
Abstract
Objective
To evaluate the long-term outcomes of linear commissuroplasty and linear skin closure with a focus on commissural migration.
Design
Retrospective study.
Patients
Individuals who underwent transverse facial cleft repair at a single institution between 2004 and 2021.
Interventions
The disrupted orbicularis oris muscle was reoriented and sutured. A simple linear commissuroplasty technique was used, and the cheek skin was closed linearly without Z-plasty.
Main outcome measures
The distances from Cupid's bow peak to the oral commissure were measured bilaterally, and the difference between the normal and cleft sides was obtained. Finally, its proportional value as a percentage of the total lip length was calculated from short- and long-term follow-up photographs. Cheek scarring and its effects on melolabial fold breakage were evaluated.
Results
Of the 18 patients who underwent transverse facial cleft repair, 12 were included in this study. The mean follow-up period based on medical photographs was 1773.5 days. The average proportional difference was 4.6%, demonstrating no observable commissural migration. There were no consistent trends in the direction of migration, either on the cleft or normal side. In patients with a transverse cleft crossing the melolabial fold, the folds appeared broken before and after the cleft repair surgery.
Conclusions
No significant long-term commissural migration was observed after transverse facial cleft repair with simple linear commissuroplasty and linear skin closure. Deliberate positioning of the new oral commissure, proper myoplasty, and meticulous skin closure with minimal scar burden can be considered key procedures for successful transverse cleft repair.
Introduction
Transverse facial cleft (Tessier type 7 cleft) is a congenital facial cleft that involves the oral commissure. Its incidence is reportedly between 1: 60 000 and 1: 300 000 live births. The cleft can present unilaterally or bilaterally, and the bilateral form is rarer (10-20% of cases). 1 It may occur with other syndromes, such as hemifacial microsomia (HFM), Treacher–Collins syndrome, and Goldenhar syndrome. 2 Transverse facial clefts have a wide spectrum of severity, from commissural defects to extensive defects involving muscular diastasis and bony deformities. 3 Most are limited to the anterior border of the masseter muscle, and even the mild types, involve disruption of oral sphincteric structures.
Discontinuation of the orbicularis oris muscle causes functional problems during feeding and speaking. In addition, there are concerns that a disharmonic appearance may lead to psychosocial problems as the patients grow up. Therefore, timely surgical intervention is essential. The objective of transverse cleft repair is to recover function and appearance. Transverse cleft repair consists of four major steps: (1) positioning of the neocommissure, (2) muscle repair, (3) commissuroplasty and (4) cheek skin closure. Several surgical techniques have been introduced for each step.
Several authors have used a vermilion flap or its variations in commissuroplasty to avoid creeping obliteration of the commissure.3–8 Some believe that the shape of the oral angle is more like a continuous web than a sharp corner; therefore, a vermilion flap is used to mimic the natural rounding of the angle. Many surgeons have raised concerned that the position of the new oral commissure gradually shifts laterally as the scar contracts, compared to its location immediately postoperatively, and this phenomenon is sometimes referred to as ‘lateral migration of the oral commissure’. Therefore, in cutaneous closure, some have advocated adding Z-plasty or W-plasty, as this disrupts the scar line and minimizes the postoperative lateral migration of the commissure.4,7,9–13 However, there is a lack of objective data supporting the superiority of the long-term outcomes of these methods over simpler method. This study aimed to objectively assess the long-term outcomes of transverse facial cleft repair using linear commissuroplasty and linear cutaneous closure with a focus on commissural migration.
Materials and Methods
This study was approved by Institutional Review Board (2022-11-113-001). Consent was exempted as there were no apparent reasons to anticipate refusal of consent from the research subjects, and the risks posed to the research subjects were extremely low. Patients who underwent transverse facial cleft repair at a single institution between 2004 and 2021 were retrospectively reviewed. Photographs and data, including demographic and cleft-related information and accompanying facial anomalies, were collected from the medical records. Patients who had missing photographs within 1 month or at least 17 months postoperatively were excluded. If a patient has undergone a revision surgery, the most recent photographs taken before the revision surgery was used. Long-term changes in anthropometric measurements and cheek-scar appearance were treated as the main outcomes.
