
Abstract
Objectives
The study aimed to comparatively assess the accuracy and retention of molding plates made of polyethylene terephthalate modified with glycol (PET-G) and polymethyl methacrylate (PMMA) materials, while also investigating the effect of adhesive addition on retention.
Design
A cross-sectional clinical study.
Patients/setting
The study included 30 infants diagnosed with non-syndromic cleft lip and palate (16 unilateral, 14 bilateral). Two molding plates were fabricated for each infant, and their accuracy and retention were evaluated. The data were analyzed using independent t-tests, Mann-Whitney U tests, and Wilcoxon rank tests.
Main outcome measures
Accuracy: The accuracy of the molding plates was assessed by measuring the virtual gap between the inner surface of the plates and their working cast using Exocad software. The accuracy was evaluated in different regions (anterior, middle, and posterior) and compared between PET-G and PMMA materials. Retention: The retention of the molding plates was measured using a digital force gauge, which recorded the force required to dislodge the plates from the infant's mouth. The retention was compared between PET-G and PMMA materials, as well as the effect of adhesive addition on retention. Overall adaptation; PET-G plates showed a significantly smaller gap (mean= 0.264 ±0.106) compared to PMMA (mean= 0.362 ±0.130). Region-specific adaptation: PET-G plates demonstrated better accuracy in all regions (means of anterior =0.246, middle =0.262, posterior =0.282 µm). Significant differences in accuracy were observed in the middle and posterior regions compared to PMMA. Retention assessment revealed that the PET-G groups (with or without adhesive) exhibited significantly higher retention compared to the PMMA groups (P<0.01).
Conclusion
PET-G plates demonstrated superior accuracy and retention compared to PMMA, with a significant difference observed in both accuracy and retention. Furthermore, the addition of denture adhesive had a positive effect on retention for both materials.
Introduction
Cleft lip and palate (CLP) are prevalent congenital malformations affecting the head and neck worldwide.1,2 From appearance to feeding, speech, psychological, and hearing problems, CLP can have a significant impact on a patient's quality of life.3,4 With a severity, ranging from a small notch in the lip to extensive defects in the roof of the mouth, CLP is a congenital malformation that requires attention and further understanding.5,6 The management of CLP involves a comprehensive and ongoing approach that begins during infancy and extends through adulthood, requiring a continuous and collaborative effort among multiple healthcare professionals. Since the 1950s, Presurgical Infant Orthopedics (PSIO) appliances have been utilized as a supplementary neonatal treatment for cleft lip and palate. 7 Their goal is to reduce defect size, simplify surgical procedures, minimize scarring, and approximate segments.4,8–11 Improving the baby's suckling function is crucial to avoid choking on milk and achieving adequate weight for surgery. 4
Although PSIO therapy has advantages, its use in CLP care is controversial as evidence does not support any long-term benefits.12–14 The cost, distance, and time required for treatment may hinder adherence to the protocol, and controlling alveolar segments presents a challenge. 14 A major concern is the considerable burden of care associated with the number of visits required, distance travelled for adjustments, visit duration, and the cost of treatment, which may reduce the likelihood of adhering to the treatment protocol.15–18
The PSIO is mainly fabricated from acrylic resin, which has been reported to be a causative factor of irritation, inflammation, and allergic responses of the oral mucosa.19–22 Intraoral soft tissue complications, such as mucosal ulceration, bleeding, fungal infections, and tissue irritation, are commonly observed.22,23 Additionally, the use of denture adhesive and tapes to improve retention may further complicate matters due to their possible cytotoxicity and irritating effects.9,23–25 To address the issue of conventional PSIO treatment dropouts, Al Khateeb et al. utilized thermoforming aligner material to create PSIO instead of acrylic resin. 22 Recently, 3D technologies have been used to successfully design and produce PSIO appliances. The goal of these techniques is to decrease the care burden, and simplify the process for both the clinician and the family of the infant.8,26–28
Proper retention of PSIO is crucial to exert the desired forces on alveolar segments and prevent the appliance from dislodging during feeding, which may cause tissue injury, milk aspiration into the nasal cavity, and prolonged treatment time.9,23 The present study was set out to compare the accuracy and retention of polyethylene terephthalate modified with glycol (PET-G) and polymethyl methacrylate (PMMA) materials. Additionally, the study aimed to assess the effect of adding adhesive on the retention of the appliance. The null hypothesis is that there is no significant difference in accuracy and retention between the two materials.
Material and Method
The study was approved by the ethical committee of the College of Dentistry, University of Baghdad, with reference number 613422. Thirty infants with non-syndromic cleft lip and palate, 16 with unilateral CLP, 14 bilateral CLP (age < 1year) were recruited to participate in the study at the Orthodontic Department, Faculty of Dentistry, University of Baghdad. The parents were informed about the treatment procedures, and informed consent was filled out by one of the parents before starting the treatment.
