
Abstract
Objective
This study aims to investigate genetic association between Non-syndromic Cleft lip with or without palate (NCLP) and 14 specific Single Nucleotide Polymorphism (SNPs) reported to be associated with NCLP from previous Genome Wide Association Studies (GWAS).
Design
A prospective case-control study.
Setting
Ministry of Health (MOH) Cleft and Craniofacial Clinic and Kuwait University.
Patients/Participants
One hundred sixty-four NCLP patients were recruited from MOH Cleft and Craniofacial clinic, and 491 controls from the Kuwait DNA bank established at Kuwait University.
Interventions
Total gDNA was extracted from whole blood withdrawn from patients and genotyped by real time PCR. Hardy-Weinberg Equilibrium was tested, and the set p value for significance (p < 0.05) was adjusted using the Benjamini - Hoochberg procedure to achieve 5% false discovery rate.
Main Outcome Measures
Logistic regression multivariate analysis was used to test statistically significant differences between cases and controls. Genotyping both groups for the variants was determined through the allele discrimination software program.
Results
There was statistically significant difference between cases and controls in relation to two SNPs; LOC102724968 (rs13041247) (MAF cases/control = C (0.28/0.39) OR Homozygous = 1.30; 95% CI = 1.09–1.56, p = 0.0041) and PVT1 (rs987525) (MAF cases/control = A (0.41/0.27) OR heterozygous = 1.48; 95% CI =1.12–1.95, p = 0.0073), increasing the susceptibility to NCLP.
Conclusions
Genetic variations are associated with the occurrence of oral clefts. Customized Next Generation Sequencing (NGS) panel to the Arab ethnicity is encouraged. In Addition, national preconception genetic carrier screening tests should expand to include common craniofacial anomalies.
Introduction
Cleft Lip with or without Palate (CLP) is one of the most common craniofacial anomalies, with a range of occurrence of 0.57–2.5 in 1000 live births globally, 1 and 0.75–2.55 in 1000 live births in Kuwait. 2 Due to this relatively high prevalence in a homogenous population in which consanguineous union is highly practiced, it is imperative to undertake thorough investigations, particularly in terms of genetic studies.
Although the exact etiology of non-syndromic cleft lip and/or palate (NCL/P) remains unresolved, advances in facial clefts research such as Genome Wide Association Studies (GWAS) that examine Single Nucleotide Polymorphisms (SNPs) across the whole genome have identified numerous associated/causative genetic polymorphisms. 3 Those advances provide some explanation of the mechanism of the anomaly. Beaty et al. identified several genetic polymorphisms, including SNPs on chromosome 8q24, IRF6 (1q32.2), MAFB (20q12), and ABCA4 (1p22.1). 4 Furthermore, THADA, EPHA3, DCAF4L2, and SPRY2 were among the genes confirmed as a risk for the occurrence of (NCL/P) reported through a meta-analysis of several GWAS studies. 3 GWAS also confirmed the association of the 8q24 common marker, rs987525, with NCL/P in Caucasians from the USA and Germany.5,6
The Orofacial Facial (OFC) genetics have not been extensively studied in the Arabian Peninsula population, resulting in the under-representation of their data in public repositories. However, a few genetic association studies have been carried out. Alamoudi et al. genotyped and investigated the associations between IRF6 polymorphisms (rs2013162, rs2235375, and rs2235371) and other environmental factors, concluding that the Saudi population exhibited a different genetic etiology of NCL/P compared to other populations worldwide. 7 In their study, the commonly reported associated IRF6 (rs2013162) rare A allele was not shown to be a marker for NCL/P risk. 7 Additionally, VAX gene polymorphisms (rs4752028) and (rs7078160) were found to be associated with NCL/P. 8 Moreover, an investigation of 15 known NCL/P high-risk loci in a Yemeni sample revealed a strong association between CLP and four loci (8q24, 9q22, 10q25, 13q31). 9 Finally, 34 Iraqi families were genotyped for MTHFR (rs1801133), TCN2 (rs1801198), and CBS (rs4920037) polymorphisms, and the associations were analyzed, showing that there was a decreased risk of OFC for children carrying the TCN2 667G allele (P = 0.02). 10
In terms of genetic research related to patients with NCL/P in Kuwait, although a genetic segregation analysis of the families of patients with NCL/P has been performed in Kuwait, showing no strong association between consanguinity and the occurrence of NCL/P in Kuwait, 11 the association of OFC and high-risk genetic polymorphisms has not been investigated. The Kuwaiti population represents an Arab ethnic group in which the genetic makeup is not completely determined, and in which consanguinity is highly practiced, making this population suitable for the investigation of commonly reported causative/associated genetic polymorphisms related to orofacial clefts. 11 Inconsistent findings regarding the association of selected genetic polymorphisms with the occurrence of NCL/P warrant further investigation through reproducibility studies. Therefore, the aim of this study was to investigate the association of 14 high-risk SNPs, previously determined from European and Asian GWAS and candidate gene studies, with NCL/P in the Kuwaiti and Arabian Peninsula population.
