
Abstract
Objective
Cleft-related speech concerns can affect the quality of life (QOL) in patients with cleft lip and palate (CLP). During the coronavirus disease 2019 (COVID-19), in-person speech therapy (ST) was restricted due to fear of getting infected. This study aimed to compare QOL in patients with CLP with and without ST during the pandemic.
Design
Cross-sectional Study
Setting
CLP team at Tehran University of Medical Sciences (TUMS).
Patients/Participants
Thirty-six CLP subjects with a mean age of 17.33 ± 4 years participated in two groups, including with and without ST. Fifteen subjects had cleft palate only (CPO) and others had CLP.
Interventions
ST group received at least 10 ST sessions, and group without ST didn’t receive ST during COVID-19.
Main Outcome Measure(s)
A virtual link of demographic and QOL adolescent cleft (QoLAdoCleft) questionnaires were sent to fill out. Results were extracted and transferred to SPSS.
Results
Total and subscales’ scores of QoLAdoCleft were lower in ST group than without ST but differences between them weren’t statistically significant (P > .05). Furthermore, according to cleft type, there weren’t any statistically significant differences in total, physical, and social subscales of QoLAdoCleft (P > .05); however, psychological subscale in CLP had a higher significant score than CPO (P < .05).
Conclusions
QOL was weak in all patients with CLP, and receiving/not receiving ST couldn’t make noticeable differences between them. It seems; COVID-19 pandemic can have an adverse effect on these results. Also, subjects with CLP had weaker psychological than CPO due to negative psychosocial feedback related to Orofacial deformities received from society.
Keywords
Introduction
In December 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), called coronavirus disease 2019 (COVID-19 a ) emerged. This infectious disease has posed significant health challenges in recent times.1–3 The World Health Organization (WHO b ) declared the COVID-19 outbreak as a pandemic on March 11, 2020, in response to the escalating number of cases and fatalities worldwide. 4 Consequently, governments worldwide implemented various temporary measures, including travel restrictions, closure of schools and universities, lockdowns, and home quarantine, in an attempt to control the spread of the virus.1,3,5,6 The COVID-19 pandemic has had a profound impact on healthcare services, causing significant disruptions. One of the consequences is that individuals have become hesitant to seek in-person medical services, due to the fear of contracting the virus. In-person medical services have been defined as services held with a patient physically present in the medical setting, not on the internet or by phone or video link. Rehabilitation sessions can be an example of in-person services. Therefore, this reluctance to receive in-person medical services has been particularly notable as rehabilitation often necessitates multiple visits per week.7,8
One of the rehabilitation services affected during the COVID-19 era; was speech therapy (ST c ) which is routinely needed for clients with different speech and language disorders to improve their speech function.9,10 it should be noted that in-person ST is the gold standard for treating patients with speech disorders. 11 Some patients didn’t receive ST due to the fear of infection and pandemic protocols such as mask-wearing, which affected in-person ST services during COVID-19. 10 In-person ST intervention primarily relies on the visual-auditory aspect that is also necessary for patients with cleft lip and palate (CLP d ). Extensive emphasis on lip and mouth expression, especially in patients with CLP is necessary for ST sessions, which were restricted during the pandemic due to mask-wearing. 12
CLP is the most common congenital craniofacial birth deformity. 13 People with CLP often need life-long care from infancy to adulthood, 14 however, during the COVID-19 pandemic, their routine of rehabilitative care was interrupted. 15 These patients need to observe and practice the intraoral airflow and correct placement of articulators during ST sessions due to their specific speech problems.16,17 It is reported that mask-wearing throughout the ST sessions for patients with CLP can pose several issues. 10 First, as mentioned before, one of the crucial aspects of ST sessions of patients with CLP is modifying the airflow pathway during speech production that can be affected by obstructed facial and oral view of the speech therapist by mask during COVID-19. This issue can affect the quality of providing ST tasks. 10 Second, in patients with CLP tensor palatini and levator palatini muscles’ deformities lead to dysfunction in the Eustachian tube and normal ventilation. This deficiency results in otitis media with effusion which can cause some degrees of hearing loss (HL e ). Different degrees of HL in patients with CLP can limit their auditory discrimination and affect their speech function during ST sessions due to mask-wearing.16,18–20 Moreover, the speech therapist sometimes asks patients with CLP to take off their masks to decrease the problems with understanding CLPs’ speech visually and acoustically.10,21 Considering that, patients with CLP suffer from other co-morbidities associated with their Orofacial deformity, like poor general health, medical problems, HL, and sometimes cognitive decline; therefore, a higher risk of COVID-19 infection is expected for them.22–25 Ultimately, each factor that increases the rate of contracting the COVID-19 virus can lead to patients’ fear of getting infected, and make them reluctant to receive and continue in-person services such as ST during the COVID-19 pandemic.26,27
The primary goal of ST in patients with CLP is to increase speech intelligibility, enhance communication skills, and achieve psychological and social well-being. 28 It is hypothesized that the ST sessions’ disruption and unwillingness to receive in-person ST due to the COVID-19 pandemic is a barrier to achieving speech improvements that can influence the quality of life (QOL f ). 9 Previous studies showed that speech and resonance problems in patients with CLP can affect the psychological/ psychiatric aspects, social aspects, self-esteem, perception of well-being, and life satisfaction, and ultimately can decrease the QOL.29–34 Furthermore, issues like CLPs’ aesthetic condition, social stigma, the expectation of better results following surgeries, and the high cost of a wide range of CLPs’ healthcare decrease their QOL significantly.32,35,36
