
Abstract
Objective
To predict the morbidity of sagittal suturectomy using preoperative computer tomographic measurement of frontal and parietal bone thickness in osteotomy sites.
Design
Retrospective analysis.
Setting
Tertiary children's hospital.
Patients
Fifty infants with nonsyndromic, isolated sagittal craniosynostosis who underwent extended sagittal suturectomy from 2015–2022.
Methods
Mean thickness of the frontal and parietal bone in regions of osteotomies were determined for each patient from preoperative CT images obtained within 30 days prior to suturectomy. The relationship between bone thickness (mm) and estimated blood loss (mL) was evaluated using Spearman's correlation and a multivariable model that adjusted for patient weight and surgery duration. The association between bone thickness and perioperative blood transfusion was evaluated using a multivariable logistic model controlling for patient weight and surgery duration.
Main Outcome Measures
Estimated blood loss, perioperative blood transfusion.
Results
Frontal and parietal bone thickness in the region of osteotomies were positively correlated with estimated blood loss (p < 0.01). After adjusting for patient weight and duration of operation, both parietal and frontal bone thickness were associated with intraoperative blood loss (R2 = 0.292, p = 0.002 and R2 = 0.216, p = 0.026). Thicker frontal and parietal bone in the line of osteotomies resulted in significantly higher odds of blood transfusion. Bone thickness in the line of parietal osteotomies was 76% accurate at identifying patients who would require blood transfusion (p = 0.004).
Conclusions
Frontal and parietal bone thickness in the line of osteotomies is associated with blood loss and perioperative blood transfusion for sagittal suturectomy operations.
Keywords
Introduction
Isolated sagittal craniosynostosis, or the premature closure of the sagittal suture, is the most common manifestation of craniosynostosis, particularly among patients without a craniosynostosis-associated syndrome.1–4 Surgical intervention is essential to increase intracranial/orbital volume, prevent elevated intracranial pressure, ensure proper visual, neurological, and cognitive functioning, and promote aesthetics.5,6 Over the past two decades, minimally invasive surgical approaches to manage isolated sagittal craniosynostosis have become more prevalent due to their lower morbidity and operative time compared to open approaches.7–9 These minimally invasive approaches combine sagittal suturectomy with directed postoperative growth, usually through a postoperative orthotic molding band.
Substantial blood loss and the need for transfusion are significant risks of suturectomy. 10 The morbidity of sagittal suturectomy has been widely studied throughout the literature and varies by institution based on intraoperative protocols, with a mean estimated blood loss ranging from 30–70 mL and the likelihood of blood transfusion ranging from 1–100%.11–13 Given these risks, it remains paramount to investigate ways to identify patients at higher risk for increased morbidity so surgical teams can prepare preoperatively and better inform families of surgical risk during their preoperative consultation.
Many researchers have analyzed how the duration of operation and patient age/weight can be utilized to predict the perioperative morbidity of craniosynostosis surgery. These models suggest that lower patient weight and longer duration of operation both correlate with increased blood loss, higher probability of transfusion, and a longer postoperative length of stay. 13 In a novel study analyzing spring-mediated cranioplasty for sagittal synostosis, researchers found that increased parietal bone thickness was a significant predictor for increased blood loss and probability of transfusion. 14 However, that study did not control for confounding factors such as tranexamic acid (TXA), thus limiting the strength of the conclusions. Given that the primary source of blood loss intraoperatively during sagittal suturectomy is a steady “ooze” from bone cuts throughout the operation, surgical morbidity may have a significant relationship to bone thickness in the region of the osteotomies. 13 To our knowledge, no study in the literature has evaluated the ability of bone thickness to predict the morbidity of extended sagittal suturectomy. This study aims to use preoperative computed tomographic (CT) measurement of frontal and parietal bone thickness in the region of osteotomies to identify patients with a higher likelihood of increased blood loss and odds of transfusion during extended suturectomy for patients diagnosed with isolated, nonsyndromic sagittal craniosynostosis.
Methods
This retrospective study was IRB approved prior to data collection. Inclusion criteria were: (1) diagnosis of isolated, non-syndromic sagittal craniosynostosis, (2) history of an extended sagittal suturectomy at our institution from 2015 to 2022, (3) adherence to our institutional anemia management protocol (described below), including preoperative bolus and intraoperative infusion of tranexamic acid (TXA), and (4) preoperative head CT obtained within 30 days prior to suturectomy and available for review. Children diagnosed with a craniosynostosis syndrome or those with a history of a prior craniosynostosis surgery were excluded. In total, 50 patients met all the inclusion criteria (n = 50).
