
Abstract
Objective
To describe long-term outcomes and complications following mandibular distraction osteogenesis (MDO) in a diverse patient cohort
Design
Cross-sectional study
Setting
Single tertiary-care pediatric center
Patients
Forty-eight patients previously undergoing MDO with minimum 4-year follow-up
Main Outcome Measures
Respiratory outcomes, feeding patterns, dental development, motor/sensory nerve function, temporo-mandibular joint function, and postsurgical scarring
Results
Forty-six patients with a median age of 7 years were evaluated. Of 20 nonsyndromic patients, none required additional airway procedures, none required continuous positive airway pressure (CPAP) during sleep, and 19 (95%) fed exclusively by mouth. Among 26 syndromic patients, 7 (27%) required CPAP and 8 (31%) were tube fed. Permanent first molar differences were seen in the majority of subjects; patterns of damage interfering with function were more common in syndromic (13/28, 46%) compared to nonsyndromic (5/24, 21%; P = .014) subjects. MDO prior to age two was associated with more frequent and worse dental damage (P = .001). Inferior alveolar nerve and marginal mandibular nerve function were fully intact in 37 (80%) and 39 (85%) of patients, respectively. Three patients (6%), all with associated genetic syndromes, demonstrated severe nerve impairment. By the Vancouver scar scale, ≥ 80% of surgical scars were rated in the most favorable category for each quality assessed. Temporomandibular joint dysfunction was rare.
Conclusions
MDO shows highly favorable long-term respiratory, feeding, nerve, and scar outcomes in nonsyndromic patients, although permanent molar changes not precluding tooth viability are commonly seen. Patients with associated syndromes demonstrate respiratory and feeding benefits, but higher rates of dental and nerve abnormalities.
Introduction
Correcting microretrognathia through mandibular distraction osteogenesis (MDO) acutely improves feeding and tongue-based airway obstruction (TBAO) in patients with moderate to severe disease unresponsive to conservative measures.1–8 MDO is commonly employed in Pierre Robin sequence and syndromes involving microretrognathia,9–11 but may also be used to avoid tracheostomy or facilitate decannulation in broader cases of TBAO.5,12–17
Mounting evidence demonstrates that MDO tends to consistently and effectively treat moderate to severe obstructive apnea, and tracheostomy is avoided in the vast majority of patients.7,18 However, little evidence attests to the long-term duration of these early interventions. Furthermore, rates of complications such as relapse, device failure, infection, scarring, temporomandibular joint ankylosis, tooth injury, and nerve injury are not well established.2,5,6,8,19–22 Most complications are reported in small institutional case studies or series, and some may reflect early techniques that have since evolved. Furthermore, retrospective reviews suffer from limited follow-up and non-standardized clinical and outcome measurement. This hinders accurate understanding of clinical outcomes, and presents challenges to patient-specific risk-benefit assessment. 20
To address this paucity of long-term outcomes data, we aimed to measure comprehensive respiratory, feeding, dental, neurologic, and functional outcomes of patients previously undergoing MDO who are now at least 4 years of age. We hypothesized that MDO would provide resolution of respiratory distress and improve feeding, with low but nonzero rates of nerve and tooth bud injuries, particularly in syndromic patients.
Methods
Patients undergoing MDO to treat TBAO between 2008 and 2017 with clinical follow up in our craniofacial center from July 2020 to June 2021 were eligible for inclusion in this cross-sectional study. Patients with less than 4 years of follow-up after MDO were excluded. To reduce attrition bias, all otherwise eligible patients who did not have a scheduled appointment during the assessment period were mailed a letter reminding them of maintaining annual follow-up. This study was approved by our center's Institutional Review Board (IRB 19-016772) and appropriate informed consent was obtained for publication of all identifiable images.
Institutional MDO Protocol
Our institutional MDO technique has been described previously. 23 An external approach via Risdon incisions 1-2 cm inferior to the mandibular angle is employed. An ultrasonic piezoelectric scalpel is used to perform an oblique osteotomy from the retromolar margin of the mandible through buccal and lingual cortical surfaces to a point approximately 1 cm anterior to the mandibular angle, without disruption of cancellous bone. Inverted-L pattern osteotomies were used in two patients at the end of the surgical period for this study cohort, with the remainder of osteotomies performed using conventional linear techniques. Internal distractors are utilized with retroauricular placement of activation arms. Activation follows 2-day latency at a rate of 1-2 mm/day and typically continues to a clinical endpoint of mandibular advancement to a 3-5 mm anterior overjet relative to the maxillary alveolus.
Comprehensive Clinical Assessment
Enrolled patients were comprehensively assessed in the following categories: respiratory and feeding (sleep disordered breathing, use of feeding adjuncts), dental and orthodontics (dental injury, occlusion, cant, open bite), temporomandibular joint (TMJ) function (patient-reported symptoms, maximal incisal opening), nerve function (inferior alveolar nerve sensation, marginal mandibular nerve function), and scarring (scar appearance).
