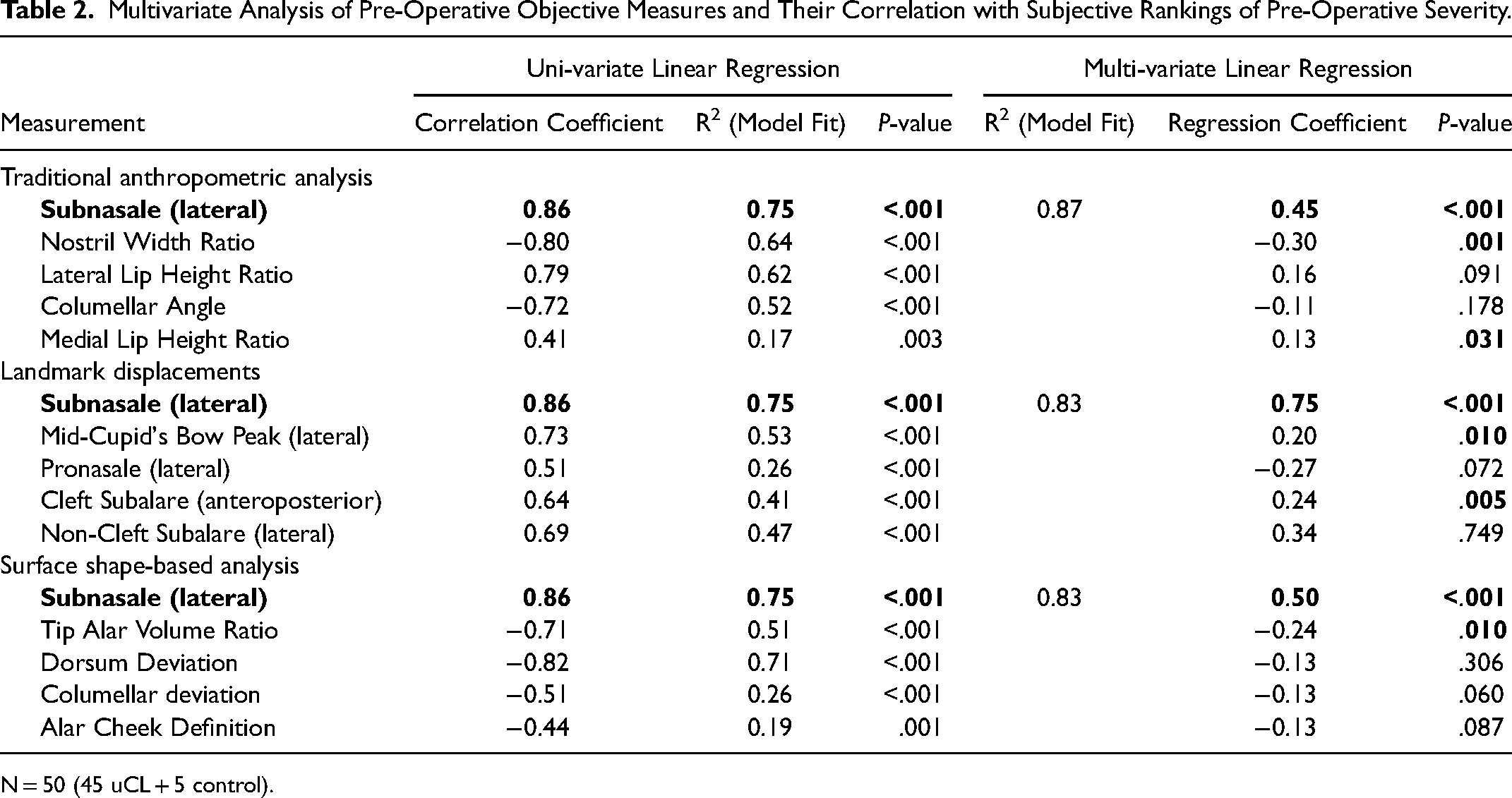
N = 50 (45 uCL + 5 control).
Discussion
Clinical assessment is qualitative and subjective whereas the measurements assessed were quantitative and objective.