Materials and Methods
National Center for Health Information, and Ministry of Health Cleft and Craniofacial Clinic digital records were reviewed to identify patients with OFC diagnosis using the International Classification of Diseases (ICD-10) diagnostic codes for the following diagnoses: bilateral and unilateral cleft lip with or without alveolus (Q360, Q369), unspecified severity and laterality of cleft lip with or without alveolus (Q36), bilateral and unilateral cleft lip and cleft palate (Q370, Q372, Q374, Q371, Q373, Q375), and cleft lip and palate with unspecified severity and laterality (Q379). A total of 3203 patients were identified. Duplicates (426 patients) were eliminated, and contact information was recorded when available (1023 patients). Three attempts were made to contact patients or families via telephone before being marked as unreachable (338 patients). Patients who were relocated out of the country, are known to have syndromic diagnosis, or refused to participate in the study were excluded, and 319 patients agreed to participate in this study, and subsequently attended the Cleft and Craniofacial Clinic to participate in this study. Out of those 319, 193 were from the Arabian Peninsula. Cases with CPO were excluded, 29 patients, since the genetic etiology is different from cases of CLP, 3 which resulted in a total sample size of 164.
All participants agreed to a written informed consent to an institutional review board–approved protocol (IRB# 2017-562). Clinical examinations were conducted, medical records were reviewed, and venous blood was withdrawn and collected into EDTA tubes. The cohort under study was 164 patients with NCL/P (cases) and 491 patients without NCL/P (controls). The cases and controls were matched by sex as the female to male ratio was 1:1.78 in cases and 1:1.31 in controls, and selected from the Kuwait DNA bank established at the Genetic Laboratory in the Department of Biological Sciences, Faculty of Science, Kuwait University. All controls had no medical or family history of OFC and had provided informed consent for use of their samples in genetic studies.
Total genomic DNA (gDNA) was extracted from whole blood for all the collected patient samples by Qiagen GentraPuregen Blood Kit-1000 ml following the manufacturer's instructions. Isolated gDNA samples were analyzed by both qualitative and quantitative measures. Agarose Gel electrophoresis was used to check the quality of the extracted DNA while quantitative analysis was determined by using ND-8000 spectrophotometer and measured at wavelengths 260 nm and 280 nm for concentrations and purity. gDNA was stored frozen at −80 in the Genetic Laboratory in the Department of Biological Sciences, Faculty of Science, Kuwait University
A total of 14 SNPs, that were previously reported with a significant association to orofacial clefts in GWAS and/or meta-analysis studies, were selected (Table 1). These polymorphisms were also selected based on the reported minor allele frequency (MAF); only those identified as “common” (MAF ≥ 0.05) were selected, as a moderate size sample is expected due to Kuwait's small population. This approach is often followed in genetic association studies for other complex traits. 12 The significant findings of this study will be compared to the results reported in the literature of different ethnicities.
Candidate Gene Variants and Their Respective Genes, Chromosomal Location, Variant Type, minor Allelic Frequencies (MAF) and Odd Ratio (OR).