Sample Size Calculation
Sample size calculation was based on data from a pilot study performed on ten cases. The mean and standard deviation values for accuracy and retention were obtained using an independent sample t-test and setting the power at 85% and the type I error at 5%. A sample of 28 infants was required for the accuracy test (0.80 effect size), while 23 infants were required for the retention test (0.88 effect size). However, for the current study, a sample size of 30 infants was included, there were no dropouts reported as we completed the procedure on the same day.
Impression Procedures
To capture the intraoral cleft defect, a flanged acrylic tray was used to obtain an impression using fast set vinyl polyvinylsiloxane impression material (Prestige-Italy) (Figure 1). The impression was carefully taken without any sedation or anesthesia while the infant was awake. To ensure the accuracy, the impression should cover the anatomy of the upper gum pads, palatal shelves, and vestibular folds. Afterward, dental stone (Zhermack, Italy) was used to create a working cast from the impression, on the working cast the plates of both materials were fabricated.
Shows one of the special trays used for taking impressions.
Fabrication of the Experimental Orthopedic Appliances
On the stone cast, the cleft region of the palate was filled with stone to approximate the contour of palatal surface and to block out any deep undercuts in order to facilitate removal of appliance without damage of the working cast or the soft tissue of the infant's mouth. Two molding plates were made from each individual stone cast, one from a 2 mm layer of PET-G (Leone- Italy) and the other from PMMA (Orthocryl, Dentarum-Germany). To fabricate the PET-G plates, a vacuum form machine (Scheu Dental Biostar thermoforming unit-Germany) was used with a pressure of 6 bars. The PMMA plates were prepared using the adapting technique. The powder and monomer liquid were mixed in a clean porcelain jar in a ratio of 2.5 parts powder to 1 part liquid. Once the mixture reached the consistency of dough, it was promptly removed and adapted onto the model for each test. Then, it was manually molded to achieve the desired shape. Curing was carried out to complete the process.
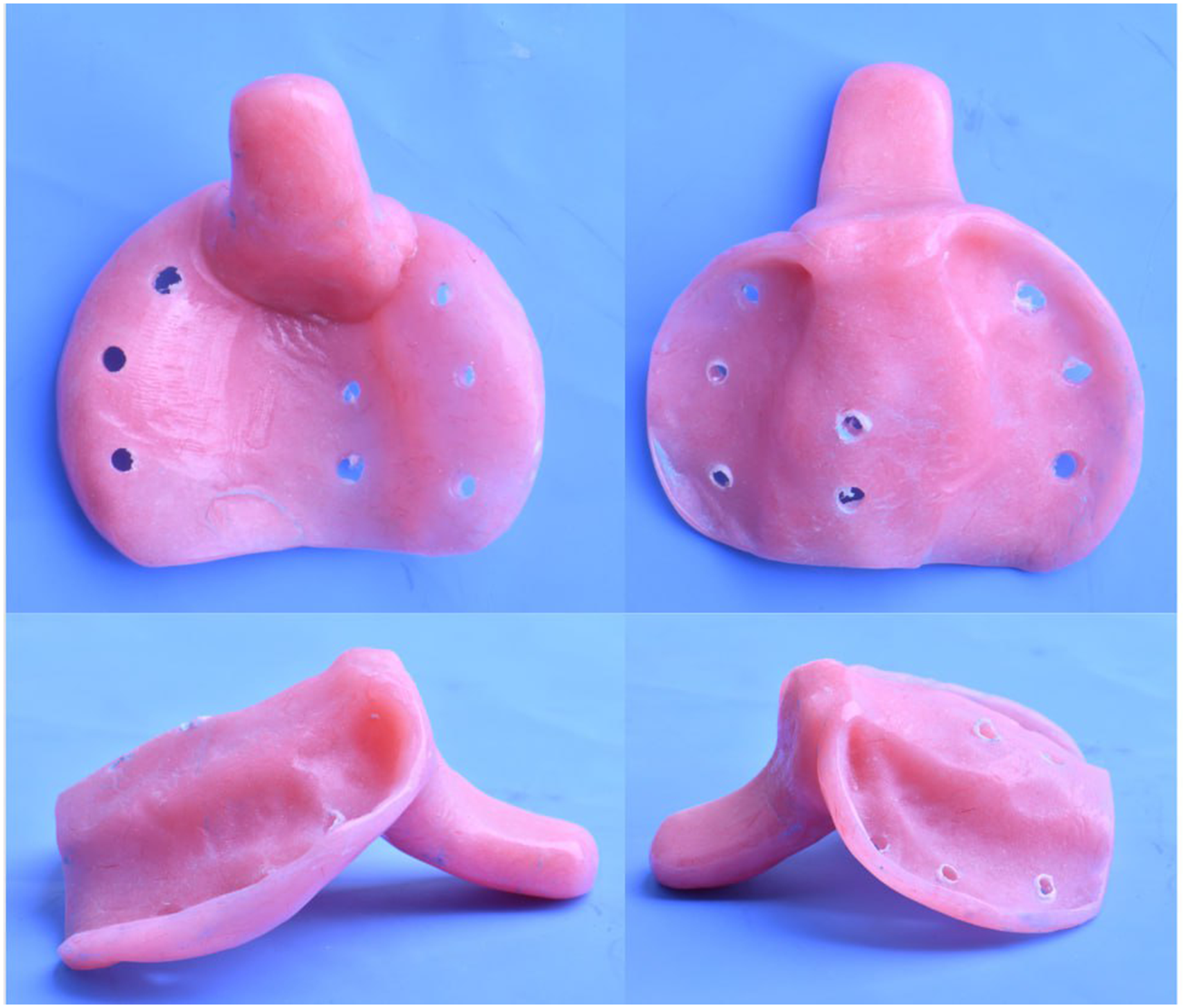
To finish the PMMA plates, acrylic burs were used to remove any acrylic flashes. Subsequently, the plates were finished using sandpaper with a grain size of 120 μm for 15 s. To prevent overheating, the specimens were cooled by immersing them in a rubber bowl filled with water for 15 s. Any rough borders or ridges of the PET-G plates were thoroughly finished with handpiece burs. Once finished, any rough areas were smoothed out, and a wire ligature was formed as a loop. Its end was fixed with cold cure acrylic at the outer surface of the palatal area and extending from the anterior alveolar ridge through the cleft area for each sample (Figure 2).