Extended Sagittal Suturectomy
At this institution, patients clinically diagnosed with craniosynostosis routinely undergo preoperative head CT imaging without contrast to confirm their diagnosis of sagittal synostosis, evaluate the brain, and for surgical planning regarding the anatomy of the relationship of the sagittal sinus to the overlying bone. CT imaging was not conducted for the purpose of this study. All patients in the study underwent sagittal suturectomy with parietal bone wedge resections, parietal bone micro-fracturing, and frontal bone-releasing osteotomies across the coronal sutures. All operations were jointly performed by a craniofacial surgeon, a pediatric neurosurgeon, and a pediatric anesthesiologist. In brief, the scalp was infiltrated with local anesthetic containing epinephrine. Two incisions were made in the scalp for access to the calvarium: a 3 cm coronal incision posterior to the anterior fontanelle, and a 3 cm sagittal incision anterior to the lambdoid suture. A rectangular piece of calvarial bone containing the sagittal suture was excised using burr holes and a craniotome with a footplate. The sagittal suturectomy was then extended with a double action flat-head rongeur to a width of approximately 4–6 cm, dependent on patient anatomy and preoperative cephalic index. In total, a rectangular piece of bone was resected from the anterior fontanelle to the junction of the sagittal suture with the lambdoid sutures. Hemostasis was maintained with bipolar electrocautery on the dura and monopolar cautery with bone wax on the bone edges throughout the operation. Floseal was used throughout the procedure immediately following use of the above local agents for further hemostasis. Bilateral wedge resections of parietal bone were performed posterior to the coronal suture and anterior to the lambdoid suture at a width dependent on patient anatomy. Frontal-releasing osteotomies were also made across the coronal sutures adjacent to the sphenoid wing to release temporal constraint. Finally, bone-bending rongeurs were used to create micro-fractures in the parietal bone to increase bone pliability and responsiveness to postoperative banding. See Figure 1 for an approximation of the osteotomies made. All patients were discharged to the PICU for monitoring with continuation of a TXA infusion for four hours post-surgery at a rate of 5 mg/kg/hr. Patients were then fitted for a cranial molding orthotic 7–14 days after surgery.
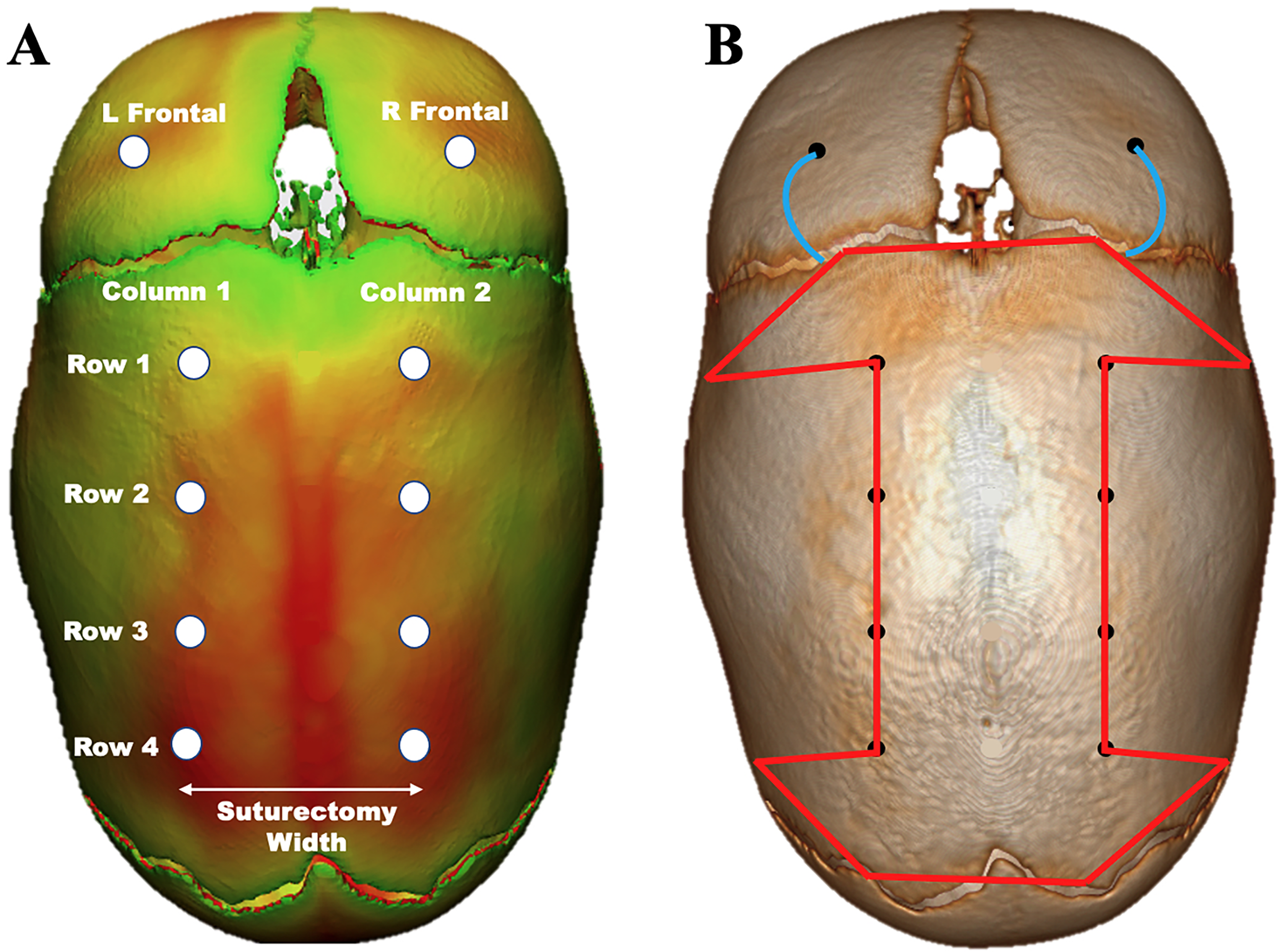
3D CT scan of a patient with isolated sagittal craniosynostosis. A: Bone thickness heat map with the eight parietal bone thickness locations and two frontal bone thickness locations measured. Darker coloration represents regions of increased bone thickness. B: Locations of osteotomies relative to the 10 areas of thickness measured. Lines in the parietal region indicate areas of bone cuts/resection and lines in the frontal bone region indicate frontal releasing osteotomies (no bone removal).