Operative Technique
The position of the neocommissure was determined to achieve symmetry by referring to the normal side. The distance between the peak of Cupid's bow and the commissure on the normal side was measured at the vermilion border using a caliper. The mirrored point positioned at the same distance from Cupid's bow on the cleft side was determined to be a neocommissure. The midpoint of the lower lip served as the reference point for measurement. In bilateral cleft cases, a distinctive border between the normal lip and the abnormal lining of the cleft was identified bilaterally and used for the proposed neocommissure. The final position of the neocommissure was confirmed based on its symmetry. Subsequently, an incision was created around the cleft (Figure 1). Medially, the perpendicular incision line linearly transected the dry vermilion, and the incision line ended at the border between the dry and wet vermilion. Laterally, the upper and lower incision lines converged into a point, creating a sharp angle to minimize dog-earing. After undermining the subcutaneous layer, the skin flap around the cleft was flipped intraorally to create the buccal mucosa. The disoriented oricularis oris muscles were identified and minimally dissected for reorientation. Subsequently, the physiological anatomy of the sphincter was reconstructed by suturing the upper and lower stumps of the muscles end-to-end using absorbable sutures. Approximation of the upper and lower vermilion at the point of neocommissure was performed in alignment with the vermilion border. The cheek skin was linearly closed after subcutaneous fat advancement to augment the lateral furrows.
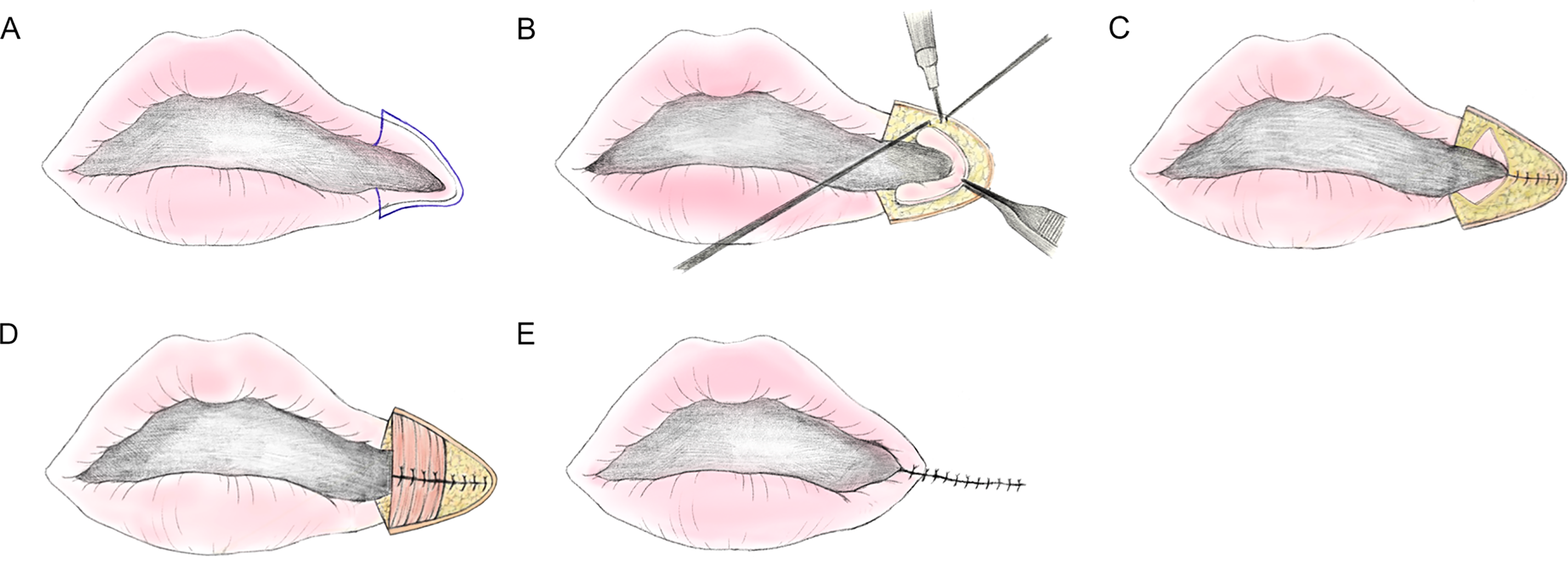
Surgical procedures. (A) The incision line was designed around the cleft; (B) After skin incision, cutaneous flap was dissected to be flipped over intraorally. (C) The flipped flap was sutured, forming the buccal mucosa. (D) Disoriented orbicularis oris muscles were minimally dissected for reorientation. The upper and lower stump of the muscles are sutured in an end-to-end fashion; (E) After approximation of upper and lower vermilion in alignment with the vermilion border,the cheek skin was closed linearly.
