
Abstract
Objectives
Alveolar ridge defects develop because of surgery, trauma, infection, or congenital malformations. Alveolar ridge defects can be resolved using an osseous replacement. The primary outcomes of osseous replacement are the maintenance of contour; the elimination of dead space, the reduction of postoperative infection; and the increase in bony and soft tissue healing. Recent research shows promising developments in dental bone grafts. This review presents the results of several clinical trials and provides updates on current alveolar bone grafting.
Design
In May 2023, we searched Clinicaltrials.gov for interventional clinical trials related to alveolar bone grafting. A total of 66 clinical trials were included using Boolean Operators AND, OR, NOT we used the “advanced search” option with the search terms [Alveolar Bone Grafting] OR [Ridge Preservation] OR [Dental Bone Grafting] OR [Ridge Augmentation]. Reviewed publications are summarized.
Results
28 out of the 66 trials were successfully completed. None of the trials had offered an invitation to enroll, and only one was terminated. Autograft was the most prevalent kind of grafting, at 28 out of 66, more than twice as prevalent as allograft, which ranked second at 12 out of 66.
Conclusion
this study shows a lack of variety in location, low results provided, and low clinical trials regarding bone rejection. The focus of published trials was mainly on cleft palate rehabilitation using secondary alveolar bone grafting, and the usage of L-prf, rh-FGF-2, rhBMP2, and hyaluronic acid in association with alveolar bone grafting showed remarkable results concerning bone's osteoconduction, osteoinduction, and osteogenesis.
Introduction
Alveolar bone grafting is commonly performed alongside oral and dental surgery, in order to resolve bone defects resulting from surgery, trauma, infection, or congenital malformations. Alveolar ridge defects can be resolved using an osseous replacement. It preserves the alveolar bone contour, which may be lost with the decrease in bone level after teeth extraction. In addition the elimination of dead spaces, presented in cleft palate cases; and the reduction of postoperative infection; and hence the increase in bony and soft tissue healing. 1
In alveolar ridge defects related to congenital malformations, cleft lip and palate cases are the most prevalent craniofacial abnormalities mainly in infant cases, with a prevalence ranging from one per 1000 to one per 650 births. In addition to that, Asian and Male cases were two times more affected than other ethnicities and females respectively. 2 This bone defect can be treated using a secondary alveolar bone grafting with 7-11 years of age an autologous graft, in order to enhance bone level that will in turn support the maxillary primordial canine germ formation, 3 and the permanent dentition positioning 4 and a proper arch morphology 5 that provides support to the nasal alar cartilage, as well as to gain more stable results after orthodontic treatment, 6 and to achieve proper bone levels with attached soft tissue for implant treatment in cases where there is a remaining dental space.7–10 Regarding alveolar ridge preservation and augmentation in preparation to receive a dental implant, bone grafting is essential to minimize the loss alveolar ridge volume after extraction, and the augmentation of ridges pre-implant. 11 Additionally, bone replacement effectively promotes the reconstruction and recovery of periodontal intraosseous defects in patients with severe periodontal diseases, which are accompanied by significant bone loss. 12
Bone grafting is achievable using different types of bone augmentation materials such as autogenous, allograft, xenograft and alloplastic. 1 In 1914, Drachter preformed the first successful alveolar bone graft to an alveolar defect, using an autologous tibial bone graft. 13 The success of bone replacement is based on the acceptance of the graft by the host, depending on the osteoconduction, osteoinduction, and osteogenesis. 14 These histological features can be altered by the graft type and the usage of Factor-based bone graft, Cell-based bone grafts, Ceramic-based bone graft substitutes, and Polymer-based bone grafts. 15
Clinical trials are essential for medical treatment improvement and an opportunity to find more reliable treatments for future outcomes. Not only that, but also approximately 9% of all Alveolar Bone grafting studies published on PubMed since the date of this paper, are clinical trials.16,17 Therefore, the aim of this study is to present the results and analysis of clinical trials, including their updates on alveolar bone grafting.