Correction of the unilateral cleft lip nasal deformity remains a formidable challenge and there continues to be a lack of consensus in classification, treatment, and outcomes assessment. Defining severity is important as it may be a starting point for developing consensus, it is relatively simple in the absence of iatrogenic variations, it provides an initial metric for longitudinal care, and it likely impacts outcomes that can be achieved. Metrics to stratify severity would allow us to develop evidence-based practices and optimize treatment. Moreover, because these metrics define the specific anatomic derangements that explain the more general assessment of overall severity, they can provide new insights regarding the deformity (Figure 2).
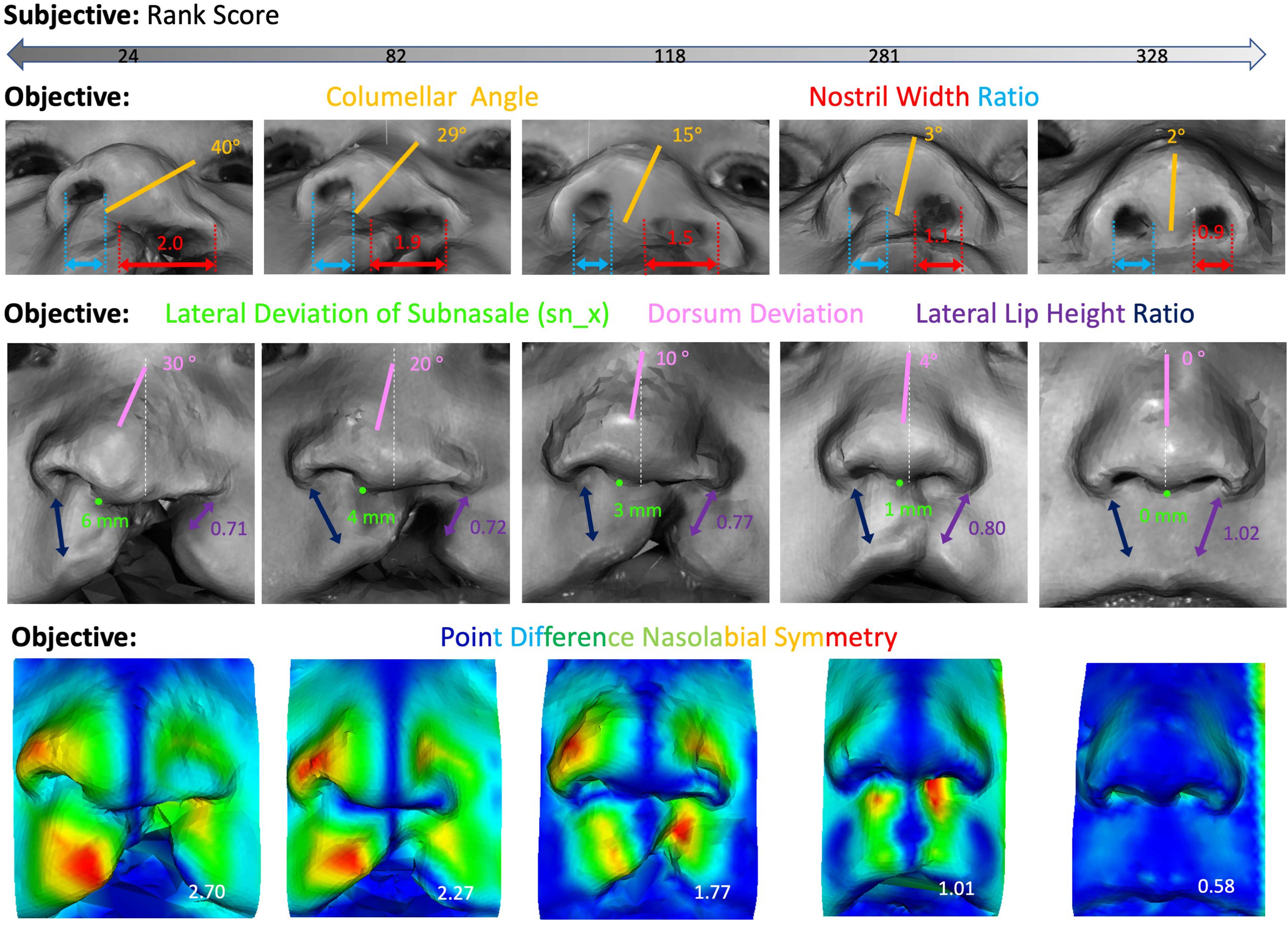
Objective measures with tight correlation with the subjective rank order standard of clinical severity. Lateral displacement of subnasale (sn_x) was the most important measure of severity and could be considered root cause of the other abberations as it reflects the uncoupled growth of premaxilla and degree of mesenchymal failure along the line of fusion. Amongst traditional anthropometric measures, columellar angle, nostril width ratio, and lateral lip height ratio were important. Most of the surface shape-based measurements of 3D form were important, however, dorsum deviation and point difference nasolabial symmetry had particularly tight correlation with the severity standard.