Anthropometric Measurement
We exclusively used photographs available in the medical record system. All photographs were taken in a standardized manner by a professional photographer from our department. Anthropometric measurements were conducted by using an on-screen pixel ruler (https://www.rapidtables.com/web/tools/pixel-ruler.html) to the photos in a repose state (Figure 2). Distances from Cupid's bow peak to the oral commissure were measured bilaterally, and the difference between the normal and cleft sides was obtained. The measured difference between the two sides was calculated in proportion to the total lip length (proportional difference [PD]). In bilateral cleft cases, the distance from Cupid's bow peak to the oral commissure was measured bilaterally, and the difference between the right and left sides was consistently obtained.
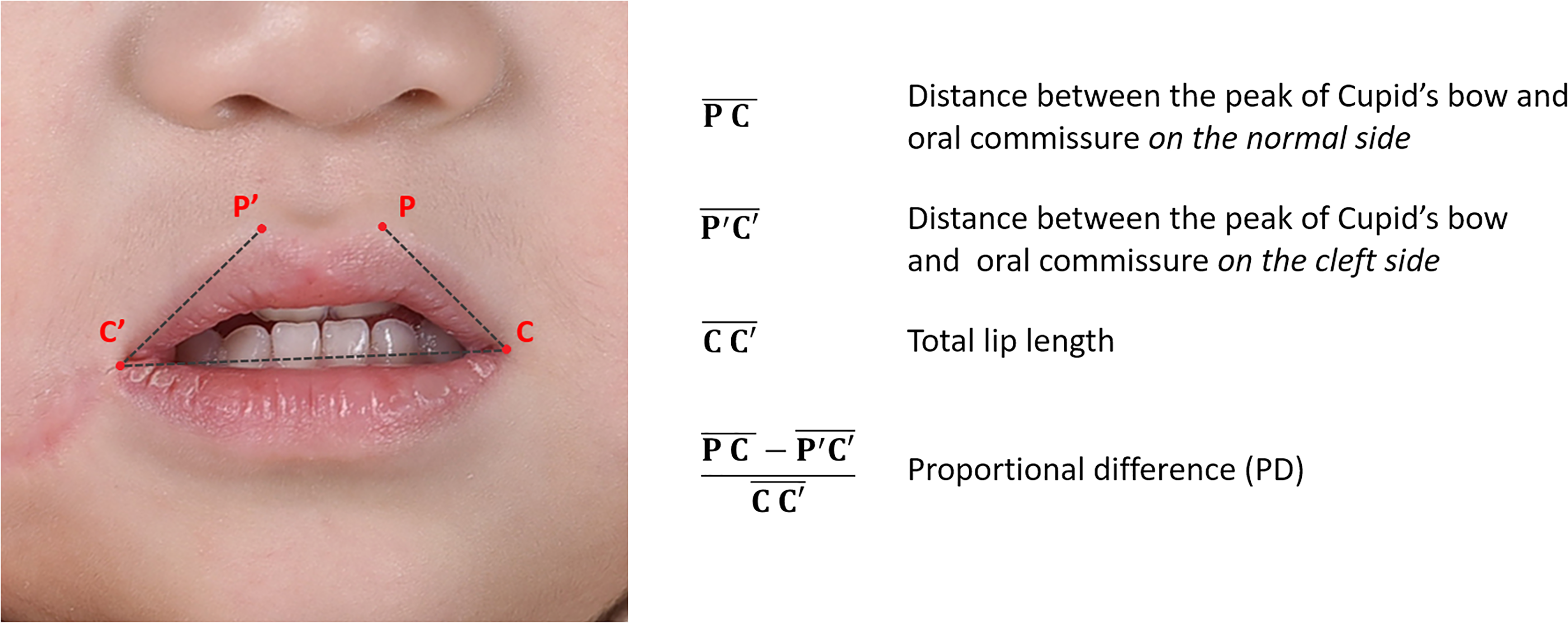
Anthropometric measurements.