Respiratory and Feeding Outcomes
Demographics, polysomnography data, syndromic status, and all respiratory and feeding adjuncts at last follow-up were abstracted from the medical record. All polysomnograms (PSGs) were conducted and scored according to American Academy of Sleep Medicine pediatric specifications. 24
Dental and Orthodontic Evaluation
Comprehensive pediatric dental/orthodontic assessment was performed by one of two pediatric craniofacial orthodontists. Occlusion status, occlusal cant, open bite, transverse dental arch discrepancy, and maxillary/mandibular midline misalignment were evaluated for both primary and permanent dentition. Each patient's most recent dental imaging was collected, as available, and evaluated by a single pediatric craniofacial orthodontist. Based on radiographic evaluation, permanent first and second molars and tooth buds were classified according to degree of damage and viability for dental restoration. Outcomes were analyzed by each hemimandible undergoing MDO.
TMJ Function
Patients and parent/caregiver proxies were interviewed regarding temporomandibular joint functionality, including history of pain when chewing, crepitus, difficulty eating, clicking/popping, and grinding/grating. Maximal interincisal opening (MIO) was assessed using a range of motion scale and compared to standardized age-adjusted means. 25
Inferior Alveolar and Marginal Mandibular Nerve Function
The inferior alveolar nerve (IAN) was assessed by touching the upper and then lower lip on both sides utilizing the same level of pressure. Patients then were asked to subjectively describe if (1) they could discern the touch and (2) if the upper and lower lip touch felt similar. Grading of lip sensation was as followed: fully intact, mildly impaired, severely impaired, and no sensation. The marginal mandibular nerve (MMN) was assessed by asking the patient to mirror a sequence of facial movements. If asymmetry was present, still photographs and videos were obtained and MMN of each side graded as: symmetrical, mild asymmetry, and severe asymmetry.
Surgical Scar Assessment
The Vancouver Scar Scale was used to assess surgical scars on four scales: vascularity, height/thickness, pliability, and pigmentation. 26
Statistical Analysis
Descriptive statistics were reported as means with standard deviations (SDs) and medians with interquartile ranges (IQRs) or frequencies with percentages. Tests of normality were performed. Comparisons were completed using the Wilcoxon rank sum test and the χ2 or Fisher exact test. Correlations were assessed using Spearman's rho with Bonferroni correction applied as indicated. Logistic regression analysis was presented as odds ratios with 95% confidence intervals with Haldane-Anscombe correction applied as indicated. P values were all 2-tailed with α< .050 being considered statistically significant. Statistical analyses were performed using StataMP Release 16 (College Station, TX) and JASP Version 0.16.4 (JASP Team, 2020).
Results
Of 113 eligible patients who underwent MDO in the reference period, 46 were enrolled. The cohort was 63% male, 66% white, and 56% had an underlying syndrome (Table 1). Of eligible patients who did not enroll in the study, 37% had a genetic syndrome. The indication for MDO was TBAO in all patients, of which 3 also had hemifacial microsomia (HFM). Median age at distraction was 2.6 months (IQR 0.6-30.0) and median duration of activation was 18 days, equating to a mean estimated distraction distance of 24 mm. Median age at study enrollment and clinical assessment was 7.0 years (IQR 5.8-8.5), with 16 patients were aged 4-5 years, 12 aged 6-7 years, 8 aged 8-9 years, and 10 aged 10 years or older. Twenty patients had a history of airway disease in addition to TBAO, most commonly laryngomalacia and tracheomalacia. Twelve patients underwent other airway-related interventions prior to MDO, most commonly adenoidectomy and/or tongue-lip adhesion (Table 1). Timing of surgery within the study period was not associated with different incidence of nerve or dental injury (P = .999, P = .587). Representative clinical imaging is presented in Supplemental Figures 1 and 2.
Patient Demographics.