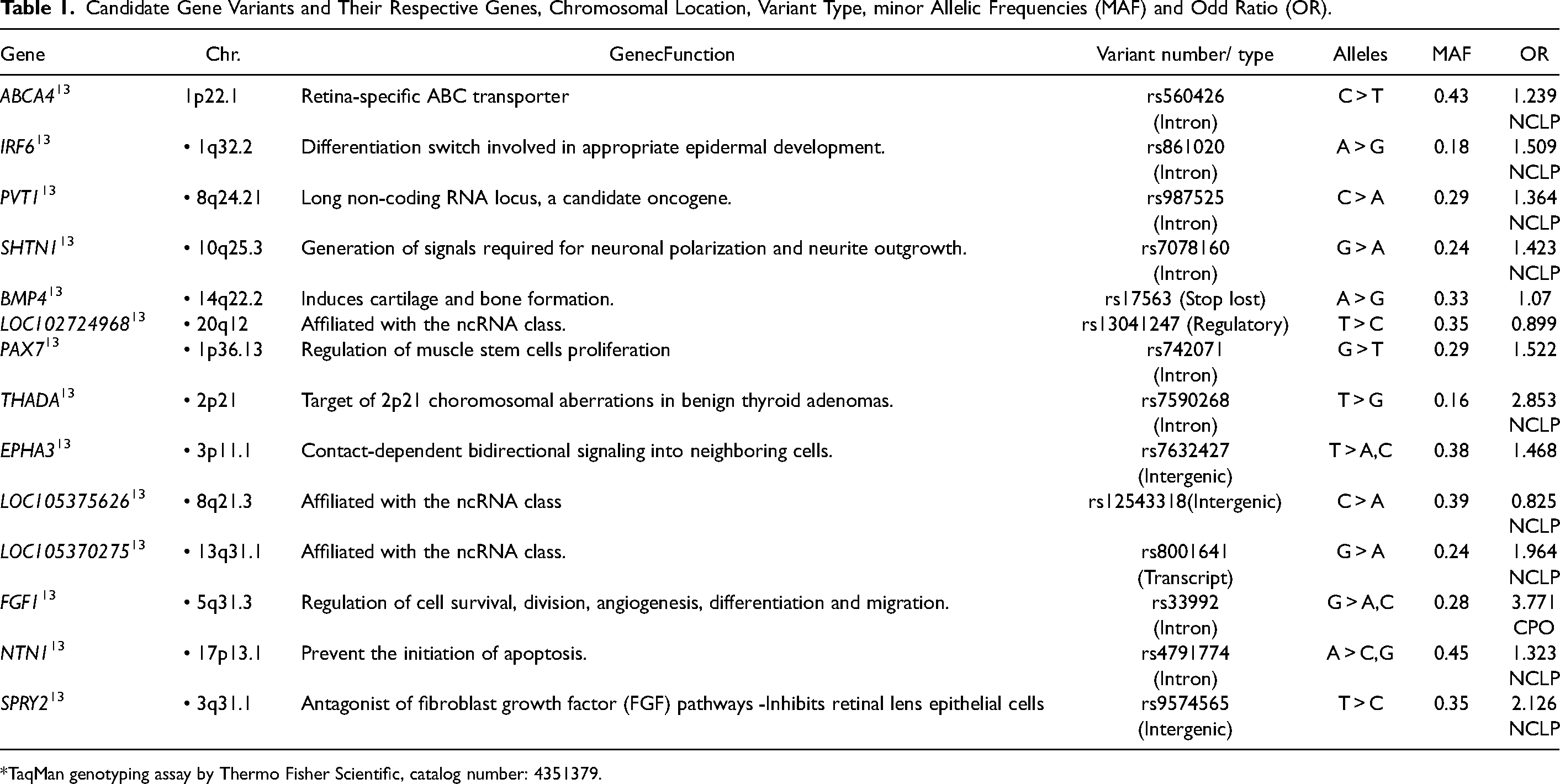
*TaqMan genotyping assay by Thermo Fisher Scientific, catalog number: 4351379.
Genotyping of the selected polymorphisms for the cohort was achieved by using the TaqMan allelic discrimination assay on a real-time polymerase chain reaction (PCR) (Applied Biosystems 9700). For each sample, 10 ng of DNA template was amplified using the applied Biosystems AmpliTaq Gold® Master Mix according to the manufacturer's protocol (GeneAmp™ PCR System 9700 (Applied Biosystems™, Thermo Fisher Scientific, Waltham, MA, USA).