Classification vs Quantifiable Metrics
Patients with clefts can be categorized by “cleft type”. Although convenient, no classification is universally accepted, and distinctions can be arbitrary. For example, the difference between microform and incomplete cleft lip have been made based on both absolute dimensions 11 (which may change with patient age) and on the percentage of upper lip height involvement. 12 In addition, the distinction of a microform cleft from a “forme fruste”, “minimal”, and “occult” cleft is unclear. While Mulliken recently proposed thoughtful definitions for 3 types of “minor form” clefts, 11 the relationship and application of that system to historic definitions is difficult to translate. Another confusing distinction is that of an incomplete cleft lip and a complete cleft lip with soft tissue band (a.k.a. “Simonart”) because the terminology has been inconsistent, and the definitions have been disputed.13–15 While the presence of a complete cleft of the alveolus or absence of muscle tissue within the band have been used as distinguishing features, those details may not be readily available and may not reflect the underlying etiology or pathogenesis. Given that clefting is not an all-or-none entity, is governed by multiple factors, and seems to involve a continuous spectrum, an index that could account for variations within groups and across groups would better reflect the condition.
Fisher et al. previously recognized that patients with unrepaired unilateral clef lip nasal deformity present along a continuum and demonstrated that consecutive patients undergoing surgery could be sorted reliably into a progressive order of severity. 16 A similar study using 3D images found the same. 7 In both studies, the order of severity was not distinctly contained by the boundaries of the cleft type, further suggesting that historic classifications may not fully reflect the underlying pathogenesis. In both studies, several objective measures were identified that could be used to stratify severity and in turn, those indices may be a better reflection of an underlying pathogenesis.
Sn_x as a Potential Surrogate Measure of the Root Cause
Although columellar angle, nostril width ratio, and lateral lip height ratios are important measures of severity,7,16 in the present study we found that sn_x was of equal or greater value. This is not surprising given that uncoupled premaxillary growth drives the deformity during embryologic development. 17 As the premaxilla swings forward, upward, and outward, so do the anterior nasal spine and columellar base. The cleft alar base gets left behind and the orthogonal vectors of displacement result in a twisting collapse of the nose.18,19 In a study examining 3D morphology across the spectrum of presentation, columellar angle, nostril width ratio, and lateral lip height ratio changed in a dependent manner relative to sn_x. 3 Based upon that study and given that lateral deviation of subnsale (the surface landmark of the anterior nasal spine) could be considered a surrogate measure of the outward swing of the premaxilla, we hypothesize that sn_x could be a measure of the root cause of the other measured abberations.
Sn_x can also explain other important metrics identified in this study including dorsum deviation and the various surface shape-based measures of nasolabial symmetry. In a recent study that modeled the spectrum of deformity across 100 infants with unrepaired unilateral cleft lip, 3 columellar angle, nostril width ratio, and lateral lip height ratio changed in a dependent manner with increasing sn_x. That study included the full spectrum of presentation, from complete to incomplete and microform clefts, thereby confirming that sn_x is an important unifying index of cleft morphology.