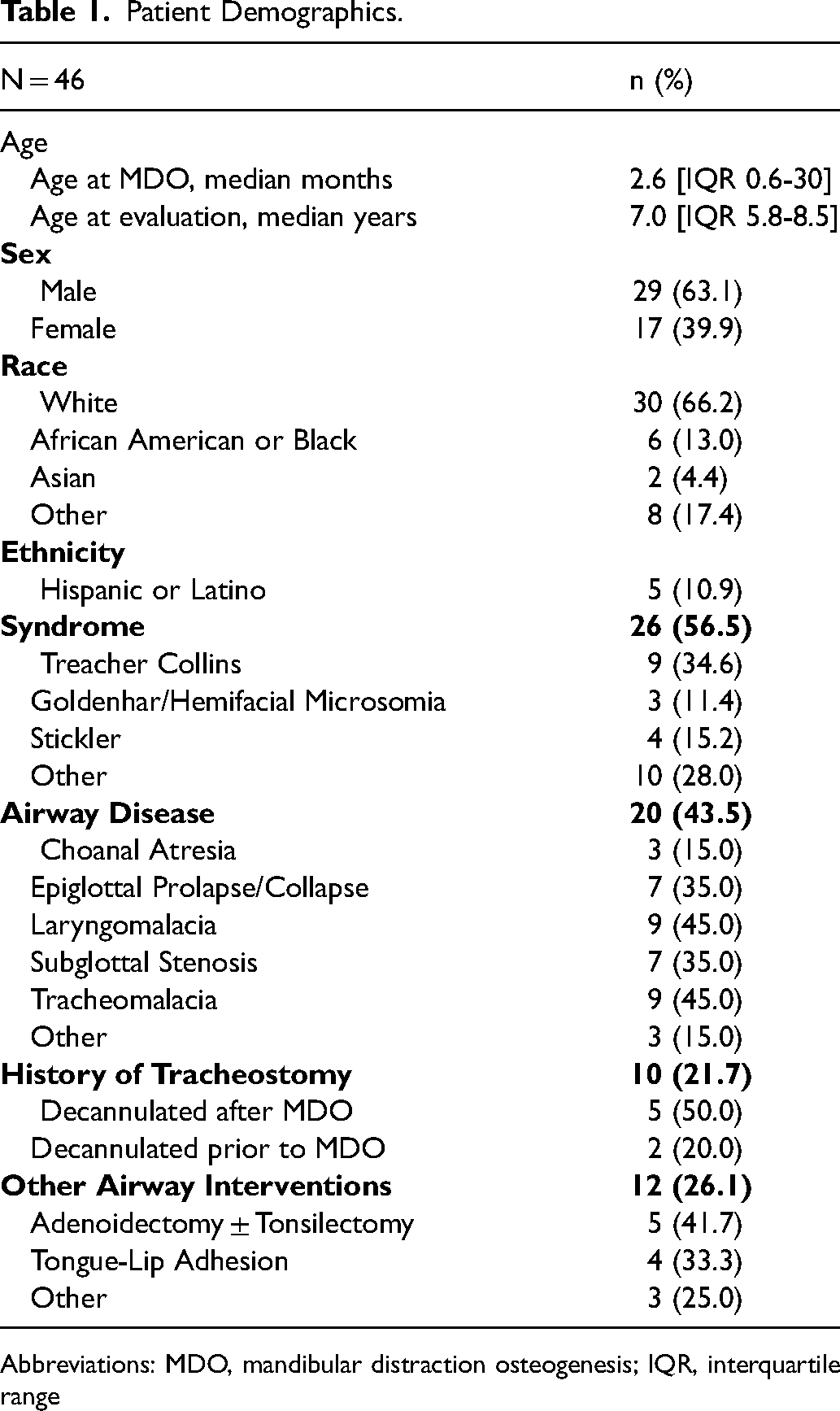
Abbreviations: MDO, mandibular distraction osteogenesis; IQR, interquartile range
Respiratory and Feeding Outcomes
Compared to baseline evaluation, most recent polysomnographic evaluation without CPAP, performed at median age 3.9 (IQR 1.1-5.4) years, showed improved median obstructive apnea-hypopnea index (32.9 vs. 2.6, P < .001) and baseline SpO2 nadir (76 vs. 90, P < .001) (Supplemental Table 1). While most patients did not require additional airway support, 7 patients (14.6%) used nocturnal continuous positive airway pressure (CPAP) for OSA (Table 2). Ten patients had a history of tracheostomy: 2 were decannulated prior to MDO, 5 were decannulated after MDO, and 3 remained cannulated. All 7 patients requiring nocturnal CPAP at last follow-up had underlying syndromes (P = .032).
Feeding and Respiratory Outcomes at Most Recent Evaluation.
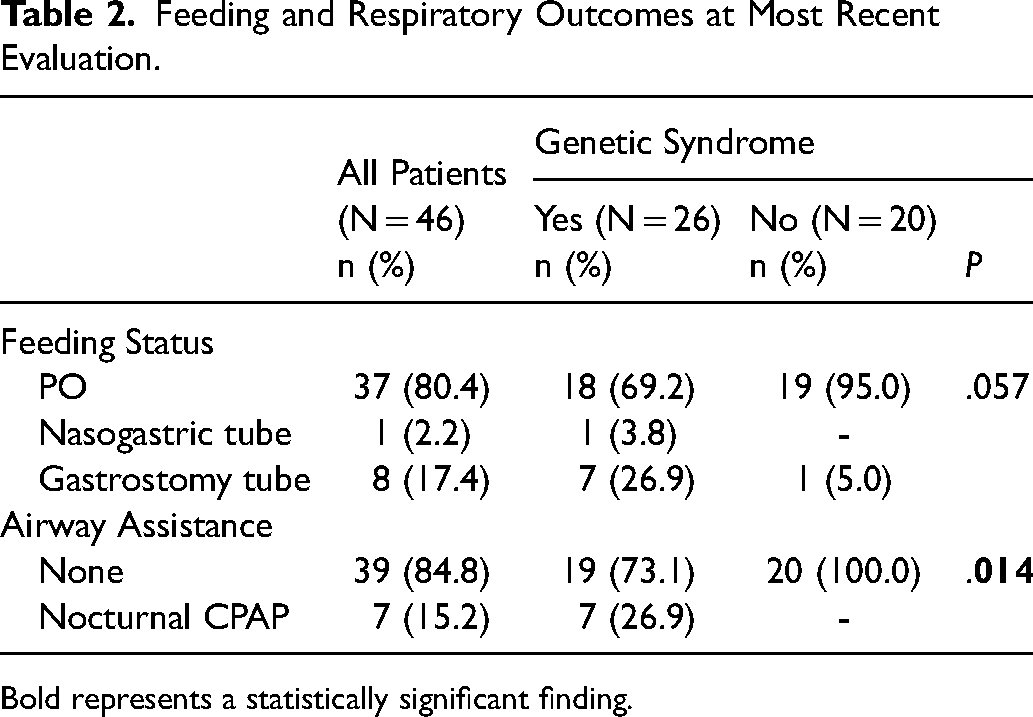
Bold represents a statistically significant finding.