Methods
Search Strategy and Selection Criteria
Clinicaltrials.gov site provided by the U.S. Library of Medicine is a database collecting clinical studies worldwide, and updated weekly. 17 All submitted trials on this database must provide specific information regarding the trial's history and the protocol of registration. 18
In May 2023, we conducted a search on Clinicaltrials.gov for all clinical trials related to alveolar bone grafting without applying any limitations using the term “alveolar bone grafting” according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses Protocols (PRISMA-P). 19 In the ClinicalTrials.gov registry, using Boolean Operators AND, OR, NOT we used the “advanced search” option with the search terms [Alveolar Bone Grafting] OR [Ridge Preservation] OR [Dental Bone Grafting] OR [Ridge Augmentation]. We collected eighty-one trials from May 2023. We included only interventional, non-behavioral trials related to alveolar bone grafting. Afterward, we excluded 10 no interventional trials, 2 soft tissue grafting trials, 2 behavioral trials, and 1 osteotomy technique trial. This led to a total of 66 clinical trials included in this study (Figure 1). The same methodologies were used in several studies.20–22
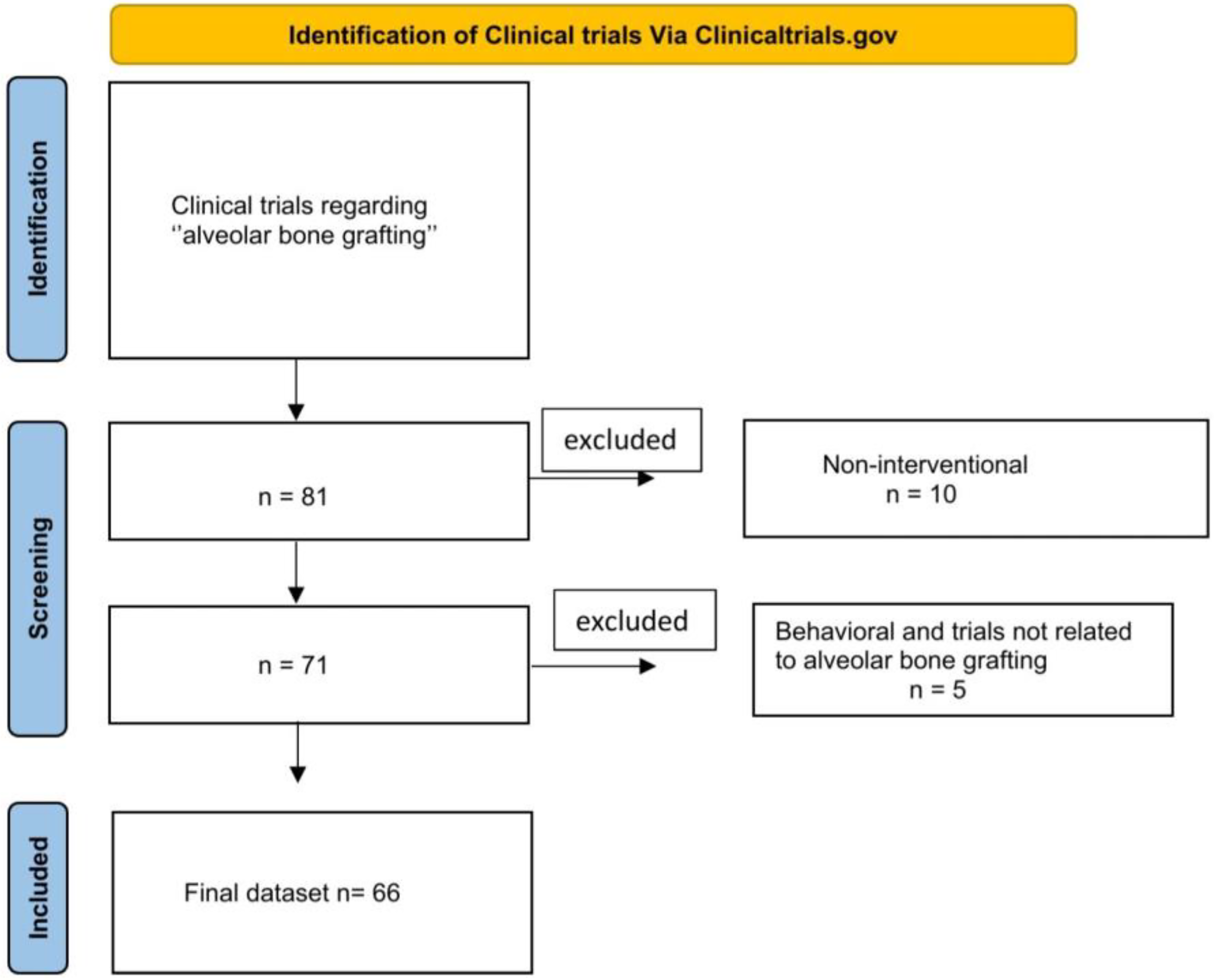
Clinical trial selection process.
Trials Collection
Using Clinicaltrials.gov site all related trials were collected regarding their Phases, trial status, primary endpoints, selection criteria, sample size, study design, experimental interventions, graft type (allograft, autograft, xenograft, alloplastic graft, isograft), trials location, results provided, and any related publication.
Retrieving Publications
Using the NTCID number (registry number), we searched two databases (PubMed/Medline and Embase/Scopus) for any corresponding published work, where the number will be mentioned in published articles. The content of publications was reviewed for current updates on alveolar bone grafting, the use of synthetic bone substitutes and the usage of different proteins to enhance osteoinduction and healing. The main findings were then summarized. Two investigators (A.A.M and Y.E.M) conducted the search to minimize the possibility of errors.
Ethical Statement and Consent Statement
Ethical and consent statements are not applicable in this study.