The genotypes were determined by QuantStudio Real Time PCR Software v1.3, which is based on the amplification plots that segregate the three genotype clusters as homozygous wildtype, heterozygous and homozygous mutant alleles. For quality control, 10 random samples were re-assayed as positive controls in subsequent Realtime PCR reactions. The same genotypes were assigned by the realtime software (ABI QuantStudio, ViiA7) in both runs confirming the genotypes determined.
The genotype and allele frequencies were estimated using the basic gene counting method. Deviation from the Hardy-Weinberg equilibrium (HWE) was estimated based on chi-square goodness of fit test using an online software HWE calculator. 14
Initial p-value was set at < 0.05 and was then adjusted using the Benjamini-Hochberg (B-H) procedure to reduce the False Discovery Rate (FDR) to 5%. The B-H adjustment was done on all the likelihood ratio test p-values to reduce the inflated Type I error from multiple testing without being too conservative in a way that increases the Type II error, as with the case of using the Bonferroni correction.
All selected independent variables were entered into a regression model and the effects likelihood ratio test p-values were determined (JMP Pro 16.2.0, SAS, Cary, North Carolina, USA). This was done for one dependent variable comparison: NCL/P versus controls. The independent variables: sex, and the remaining SNPs underwent stepwise regression with a probability to enter and leave at a p-value = 0.1.
Power calculation was performed using Epi Info version 7. 15 The number of cases and controls in this study were sufficient to detect a power of 80% and above at an odds ratio of 2.0 with significance set at p < 0.05 assuming variant exposure in controls was 20%.
Results