PSIOs fabricated from two different materials (PET-G, PMMA) with wire loops that act as attachments for the retention test.
Measurement of Retentive Force
The retention test was conducted immediately after creating the PSIO samples. Initially, both the PET-G and PMMA samples were tested without adhesive, followed by testing with adhesive (polygrip zinc-free denture adhesive cream, Ireland). The amount of denture adhesive was controlled using a serial plastic syringe and was placed on the mucosal side of the plates. The plates were then positioned in the infant's mouth with moderate finger pressure for 20 s (using stop watch from xiaomi smart band 7 pro/ China) to ensure even spreading of the adhesive over the entire mucosal surface of the experimental plate. All measurements were taken by the same clinician. After seating the plates with or without adhesive, the infant was allowed to suck normally for five minutes to facilitate tissue adaptation. To measure the retentive force in the patient's mouth, a digital force gauge (500 N Mxmoonfree digital force gauge, USA) with an accuracy of 0.1N was used to measure the dislodgement forces (Figure 3). The peak force required to separate the plate from its position was considered the retention force and was measured in newtons. The infants’ heads were positioned straight to place the Frankfort horizontal plane parallel to the floor. Three measurements were performed for each plate, with a one-minute waiting time after each measurement, and the average of the three measurements was taken as the retention value. 29

The digital force gauge used in the study.
Verification of PSIOs Adaptation
After mattifying the reflective surfaces with titanium oxide spray, the plates and casts were scanned by intraoral scanner (3Shape intraoral scanner). The scanned data was exported as STL file and by EXO CAD software (DentalCAD, Germany). These files were matched and aligned virtually (Figure 4). The gap (distance) between the inner surface of the plate and the cast was measured virtually at 18 points: nine for each side, three points for each of anterior, middle, and posterior regions. These points were identical between the PET-G and PMMA plates by making the points guide which was a copy of scan data of the working cast with the points on it. The points guide acted as a template to standardize the points location between the PET-G and PMMA for each case. Finally, the points guide matched with cast and the plates so the measurements were done at the same points for both plates (Figures 4,5).