Anemia Management
All patients received the same standardized perioperative anemia management protocol. Blood was available in the operating room during all craniosynostosis surgical operations given the benefits of transfusing in a timely manner when transfusion is necessary. Patients received a 10 mg/kg IV bolus of TXA at the time of surgical prep in the operating room and a continuous 5 mg/kg/hr TXA infusion intraoperatively and for four hours postoperatively to decrease blood loss and the likelihood of transfusion.15–17 No operations included the use of a cell-saver or preoperative erythropoietin. The need for blood transfusion was carefully monitored throughout the procedure by the involved craniofacial surgeon, neurosurgeon, and pediatric anesthesiologist. All transfusions adhered to standardized craniosynostosis pathway transfusion criteria and were carefully discussed jointly by the surgical team and anesthesiologist. Blood transfusion was considered if acute blood loss resulted in an estimated blood loss greater than 10% of total blood volume and/or for symptoms consistent with inadequate perfusion and oxygenation. Indication for blood transfusion was also carefully monitored postoperatively following transfer to the PICU based on postoperative hemoglobin and/or for symptoms of inadequate perfusion and oxygenation. Preoperative and postoperative hemoglobin were monitored with complete blood counts (CBC) and arterial blood gas (ABG) and utilized during transfusion decision making. Transfusions were given if the hemoglobin was found to be 5 g/dL or lower. For patients with a hemoglobin of 5–7 g/dL, transfusions were given if the patient had symptoms of inadequate perfusion and oxygenation.
Collection of Outcome Measures and Covariates
Data was collected from plastic surgery and neurosurgical operative notes, progress notes, and anesthesia records. Patient demographics were collected including patient age and weight at the time of surgery, diagnosis, and comorbidities. Perioperative variables included the duration of operation, incidence of blood transfusion, intraoperative blood loss, hospital length of stay, and the width of the sagittal suturectomy.
Bone Thickness Measurements
Preoperative head CT scans without contrast completed within 30 days of surgery were uploaded to Materialise Mimics 25.0 (Materialise, Leuven, Belgium) for generation of three-dimensional maps. These renderings were then imported to Materialise-3-Matic 17.0 (Materialise, Leuven, Belgium) for bone thickness measurements in the parietal and frontal bone. Bone thickness calculations were made with the thickness function within the Materialise program at eight distinct points in the parietal region in the area of parietal osteotomies and two points in the frontal bone in the area of frontal releasing osteotomies (Figure 1). In the anteroposterior direction, bone thickness was determined 1 cm posterior to the coronal suture (row 1) and 1 cm anterior to the lambdoid suture (row 4). Thickness was also analyzed at locations equally spaced between the anterior and posterior measurements (rows 2 and 3). All parietal bone thickness measurements were located at the lateral-most aspects of the suturectomy to assess osteotomy sites (columns 1 and 2). Bilateral spot measurements of each frontal bone in the region of frontal releasing osteotomy were taken 10 mm anterior to the coronal suture and 5 mm lateral to the lateral-most aspect of the parietal bone suturectomy line which are in the region of frontal releasing osteotomies (see Figure 1). All thickness measurements were collected one time by the same pediatric neuroradiologist.
The mean bone thickness in the parietal region at the site of parietal osteotomies was calculated for each patient by averaging the thickness of all eight points in the parietal bone (columns 1 and 2). The mean bone thickness in the frontal region at the site of frontal releasing osteotomies was calculated for each patient by averaging the thickness of the left and right spot measurements of the frontal bone.
Statistical Analysis
All statistical analyses were performed using JASP 0.17.1 for Mac (JASP, Amsterdam, Netherlands). 18 Demographic data was analyzed with standard descriptive statistics. The relationship between bone thickness and intraoperative estimated blood loss was compared via Spearman's rank correlation coefficients. The relationship between bone thickness and blood loss was assessed with a multivariable linear regression model controlling for patient weight and the duration of operation. The impact of bone thickness on blood loss was determined from the linear regression model. The association between bone thickness and transfusion was assessed via a multivariable logistic regression model controlling for patient weight and duration of operation. The accuracy of the logistic model was analyzed using a confusion matrix with a prediction cut-off value set to 50% probability of blood transfusion. The bone thickness in the transfusion and non-transfusion groups was evaluated using a Mann-Whitney U test.
Results
In total, 50 patients with isolated, nonsyndromic sagittal craniosynostosis underwent sagittal suturectomy between 2015–2022 and met all inclusion criteria (Table 1). The mean age at the time of suturectomy was 3.72 months with a mean weight of 6.5 kg (Table 1). Most of the cohort was male (78%; n = 39), while 22% (n = 11) was female. The mean operative duration was 73 min, measured as the time between the first incision and the patient's emergence from anesthesia. Twenty-seven patients received a blood transfusion (54%) and had a mean weight-adjusted blood loss of 12 mL/kg. Twenty-five patients received a transfusion intraoperatively (50%) and two patients (4%) received a postoperative transfusion while in the PICU. For patients who required a transfusion, the mean transfusion volume was 21.8 mL/kg of packed red blood cells. No patients in the cohort received fresh frozen plasma (FFP) or platelets. The mean width of the sagittal suturectomy was 54 mm with a range of 30–70 mm. The mean postoperative length of stay, measured as the number of nights spent in the hospital, was 1.7 days, with a range of 1 to 4 days. One patient sustained an intraoperative dural injury which was repaired with a piece of DurepairTM without postoperative cerebrospinal fluid (CSF) leakage. Additionally, one patient was readmitted to the hospital for subgaleal hematomas in the biparietal and occipital region which were stable and did not require surgical intervention. No patients sustained any major intraoperative complications or underwent additional craniosynostosis surgery during their respective follow-up at our institution.