On the other hand, COVID-19 can cause mental health issues such as depression and anxiety, as well as a negative impact on the QOL of patients.37–40 As people are not immune to future infections, it may further decrease their QOL. 41 Patients with CLP face psychological and emotional challenges during their life due to their condition, and the additional challenges associated with COVID-19, such as the fear of getting infected negatively impact their mental well-being. Therefore, previously mentioned reasons can influence their willingness to continue health care services like rehabilitation sessions and ultimately affect their overall QOL and QOL related to disease.7,8,35,42
According to the WHO definition, QOL is defined as a person's perceptions of their status based on expectations, goals, standards, and concerns in the context of the culture and values in their country. QOL can be investigated in different aspects. It is categorized into two main sections, including physical and mental health. 3 Several methods are used to assess health-related QOL, classified into two types of questionnaires including general health-related QOL such as 36-item Short Form (SF-36), and disease-specific QOL like the quality of life adolescent cleft (QoLAdoCleft g ). 43
The previous studies on the QOL of patients with CLP have shown that these patients have weaker scores in different aspects of QOL compared to the non-cleft subjects.29,35,44,45 In a systematic review study, Aljohani et al. (2021) categorized the studies that evaluated the QOL in patients with CLP. They have noted that most patients with CLP have lower general QOL compared to people without CLP in total and subscales’ scores. 35 Considering that the QOL is related to culture and different factors such as language, region, and ethnicity it can affect psychosocial well-being 46 and how people interpret others’ expressions..43,47,48 Regarding the importance of the cultural factors in the QOL, it is necessary to investigate it in different languages and cultures. 46
According to previous studies, any disruption in speech intelligibility in patients with CLP can also affect the QOL.49–51 Therefore, it is necessary to determine the QOL in different cultures and investigate the impact of receiving ST on it. This study was done in Tehran, Iran, and the ST sessions were provided in the CLP clinic of Tehran University of Medical Sciences (TUMS h ). This study aims to 1. Determine QOL in adolescents and young adults with CLP during COVID-19 2. Compare the QOL in adolescents and young adults with CLP with and without ST during COVID-19. The findings of this study can highlight the importance of investigating CLP-related QOL to provide helpful information for accurate evaluation and more effective treatment for patients with CLP.
Methods
Ethical Consideration
The institutional review board of the School of Rehabilitation, TUMS, approved this cross-sectional study (IR.TUMS.AMIRALAM.REC.1400.043). All subjects filled out an informed consent form before participating in the study.
Participants
Thirty-six subjects with cleft palate only (CPO i ) and CLP between 13 to 26 years old (with a mean age of 17.33 ± 4 years) were recruited in the present study. The included subjects were categorized into two groups: the first group comprised 18 patients with CPO/CLP (8 CPO and 10 CLP) with ST, and the second group consisted of 18 patients with CPO/CLP (7 CPO and 11 CLP) without ST during the COVID-19 pandemic.
All participants were selected from the CLP team at TUMS, Tehran, Iran, according to inclusion criteria. A maxillofacial surgeon diagnosed the cleft type of patients, and an experienced speech therapist confirmed it. All the participants of both groups in this study were patients with CLP who were referred to the CLP team of TUMS, and the presence of speech concerns and the need for ST had been documented in their medical records.
The inclusion criteria for subjects who participated in the group with ST were having CPO/CLP, having speech disorder, not having any other syndrome co-occurring with CLP, being in the age range between 13 to 26 years, receiving 10 in-person ST sessions during the COVID-19 pandemic, and not using hearing aids. Due to the lack of access to the subjects and considering the study's limitations during the COVID-19 pandemic, hearing screening was not possible. The hearing status of the participants and whether they received any audiology treatment was determined based on their history and their response. Also, the inclusion criteria for the subjects without ST were similar to those in the ST group except for receiving any type of ST sessions (in-person or telehealth) during COVID-19. In their medical history in the CLP team of TUMS they had speech concerns and had received ST sessions or other medical interventions in the CLP team at least once, but they have not received ST with commencing the COVID-19 pandemic began.
Patients who were unwilling to continue participating in the study, or those who had completed their questionnaires incompletely, were excluded from the study. In the current study, three people from the group with ST and one person from the group without ST were excluded from the study on the basis of incomplete questionnaires.
Questionnaire
In this study, the CLP-related QOL was assessed by the QoLAdoCleft questionnaire, which was first developed and validated by Pasquale Piombino et al. 34 Jafari Rasa et al. (2021) conducted the validity and reliability of this questionnaire in the Persian language. They have reported good face and content validity (CVI = 0.74) for the QoLAdoCleft questionnaire as well as good internal consistency (Cronbach's alpha coefficient = 0.95) and test-retest reliability (ICC = 0.98) in the Persian version. 44
The QoLAdoCleft questionnaire has two main parts; one for a clinical profile, and another for determining physical, psychological, and social health subscales. The clinical profile includes age, gender, cleft type, the date of first surgery, further surgeries, education, and marital status. The second part of this questionnaire consists of 50 questions categorized into three subscales; physical health, psychological health, and social health. The physical health subscale consists of 19 questions that assess different variables including communication, pain, physical function, and general health. Psychological health has 14 questions examining self-concept, behavior, satisfaction with appearance, psychological distress, and cognition. The peer relation, school, family, social support, and social function are determined by the social health subscale in 17 questions.