The reason that sn_x may be applicable across all cleft types is that clefts originate from varying degrees of failed mesenchymal penetration. In complete clefts, the lack of fusion is apparent. However, in incomplete clefts the degree and extent of clefting under the surface tissues is not directly visible because the mesenchymal defect manifests as a lack of union of bone and muscle. Researchers have proposed that individuals with discontinuity of orbicularis detected on ultrasound should be considered a cleft phenotype. 20 Sn_x as a measure of mesenchymal severity follows. With varying degrees and extent of bony defects, the anterior nasal spine will swing away from midline, and the correlation of these can be seen at primary cleft lip repair when mobilizing mucoperiosteum for exposure to centralize the caudal septum. For example, in Figure 3 (above), the patient has an incomplete cleft lip with a minor notch in the gingiva. While many would classify the cleft as an isolated cleft lip, there is an incomplete union of bone along the site of fusion resulting in an incomplete “submucosal” alveolar cleft (Figure 3, below). That bony defect accounts for the shift of the anterior nasal spine and subnasale from midline. Similar mesenchymal defects likely explain why a given nasal deformity may appear significant despite a minor appearing defect of the lip. Sn_x could be a way to estimate “cleft width” in both patients with complete clefts and incomplete clefts (in which the mesenchymal defect is not readily apparent). Our current clinical classification schemes rely on examination of the external surfaces when the etiology involves mesenchymal defects. In the absence of advanced imaging, such as CT scan, to detect the underlying bony clefts, sn_x may provide a “window” that reflects the mesenchymal defect.
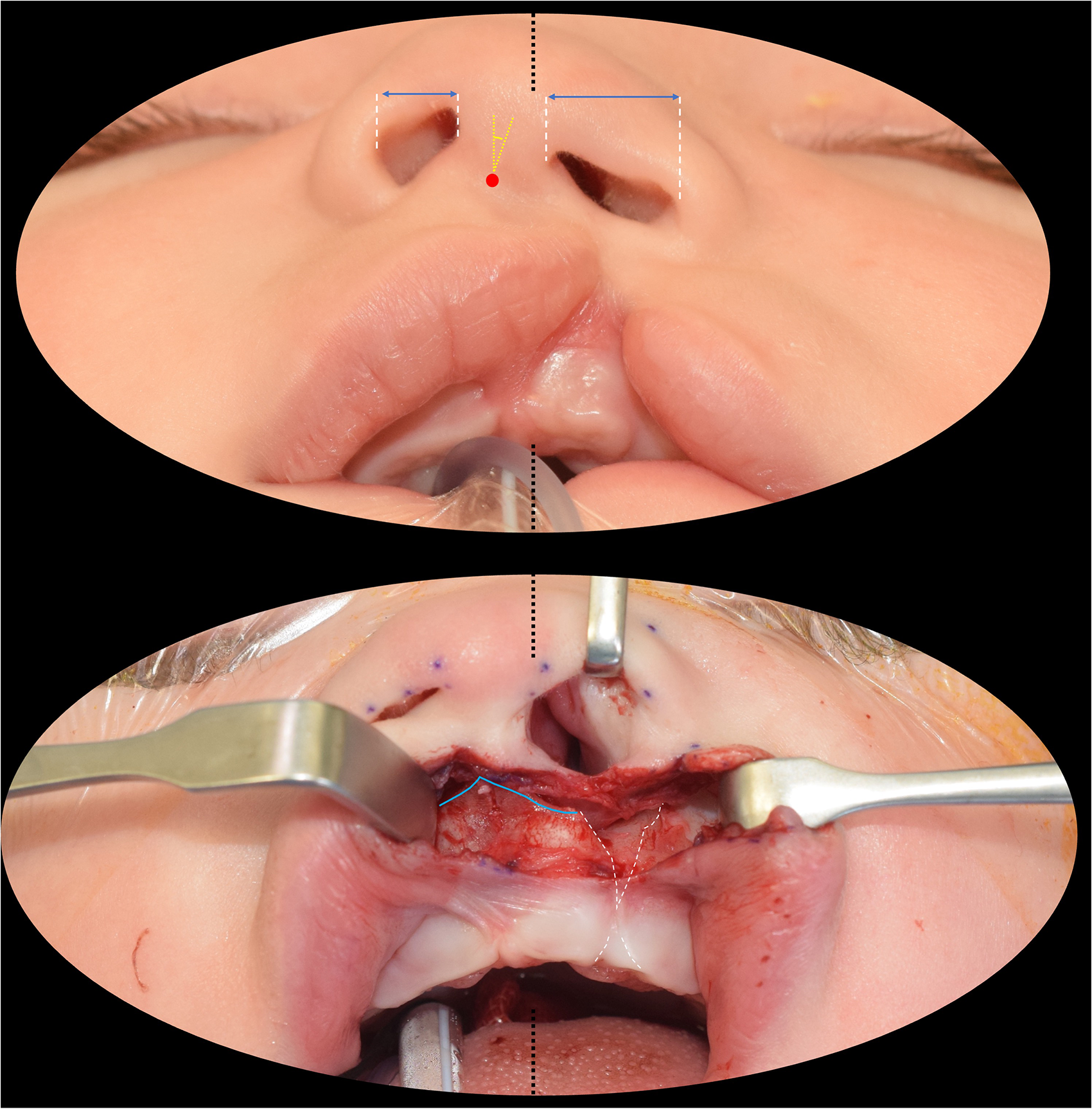
Mesenchymal defects as the etiology of the nasal deformity through the full spectrum of presentation. Although alveolar cleft width is often used as a measure of severity, it is not readily available in cases when the alveolar surface is intact. (above) In this example, which would normally be classified as an incomplete cleft lip, there are abberations of nostril width, columellar angle, and subnasale (red dot) in the absence of an obvious skeletal defect. (below) Upon exposure of the nasal floor for primary septoplasty the bony defect can be more fully appreciated. The submucosal cleft (white dotted lines) explains the outward rotation of the anterior nasal spine and premaxilla (blue) and is consistently present in a direct relation to the deviation of subnasale from midline. Sn_x could be considered a surrogate measure of cleft width when the bony defect is not readily available.
Clinical and Phenotypic Severity United