Cohort Demographics & Perioperative Outcomes.
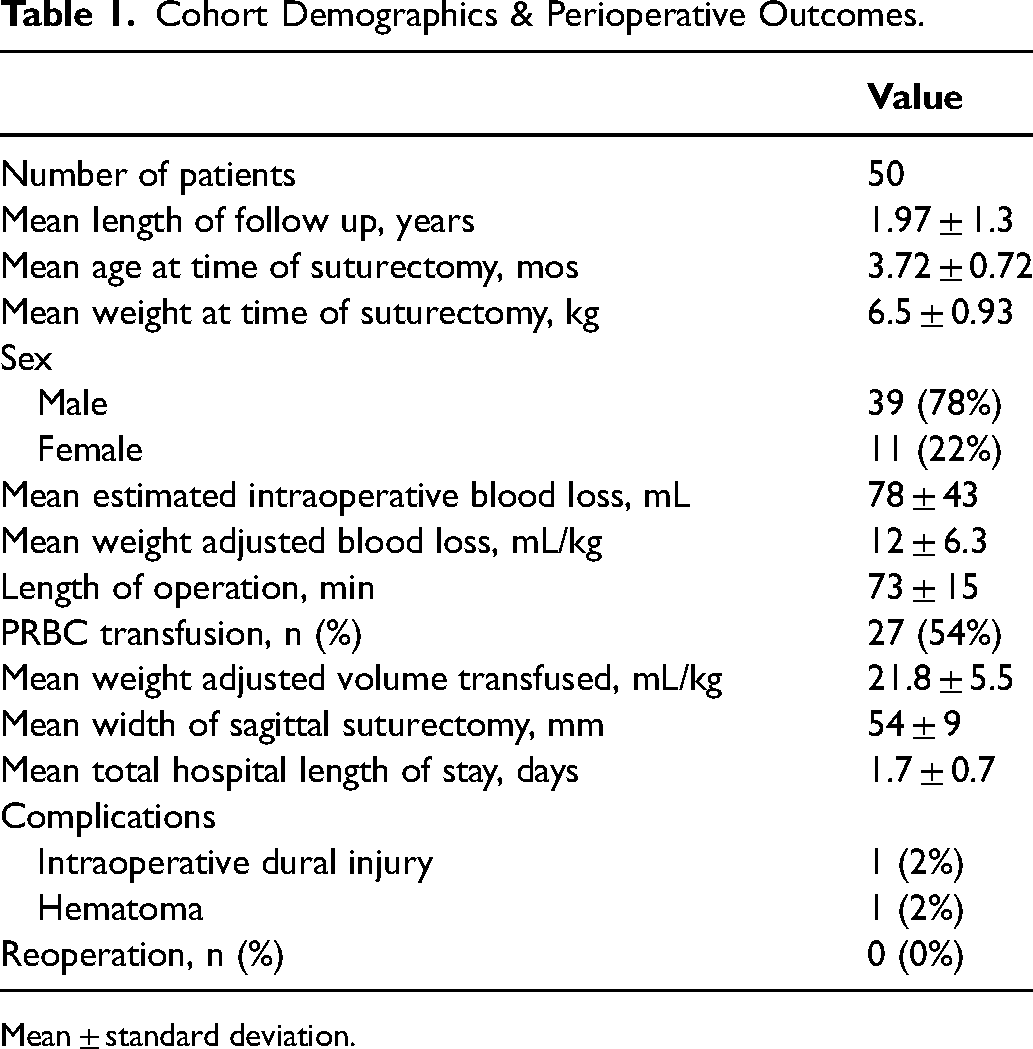
Mean ± standard deviation.
Calvarial Bone Thickness
The mean bone thickness of the parietal bone in the region of osteotomies was 1.84 ± 0.46 mm. The mean thickness of the right and left spot measurements of the frontal bone in the region of frontal releasing osteotomies were both 2.00 ± 0.4 mm; these did not differ significantly in pairwise analysis (p = 0.916). Table 2 displays the mean bone thickness throughout the calvarium, which differs both on laterality and anteroposterior positioning. On both the left and right parietal bone measurements, the bone thickness increased posteriorly (rows 1–3), with a decrease in bone thickness on the most posterior measurement 1 cm anterior to the lambdoid suture (row 4). The bone thickness was not significantly different on the left and right of the same anteroposterior position in the parietal region (p > 0.05). The thickness of the parietal region displayed a significant positive correlation to frontal bone thickness (ρ=0.483, p < 0.001). Patient weight and age at the time of surgery did not correlate with bone thickness in the parietal or frontal region (p > 0.05). See Figure 1 for a representation of the locations analyzed in relation to osteotomies and a three-dimensional bone thickness heat map of a patient included in the study.