In the present study, the participants were asked to answer each question with a 5-point Likert scale from 0 to 4 through an online survey. Finally, the total score of QoLAdoCleft is calculated between 0 and 200; in fact, a higher score in this questionnaire in subscales and total indicates weaker QOL related to CLP.
Procedure
This study was done on thirty-six adolescents and young adults with CLP in two groups with and without ST during COVID-19. At first, the patients who matched the inclusion criteria were recruited into the study from the TUMS CLP team. Then through a call, the patients with CLP who had speech disorders in their medical record in the CLP team were asked about their experience of receiving/not receiving ST during the COVID-19 pandemic. The patients who didn’t receive ST were asked about the reasons for not receiving ST. The answers were recorded based on their self-statement. After that, according to their response to the mentioned question about receiving/not receiving ST sessions during the COVID-19 pandemic, they were categorized into two groups in this study including with and without ST.
In the next step, an online link that included two questionnaires was sent to all participants in two groups with and without ST for data gathering. This online link included a brief demographic and medical history questionnaire and the QoLAdoCleft questionnaire. Firstly, the participants were asked to complete a questionnaire comprising demographic features, medical profile, and clinical history. To provide more explanations about the questions asked, an additional box was designed at the end of the demographic data and medical history questionnaire. The participants were asked to fill it out if they want to clarify their answers. For example, the subjects could have provided more details about each answer such as providing the date of each surgery in the box. After completing the demographic data and medical history questionnaire, the online form of the Persian QoLAdoCleft questionnaire was filled out. To fill out the questions of the QoLAdoCleft questionnaire, patients with CLP had to choose a desired answer from multiple-choice answers for each question. This self-assessment questionnaire has 50 questions; each question is scored 0-4. To avoid filling out the questionnaire incompletely, the participants could only go to the next page when they answered the questions on each page thoroughly.
Finally, the results were automatically available to us when the participants filled out their forms and QoLAdoCleft questionnaire. The data was registered with special ID codes to preserve the patients’ security. As the data was received, analyses were conducted on the results. Then the results were transferred to SPSS software version 25.0. In this study, data were collected between December 2021 and November 2022 by the CLP team of TUMS.
Statistical Analysis
In this study, for descriptive data, mean, Standard Deviation (SD), and frequency were reported by descriptive statistical analysis. The one-sample Kolmogorov-Smirnov test was used to determine the normal distribution of data. To compare total and subscales’ scores of the QoLAdoCleft questionnaire results between two groups of patients with CLP, including with and without ST, an independent sample t-test was utilized. Furthermore, the results of the QoLAdoCleft questionnaire were compared according to the type of cleft (CPO vs. CLP).
The statistical analyses were performed by SPSS 25.0, the significance level was set at P ≤ .05, and a confidence interval of 95% was considered statistically significant.
Results
In this study, thirty-six subjects with CPO/CLP participated in two groups, including with and without ST, during the COVID-19 pandemic. The Kolmogorov-Smirnov test demonstrated the normal distribution of the total score of QoLAdoCleft and its subscales in both groups (P > .05). A descriptive analysis of the demographic data was presented in each group in Table 1.
Demographic Characteristics of CLP Patients with (n = 18) and Without (n = 18) ST.
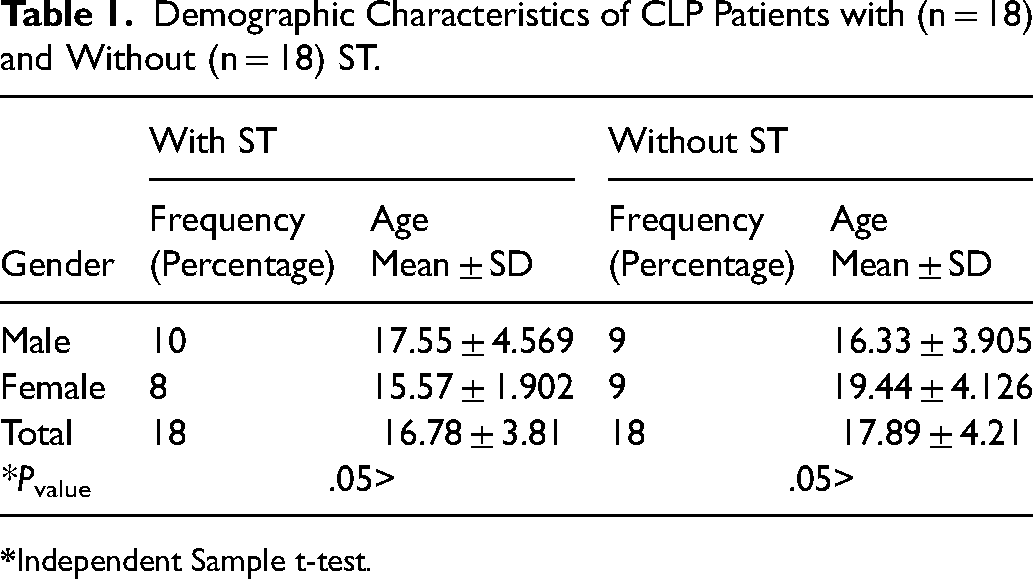
Considering Table 1, subjects who participated in this study were matched in age and gender in both groups (P > .05).