At most recent evaluation, 39 patients fed completely orally ad lib, while one required a nasogastric tube and 8 had a gastrostomy tube in place (Table 2). Feeding adjuncts were more common in syndromic compared to nonsyndromic patients (30.7% vs. 5.0%; P = .057).
Dental and Orthodontic Evaluation
At evaluation ≥4 years following distraction, 23 (50%) of patients demonstrated a normal occlusal relationship, while 18 (35%) were in class II occlusion and 7 (15%) class III occlusion. All three HFM patients had an occlusal cant to the affected side; 11 (23%) non-HFM patients displayed occlusal cant. Anterior open bite was present in 20 (43%) patients. Posterior open bite ranging from 2-8 mm was observed in 3 (6%) patients, all with syndromic diagnoses. Seven (15%) patients had transverse discrepancy with or without posterior crossbite and 6 (13%) patients without HFM had maxillary-mandibular midline misalignment (Table 3).
Clinical Orthodontic, Nerve, and Scar Outcomes.
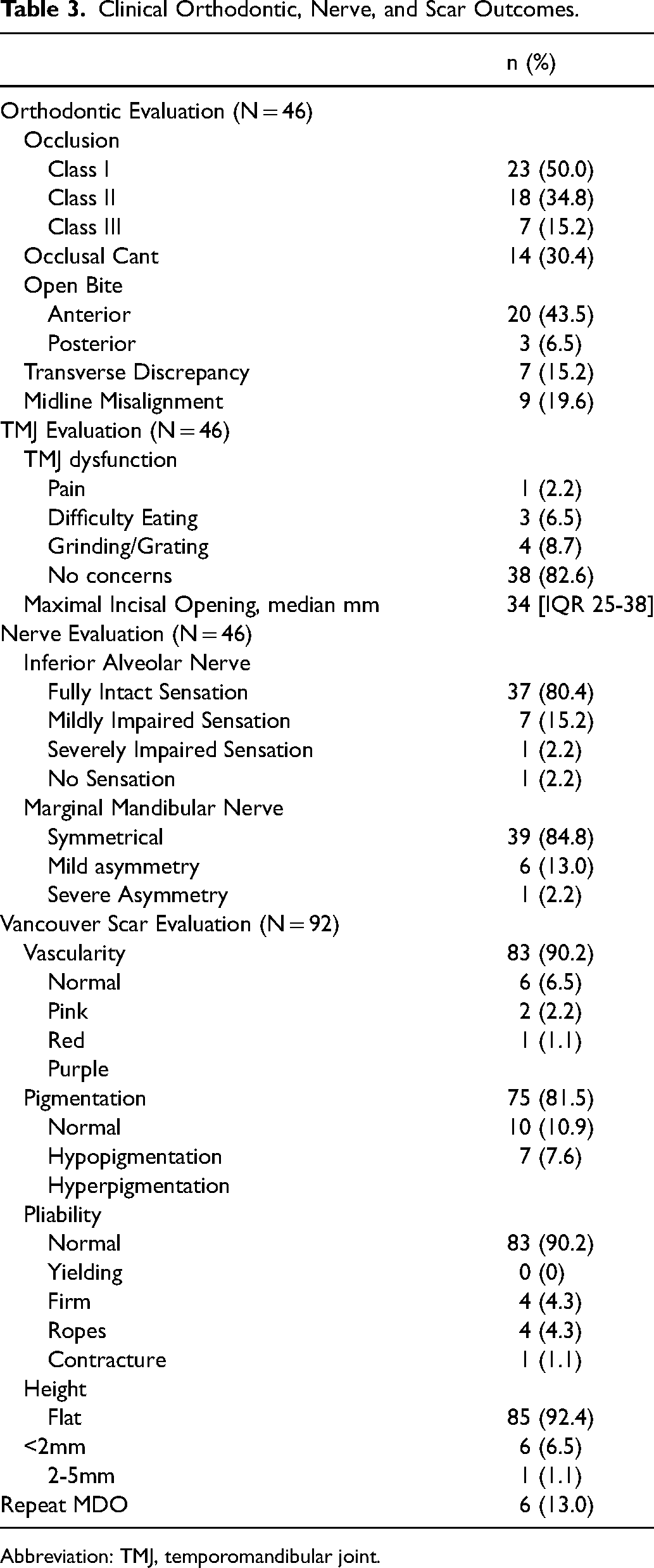
Abbreviation: TMJ, temporomandibular joint.