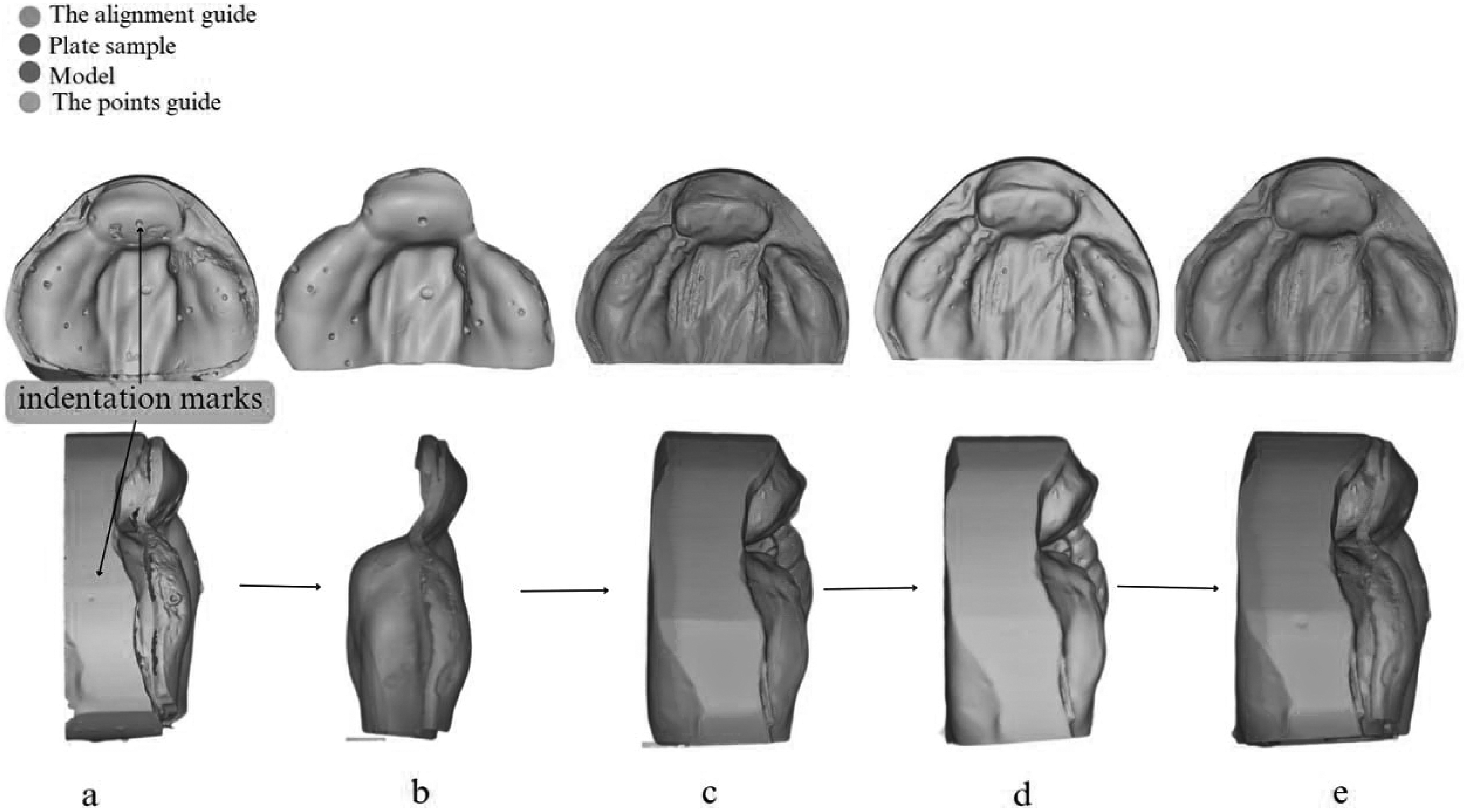
Represents the steps of the virtual setup:
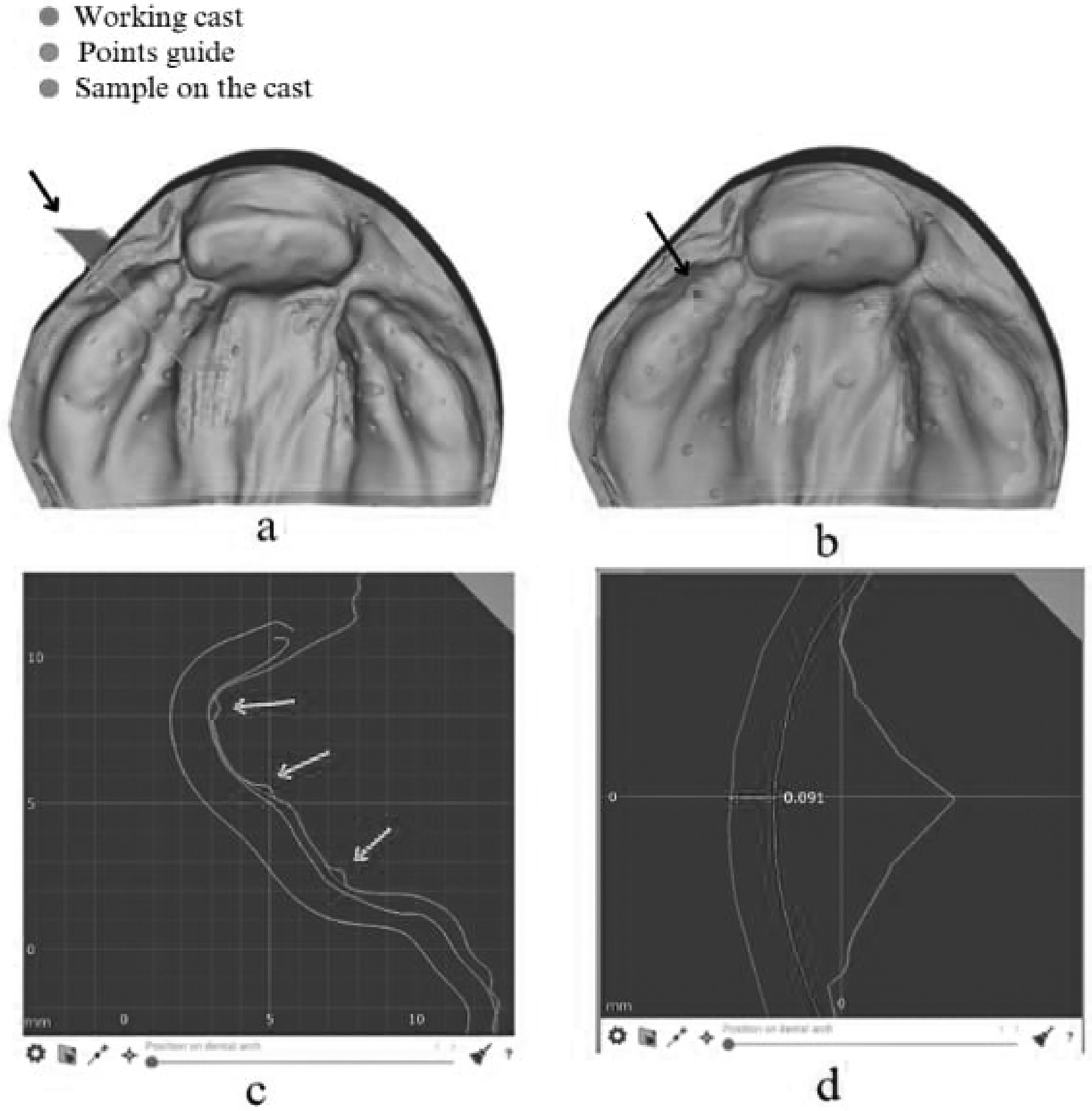
Describe the method of measurement:
Statistical Analysis
The collected data was analysed using SPSS version 25 (SPSS Inc., Chicago, Illinois, USA) to check for normality and homogeneity. A significance level for statistical tests was set at α =0.05, and α = 0.01 was set as the level of high statistical significance. Microsoft Excel software was used for data handling. The accuracy data was normally distributed, and the independent t-test was used to explore it. However, the retention test data was not normally distributed, so non-parametric tests such as Mann-Whitney U and Wilcoxon rank were used to analyse the retention data after checking the assumptions. The Mann-Whitney U test was used to compare the means of the PET-G and PMMA, while the Wilcoxon rank test was used to test the effect of adhesive addition within the same group.
Results
Overall Surface Adaptation
The independent t-test showed that PET-G superior to PMMA plates with minimum gap between the molding plate and the working cast (mean= 0.264 ± 0.106) in comparison to PMMA (mean= 0.362 ± 0.130), with a highly significant difference P value 0.002 (Table 1). Figure 6 explains the color maps of plates for one of the cases; the plate fabricated from PET-G had better adaptation (red to orange in the scale) with less purple areas. On the contrary, the plate of PMMA showed irregular surfaces with poor adaptation and more purple color, which represents zones of negative reading due to dimensional changes. Purple, green and blue colors are indicators of poor adaptation; purple refers to inward deviation, while the green and blue colors refer to outward deviations.