Results
Of the 18 patients who underwent transverse facial cleft repair, 6 were excluded because of missing long-term follow-up photographs, and 12 were available for analysis in this study. The characteristics of the 12 patients and their anthropometric measurements are shown in Table 1. Five of the participants were male and seven were female. Regarding cleft characteristics, five were right-sided, five were left-sided, and two were bilateral. Mandibular hypoplasia was observed in seven patients: two with HFM, four with Goldenhar syndrome, and one with micrognathia. The mean age at the time of the transverse cleft surgery was 8.2 months (range, 4 months 10 days to 13 months). The mean follow-up period based on latest medical photographs was 1773.5 days (range, 520-3599 days). The average PD was 4.6% (range, 0.2-7.8%). The result of PD demonstrated that commissural migrations occurred minimally in the long term, and there was no consistency in the direction of the migration in either the cleft or normal side. In patients with a transverse facial cleft crossing the melolabial fold, the folds appeared broken after cleft repair surgery. This difference was significant when the mouth was open (Figure 3). In contrast, in patients with a transverse facial cleft that did not reach the melolabial fold, the folds remained intact after cleft repair surgery.
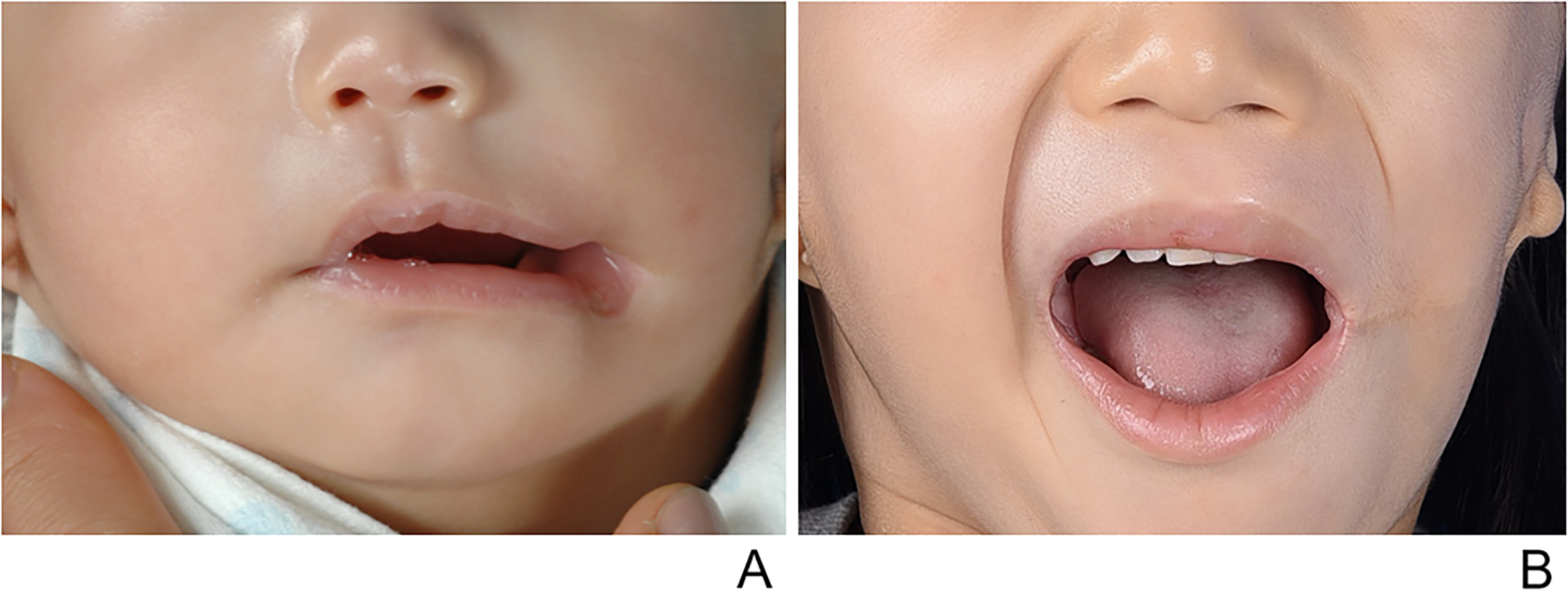
(A) Preoperative photograph of a patient with left transverse facial cleft crossing the melolabial fold at age 5 months. (B) Five years and 6 months postoperatively. The melolabial fold on the left side appeared broken after cleft repair surgery.