Out of 164 patients investigated, 77(47%) presented with cleft lip with/without alveolus only (13 bilateral, 67 unilateral), and those with cleft lip and palate were 87 (53%) (31 bilateral, 56 unilateral). The sex distribution of the total cases was as follows: Fifty-nine were females (36%), while 105 were males (64%). The majority of patients were Kuwaiti (80%), and 20% were non-Kuwaiti Arabs from the Arabian Peninsula. Fifty three percent of the patients’ families were of a consanguineous union. Forty three percent of the patients reported a family history of OFC.
The minor allele (MAF) distribution in the control group is summarized in Table 2. The MAF for the studied SNP's ranged from 0.12 to 0.478 in the studied population. Of the 14 polymorphisms analyzed, the 5 that deviated from the HWE (p ≤ 0.01) were either in the cases sample (rs12543318, rs742071, rs560426), the control sample (rs861020) or the overall cohort (rs7078160) (Table 2). These were all excluded from further analysis to avoid false association outcomes.
MAF Distribution and HWE for the 14 SNPs Genotyped in Cases and Controls (n = 695).
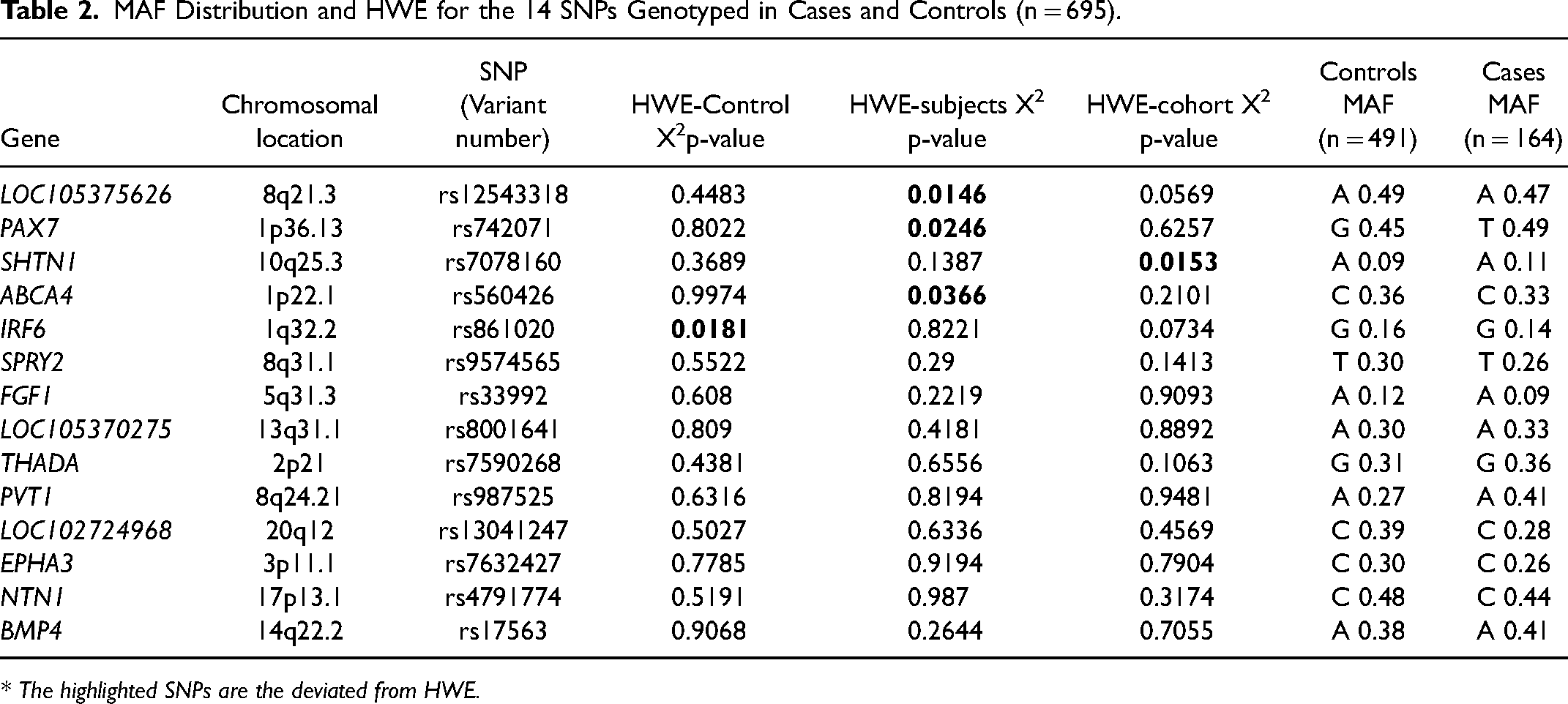
* The highlighted SNPs are the deviated from HWE.
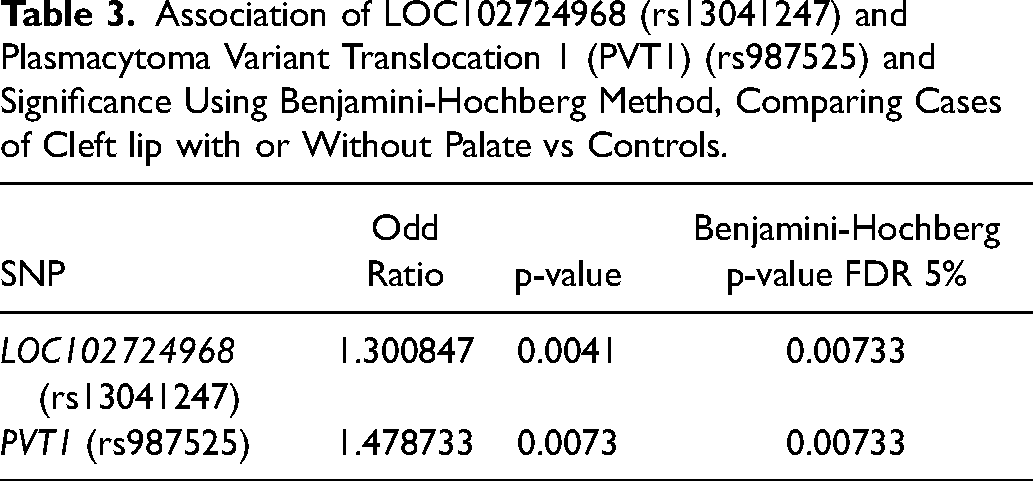
The genotype distribution for the nine remaining SNPs were compared between the controls and cases using a contingency table and the statistically significant difference was determined by multivariate logistic regression analysis test. All independent variables were placed in a stepwise logistic regression model (JMP Pro 16.2). Only two SNPs passed the stepwise regression control with a significant probability of < 0.05. The two SNPs were: LOC102724968 (rs13041247) and PVT1 (rs987525). They were then entered into a logistic regression model and again showed significant association with NCL/P, after B-H correction with 5% FDR that was applied to the p value threshold, as shown in Table 3.
