
Abstract
Background
The nasal floor and intraoral lining reconstruction of unilateral complete cleft of lip and primary palate has sparsely been reported. Solution: This article combines the previously-described C-flap mucosal flap and inferior turbinate flap with the newly-described lateral nasal mucosal flap for the mucosal repair of this uncommon subtype of deformity. Valuable practical strategies are offered to optimize the surgical execution within a limited pediatric intranasal surgical access, targeting to minimize tissue trauma and bleeding.
Introduction
In the unilateral complete cleft lip repair, the nasal floor and intraoral lining reconstruction has received relatively less attention over time compared to the significance attributed to the cutaneous, vermilion, muscle, and nasal elements.1,2 No consensus exists on the optimal mucosal reconstruction approach, which can range from leaving the raw surface of the dissected pyriform margin uncovered to conducting extensive dissections of the maxillary bone, septum, and buccal mucosal tissue.1,2
For the mucosal repair, Dr. Noordhoff utilized the C-flap mucosal flap (CM flap) in combination with the U-shaped inferior turbinate mucosal flap (T flap), as well as the lateral buccal alveolar mucosal flap (B flap) or lateral buccal mucosal flap (L flap). 3 To preserve the buccal mucosal tissue, Dr. Lo introduced the lateral nasal mucosal flap (N flap) as a replacement for the B and L flaps in the T flap-based mucosal repair of narrow and wide clefts. 4
The technical challenges of harvesting the anteriorly-based T flap within a small intranasal surgical field and the potential risk of mucosal damage and bleeding during manipulation on the delicate and densely vascularized turbinate tissue (Figure 1) could have historically contributed to the limited popularity and scarcity of reports on this flap.1–4 For patients with unilateral complete cleft of lip and primary palate, the utilization of T flap poses additional challenges (Figure 1), particularly due to the absence of a cleft of secondary palate, further narrowing the already limited surgical field. While the literature indicates that T flap harvesting requires an open cleft palate for posterior incision/release, 2 the authors have routinely utilized this technique for repairing unilateral complete cleft of lip and primary palate. Nevertheless, a full explanation of the procedure is still lacking.

(A–D) Schematic drawings and intraoperative image (surgeon view) displaying the anatomical details utilized for creating the inferior turbinate mucosal flap (T flap). (A) The inferior turbinate (B) receives rich vascularity from three main sources: the posterior lateral nasal branch supplies the posterior half of the inferior turbinate, while the anterior lateral nasal branch and lateral nasal branch supply its posterior half. (A) Stars indicate critical areas of potential bleeding during T flap harvesting. (A, D) The T flap is harvested using a three-incision approach. The pyriform margin incision is connected to the inferior border of the turbinate. The inferior incision runs parallel to the lateral nasal wall and joins the vertical incision. The entering point for the superior border incision is the intercartilaginous location, which extends along the superior aspect of the inferior turbinate and continues posteriorly parallel to the lateral nasal wall until reaching the incised vertical part. (A) The width and length of the T flap can be adjusted according to the cleft size. The superior incision is positioned either through the inferior turbinate or at the mucosa superior to the edge of the inferior turbinate for the reconstruction of narrow and wide clefts, respectively. The vertical incision is positioned more anteriorly or posteriorly for smaller or larger vertical gaps, respectively. (C, D) Dashed lines indicate the obstructed region, which may limit visibility and maneuverability.
This article provides a detailed description of our modified mucosal repair technique. It also offers valuable insights and practical tips to optimize its execution.
Preoperative Evaluation
Modified rotation-advancement repair of the lip, along with nasal overcorrection and without periosteal dissection around the alveolar ridges, is indicated at 3 months of age. 4
Mucosal Flaps
Nasal and Intraoral Linings
Children are allowed to breastfeed or bottle feed as soon as they recovered. Oral antibiotics are prescribed for 7 days, with no need for hemostatic agents, nasal packing, or arm splints.