Characteristics of the Patients and Anthropometric Measurements.
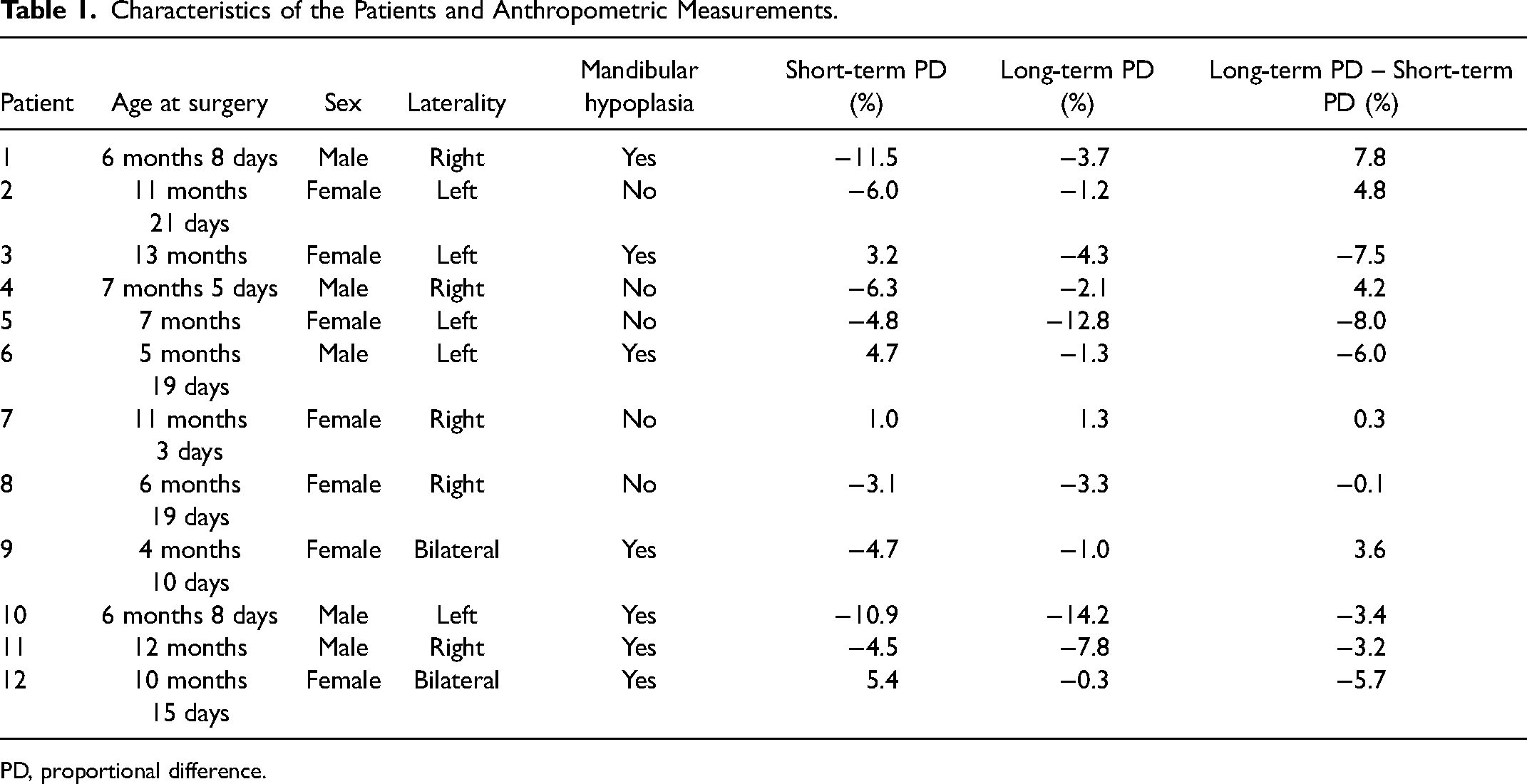
PD, proportional difference.