Association of LOC102724968 (rs13041247) and Plasmacytoma Variant Translocation 1 (PVT1) (rs987525) and Significance Using Benjamini-Hochberg Method, Comparing Cases of Cleft lip with or Without Palate vs Controls.
A comparison of the associated SNPs, their frequency distribution, and odds ratio was also compared to other studies with different ethnicities (Table 4). The MAF and association of LOC102724968 (rs13041247) was not statistically significant in the Caucasian population. 16 However, it has been both non-significantly17,18 and significantly19–23 associated in the Asian, South Asian, 24 Middle Eastern,9,25 and mixed26,27 populations, where it had mostly a protective role, which is not consistent with the findings of our study, where it was found to be the risk allele. The MAF (0.41) in the studied cases for the PVT1 (rs987525) SNP was consistent with central European populations6,13,28 as well as with some African populations.29,30 However, the reported MAF and risk scores were lower in other reported populations, such as the Brazilian 31 and Asians. 32 The GWAS analysis of this SNP in the European population indicated a much lower MAF with similar risk scores, further supporting the moderate risk of this SNP in the development of CL/P. 6
Comparison of the MAF and Risk Scores of the Associated Variants with Other Reported Studies from Different Ethnic Groups.
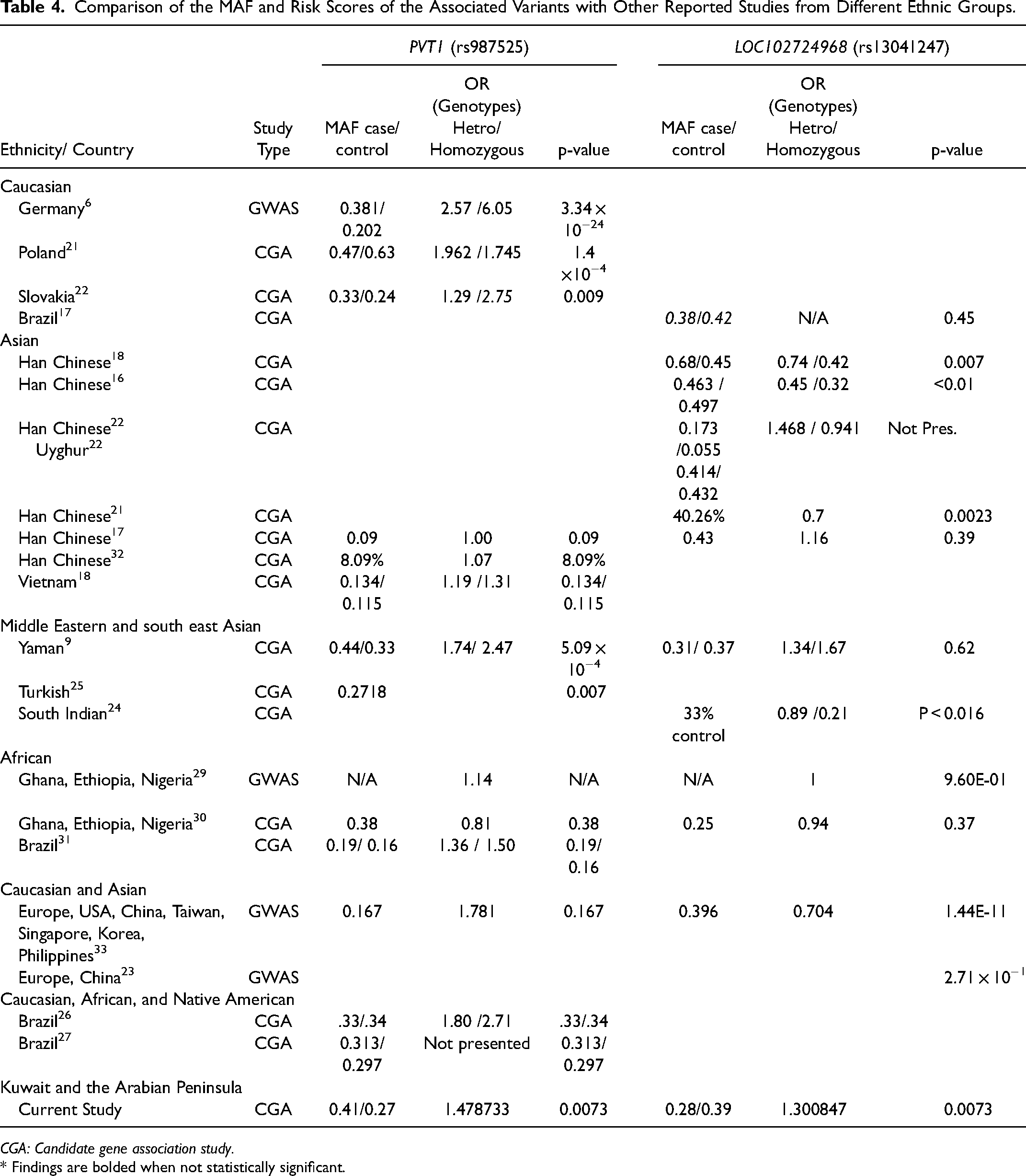
CGA: Candidate gene association study.
* Findings are bolded when not statistically significant.