Results
Trial Characteristics
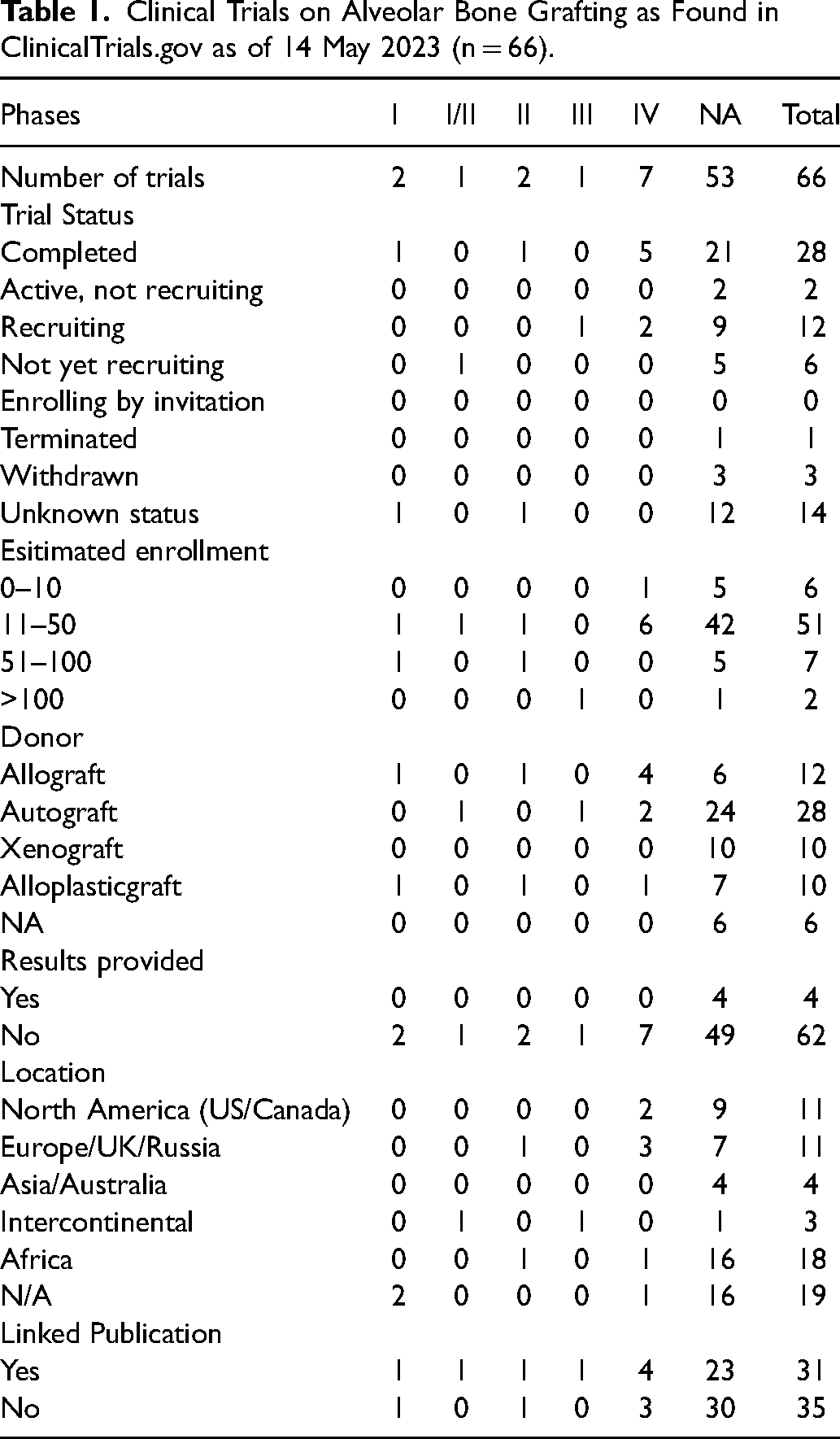
Only 66 clinical trials met the criteria for inclusion in our study. Table 1 displays the distribution of these trials according to the following criteria: phase, trial status, estimated enrollment, donor type, results provided, location, linked publications, and duration. Overall, 28 out of the 66 trials were successfully completed. None of the trials had offered an invitation to enroll in the trial, and only one was terminated. In 51 trials, the numbers of participants ranged from 11 to 50, from 51 to 100 in 7, fewer than 10 in 6, and only in 2 trials were there more than 100 participants. Autograft was the most prevalent kind of grafting, at 28 out of 66, more than twice as prevalent as allograft, which ranked second at 12 out of 66. An