Bone Thickness Measurements.
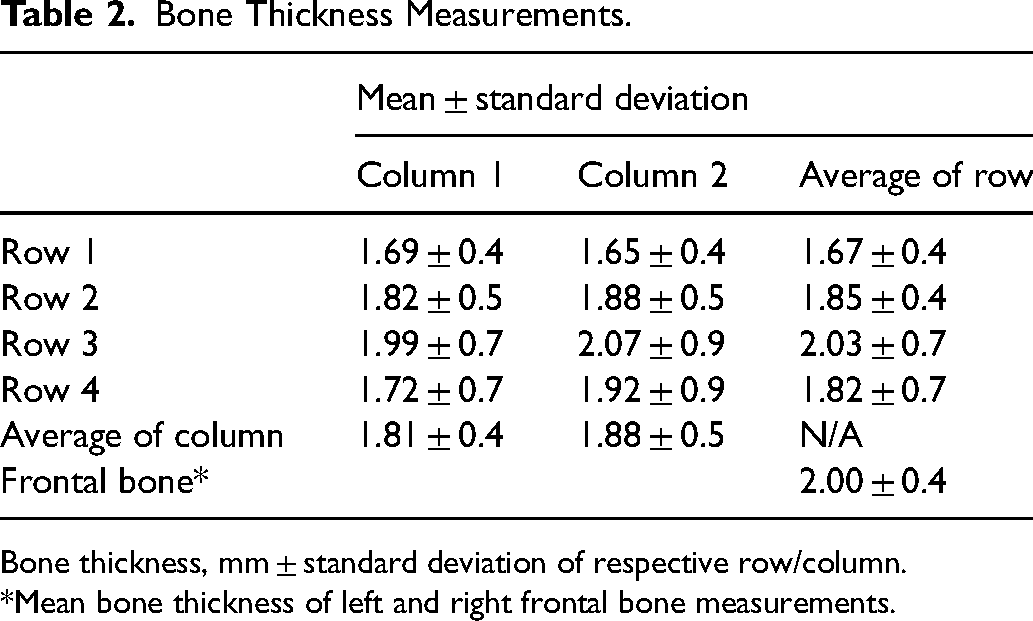
Bone thickness, mm ± standard deviation of respective row/column.
*Mean bone thickness of left and right frontal bone measurements.
Bone Thickness, Estimated Blood Loss, and Length of Stay
Table 3 shows the relationship between estimated blood loss and bone thickness. Parietal bone thickness in the line of osteotomies had a significant positive correlation to estimated blood loss (ρ=0.620, p < 0.001) and weight-adjusted blood loss (ρ=0.560, p < 0.001). Similarly, frontal bone thickness showed a significant positive correlation to both estimated blood loss (ρ=0.380, p = 0.007). and weight-adjusted blood loss (ρ=0.390, p = 0.006). Both the left and right aspects of the parietal bone (columns 1 and 2) positively correlated to blood loss (p < 0.001), as well as each row anteroposteriorly (p < 0.05). Both patient age, maximum calvarial bone thickness, and width of the suturectomy did not correlate with blood loss (p > 0.05). Of note, bone thickness, patient weight, duration of operation, and patient age did not have an association with the postoperative length of stay in the hospital (p > 0.05).
Correlation Between co-Variates and Intraoperative Blood Loss.
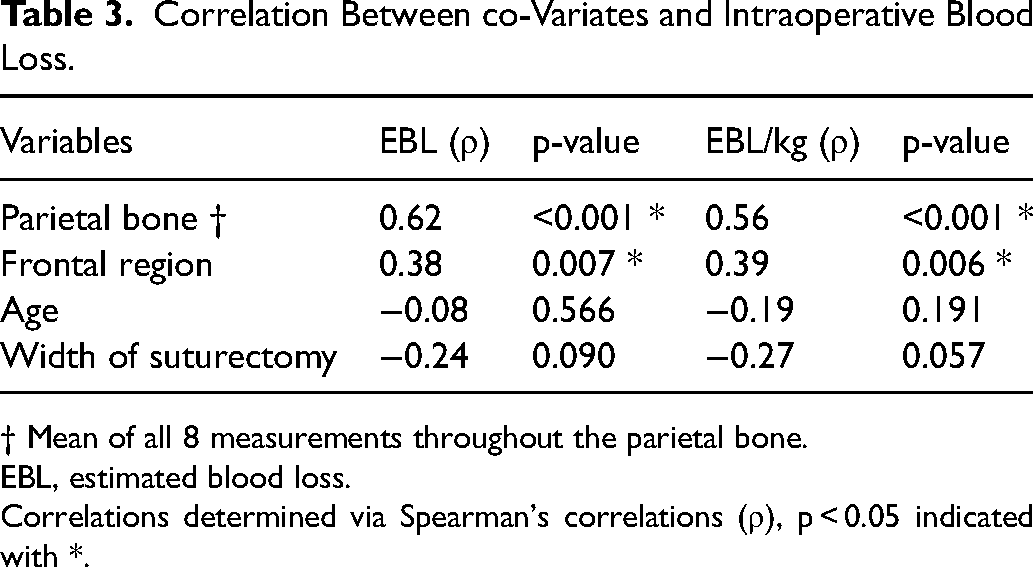
† Mean of all 8 measurements throughout the parietal bone.