Discussion
A transverse facial cleft is a rare congenital malformation with an unclear etiology. Several theories explaining its etiological mechanisms have been developed. Embryologically, the mandible and auricle develop from the mesoderm of the first brachial arch. Considering that a significant number of lateral facial clefts are associated with other facial defects including mandibular hypoplasia, microtia and preauricular skin tags, it is plausible that faulty development of the first brachial arch contributes to this malformation. 2 The most commonly associated syndrome is HFM. It is reported that 25% of patients with unilateral transverse facial cleft have HFM, and such clefts have been reported in up to 60% of patients with HFM.3,14 In addition, bilateral transverse facial clefts are more often isolated than unilateral ones. 15 There are theories explaining the pathophysiology of isolated transverse facial clefts.16,17 At week 6 of embryonic development, the maxillary and mandibular processes begin to fuse. Ideas that failure of this may result in a transverse facial cleft were published a century ago, but it is still not fully understood why this occurs. Another theory is that amniotic bands may be responsible for the genesis of the transverse facial cleft.
Since the transverse facial cleft interferes with feeding and causes psychosocial problems owing to disfigurement, early surgical correction is generally recommended. Several surgical methods and modifications have been developed to improve function, shape, and scar formation. Reconstruction of the physiological shape of the orbicularis oris muscle is undoubtedly an essential step in achieving functional recovery. This procedure provides oral continence and counterforce against scar contraction.3,10
Tuersunjiang dissected the zygomaticus major and risorius muscles and overlapped the muscle bundles to imitate the normal modiolus. 18 Meanwhile, Tse et al. refrained from performing excessive muscle dissections to prevent overt tissue trauma and scarring. 19 Instead, they added detail to myoplasty: preservation of the “J” shape of the orbicularis oris contributes to the pout of the lip.
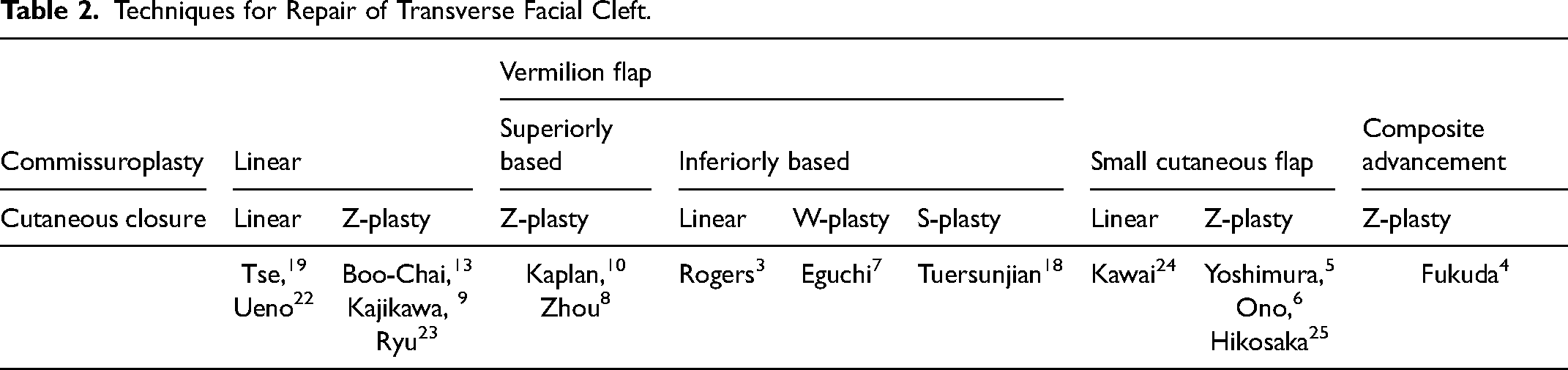
Several authors have considered the natural shape of the oral angle to be a smooth curve rather than a corner.10,20,21 Some are concerned that positioning scars on the commissure may result in further scarring and distortion of the commissural shape.3,4,7 For these reasons, many surgeons have used vermilion flaps to create oral commissures with the development of several modifications. Tse pointed out the complexity and low reproducibility of flap procedures and adopted simple linear commissuroplasty. 19 In this case, only simple linear commissuroplasty was performed, and long-term follow-up revealed the natural appearance of the oral commissure without any distortion or scar thickening (Figure 4). Because our results demonstrated that postoperative changes in the commissural shape and proportional lip length were minimal, the importance of precise preoperative measurements and deliberate design can be emphasized (Table 2).