unknown method was employed in only six of the studied trials. Xenografting and allografting accounted for the same number of cases, 10 each out of the 66. Only 4 trials provided results, in addition 14 trials showed linked publications. As for trials’ locations, 18 were carried out in Africa and 19 took place in unknown region. The same number of trials, 11, was reached in North America (US and Canada) and Europe/UK/Russia. The 66 trials were distributed among different phases, of which 53 were not applicable (NA). A total of 2336 participants were enrolled in these trials, with 1847, of them in an unknown phase (Figures 2 and 3).
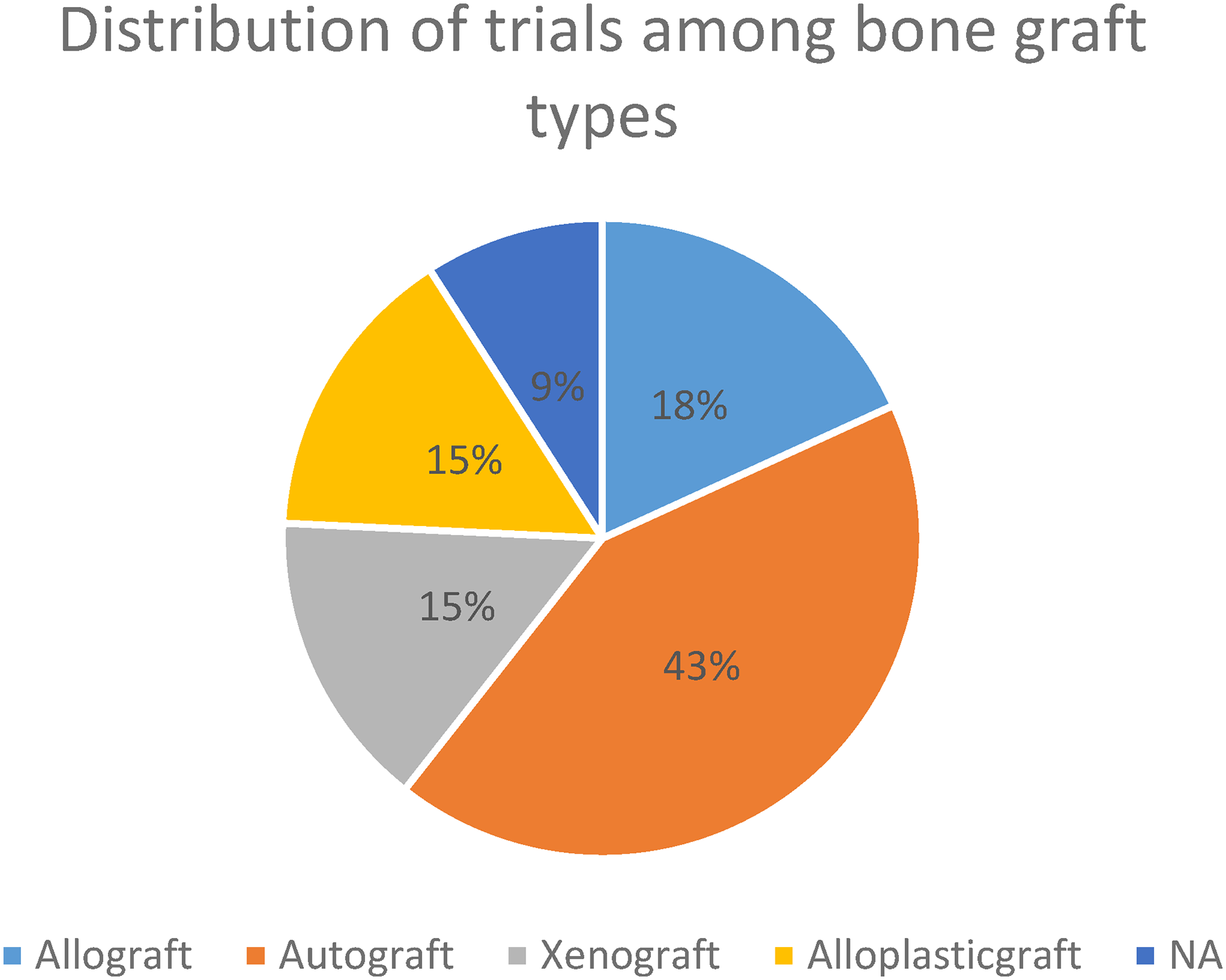
Distribution of trials among bone graft types.
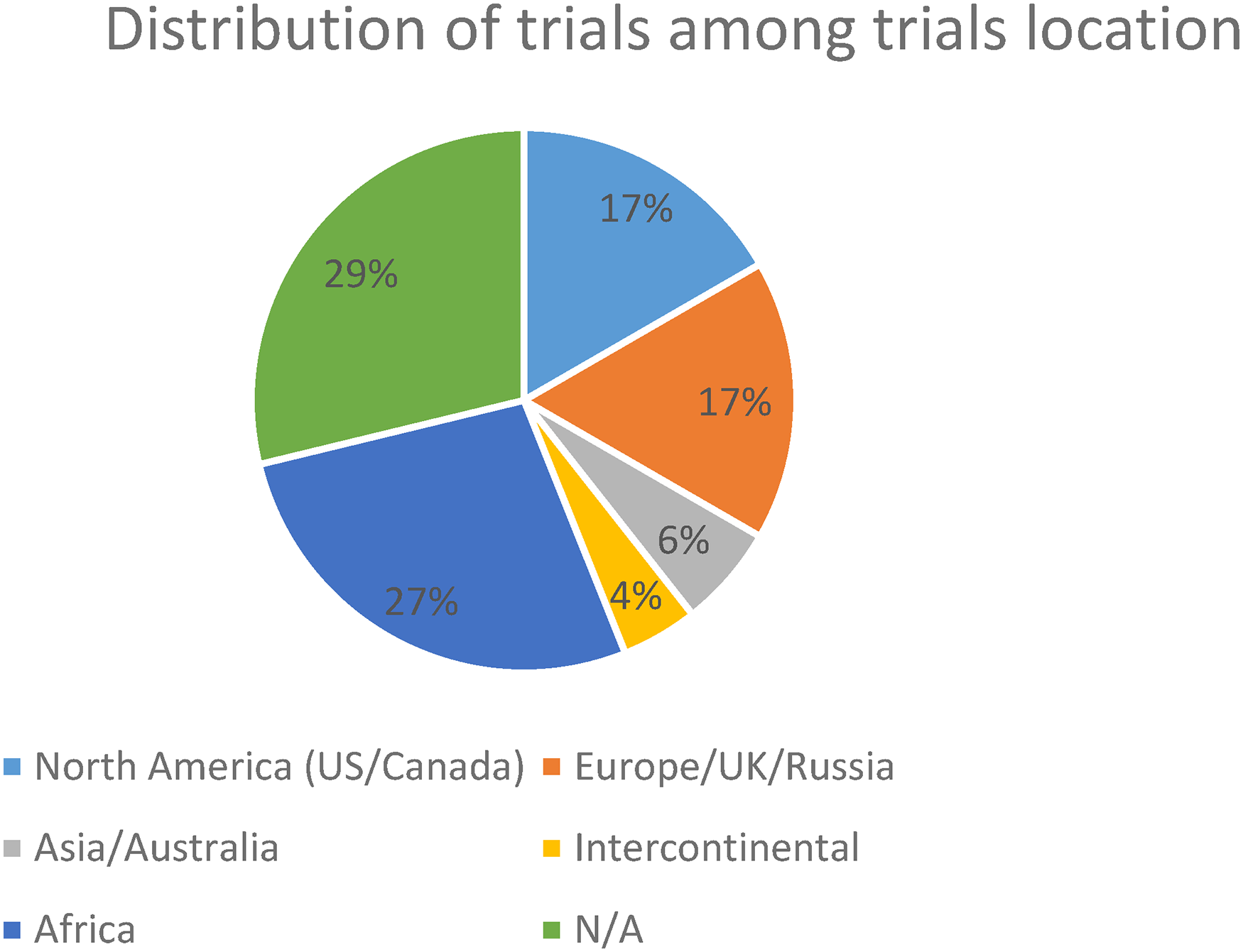
Distribution of trials among trials location.