Figure 1 illustrate the percentage and frequency of homozygous and heterozygous genotypes of PVT1 (rs987525) and LOC102724968 (rs13041247) in cases and controls. In both SNPs, PVT1 (rs987525) and LOC102724968 (rs13041247), there is an increased incidence of the occurrence of NCL/P with the homozygous genotypes AA and TT, respectively. The step-wise gene dosage pattern demonstrates the potential existence of a recessive mode of inheritance, in which a correlation with consanguinity is plausible.
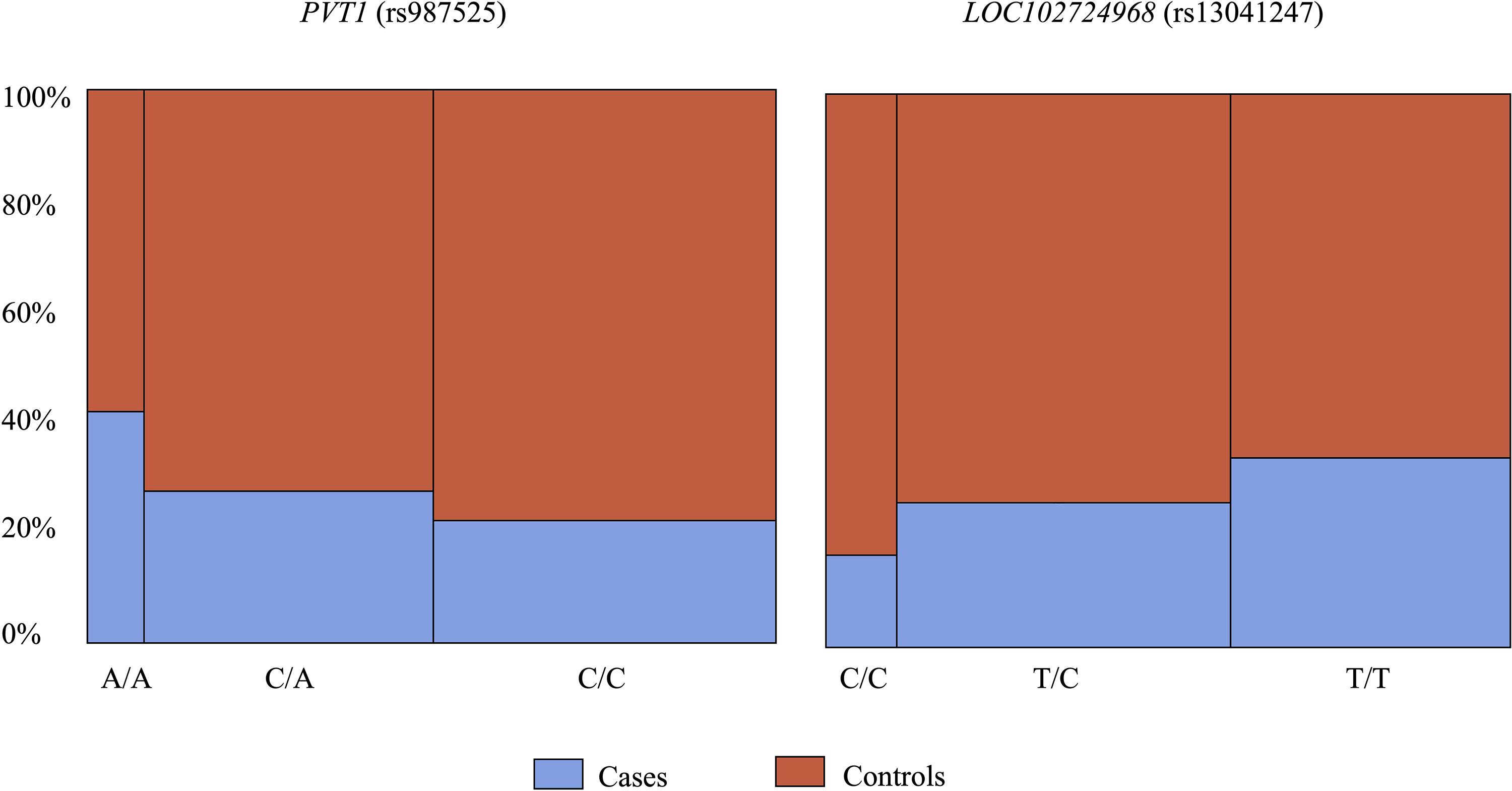
Genotype comparison of PVT1(rs987525) and LOC102724968(rs13041247) between cases and controls.
Discussion
This study presents a reproducibility study in an understudied population in which the findings for the population studies is of novelty. The main goal of identifying potential candidate genes provides further insight into the molecular mechanisms of the anomaly and that can be further investigated in the future through a targeted sequencing project was achieved. Two SNPs were identified in the studied cohort to be significantly associated with NCL/P among the Kuwaiti Arab population.
LOC102724968 is the locus where the uncharacterized SNP rs13041247 is located, near MAFB, a gene involved in palatal development. MAFB has strong expression in palatal and oral epithelium and encodes transcription factors heavily involved in palatal development. 34 When comparing the allele distribution between controls and cases (Tables 1 and 2), one can hypothesize that the recessive allele C may be a minor risk allele by increasing the overall risk to NCL/P by 1.3. Furthermore, as this variant is located near the MAFB gene, it may be influenced by the functional role of MAFB, especially since it has been reported that MAFB was expressed during the development of the secondary palate in mice. 33