Whereas clinical severity is subjective in nature, basic science researchers seek objective ways to define phenotype when studying genetics, embryology, and dysmorphology. Sn_x provides a common metric that can be applied to both realms. In this study, it could be considered the “root cause” of the other measured aberrations. In previous studies, it was identified as the dependent variable when modeling the spectrum of presentation. 3 Sn_x is a simple, continuous, and quantitative measure of severity that, if applied in both realms, may provide opportunities for greater insights, correlations, and collaboration.
Documentation and Future Directions
Meticulous record keeping is a central tenet of cleft care and any reconstruction. 21 3D stereophotogrammetry is ideal as it captures form for immediate and later objective measure 1 and may become widely available as mobile technology evolves.22,23 Although important anthropometric measures have been identified10,16 and incorporated into documentation tools,24,25 sn_x should be documented for each repair as it is the single best correlative objective measure of severity. In the absence of 3D imaging, it can be measured directly by any surgeon in any setting (using a stick to mark the mid endocanthion line and a ruler to measure the distance of the mid columella to that midline). Without records of initial severity, we will not be able to compare outcomes of techniques and approaches and audit our craft over time.
In addition to traditional anthropometric analysis and 3D landmark tracking, in this study we used sophisticated computer vision techniques applied to 3D surface images to measure form. Although many of the indices were found to have tight correlation with the consensus clinical severity, such analysis currently requires 3D image capture and a computer science engineer. Ultimately, those indices were no better than sn_x or other traditional anthropometric measures in grading severity. Development of these more resource intensive approaches to morphology4–6 nonetheless still has value, as it may lead to better evaluation of post-operative appearance. We have previously found the normalization of anthropometric measurements is inadequate to differentiate post-operative appearances that are visible to human raters 26 and we are still working to develop and validate methods to objectively measure outcomes. Surgeons may find that correcting the major pre-operative abberations, such as sn_x relatively easy, whereas normalization of the more subtle deviations could be harder. The sum of the subtle residual deformities may dictate the quality of the post-operative result. In addition, whereas pre-operative appearance follows the single “dimension” of initial severity, post-operative appearance is the combination of multiple “dimensions” of initial severity, over-correction, under-correction, variations in healing, and iatrogenic alterations. Assessing the utility of objective measures in differentiating post-operative outcomes is the focus of further investigation and in those circumstances, the sophisticated computer vision analysis may have greater value.