Twenty-nine patients (63%), representing 58 distracted hemimandibles, obtained comprehensive dental imaging. Fifty-two permanent first molars and 24 permanent second molars were evaluable for long-term dental damage (Supplemental Table 2). Overall, permanent first molar injury was seen in 79% of hemimandibles evaluated, with 55% of injured first molars retaining functionality and the remaining 45% considered nonfunctional and unrestorable (Table 4, Figure 1). MDO at the age of two or more years was associated with less frequent permanent first molar damage (P = .001). Syndromic patients had lower incidence of damaged but functional first molars relative to nonsyndromic patients (25% vs. 62%, P = .023), with most evaluated teeth instead categorized as normal or nonfunctional (Table 4). Inverted-L osteotomies were employed for 4 hemimandibles and were associated with restorable injury to permanent first molars in 3 cases, with one permanent first molar demonstrating normal development.
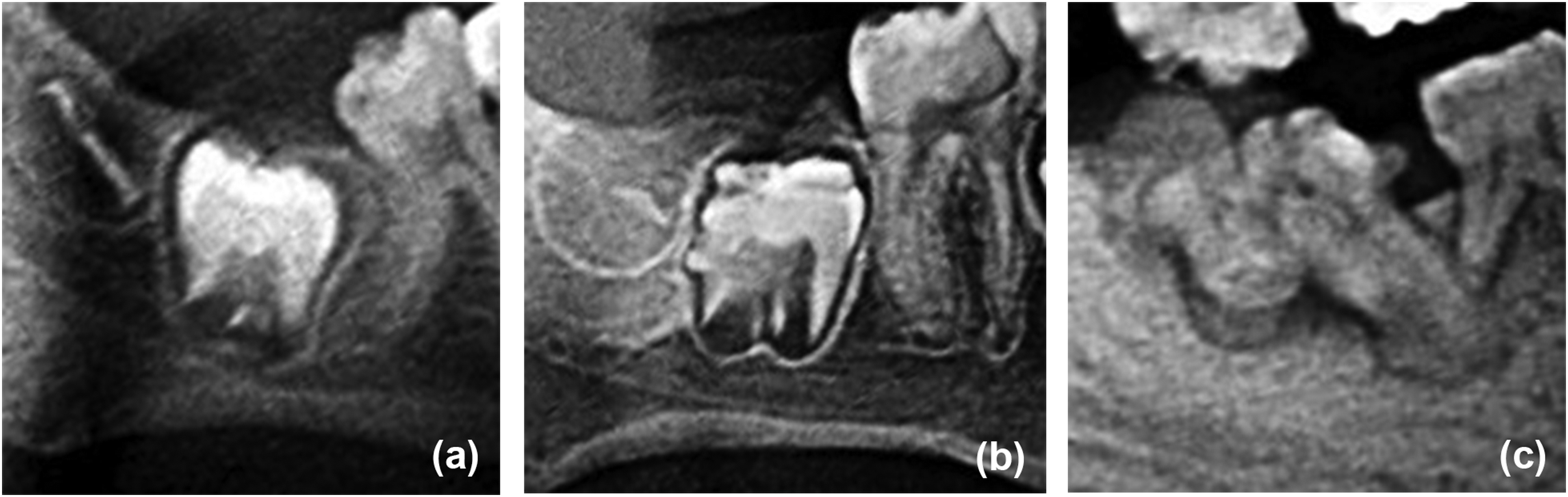
Dental injury following MDO. (a) Permanent first molar in an 8-year-old patient assessed as functional and restorable with good prognosis; (b) permanent second molar in an 11-year-old patient assessed as functional and restorable with a guarded prognosis; (c) permanent first and second molars in a 9-year-old patient assessed as non-functional and non-restorable.
Radiographic Dental Outcomes by Clinical Risk Factor.