The comparative results of the total and subscales’ scores of QoLAdoCleft in the two groups with and without ST were demonstrated in Table 2.
Comparison the Total and Subscales Score of QOLAdoCleft Questionnaire Between CLP Patients with (n = 18) and Without (n = 18) ST.
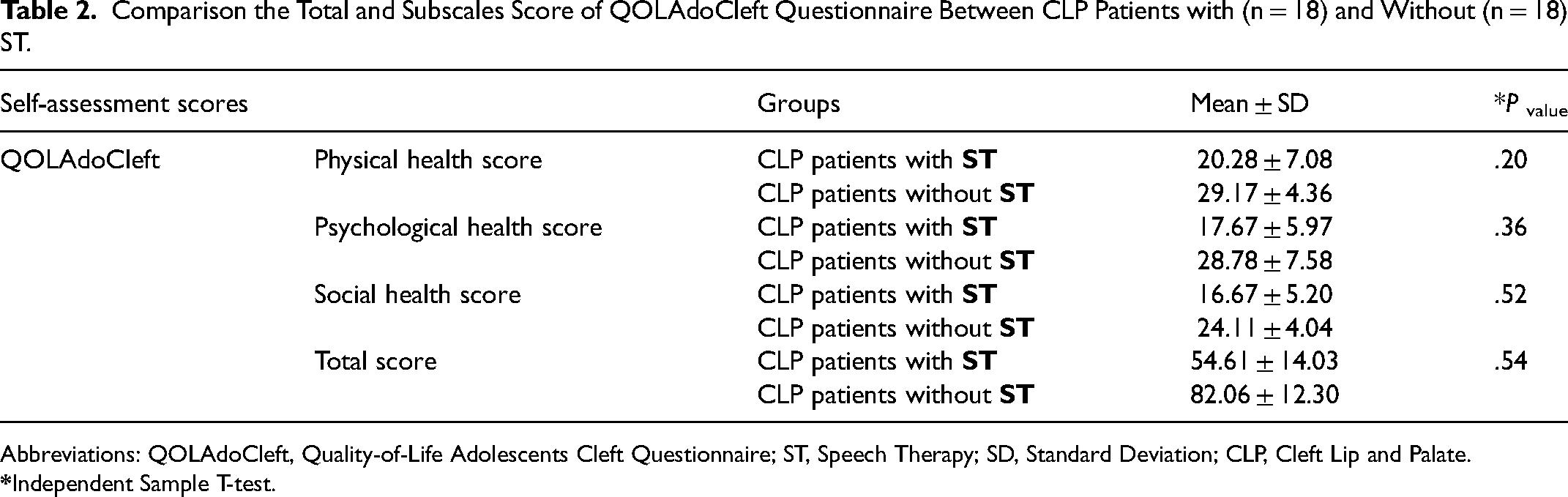
Abbreviations: QOLAdoCleft, Quality-of-Life Adolescents Cleft Questionnaire; ST, Speech Therapy; SD, Standard Deviation; CLP, Cleft Lip and Palate.
As shown in Table 2, the mean of the total score of QoLAdoCleft was 54.61 ± 14.03 in patients with CLP with ST and 82.06 ± 12.30 in patients with CLP without ST. The mean scores of physical, psychological, and social health were higher in subjects with CLP without ST than in subjects with ST. The mean score of the total and subscales’ scores of QoLAdoCleft was lower in the group with CLP with ST than without ST. However, the Independent Sample t-Test results demonstrated no significant difference between the two groups (P > .05).
Moreover, in Figure 1, the results of comparing the total and subscales’ scores of QoLAdoCleft between the two groups were illustrated.