Goals and Priorities of Treatment
Given that the most significant aberrations that define clinical severity should be the priorities of correction (Figure 4), the findings of this study can be used to verify treatment goals. Findings of this study confirm recent paradigms. 3
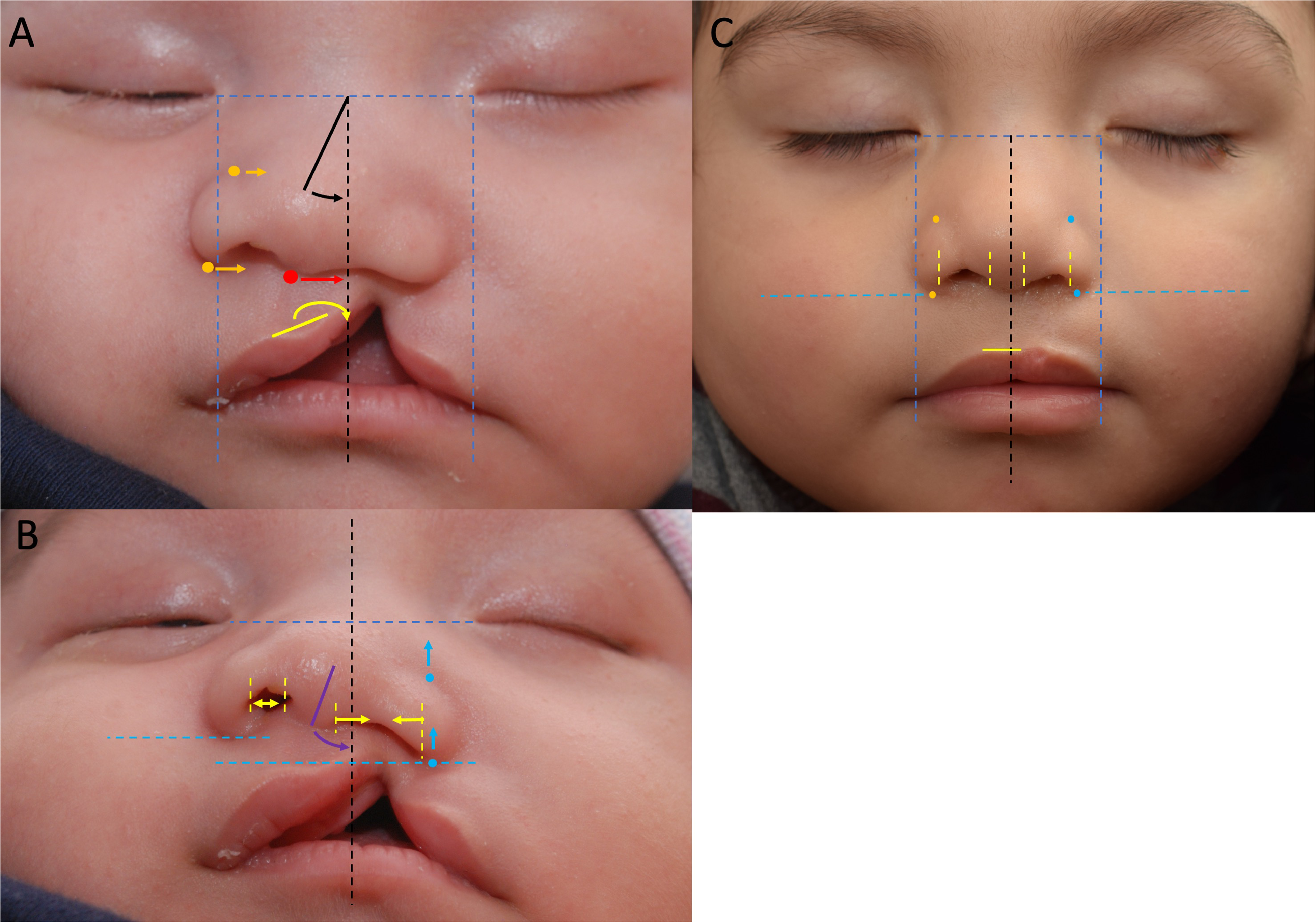
Treatment goals. Based upon objective analysis of the consensus standard, these should be primary goals of treatment. (A) Centralization of the columella (red) and prolabium (yellow); medial advancement of the non-cleft side ala (orange); and centralization of the nasal dorsum (black), moving it towards the midline and cleft. (B) Anterior advancement of the cleft side ala (blue), correction of columellar angulation (purple), narrowing of the cleft-side nostril width and widening of the non-cleft side nostril width (yellow). (C) Appearance 1 year after surgery with approximation of most objective measures to normal. Note that residual stigmata may not be captured by the key pre-operative objective measures.