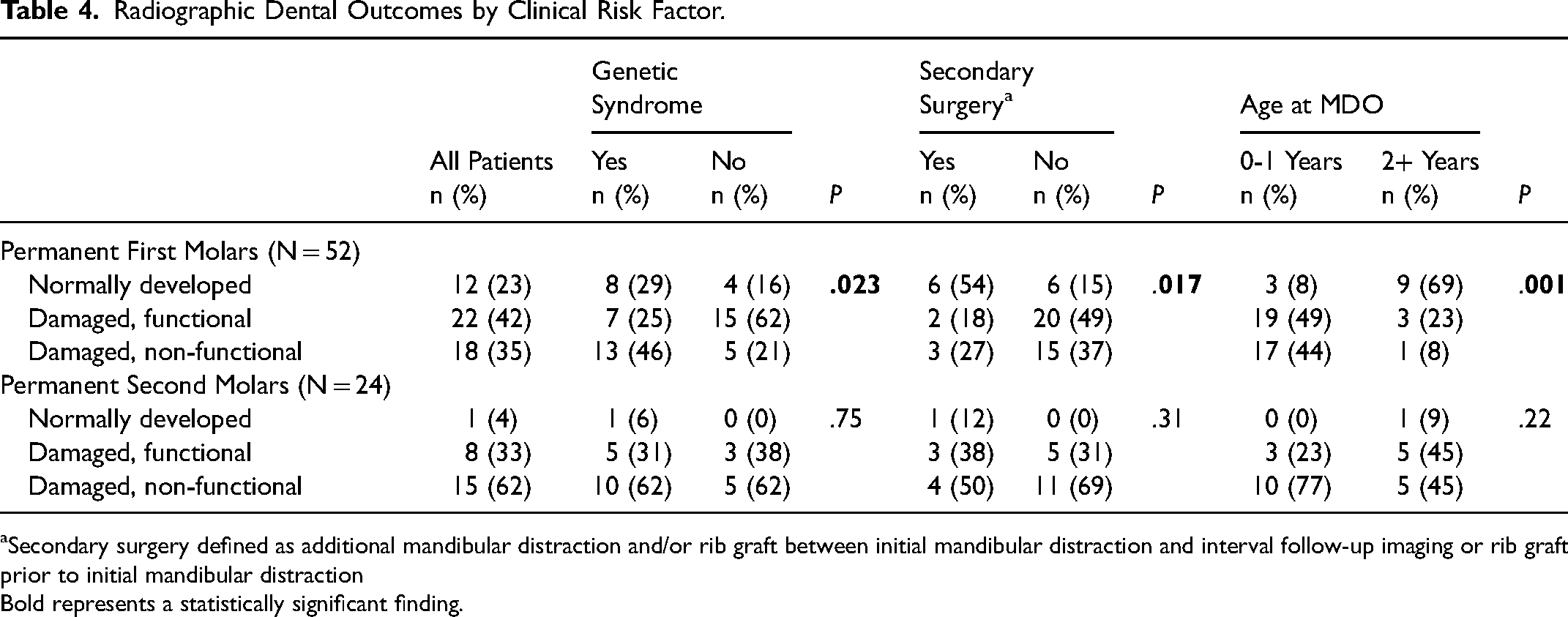
Secondary surgery defined as additional mandibular distraction and/or rib graft between initial mandibular distraction and interval follow-up imaging or rib graft prior to initial mandibular distraction
Bold represents a statistically significant finding.
Permanent second molars were most frequently judged to be nonfunctional and unrestorable (62%), with only one evaluable molar classified as normally developed. No specific risk factors for permanent second molar damage were identified (Table 4). Permanent first or second molar damage was correlated with symmetric damage to the contralateral mandibular permanent first or second molar (P < .001). Of 24 hemimandibles with evaluable permanent second molars, 7 (29%) had both permanent first and permanent second molars classified as damaged and non-functional. All such instances of adjacent non-functional permanent first and second molars were found in syndromic patients, with 2 patients bilaterally affected.
TMJ Function
No cases of TMJ ankylosis were identified. Eight patients, including 4 with underlying syndromes, reported TMJ-related symptoms. Four (8.7%) reported grinding or grating, 3 (6.5%) difficulty eating, and 1 (2.2%) pain (Table 3). Median maximal incisal opening was 34 mm (IQR 25-38) (Table 3). Twenty percent of syndromic patients had a maximal incisal opening that was 2 or more standard deviations below the mean for their age.
Inferior Alveolar and Marginal Mandibular Nerve Function
Most subjects demonstrated normal (80%) or mildly impaired (15%) lip sensation. One subject reported unilaterally absent sensation in the inferior alveolar nerve region while another reported bilaterally absent sensation (Table 3). Both patients had genetic syndromes. Additionally, 21% of syndromic patients reported mild sensation impairment compared to 10% of nonsyndromic patients (P = .43). Similarly, 85% of patients demonstrated full and symmetric marginal mandibular nerve (MMN) function, with 13% displaying mild asymmetry and 2% (1 subject) with severe asymmetry (Table 3, Figure 2). Only 5% of nonsyndromic patients suffered from mild asymmetry compared to 20% of syndromic patients (P = .20). Subjects with MMN impairment were 11.2 times more likely to have IAN impairment than those that did not have any impairment and vice versa (95%CI: 2.7-47.0, P < .001).

Mild smile asymmetry due to right marginal mandibular nerve weakness in a patient 7 years post-MDO.
Surgical Scar Evaluation
Ninety-four surgical scars were evaluated using the Vancouver Scar Scale. Most scars were of normal vascularity (90%), normal pigmentation (81%), normal pliability (90%), and flat (92%) (Table 3).