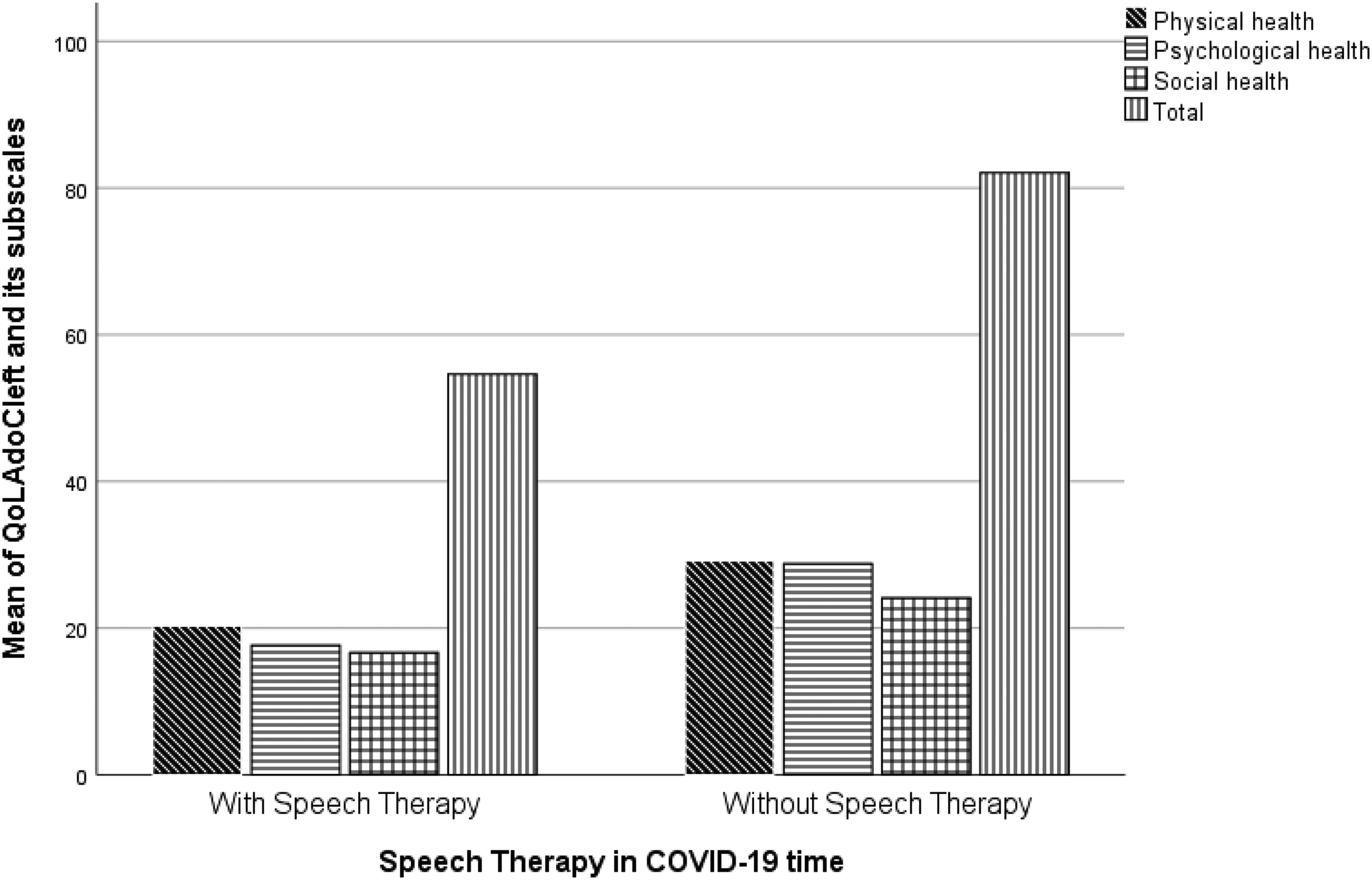
Comparison the total and subscales score of QOLAdoCleft between CLP patients with and without ST.
As shown in the figure, the group with CLP without ST had higher mean scores than the group with ST in total and subscales of QoLAdoCleft. However, the Independent Sample t-Test results showed no significant difference between the two groups (P > .05).
Furthermore, the results of the total and subscales’ scores of QoLAdoCleft were compared according to the type of cleft (CPO only or CLP). The findings are presented in Table 3.
Comparison the Total and Subscales Score of QOLAdoCleft Between CPO (n = 15) and CLP (n = 21) Patients.
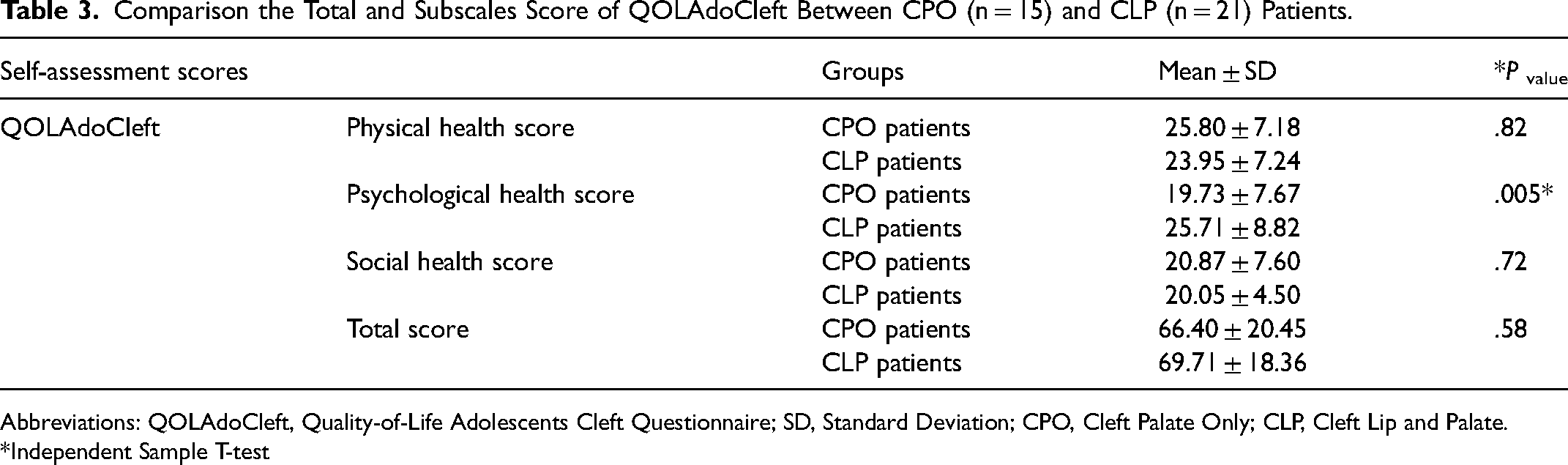
Abbreviations: QOLAdoCleft, Quality-of-Life Adolescents Cleft Questionnaire; SD, Standard Deviation; CPO, Cleft Palate Only; CLP, Cleft Lip and Palate.