Discussion
The outcome investigation of our surgical approach to treating unilateral complete cleft of lip and primary palate
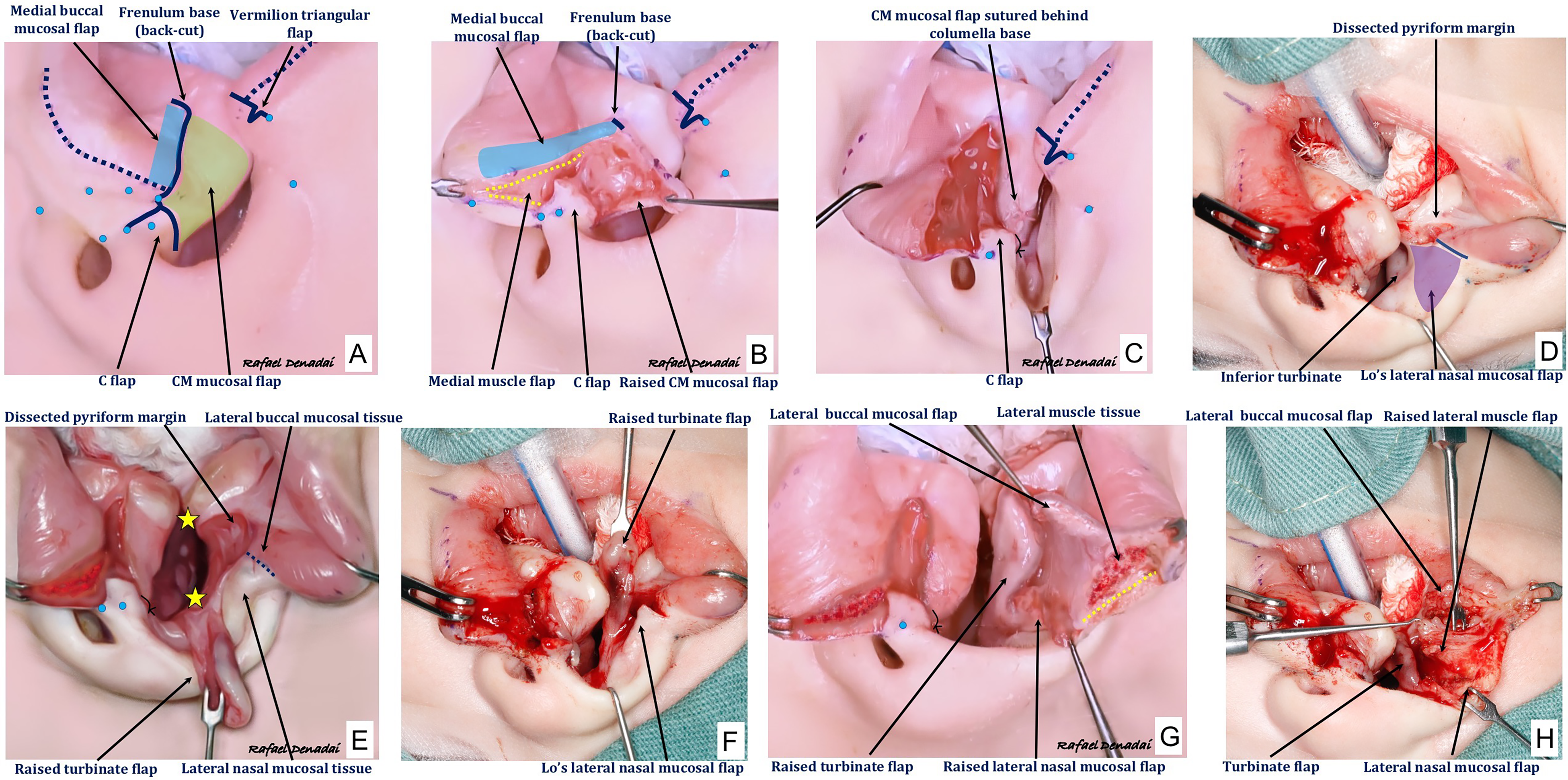
(A-H) Design and harvesting of medial and lateral mucosal flaps shown in (A–C, E, G) schematic drawings and (D, F, H) intraoperative images. (A) Modified rotation advancement principle for medial cutaneous and mucosal markings. (B) Raising the medial buccal mucosal and C-flap mucosal flaps (CM flap) and performing a back-cut at the frenulum base for mucosal lengthening. (C) Suturing of CM flap behind the columella base (5-0 Polyglactin 910). (D) Following the dissection of the pyriform margin, (E) the inferior turbinate flap (T flap) is carefully harvested. The T flap is detached from its inferior, superior, and posterior attachments as well as from the underlying turbinate bone. The mucoperiosteum covering the turbinate is elevated in a posterior-to-anterior direction. The bone of the inferior turbinate is preferably left in place for mucosalization. (D, E) In cases of an intact secondary palate, all scissors-based maneuvers are performed through the cleft. The limited visibility and restricted access in the surgical field can pose challenges in identifying and controlling bleeding. Critical areas prone to bleeding, including the dissected cranial region of the pyriform aperture and the posterior edge of the dissected turbinate tissue, are marked with stars. These sites require special attention for effective hemostasis. (F) The Lo's lateral nasal mucosal flap (N flap) is raised from the underlying orbicularis oris muscle. Wide dissection of (G) mucosa, (H) muscle, and skin is performed to create the three-layered lateral lip element. Courtesy of Rafael Denadai, M.D.