(A) Bilateral transverse facial cleft with micrognathia. Preoperative photograph at age 10 months. (B) Postoperative photograph at age 5 years. (C) Right transverse facial cleft without mandibular hypoplasia. Preoperative photograph at age 11 months. (B) Postoperative photograph at age 3 years.
Techniques for Repair of Transverse Facial Cleft.
There are also conflicting opinions on cutaneous closure during lateral cleft correction. Many authors have adopted Z- or W-plasty to break scar lines. To camouflage, the central limb of the “Z” should fall into the natural skin folds, such as the melolabial fold. Because skin folds are usually indistinct in young patients, there is a high possibility of faulty positioning which could make the scar more conspicuous. Even in cases with perfect alignment of the central limb, two nearby oblique scars were always present. In addition, a large “Z” on the cheek leaves a conspicuous scar that is more intricate to revise than a linear scar. In terms of symmetry, breakage in the melolabial fold may be a matter of concern. As cheek scars following lateral cleft correction are made via transmural injury, melolabial fold breaking inevitably occurs after the correction of clefts extending over the fold. Performing Z-plasty on transverse scar shifts the direction of tension vertically. This seems disadvantageous, especially in patients with HFM, as vertical tension might shorten the face. Despite these shortcomings, it is reasonable to use Z-plasty to reduce scar length and dog-earing in cases of a length mismatch.
This study had several limitations. The anthropometric measurements based on the two-dimensional photographs we used were less reliable than anthropometry performed on actual human faces or on a three-dimensional photographs. In particular, in syndromic patients featuring transverse facial clefts, such as Goldenhar syndrome and hemifacial microsomia, maxillary or mandibular hypoplasia is highly associated, and the accuracy of two-dimensional measurements can be compromised depending on the presence and severity of the skeletal anomalies.26,27 Because symmetry is perceived as not only confined to the lips but also considers harmony with surrounding structures in the face, lip-only measurements are insufficient, especially in patients with facial asymmetry. There was also no dynamic evaluation, such as during smiling or whistling. A comparison of outcomes between the surgical techniques was not feasible because the same technique was used for all patients in this study. Furthermore, it is necessary to collect patient-reported outcomes of satisfaction with appearance and psychosocial well-being.
Conclusion
By simple linear commissuroplasty and linear cutaneous closure in transverse facial cleft repair, the natural appearance of the oral commissure was achieved, and no significant commissural migration was observed during long-term follow-up. Deliberate positioning of the new oral commissure, proper myoplasty, and meticulous skin closure with minimal scar burden can be considered key procedures for successful transverse cleft repair.
Footnotes
Acknowledgements
The authors would like to thank Da Hyeun Lee, an audiovisual engineer at Samsung Medical Information & Media Services, for providing the medical illustrations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.