EBL, estimated blood loss.
Correlations determined via Spearman's correlations (ρ), p < 0.05 indicated with *.
Estimated blood loss intraoperatively was associated with frontal and parietal bone thickness using a multivariable linear regression model controlling for patient weight and duration of operation (see Supplemental Table 1). For each 0.1 mm of increased parietal bone thickness in the region of osteotomies, regression modeling predicted an additional 4.17 mL of blood loss intraoperatively (95% CI: 1.62–6.71, p = 0.002). Of all the variance in blood loss, 29% was explained by parietal bone thickness in this model (R2 = 0.292). Additionally, a 0.1 mm increase in frontal bone thickness resulted in an additional 3.92 mL of blood loss (95% CI: 0.50–7.34, p = 0.026), with 22% of the variance in blood loss explained by frontal bone thickness (R2 = 0.216).
Perioperative Blood Transfusion
Twenty-five patients (50%) required an intraoperative blood transfusion, with a mean transfusion volume of 21.8 mL/kg (range, 10–34 mL/kg). Two additional patients (4%) required a postoperative blood transfusion while in the PICU, both of which occurred on the same day of surgery. Supplemental Table 2 shows the mean bone thickness in the transfusion versus non-transfusion groups. The mean bone thickness in the parietal region was significantly higher for patients who received transfusion (2.04 mm versus 1.61 mm, p < 0.001). Similarly, the mean thickness of the frontal region was significantly higher for patients who received transfusion (2.14 mm versus 1.84 mm, p = 0.004). Table 4 shows the relationship between transfusion and bone thickness in the parietal and frontal regions using a multivariable logistic regression model controlling for patient weight and the duration of operation. The bone thickness in the parietal and frontal region were both associated with higher odds of blood transfusion (p < 0.01). Parietal bone thickness was the strongest predictor of blood transfusion, with logistic modeling indicating that a 1 mm increase in parietal bone thickness corresponded to 39.2 times higher odds of receiving an intraoperative transfusion (95% CI: 3.2–488, p = 0.004). Similarly, a 1 mm increase in frontal bone thickness resulted in 22.1 times higher odds of receiving a transfusion when controlling for weight and duration of operation (95% CI: 2.5–197, p = 0.006). Patient weight (p = 0.806) and the duration of operation (p = 0.271) were not significant predictors of transfusion with univariable logistic regression modeling.
Multivariable Logistic Regression Models for Tranfusion §.
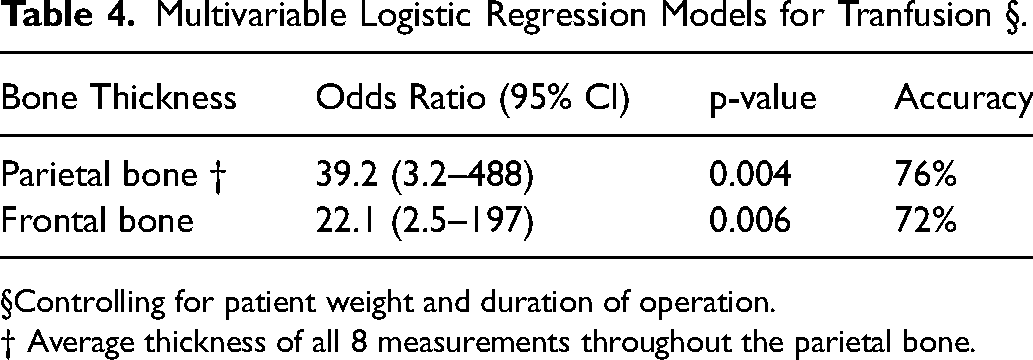
§Controlling for patient weight and duration of operation.
† Average thickness of all 8 measurements throughout the parietal bone.
This logistic model using parietal bone thickness to predict the need for blood transfusion was able to correctly identify 78% of all patients who would require a transfusion and 74% of patients who would not require a transfusion, giving an overall predictive accuracy of 76%. Conditional estimate plots provided a visual representation of these probabilities which indicate that a mean parietal bone thickness of 1.75 mm corresponded to a 50% probability of transfusion (95% CI: 33% - 66%). A mean parietal bone thickness of 2.05 mm corresponded to a 75% probability of transfusion (95% CI: 53–88%). Multivariable modeling using frontal bone thickness to predict blood transfusion was 74% accurate at identifying patients who would receive a transfusion and 70% accurate at identifying patients who would not receive a transfusion, giving a total model accuracy of 72%. Patients with a mean frontal bone thickness of 1.9 mm had a 50% probability of transfusion (95% CI: 30–65%). A mean frontal bone thickness of 2.25 mm corresponded to a 75% probability of transfusion (95% CI: 53–88%). See Figure 2 for a graphical representation of these probabilities.