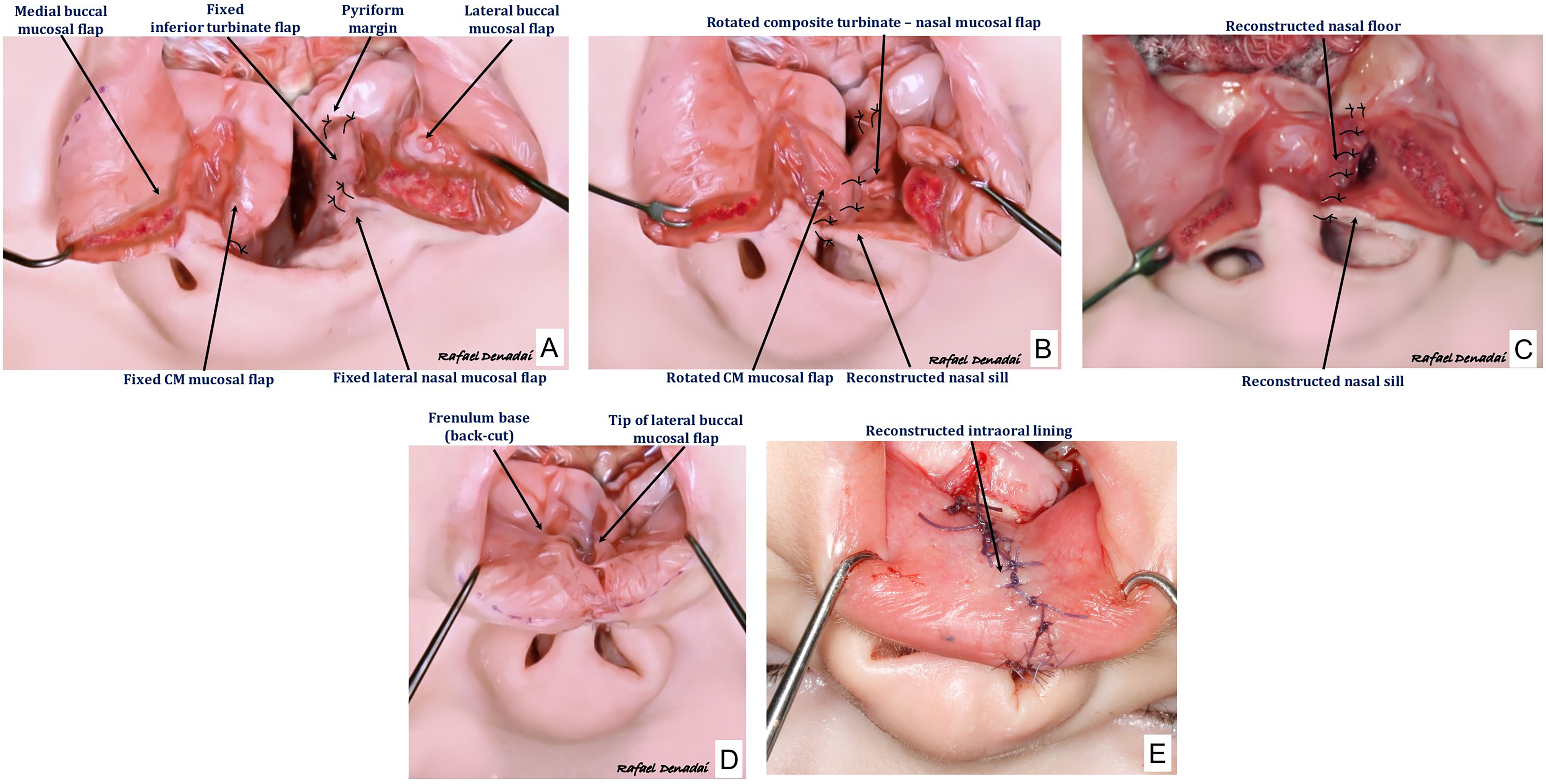
Schematic drawings and intraoperative view showing the modified reconstruction of the nasal and intraoral linings. (A) The tip of the turbinate flap (T flap) is sutured (5-0 Polyglactin 910) to the dissected pyriform margin. The lateral nasal mucosal flap (N flap) is then sutured to the T flap. (B) The composite T-N flap is advanced across the cleft and sutured behind the columella, restoring the nasal sill and equalizing the symmetry in nostril size and lip length on the cleft side. (B) The C-flap mucosal flap (CM flap) and the composite T-N flap are turned and sutured together (C) to reconstruct the nasal floor. (D) The tip of the lateral buccal mucosal flap is sutured to the back-cut at the frenulum base. (E) The lateral buccal mucosal flap is advanced to fit the rotated medial buccal mucosal flap, reconstructing the intraoral lining (labial sulcus). Courtesy of Rafael Denadai, M.D.
Over the years, we have gathered practical measures to improve the operational flow and safety, focusing primarily on the T flap-related issues. Ensure good lighting and magnification (surgical loupes), surgeon positioning in an oblique-cranial view, and delicate hooks-guided lip and nose opening to improve visualization and access to the narrow operative field. Perform careful atraumatic dissection by utilizing finely sharpened delicate scissors and a small double-hook for handling the mucosal tissue, preventing any stretching forces. Ensure that the scissors tip is placed parallel to the lateral nasal wall for both inferior and superior dissections, avoiding any submucous damage. Certify the flap is detached from surrounding connective tissue via the three-incision approach. Complete meticulous dissection until it is only attached anteriorly. The attempt to raise the T flap with grasping forceps should be resisted, as the turbinate is very fragile and can easily be avulsed from the nasal wall. Exercise caution when dividing the bone and mucosal components; if the bone is harvested attached to the mucosal flap, gently open the mucosa like a book and delicately remove the bone