Clinical Trials on Alveolar Bone Grafting as Found in ClinicalTrials.gov as of 14 May 2023 (n = 66).
Phase I Trials
Only two trials, one completed and one whose status is unknown, were phase I trials. One of them had between 11 and 50 participants, and the other had a minimum of 51, not exceeding 100. These two trials had different methods of grafting: one allograft and one alloplastic graft. Both trials were carried out in unknown regions, lasted between one and four years, and had results provided, one with linked publications and the other without.
Phase II Trials
Two trials were in phase II, of which one was completed and the other had an unknown status. One had between 11 and 50 participants, and the other had between 51 and 100. These two trials used different grafting techniques, one using an allograft and the other an alloplastic graft. Both trials lasted between one and four years, accounting for an average of 4.5, and both didn’t have results provided. They differed in terms of location, with one carried out in Europe/UK/Russia and the other in Africa. Additionally, one of these two trials had linked publications, whereas the other did not.
Phase III Trials
Only 1 out of the 66 trials, with an active but not recruiting status, is in phase 3. More than 100 people participated in this autografting trial. This intercontinental trial provided results with linked publications and lasted between 5 and 9 years.
Phase IV Trials
Phase IV trials included seven, of which five were finished and two were still active and recruiting. Only one of these trials had fewer than 11 participants; the rest ranged in size from 11 to 50. These trials employed a variety of grafting methods, including four allografts, two autografts, and one alloplastic graft. All these trials had results provided, but only one had linked publications. These trails were carried in different regions, with two in North America (US and Canada), three in Europe/UK/Russia, one in Africa, and one in an unknown region. An average of 3.5 years was recorded by these seven trials, with only one trial lasting more than four years.
Unknown Phase Trials
The majority of the trials had an unknown phase. These trials varied widely in terms of status, with none enrolling by invitation. Between 11 and 50 people participated in 42 trials, and only one trial had more than 100 participants. Regarding grafting methods, 24 trials used autografting, 10 xenografting, 7 alloplastic grafting, 6 allografting and 6 trials did not provide what type of graft; the majority of these unknown trials had neither results provided nor publications linked, 49 and 44, respectively. The same number of trials, 16, was carried out in Africa and in unknown regions. All these unknown trials provided a specific duration; a time frame between one and four years was recorded in 48 trials, and none lasted more than 10 years.
Publications Linked to Clinical Trials
Qualitative Analysis
A summary of the major findings of each publication is listed below:
Linked publications of clinical trials related to the usage of leucocyte- and platelet-rich fibrin (L-prf), recombinant human basic fibroblast growth-factor (rh-FGF-2), recombinant human bone morphogenetic protein-2 (rhBMP-2), and hyaluronic acid associated associated with alveolar bone grafting (Table 2):
Clinical Findings of Published Trials on the Usage of L-prf,rh-FGF-2,rhBMP-2,and Hyaluronic Acid Associated with Alveolar Bone Grafting, as of may 14, 2023 (n = 5).