*Independent Sample T-test
Table 3 shows no significant differences between patients with CLP and CPO patients in total, physical, and social subscales’ scores of QoLAdoCleft. However, the group with CLP had a higher score in the psychological health subscale than the CPO group, which was statistically significant (P ≤ .05; Table 3). In the following, differences between the two groups according to the cleft type were shown in Figure 2.
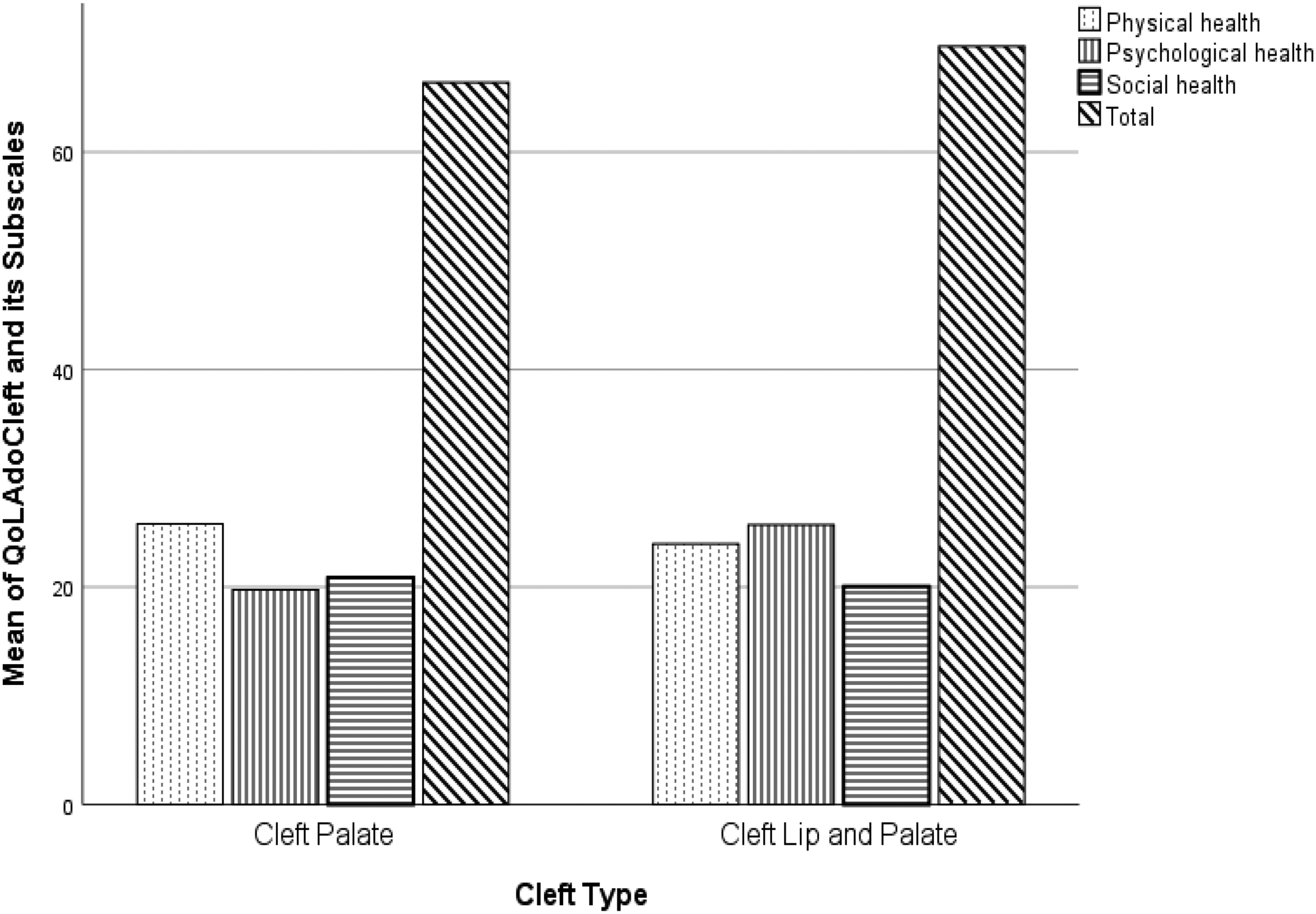
Comparison the total and subscales score of QOLAdoCleft between CPO and CLP patients.
Based on the results shown in Figure 2, the group with CLP had a higher mean score in the psychological health subscale of QoLAdoCleft than the CPO group, which was statistically significant (P < .05).