Impact of Secondary Surgeries
Repeat distraction was performed in 6 patients, with 2 patients undergoing rib grafts to the mandible either prior to or following MDO. Secondary mandibular surgery was associated with lower rates of permanent first molar damage (P = .017, Table 4), though this finding is confounded by an association between secondary surgery and older age at initial MDO (3 years vs. 0.7 years, P < .001). Those with repeat MDO procedures had greater risk of issues with scarring, specifically increased vascularity (OR = 5.74, 95%CI: 1.4-28.7, P = .037), pigmentation (OR = 5.63, 95%CI: 1.1-29.1, P = .047), and worse pliability (OR = 7.4, 95%CI: 1.2-47.2, P = .050).
Discussion
In this cohort of patients with diverse diagnoses and median 4.4 years of follow-up, MDO reliably achieved its primary goal: relieving TBAO as reflected in improved obstructive apnea during sleep. We observed not only a median OAHI reduction of 92% and 18% increase in oxyhemoglobin saturation nadir acutely following MDO but maintained resolution of airway obstruction in nearly all patients. This contrasts with previous reports of persistent severe obstructive sleep apnea in half of patients with Pierre Robin sequence treated with MDO. 3 Similarly, feeding gains were not only seen in the early post-operative period but improved further and were maintained over the long term. Despite these successes, we found evidence of long-term sequelae of MDO in a substantial portion of evaluated patients. Of most concern were high rates of permanent molar changes in both nonsyndromic and syndromic patients. While most long-term impacts were typically mild, with few patients suffering impaired function, we found that one-fifth of nonsyndromic patients exhibited function-impairing first molar damage.
Rates of dental injury following MDO have been previously estimated at 8-48%, however, interpretation of these results is complicated by varying patient population, surgical technique, duration of follow up, and criteria for dental damage.27,28 In a cohort of mainly nonsyndromic patients with at least 5 years of follow up, Steinberg et al., identified a 48% rate of permanent first molar injury with 76% of injured molars restorable with composite or crowns. 21 Our nonsyndromic subgroup demonstrated considerably higher rates of dental sequalae, with permanent first molar injury noted in 83% of distracted hemimandibles, though we similarly found 75% of injured molars were likely restorable. Late in the treatment period, our institution started to employ inverted-L shaped osteotomies, which may reduce molar injury by positioning the vertical osteotomy further posteriorly and improving technical fidelity. While inverted-L osteotomy pattern was not used with sufficient frequency in this cohort for analysis, dental injury in 3 out of 4 hemimandibles osteotomized with this technique suggests permanent molars remain at substantial risk for damage even with this modification. We did not routinely utilize pre-operative virtual surgical planning or patient-specific cutting guides for the majority of cases, which have also been described, because permanent tooth buds are generally not visible in infancy.
Literature regarding syndromic patient populations undergoing mandibular distraction is more limited, however, da Silva Freitas et al. reported a 33% dental injury rate in a cohort of patients with multiple craniofacial anomalies undergoing MDO. 29 Our subgroup of syndromic patients showed double this rate of dental injury (71%). This discrepancy may be due in part to the older age at which patients in the aforementioned study underwent distraction relative to patients with syndromes included in our analysis (mean 8 years vs. 2 years), as larger mandibles and more mature dentition facilitate avoidance of tooth buds when performing osteotomies and placing screws.
Additionally, prior studies describe permanent second molar injury as the third most common site of dental injury following MDO, after permanent first molars and primary second molars. 30 However, we noted damaged, non-functional permanent second molars in the majority of patients with sufficient tooth development for assessment. In 5 patients, all with genetic syndromes, non-functional permanent second molars were observed adjacent to non-functional permanent first molars. While functional dentition can be achieved despite loss of one permanent molar – through orthodontics, dental implants, or without intervention – management of two adjacent missing permanent molars is more challenging. 31 This highlights the importance of long-term follow-up in order to fully capture dental outcomes in this population.
We observed mild and severe lower lip depressor asymmetry in 13% and 2% of patients respectively, with asymmetry more common in patients with syndromes than those without. This incidence is in line with previous reports.21,32–35 Similarly, 10% of nonsyndromic and 27% of syndromic subjects reported decreased lower lip sensation compared to the upper lip, consistent with previous reports ranging from 2-20%.8,20,21,32,36,37 Specific risk factors for nerve injury remain controversial, with multiple procedures (imparting scarred tissue planes) and greater rates of distraction (greater risk of shear) proposed as contibutors.20,21,38 Use of intraoperative nerve stimulation has been proposed to minimize risk of marginal mandibular nerve injury. Although this was not routinely used during the study period, based on the findings of this study, it is now utilized selectively in cases to guide the dissection plane and minimize risk of nerve division.