Dogma dictates that treatment involves downward rotation of the prolabium and medial advancement of the cleft side alar base.27–32 Our findings indicate otherwise (Figure 4). Severity was defined by lateral deviation of the non-cleft side ala, prolabium, and columellar base (sbalN, cphiN, cphiC, sn); and retrusion of the cleft side ala (sbalC). Treatment goals should therefore be re-defined as: centralization of columella and prolabium; medial advancement of non-cleft side ala; and anterior advancement of cleft side.
Previous descriptions of uCLND have also described nasal dorsum deviation towards the cleft.33–36 We found the contrary. Dorsum deviation, one of the most important measures of severity, was in the opposite direction and was away from the cleft (Figure 4). Treatment goals should therefore be re-defined as: correction of nasal dorsum deviation from the non-cleft side to midline.
Given that severity was also defined by columellar angle and nostril width ratio, treatment priorities should also include: uprighting the columella and achieving nostrils of similar shape and dimension.
Techniques and approaches to achieve these goals are outside of the scope of this study, however, methods have been described that can produce those changes.10,37–39 As we accumulate more objective evidence, those and other methods can be refined.
Conclusions
Lateral deviation of subnasale from midline was the strongest objective measure of pre-operative severity. Sn_x may be a surrogate measure of cleft width or of a cleft related mesenchymal defect that can’t be readily visualized. Sn_x can be easily measured and should be considered a standard pre-operative measurement to collect and report. Consideration should also be given to using sn_x to stratify severity in basic and genetic studies so that clinical and research metrics can be aligned.
Assuming that key measures of severity in this study can be used to define goals of treatment, the following should be priorities: centralization of columella, nasal dorsum, and prolabium; medial advancement of the non-cleft side ala; anterior advancement of the cleft side ala; and equalization of nostril widths.
While this study has identified important objective measures of clinical severity, further studies are required to determine the utility of these measures in evaluating post-operative outcomes.
Supplemental Material
sj-tiff-1-cpc-10.1177_10556656231202173 - Supplemental material for Measuring the Unilateral Cleft Lip Nasal Deformity: Lateral Deviation of Subnasale Is a Clinical and Morphologic Index of Unrepaired Severity
Supplemental material, sj-tiff-1-cpc-10.1177_10556656231202173 for Measuring the Unilateral Cleft Lip Nasal Deformity: Lateral Deviation of Subnasale Is a Clinical and Morphologic Index of Unrepaired Severity by Raymond W. Tse, Thomas J. Sitzman, Alexander C. Allori, Russell E. Ettinger, David M. Fisher, Michael Bezuhly, Thomas D. Samson, Stephen P. Beals, Damir B. Matic and Ezgi Mercan in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231202173 - Supplemental material for Measuring the Unilateral Cleft Lip Nasal Deformity: Lateral Deviation of Subnasale Is a Clinical and Morphologic Index of Unrepaired Severity
Supplemental material, sj-docx-2-cpc-10.1177_10556656231202173 for Measuring the Unilateral Cleft Lip Nasal Deformity: Lateral Deviation of Subnasale Is a Clinical and Morphologic Index of Unrepaired Severity by Raymond W. Tse, Thomas J. Sitzman, Alexander C. Allori, Russell E. Ettinger, David M. Fisher, Michael Bezuhly, Thomas D. Samson, Stephen P. Beals, Damir B. Matic and Ezgi Mercan in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231202173 - Supplemental material for Measuring the Unilateral Cleft Lip Nasal Deformity: Lateral Deviation of Subnasale Is a Clinical and Morphologic Index of Unrepaired Severity
Supplemental material, sj-docx-3-cpc-10.1177_10556656231202173 for Measuring the Unilateral Cleft Lip Nasal Deformity: Lateral Deviation of Subnasale Is a Clinical and Morphologic Index of Unrepaired Severity by Raymond W. Tse, Thomas J. Sitzman, Alexander C. Allori, Russell E. Ettinger, David M. Fisher, Michael Bezuhly, Thomas D. Samson, Stephen P. Beals, Damir B. Matic and Ezgi Mercan in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Seattle Children's Hospital CCTR TRIPP fund; Seattle Children's Hospital CCTR Pediatric Pilot fund.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.