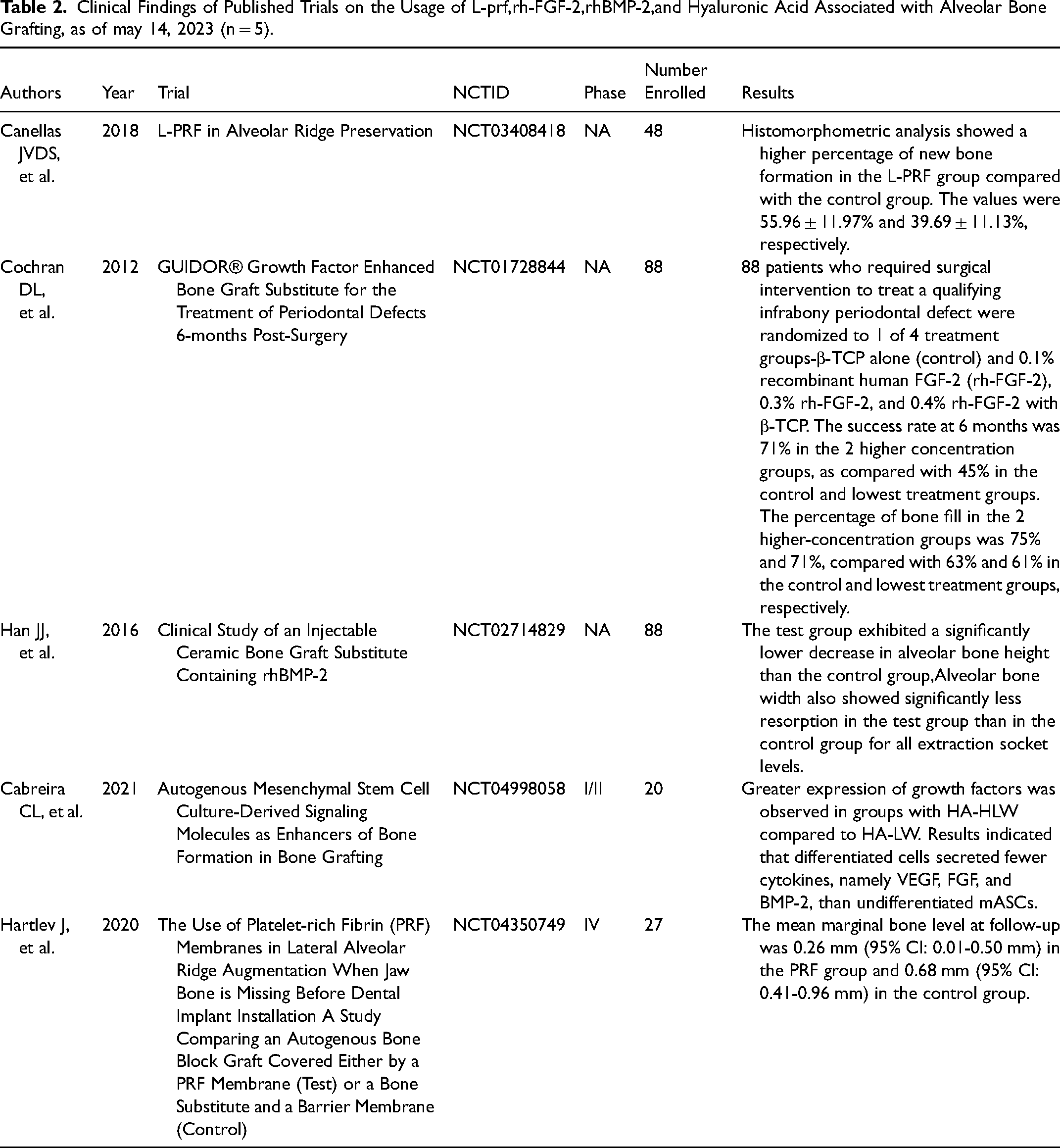
L-PRF in Alveolar Ridge Preservation 23
L-PRF showed a higher percentage of new bone formation (55.96% ± 11.97%) in the alveolar ridge preservation in patients who must undergo tooth extraction under ideal circumstances for receiving dental implants and who had ridge width between the baseline and after three months of healing one mm below the crest. This was in comparison to the control group, which had (39.69 ± 11.13%).
GUIDOR® Growth Factor Enhanced Bone Graft Substitute for the Treatment of Periodontal Defects 6-Months Post-Surgery 24
To enhance bone graft substitutes for the treatment of periodontal defects, a growth factor was used. A sufficient amount of keratinized tissue was used to allow complete tissue coverage of a 4 mm or greater intrabony defect with at least one bony wall after a surgical debridement. The four treatment groups, β-TCP alone (control), 0.1% recombinant human FGF-2 (rh-FGF-2), 0.3% rh-FGF-2, and 0.4% rh-FGF-2 with β-TCP, were randomly assigned to 88 participants who needed surgical attention to repair a qualifying infrabony periodontal lesion. In comparison to 45% in the control and lowest treatment groups, the success rate at six months was 71% in the two higher concentration groups. In contrast to the 63% and 61% in the control and lowest treatment groups, the percentage of bone fill in the two higher concentration groups was 75% and 71.2%, respectively.
Clinical Study of Injectable Ceramic Bone Graft Substitute Containing rhBMP-2 25
When injecting BMP (β-TCP containing rh BMP-2) for socket preservation in people without periodontal diseases, a change in alveolar bone width and resorption was noticed. As compared to the control group, a significant low resorption in the tested tube of the alveolar bone width was recorded compared to that of the control group.
Autogenous Mesenchymal Stem Cell Culture-Derived Signaling Molecules as Enhancers of Bone Formation in Bone Grafting 26
Targeting patients older than 35 years, presenting a highly atrophic edentulous maxilla (residual bone height < 5 mm), in need of bilateral sinus floor augmentation, aiming for a mouth full of implant-supported rehabilitation, and having teeth extracted at least 8 weeks prior to bone augmentation, changes in bone density and quantity were assessed. Groups with HA-HLW showed greater expression of growth factors compared to HA-LW upon usage of autogenous mesenchymal stem cell culture-derived signaling molecules as enhancers of bone formation. These results demonstrated that differentiated cells secreted fewer cytokines, namely VEGF, FGF, and BMP-2, than undifferentiated mASCs.
The Use of Platelet-rich Fibrin (PRF) Membranes in Lateral Alveolar Ridge Augmentation When Jaw Bone is Missing Before Dental Implant Installation A Study Comparing an Autogenous Bone Block Graft Covered Either by a (PRF) Membrane or Bone Substitute and a Barrier Membrane 27
When using platelet-rich fibrin (PRF) membranes in lateral alveolar ridge augmentation with a missing jaw bone before installing a dental implant, several changes were noticed in comparison to the control group. Differences in the augmented volumetric bone, tissue components, and implant survival between the tested and control groups were recorded, with a mean marginal bone level of 0.26 mm (95% Cl: 0.01-0.50 mm) in the PRF group instead of 0.68 mm (95% Cl: 0.41-0.96 mm) in the control group.