Discussion
The previous studies noted that the QOL in patients with CLP is negatively affected and decreased due to social, physical, and psychological functions, and Orofacial problems.34,45,52–54 This study aimed to compare the QOL related to CLP in patients who received/did not receive ST during the COVID-19 pandemic. The results showed that the total score of the QoLAdoCleft questionnaire and its subscales were weak in both groups. Moreover, although the score of QOL related to CLP was better in the ST group than the without ST group, the differences were not statistically remarkable between the two groups. Also, in comparison of the total and subscales’ scores of the QoLAdoCleft questionnaire between two groups according to the type of cleft (including CPO vs. CLP), no significant differences were observed between them. Only in the psychological health subscale, the patients with CLP had a higher score than the CPO patients and the difference between the two groups was remarkably significant (P < .05).
As mentioned before, the findings of this study showed decreased QOL in the QoLAdoCleft questionnaire, a specific-disease questionnaire in patients with CLP in both groups, including with and without ST. In the study of Jafari Rasa (2021), they compared the total mean score of the QoLAdoCleft questionnaire between patients with CLP and the control group. The total mean score of the QoLAdoCleft questionnaire was 49.13 ± 8.91 in the group with CLP and 10.64 ± 2.63 in the control group. The difference between the two groups was statistically significant. The group with CLP had weaker QOL than the other group. 44 However, the present study compared the QOL between patients with CLP with/without ST; based on the results, it is notable that QOL was decreased in all participants regardless of receiving or not receiving ST intervention during the COVID-19 pandemic. These findings suggest focusing on different aspects of QOL in all patients with CLP is a critical issue that should not be neglected in ST sessions.35,44,55 It seems that decreased QOL in patients with CLP who participated in this study can be due to Orofacial anomalies, speech difficulties, emotional problems, lowered self-esteem, lower social skills, cultural variation, and ethnic differences following their CLP problem. These results were parallel with the previous studies in this field.35,56–58
A higher risk of depression and anxiety among patients with CLP can cause their higher scores in the psychological health subscale. 59 Moreover, patients with CLP are less satisfied with their appearance, even after many types of treatment. Less satisfaction with their appearance may have a negative impact on their mental health. 60 Furthermore, in previous studies, the psychological subscale's score has been reported as the weakest subscale in QOL questionnaires in patients with CLP, which was in line with our study.34,44 According to the former studies, patients with CLP perceive to be less socially acceptable than their non-CLP peers; therefore, they experience more negative self-perception and subsequently would have weaker social health subscale result.55,59,61 In addition, weaker outcomes in the physical health subscale in patients with CLP may be due to their physical pain such as toothache, earache, and physical disability.14,62 Ultimately, the total and subscales of QoLAdoCleft could be deteriorated in patients with CLP due to the mentioned possible reasons. The results of the previous QOL research in subjects with CLP indicated weaker QOL compared to subjects without CLP, which was parallel with our findings.35,44,63 The studies of Jafari Rasa et al., and Piombino et al., which investigated the QOL with the QoLAdoCleft questionnaire in the adolescents with CLP demonstrated weaker QOL in the group with CLP compared to adolescents without CLP.34,44
It is important to note that the COVID-19 pandemic has led to increased levels of anxiety and depression in many people. 41 For patients with CLP, who may already have been facing psychological and emotional challenges related to their condition, the additional stressors associated with COVID-19 can further impact their mental well-being and overall mental health.29,35,64 Additionally, COVID-19 has resulted in social distancing measures and restrictions on social gatherings, which have increased social isolation for patients with CLP. These individuals may already face difficulties in social interactions, and the pandemic has exacerbated feelings of loneliness and social isolation. All of these stressors associated with COVID-19 had a negative impact on their overall QOL.65–67
Although there were not any remarkable statistical differences between the two groups with and without ST in the total and subscales’ scores of the QoLAdoCleft questionnaire, the ST group had a better mean QOL score than the group without ST during COVID-19. In this study, most of the participants in the group without ST claimed they were anxious to receive their in-person ST sessions due to COVID-19. These patients attributed their anxiety to the high mortality rates, the disease's unknown aspects, and their belief about contracting the COVID-19 infection due to their physical health deficits. As mentioned, This study was conducted during the COVID-19 outbreak in Iran; it seems unwillingness to receive healthcare services during the pandemic led to limitations in receiving necessary medical interventions for patients with CLP. This reluctance resulted in postponed surgeries, delayed orthodontic management, and a reduction in receiving specialized care like ST.27,68 These factors had a negative impact on the overall QOL of patients with CLP. 69 The positive effect of receiving ST during the COVID-19 pandemic may be a potential reason for a better mean QOL score in the group with ST. The ST services are essential for improving communication skills in individuals with CLP. It is crucial to recognize the impact of the COVID-19 pandemic on the relationship between QOL and ST in these patients. ST aims to enhance speech intelligibility, language skills, and overall communication abilities, which can impact the individual's QOL. Effective ST can also enhance social interactions, boost self-confidence, and improve overall well-being. 70 However, the disruption of in-person ST sessions due to COVID-19-related fears and issues prevented many patients from receiving their in-person ST sessions, leading to interruptions in their ST intervention. As a result, this led to inefficient speech improvement, hindered speech progress, and consequently impact their overall QOL.9,71
As mentioned above, there was no significant statistical difference in the physical, psychological, and social health subscales’ scores between the two groups with and without ST. However, the group that received ST had better mean scores in the subscales of QoLAdoCleft than the group that did not receive ST. Speech difficulties are important factors that can impact the subscales of QOL in patients with CLP. 70 Previous studies indicated that speech concerns can affect emotional function and social communication,72,73 which can lead to poor emotional and social health. Since the speech function is strongly related to QOL subscales, the effect of ST on improving these subscales is expected. 70 It is supposed that ST intervention can lead to improvements in psychological health by promoting speech and communication skills, which can decrease anxiety, psychological distress, and depression, and boost self-confidence. This reason leads to a better psychological health subscale's score. Continuing ST sessions during the COVID-19 era could help people with CLP to maintain their engagement in ST intervention, feel less socially isolated, and score better in the social health subscale. Although ST intervention may not directly affect the physical health of patients with CLP, it can be hypothesized that ST's positive impact on mental health, which is linked to physical health, could influence patients’ perceptions of their physical and aesthetic conditions. It seems this reason could have a positive impact on their physical health.