Rates of TMJ ankylosis due to retropulsion of the condyle during MDO have been estimated at 2-16%.18,39,40 Syndromic patients – with more frequent pre-operative TMJ abnormalities and greater distraction distances – have demonstrated ankylosis rates of up 50% without unloading elastics. 39 We predominantly utilize a horizontal distraction vector in infant mandibular distraction, which has been suggested to have lower rates of ankylosis compared to vertical ramus distraction vector. No cases of complete TMJ ankylosis were identified in our cohort, but 9 patients (19%), all syndromic, had severely limited mouth opening over 2 standard deviations below the mean for their age. Furthermore, 17% of patients reported TMJ complaints, though these symptoms are likely polyfactorial and less representative of TMJ function than maximal incisal opening. Notably, we did not utilize a vertical distraction vector in the included patient cohort, which is thought to be a substantial risk factor for TMJ ankylosis. Nonsyndromic patients generally are at low risk for TMJ concerns, as corroborated by our findings, even with quite robust distraction lengths. 39
Patients in our cohort with associated syndromes showed relatively greater incidence of permanent first molar damage resulting in nonfunctional teeth (46%) and nerve impairment (38%) compared to nonsyndromic patients. This may reflect increased risk associated with more complex anatomy, as has been reported in Treacher Collins syndrome and HFM.40,41 It may also represent underlying dental agenesis, though this is more likely to involve pre-molars than molars and has also been reported in up to 33% of nonsyndromic RS patients not treated surgically. 42
This study has several limitations. First, historical treatment and diagnosis details were limited by retrospective review of available chart data and assessment of nerve function was limited to basic physical exam maneuvers that did not require specialty equipment. Baseline nerve deficit prior to distraction could not be ruled out but may have been present in some patients, particularly those with genetic syndromes. Second, despite our methodological attempts to limit selection bias, we note a study cohort weighted towards patients with syndromic diagnoses. The COVID-19 pandemic may have played a role in our total enrollment rate and participation of fewer nonsyndromic patients than would be expected. The majority of patients deferring follow-up we suspect are doing well and have outgrown their TBAO-related issues and have no considerable ongoing issues or sequalae, perhaps resulting in an overestimate of complication rates in this study. Third, while we incorporated a diverse group of patients in order to surveil outcomes as widely as possible, cohort heterogeneity impedes application of these findings to prospective risk assessment for individual patients. In response, we have presented multiple subgroup analyses to separate out outcomes associated with specific clinical factors.
Conclusion
This study of comprehensive long-term outcomes after MDO demonstrates maintained resolution of TBAO – with a small number of patients using CPAP at elementary age – and successful weaning of feeding adjuncts in nonsyndromic patients. Permanent first molar injury was noted in 77% of patients, with damage rendering molars non-functional more likely in syndromic patients and those undergoing distraction before the age of two. Marginal mandibular and inferior alveolar nerve dysfunction were uncommon and, if present, generally mild. Scarring was minimal, with worse outcomes noted in patients undergoing multiple mandibular procedures. Overall, MDO is effective and rarely associated with severe long-term complications, though monitoring of dental development in anticipation of permanent molar injury requiring intervention is advisable.
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231206884 - Supplemental material for Comprehensive Long-Term Outcomes Following Mandibular Distraction Osteogenesis
Supplemental material, sj-docx-2-cpc-10.1177_10556656231206884 for Comprehensive Long-Term Outcomes Following Mandibular Distraction Osteogenesis by Mychajlo S. Kosyk, Lauren K. Salinero, Carrie Z. Morales, Sameer Shakir, Christopher M. Cielo, Michelle Scott, Hyun-Duck Nah, Scott P. Bartlett, Jesse A. Taylor and Jordan W. Swanson in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231206884 - Supplemental material for Comprehensive Long-Term Outcomes Following Mandibular Distraction Osteogenesis
Supplemental material, sj-docx-3-cpc-10.1177_10556656231206884 for Comprehensive Long-Term Outcomes Following Mandibular Distraction Osteogenesis by Mychajlo S. Kosyk, Lauren K. Salinero, Carrie Z. Morales, Sameer Shakir, Christopher M. Cielo, Michelle Scott, Hyun-Duck Nah, Scott P. Bartlett, Jesse A. Taylor and Jordan W. Swanson in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656231206884 - Supplemental material for Comprehensive Long-Term Outcomes Following Mandibular Distraction Osteogenesis
Supplemental material, sj-docx-4-cpc-10.1177_10556656231206884 for Comprehensive Long-Term Outcomes Following Mandibular Distraction Osteogenesis by Mychajlo S. Kosyk, Lauren K. Salinero, Carrie Z. Morales, Sameer Shakir, Christopher M. Cielo, Michelle Scott, Hyun-Duck Nah, Scott P. Bartlett, Jesse A. Taylor and Jordan W. Swanson in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
JWS has received an educational grant and developed educational content for KLS Martin and Depuy Synthes, both of which produce mandibular distraction devices. JAT is co-founder of Ostiio, LLC.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
IRB
This study was approved by the Children's Hospital of Philadelphia Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.