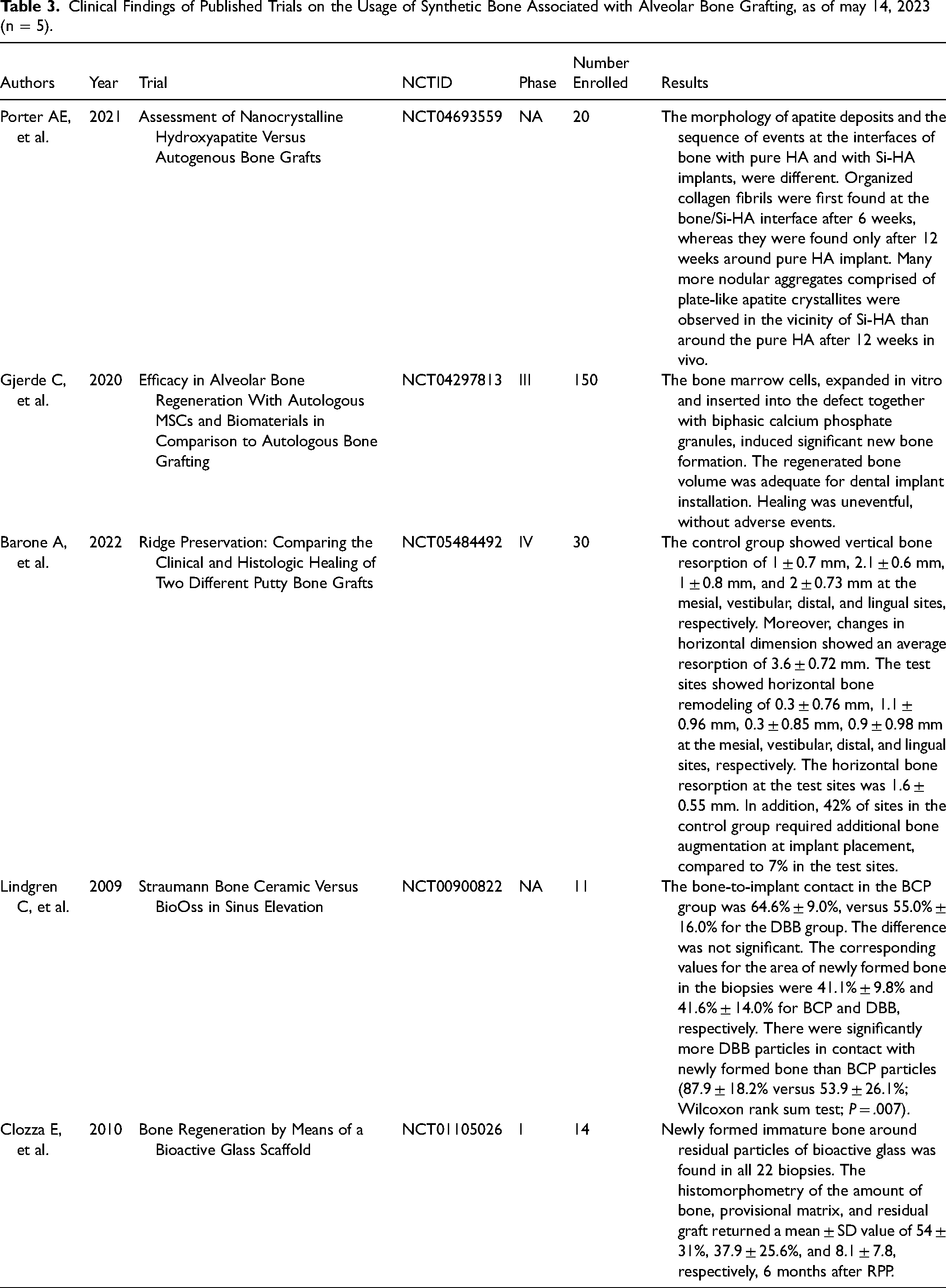
Linked publications of clinical trials related to the usage of synthetic bone materials in alveolar bone grafting (Table 3):
Assessment of Nanocrystalline Hydroxyapatite Versus Autogenous Bone Grafts 28
Based on studies, autogenous and nanocrystalline hydroxyapatite bone grafting revealed distinct outcomes when tested in patients aged between 7 and 12 years with nonsyndromic CLA and CLP and monitored for more than 6 months. Findings demonstrated the presence of organized collagen fibers at the bone/Si-HA interface after 6 months, which were found only around the pure HA implant around 12 months. On the contrary, more nodular aggregates made of apatite crystallites that resemble plates were seen close to the Si-HA than pure HA.
Efficacy in Alveolar Bone Regeneration With Autologous MSCs and Biomaterials in Comparison to Autologous Bone Grafting 29
Prior to receiving dental implants, healthy, nonsmoking patients with a decrease in vertical height and less than 4 mm in lateral width had their jawbone examined using a mix of autologous mesenchymal stem cells and biomaterial. When bone marrow cells and biphasic calcium phosphate granules were inserted into the lesion, a significant amount of new bone growth was generated. This amount was sufficient for placing dental implants.
Ridge Preservation Comparing the Clinical and Histologic Healing of Two Different Putty Bone Grafts. 30
After the healing of the two different putty bone grafts, a change was detected in terms of vertical and horizontal bone resorption. Patients having a non-molar tooth requiring extraction showed vertical bone remodeling of 0.3 ± 0.76 mm, 1.1 ± 0.96 mm, 0.3 ± 0.85 mm, and 0.9 ± 0.98 mm, less than the control group, which showed 1 ± 0.7 mm, 2.1 ± 0.6 mm, 1 ± 0.8 mm, and 2 ± 0.73 mm at the mesial, vestibular, distal, and lingual sites, respectively. Also, a horizontal dimensional decrease was noticed in the tested group, reaching 1.6 ± 0.55 mm compared to 3.6 ± 0.72 mm in the control group. In addition, an additional bone augmentation at implant placement was required by 42% of sites in the control group, whereas it was needed by only 7% of the tested patients.