As far as we searched, we didn’t find any study investigating the effect of ST on QOL in patients with CLP during the COVID-19 pandemic. However, Baghban et al. (2021) investigated the impact of intensive ST on the QOL of children with cleft palate using the Persian version of the pediatric QOL (PPedsQL) questionnaire. Pre and post-intensive ST results showed that the total score, emotional, social, and school function subscales of the QOL questionnaire improved after intensive ST. 70 Bruneel et al. found a direct negative correlation between speech output and health-related QOL in patients with CLP; therefore, patients with weaker speech output tended to have lower QOL. 56 Piombino et al. (2014) reported that CLPs’ speech difficulties can be associated with anxiety, depression, and weak self-esteem,. 34 They mentioned the importance of improving speech production in patients with CLP to increase their QOL. 34 Regarding the findings in the literature, psychological support and ST sessions are crucially needed to be considered in the CPO/CLP intervention plans.35,57
Furthermore, in this study, the comparison of the QOL analysis based on the cleft type (CPO vs. CLP) indicated no remarkable statistical difference in total and subscales’ scores of QoLAdoCleft, except in the psychological health subscale. Psychological health was significantly weaker in patients with CLP than in the CPO group. This study suggests that the difference in psychological health based on the type of cleft might be due to the severity of deficiencies in their facial structure. People with CLP feel discomfort and distress depending on the severity of their structural deformities, particularly in their face, and this condition makes them believe that more surgeries are needed to improve their facial structure 34 ; as a result, people with CLP are less confident and less satisfied with their appearance. 44 For these reasons, the psychological health subscale results are not unexpected in CLP vs. CPO. In similar studies, Capelozza Filho et al. (1993) and Hathaway et al. (2011) claimed that differences in cleft phenotype can lead to distinct impairments in aesthetic and functional domains; hence the cleft type was defined as a crucial associating factor in QOL of the patients with CLP which was parallel with our findings.74,75 Moreover, the study of Bos and Prahl (2011) which used the child oral health impact profile (COHIP) questionnaire to evaluate oral health-related QOL (OHRQOL) in adolescents with CLP, has shown a difference based on the cleft type related to HRQOL. 76 However, Klassen et al. (2012) mentioned the impact of the cleft type on HRQOL is still under debate. 36 In conclusion, based on our findings, the phenotype differences in patients with CLP should be noticed for providing efficient ST. Moreover, considering the differences between cleft types, it is necessary to highlight psychological intervention for patients with CLP with a more severe phenotype status.
Conclusion
The results of the present study demonstrated that the specific-disease QOL assessed by the QoLAdoCleft questionnaire was weak in all subjects, and receiving ST couldn’t create a significant difference between the two groups with/without ST during the COVID-19 pandemic. Moreover, comparing the results according to the type of cleft (CPO vs. CLP), showed that the subjects with CLP had weaker scores only in the psychological health subscale compared to the CPO group. Also, no significant differences were found for physical health, and social health subscales between these two groups.
The present study investigated CLP-related QOL in adolescents and young adults with and without ST during the COVID-19 pandemic. This study faced some limitations. Considering that this study was done during the pandemic, it seems the QOL not only can be affected by receiving/not receiving ST during the COVID-19 pandemic but also, the COVID-19 condition itself could affect the QOL. Therefore, it is suggested to perform further studies on this topic. The second limitation is the small sample size due to difficult accessibility to subjects during the COVID-19 pandemic and it seems a larger sample size can create different results and lead to better outcomes in similar situations. It is suggested to perform more studies with larger sample sizes in the future and compare the results between general HRQOL and specific-disease questionnaires in these patients. Furthermore, it would also be beneficial to investigate and compare the impact of telehealth ST services with in-person services because telehealth ST became common for many people worldwide to access these services during the pandemic.
Although there was no significant statistical difference in the three subscales’ scores between the two groups with and without ST, the results of this study showed the group with ST had better scores compared to the group without ST. These findings can indicate the importance of addressing physical, psychological, and social health aspects of QOL in the ST sessions and highlight the need for a multidisciplinary approach to treating patients with CLP. Since the psychological health subscale was affected more than other aspects of our study, referring these patients to psychologists and psychiatrists is necessary. In addition, it is suggested that the process of ST sessions should never be interrupted in similar circumstances in the future, and alternative methods such as telehealth ST should be used to compensate for the limitation.
Footnotes
Acknowledgments
The authors would like to thank Yasamin Molazeinal for native editing the manuscript. Also, we are thankful for all the subjects who participated in our study and all who helped us perform this investigation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tehran University of Medical Sciences and Health Services