in pieces due to the fragility of the mucosa. Perform careful electrocautery needle-based hemostasis after T flap harvest and before its insertion. Avoid handling or suctioning of the mucosal tissue during muscle- or skin-focused tissue dissection, mobilization, and suturing. Gently stabilize the mucosal flap prior to suturing to prevent mechanical damage.
By employing these maneuvers, both novice and senior surgeons have mitigated the occurrence of inadvertent tearing or avulsion of the delicate turbinate tissue and reduced the potential risk of perioperative bleeding in repairing both unilateral and bilateral clefts of lip and primary palate. The described technique and practical strategies could be added to the repertoire of technical maneuvers of surgeons delivering cleft care.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231212264 - Supplemental material for Modified Mucosal Reconstruction in Unilateral Complete Cleft of Lip and Primary Palate: Surgical Technique and Practical Strategies
Supplemental material, sj-docx-1-cpc-10.1177_10556656231212264 for Modified Mucosal Reconstruction in Unilateral Complete Cleft of Lip and Primary Palate: Surgical Technique and Practical Strategies by Rafael Denadai and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
The first author would like to thank the Noordhoff Craniofacial Foundation for their invaluable support in delivering surgical cleft care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The use of human subjects followed an approved protocol or otherwise satisfied the requirement of your IRB and that informed patient/participant consent was obtained. The nasolabial images used in the study have been anonymized, with any identifying features cropped. All drawings and intraoperative images used in this study are credited to Rafael Denadai, MD.
Author Contributions
Study concept and design: Rafael Denadai and Lun-Jou Lo. Acquisition of data: Rafael Denadai and Lun-Jou Lo. Analysis and interpretation: Rafael Denadai and Lun-Jou Lo. All authors read and approved the final manuscript. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.