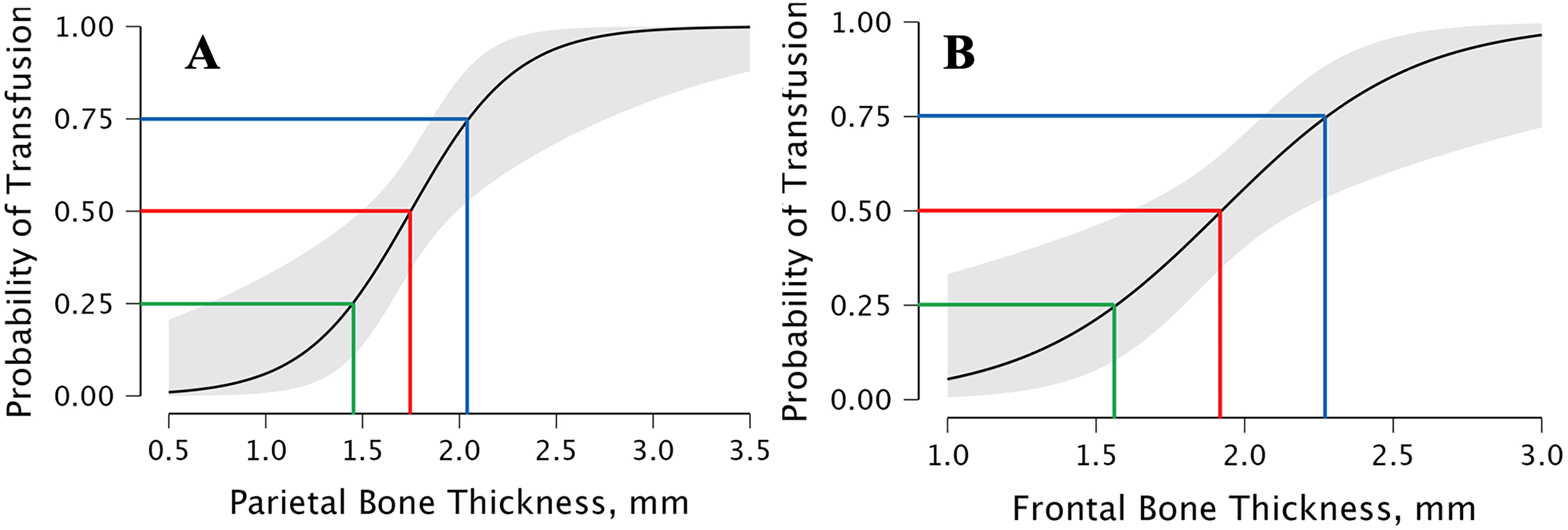
Conditional estimate plots from multivariable logistic regression modeling using bone thickness of the parietal bone (A and frontal bone thickness (B) to predict the probability of transfusion. Green, blue, and red lines represent the bone thickness corresponding to 25% (green), 50% (blue), and 75% (red) probability of transfusion as found with the logistic model. Light gray shading corresponds to the 95% confidence interval.
Discussion
Over the last two decades, extended sagittal suturectomy followed by postoperative orthotic therapy has gained popularity in the care of patients with single suture craniosynostosis due to the lower morbidity compared to open calvarial vault remodeling. 19 Although extended sagittal suturectomy is less invasive than open procedures, it still imposes a significant risk of intraoperative blood loss and transfusion due to extensive tissue dissection and bone cuts. It remains paramount to look for ways to better predict patients at higher risk for increased blood loss and likelihood of transfusion. Currently, surgical teams must frequently rely upon aggregate statistics to predict the morbidity of extended suturectomy without integration of patient-specific anatomy that may make blood transfusion more likely. This study provides a promising new mechanism to identify patients with a higher likelihood of transfusion and significant blood loss using preoperative thickness measurements of the frontal and parietal bone in the line of osteotomies. These models have the potential to improve preoperative surgical expectations and allow craniofacial teams to provide families with a more accurate representation of the probability of blood transfusion during this operation.
Three-dimensional head mapping technology for craniosynostosis has been used for a variety of purposes throughout the literature and with great accuracy to clinical observations.20,21 The frontal and parietal bone thickness measurements displayed in Table 2 vary both anteroposteriorly and laterally, consistent with the existing understanding of cranial anatomy.14,22,23 Additionally, the calvarial tomography described in this study is in accordance with previous studies of isolated sagittal craniosynostosis using the same image analysis software, with small variation likely attributable to the margin of error of bone thickness calculations and slight variability in the locations analyzed. 14 All thickness measurements in this study were collected by a single pediatric neuroradiologist rather than a craniofacial or neurological surgeon which may have contributed to more precise measurements than other analyses in the literature. Given the intricacy of performing these thickness calculations, it may be advised to look for ways to integrate these thickness calculations into the standardized craniosynostosis CT readings which are routinely performed by radiologists.
Our multivariable regression models identifies a moderate association between bone thickness and surgical morbidity. These findings are in agreement with prior research and surgical observation, which indicate that increased bone thickness is positively correlated to an increase in diploic space and arteriovenous sinuses for blood flow; thus, increased thickness in the osteotomy sites could result in increased blood loss.14,24 Multivariable linear regression modeling predicts that a 0.1 mm increase in parietal bone thickness corresponds to a 4.17 mL increase in blood loss. Given that the mean parietal bone thickness observed in our cohort ranged from 1.3 to 3.3 mm, bone thickness has the potential to explain a significant amount of variation in blood loss between patients. Patient weight and age were not found to have significant relationships to estimated blood loss in this study, although other papers have discussed the impact of these factors on perioperative morbidity in craniosynostosis surgery. 25 This is likely attributable to our institutions reduced range of patient age (corrected for prematurity) which sagittal suturectomy is performed before we would recommend spring cranioplasty or open calvarial vault remodeling due to increased mineralization of the calvarium resulting in less responsiveness of the bone to the orthotic molding treatment postoperatively.