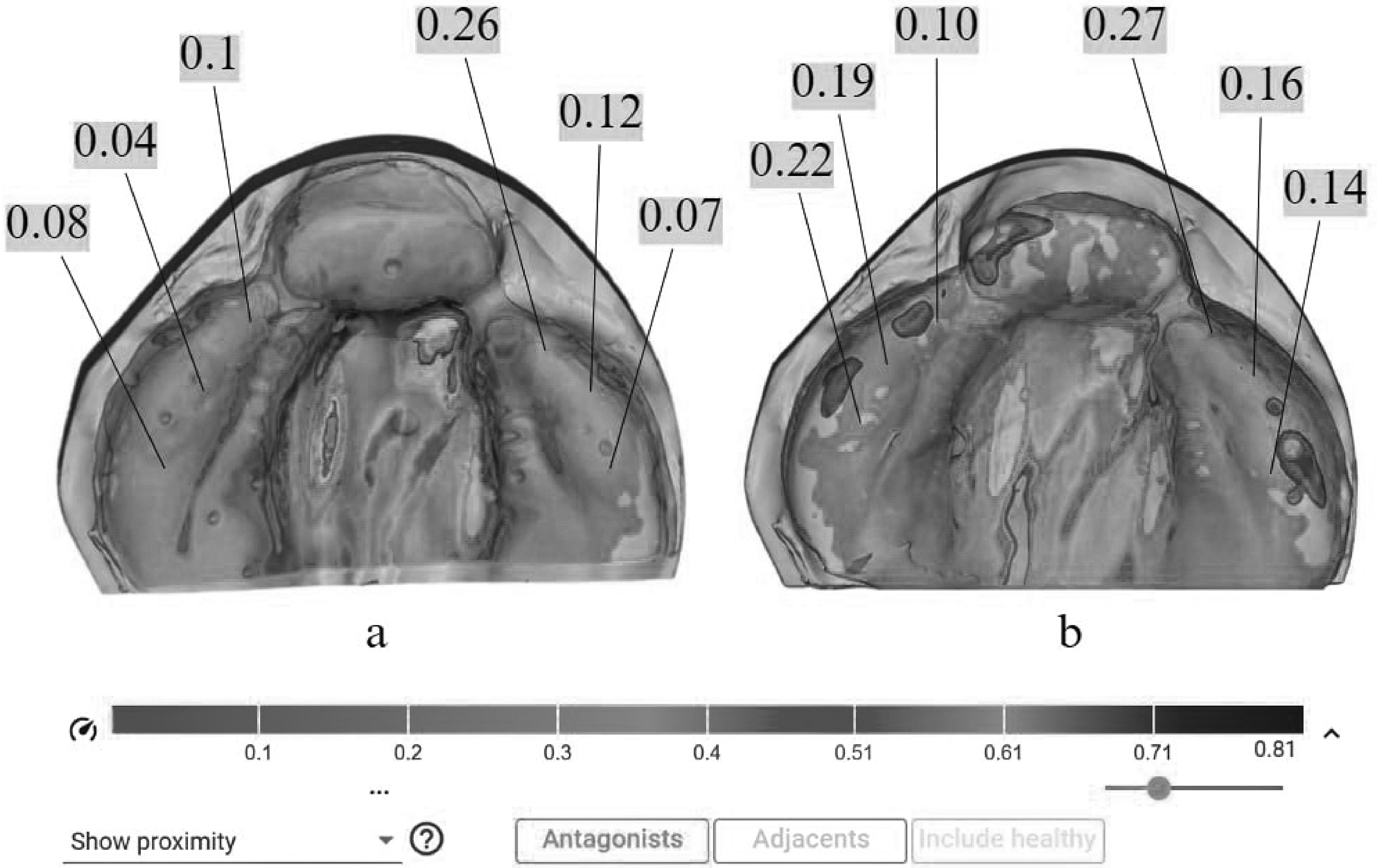
Color maps show the adaptation and measurement; (a) PET-G plate sample; (b) PMMA plate sample.
Data Analysis Between Hard Aligner and PMMA for Overall and Region-Specific Accuracy Using T-Independent Test.
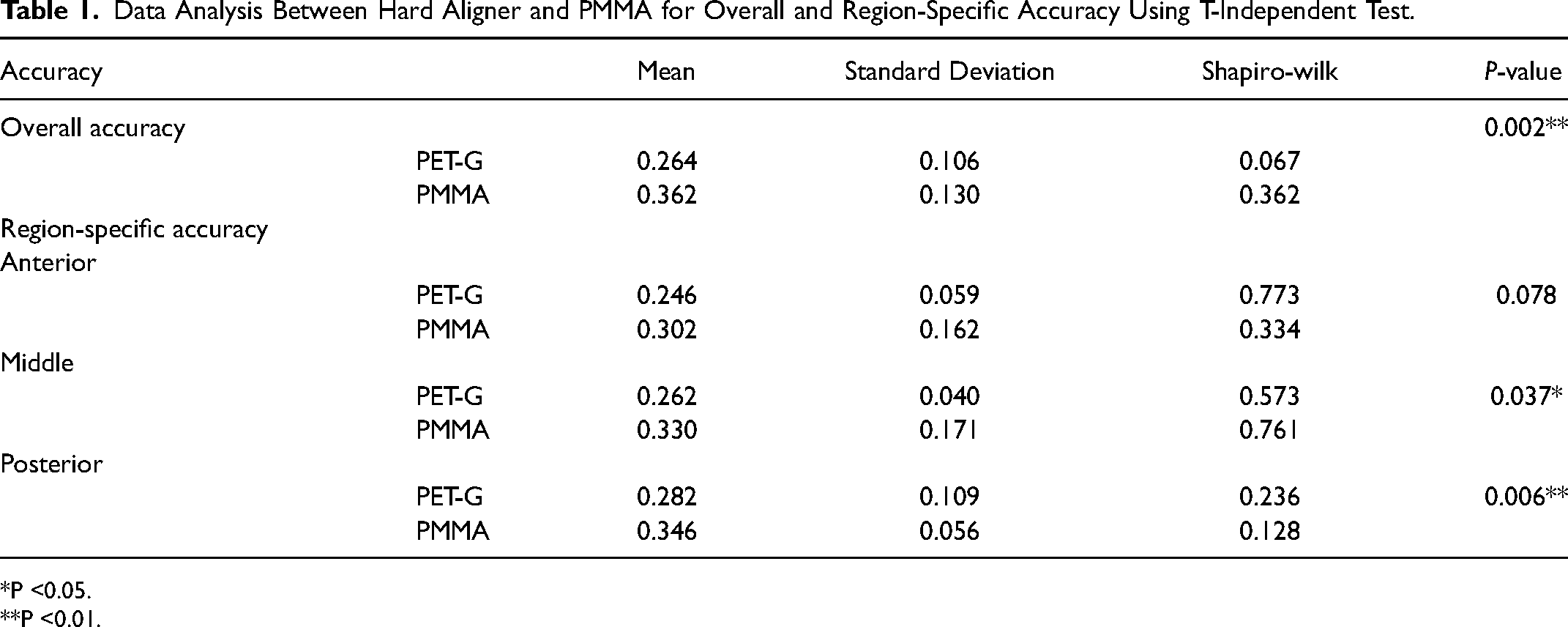
*P <0.05.
**P <0.01.
Region-Specific Misfit
The study divided the molding plate area into three regions (anterior, middle, and posterior) and assessed the accuracy of the PET-G and PMMA at six points for each region (three right and three left). The results showed that the PET-G had better accuracy than PMMA in all regions, with mean deviations of 0.246 mm in the anterior, 0.262 mm in the middle, and 0.282 mm in the posterior region. The best outcomes were observed in the anterior region for both materials, while the greatest misfit was found in the posterior region for both PET-G and PMMA. The t-test analysis showed no significant difference in the anterior region between the two materials (P = 0.078), a significant difference in the middle region (P = 0.037), and a highly significant difference in the posterior region (P = 0.006) (Table 1).
Retention Test Results
The Mann-Whitney U test revealed that the retention force was significantly higher in the PET-G groups, both with and without adhesive, when compared to the PMMA groups (P < 0.01). In the adhesive groups, the median retention force was 2.167 N (n = 30) for PET-G and 1.050 N (n = 30) for PMMA. In the non-adhesive groups, the median retention force was 0.950 N (n = 30) for PET-G and 0.550 N (n = 30) for PMMA. No significant difference (P = 0.976) was found between PET-G (without adhesive) and PMMA (with adhesive). The results from the Wilcoxon rank test show that the addition of denture adhesive had a positive effect on retention force for both materials, with a significant difference (P value < 0.01, effect size r=0.87). The results are summarized in Tables 2 and 3.
Descriptive Statistics of Retention Test for PET-G and PMMA with and Without Adhesives.

**P <0.01.
Statistical Analysis of Retention Test for PET-G and PMMA; with and Without Adhesive.