Straumann Bone Ceramic Versus BioOss in Sinus Elevation 31
Patients expected to present a bilateral bone defect in the sinus area, both needing floor augmentation, were under a randomized and controlled clinical study aiming to compare bone formation around micro-implants in the maxilla. After this augmentation, no significant difference was noticed when the bone-to-implant contact was made with the BCP and DBB groups, reaching 64.6% ± 9% versus 55% ± 16% and corresponding to 41.1% ± 9.8% and 41.6% ± 14%, respectively, for the area of newly formed bone in the biopsies. Regarding particles in contact with the newly formed bone, a significant increase was noticed with DBB particles compared to BCP particles, with 87.9 ± 28.2% and 53.9 ± 26.1%, respectively.
Bone Regeneration by Means of a Bioactive Glass Scaffold 32
In all 22 biopsies of systemically healthy patients without any medical history or smoking habits, immature bone was found around residual bodies. 6 months after RPP, the histomorphometry of the amount of bone, provisional matrix, and residual graft returned to a mean ± SD value of 54 ± 31%, 37.9 ± 25.6%, and 8.1 ± 7.8%, respectively, by means of a Bioactive Glass Scaffold.
Discussion
The presented results summarized the status of clinical trials related to “alveolar bone grafting”. Regarding craniofacial rehabilitation and oral procedures alveolar bone grafting plays a crucial role, therefore an updated clinical trials review is important to introduce new details on alveolar bone grafting and updated technics, in order to ameliorate its therapeutic outcomes in craniofacial and oral surgeries.
Clinical Findings of Published Trials on the Usage of Synthetic Bone Associated with Alveolar Bone Grafting, as of may 14, 2023 (n = 5).
Concentrated Geographic Territory
27% of clinical trials were conducted in Africa, mainly in Egyptian facilities, overtaking the USA, Canada, and Europe with 17% for each. This high rate of clinical trials coincides with the high rate of cleft cases in Egypt (1 in 750), 33 these results showing similarity with several publications,34–36 In contrast with lung and liver transplant rejection publications,20,21 this stunning finding demonstrates that developing countries facing limited resources, a poor healthcare infrastructure and a low education level 37 are leading the field of clinical trials regarding alveolar bone grafting.
Distribution of Trials and Patients on Phases
Half of the trials were in the “not applicable” phase, which had the highest number of participants, shedding light on the low number of meaningful studies done on alveolar bone grafting. 38 Therefore, newer trials should be managed with known phase's status in order to introduce more reliable trials.
Low Published Results
Only four clinical trials provided results regarding their primary outcomes. Moreover, 24 trials had published work in opposition to lung and liver transplant rejection. Several studies discussed why few trials provide their results or publish their outcomes, according to Anderson ML et al., the low number of published data maybe due to negative outcomes obtained or the authors showed no curiosity to publish their outcomes. This lack of results may negatively affect the medical staff and patients.39–41
Therapeutic Benefit
We cannot deny the importance of bone grafting and the successful results it has brought to the medical field, therefore introducing several materials to enhance bone augmentation and stability. Nevertheless, the choice of bone graft source and the application of growth factors differ in the regard of the presented cases, surgical technic, and financial status. Regarding graft material, iliac cancellous bone (autograft) is considered to be the gold standard concerning secondary alveolar bone grafting for cleft lip and palate patients, due to the high concentration of osteogenic cells and biocompatibility, showing a success rate of 89.9% in patients.
On the other hand, though, surgical intervention to obtain the graft material, and the postoperative pain both play a major limitation in the concern of iliac cancellous grafts. 42 Several other alternatives showed promising outcomes, such as the usage of Recombinant human bone morphogenetic protein (rhBMP)-2, and the allograft bovine-derived demineralized bone matrix (DBM) showed comparable results with autografts regarding bone volume, maxillary canine eruption, facial symmetry after secondary alveolar bone grafting, alveolar ridge preservation after extraction and sinus lifting.25,43,44
However, there also are several limitations regarding (rhBMP)-2 such as local gingival edema, and the lack of data regarding long-term evaluations of efficacy and safety of (rhBMP)-2 on children. 45 In addition to that, leukocyte-platelet-rich fibrin (L-PRF) usage regarding ridge preservation and sinus lifting showed moderated and non-significant outcomes regarding bone augmentation and preservation. 46 Therefore, the usage of the graft type and growth factors depends on both, the clinical case, and the desired outcome.
Study Limitation
Our study targeted clinical trials that explored patients who had alveolar bone grafting exclusively and published on ClinicalTrials.gov. Despite taking many precautions and steps to avoid any variety of bias or improper analysis, the validity of our results rests on the validity of the information from the first source, ClinicalTrials.gov. Some data may not be up-to-date, missing, or registered incorrectly, which is the main limitation.
Conclusion
This study is a descriptive analysis of clinical trials targeting alveolar bone grafting. This study shows a lack of variety in location, low results provided, and low clinical trials regarding bone rejection. The focus of published trials was mainly on cleft palate rehabilitation using secondary alveolar bone grafting, and the usage of L-prf, rh-FGF-2, rhBMP-2, and hyaluronic acid in association with alveolar bone grafting. In addition to that, no specific graft type or bone substitute shows the ideal treatment procedures and outcomes in all clinical cases. That being the case, it explains the need to manage further research efforts to bridge in any gaps in alveolar bone grafting; especially in the concern of graft failure, to finally lead to new, affective therapies with minimal adverse effects.
Footnotes
Author Contribution
Conceptualization: A.A.M, Data Curation: A.A.M, M.A.Z, Investigation: P.S, A.M.M, Methodology: A.A.M, Y.E.M, Supervision: P.S Writing – Original Draft Preparation: A.A.M, Y.E.M, M.G, Writing – Review & Editing: M.G, A.A.M.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.