Our perioperative anemia management protocol for craniosynostosis surgery did not change across the study duration. Although TXA was infused during all included operations, the proportion of patients receiving a blood transfusion (54%) was higher than in some prior literature.11,12 This may be attributable to the fact that our analysis includes both intraoperative and postoperative transfusions rather than only intraoperative transfusion. Additionally, some institutions with a lower transfusion rate utilize presurgical erythropoietin for elevation of the hemoglobin and/or intraoperative cell saver. 26 While we have explored these options, we do not currently utilize either one. Some institutions also accept lower perioperative hemoglobin levels in this age group; thus, transfusion rates can vary widely based on institutional protocols. Although there are small risks associated with transfusion, our institution considers blood transfusion in all patients whose estimated blood loss is greater than 10% of their total blood volume and/or for symptoms consistent with inadequate perfusion and oxygenation given that the benefits of transfusion far outweigh the risks. Additionally, transfusion risks are minimized to the greatest extent possible with fellowship-trained pediatric anesthesiologists and hospitalists who carefully monitor all transfusions to avoid over-transfusing.
The findings of this study are promising; however, they are only useful if they can be easily integrated into clinical practice and during presurgical consultation. The process of calculating bone thickness throughout the parietal bone was time-consuming to obtain for the current study, as numerous locations had to be analyzed. Additional challenges can also arise based on the positioning of the patient in the CT scanner, leading to difficulties with measuring the bone thickness in the correct plane in many of these locations. Given these challenges, frontal bone thickness may be a more efficient measure for clinical use, with only one or two measurements needed because of similarities in frontal bone thickness bilaterally. Although the predictive significance of frontal bone thickness is slightly less than that of parietal bone thickness, frontal bone thickness displayed a similar relationship to blood loss. Indeed, frontal bone thickness was 72% accurate at predicting patients who would require transfusion compared to 76% with parietal bone thickness as the predictor variable.
The findings presented in this study are most useful for patients with high percentile frontal/parietal bone thicknesses, indicative of a transfusion probability nearing 90–100% based on our institution's transfusion guidelines. In these instances, families can be informed that the likelihood of requiring transfusion is much higher than aggregate statistics may indicate. Additionally, this information could be used to better prepare the operating room team preoperatively (nurses, anesthesia, surgeons) regarding the high probability of transfusion during an operation, as the surgical time is relatively short with an average duration of approximately one hour. Although patients with lower percentile frontal/parietal bone thicknesses have a lower likelihood of needing a transfusion, we still believe that it is best practice during preoperative consultation to prepare all families for chance of a blood transfusion given the occurrence of unanticipated intraoperative events unrelated to calvarial bone thickness and the need to properly manage perioperative family expectations.
All conclusions of this study must be taken in the context of its study design and sample size. Given the retrospective nature of this study, no direct causation between bone thickness and blood loss can be drawn. Additionally, the generalizability of these conclusions must be taken in the context of our operative technique. Future research should focus on how bone thickness can be used to predict the surgical morbidity of suturectomy operations involving other cranial sutures and for frontal orbital advancement, given that tissue dissection and bone cuts are more extensive with longer duration of surgery. Further research should compare the morbidity of suturectomy and spring-mediated cranioplasty with bone thickness as a co-variate. Although this study has limitations, this study provides a promising new mechanism to predict the surgical morbidity of extended sagittal suturectomy for patients with isolated, nonsyndromic sagittal craniosynostosis. These models will benefit from continued monitoring with re-analysis to increase sample size in future work.
Conclusion
Frontal and parietal bone thickness in the line of osteotomies is associated with intraoperative blood loss and odds of transfusion for patients with isolated sagittal craniosynostosis undergoing extended sagittal suturectomy. Frontal bone thickness in the region of the frontal releasing osteotomy is highly correlated with parietal bone thickness and is an efficient measurement to utilize when assessing the probability of perioperative transfusion; thus, may be utilized to provide families with a more accurate representation of the likelihood of transfusion.
Supplemental Material
sj-xlsx-1-cpc-10.1177_10556656231202840 - Supplemental material for Preoperative Frontal and Parietal Bone Thickness Assessment to Predict Blood Loss and Transfusion During Extended Suturectomy for Isolated Sagittal Craniosynostosis
Supplemental material, sj-xlsx-1-cpc-10.1177_10556656231202840 for Preoperative Frontal and Parietal Bone Thickness Assessment to Predict Blood Loss and Transfusion During Extended Suturectomy for Isolated Sagittal Craniosynostosis by Austin M. Grove, Hannah M. Kirsch, Nicole M. Kurnik, Ruth E. Bristol, Thomas J. Sitzman, Cory Pfeifer and Davinder J. Singh in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-xlsx-2-cpc-10.1177_10556656231202840 - Supplemental material for Preoperative Frontal and Parietal Bone Thickness Assessment to Predict Blood Loss and Transfusion During Extended Suturectomy for Isolated Sagittal Craniosynostosis
Supplemental material, sj-xlsx-2-cpc-10.1177_10556656231202840 for Preoperative Frontal and Parietal Bone Thickness Assessment to Predict Blood Loss and Transfusion During Extended Suturectomy for Isolated Sagittal Craniosynostosis by Austin M. Grove, Hannah M. Kirsch, Nicole M. Kurnik, Ruth E. Bristol, Thomas J. Sitzman, Cory Pfeifer and Davinder J. Singh in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.