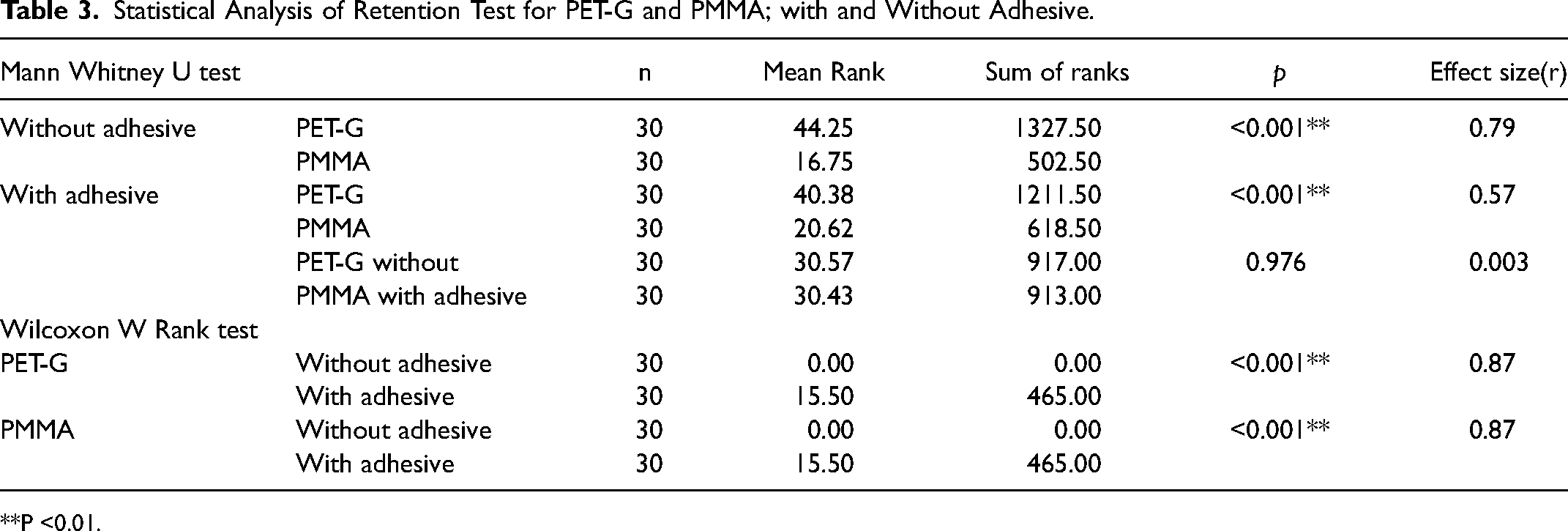
**P <0.01.
Discussion
The present study set out primarily to assess which material is the best to be used as PSIO considering two physical properties (accuracy and retention). The second objective was to investigate the effect of adding denture adhesive as adjunctive to increase the retention of the PSIO.
PSIO had been widely used as first step during treatment of clefted babies to realign and approximate the cleft segments before lip surgery. 30 Any successful orthodontic or orthopedic treatment depends on wearing time, so the PSIO should be well fitted and retentive to increase the active time. 9
The retention of the PSIO is crucial to apply the optimum forces that move the alveolar segments and to prevent the PSIO falling from the infant's mouth and mobility during feeding, which could cause tissue laceration and escape of milk into the nasal cavity.4,9,23 Although PMMA is commonly used for PSIO fabrication, multiple drawbacks related to PMMA usage had been counted such as dimensional instability, ulceration-causing rough surfaces, bacterial accumulation, monomer-induced inflammatory reactions, and time-consuming fabrication and activation processes.20–22,31,32
Recently, Al Khateeb et al. used the vacuum form aligner on stone cast and did the activation by adding and removing layers from the stone cast, while other researcher made a series of plates made from thermo-formed aligner on a scale of 3D printed models.28,33,34 While, Al ghafour focused on virtual activation with printing appliances using light curable acrylic resin. 35
PET-G material showed excellent transparency, adequate flow property, and resistance against various solvents which can be either printed or hot stamped. PET-G materials are exceptionally durable, have high impact strength, are resistant to chemical changes and are materials of choice for the fabrication of complex and intricate designs. 36 The retention depends on many factors; the close adaptation (accuracy) of the plate is one of the main factors. 37 Dimensional stability and accuracy of the molding plates will lead to intimate adaptation to the oral tissues that will result in better accuracy and retention.38,39 Al Khateeb et al. state that vacuum formed PSIO more efficient in approximation of alveolar cleft segments than the conventional PSIO. 22
The result of the present study had revealed that the PET-G material significantly showed the best accuracy and retention and a significant improvement in retention after adding denture adhesive. The most likely causes are, better dimensional stability of the aligners’ plates after setting, and better adaptation to the cast configuration comparing to PMMA plates. PMMA plates showed inward deviation as shown in the color map (Figure 6), which may cause pressure spots and irritation.
Some clinicians use denture adhesive to increase the retention. A positive effect was found from the addition of adhesive on retention of PSIO with valuable effect size, but still there are complications related to adhesives usage, such as zinc cytotoxic effect, difficult to clean from the plates, and smothering during cleaning the infant's mouth.24,35 The result of the present study showed not a remarkable difference between the PET-G (without adhesive) group and PMMA (with adhesive) group; it is advisable to abandon the usage of adhesive when retention is accepted.
Conclusion
The study found that PET-G plates showed better adaptation and minimal gap compared to PMMA, resulting in superior retention. The use of denture adhesive significantly improved retention for both materials. PET-G may be a better option for PSIO treatment in infants due to their higher accuracy and stability. Overall, this study provides valuable insights into the use of appropriate materials and techniques for PSIO treatment. However, further research is needed to evaluate the long-term effects of denture adhesive use in pediatric patients.
Footnotes
Disclosure Statement
The manuscript has been read and approved by all the authors. The requirements for authorship have been met, and each author believes that the manuscript represents honest work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.