PVT1 Oncogene (Plasmacytoma Variant Translocation 1) is a non-protein coding gene and a long non-coding RNA locus. Mutations and fusions of the gene are strongly associated with the occurrence of a variety of cancers, including malignancies of epithelial origin. The mechanisms of such associations are unclear. 6 In accordance with our findings, the relationship of such mutations to the increased risk of NCL/P has been demonstrated, 6 but the mechanism behind its role is yet unclear. Comparison of the allele frequency distribution (Figure 1) supports the observed increased risk of recessive minor allele A to the occurrence of NCL/P. Disruption or alteration in any of these processes can contribute to the development of craniofacial anomalies.
The inconsistency in the associated risk allele (Table 4) is most likely due to the ethnic differences and accumulation of other SNPs that may interact in the development of OFC. Another reason for the discrepancy could be that there the studied SNP is a linkage disequilibrium with the causative variants located in the MAFB gene or that it may be influenced by extragenic modifying gene variants. Further investigation should be carried out using Whole Exome Sequencing (WES), or animal studies to confirm the role of this SNP in the etiology of NSCLP.
Extensive genetic studies in Arabian ethnicity are limited. Nonetheless, one peer-reviewed study investigated the association of 15 risk loci in a novel case-control sample recruited in Yemen. 20 Four of those risk loci are within the group of 14 SNPs investigated in our study. The strongest association was reported for the variant PVT1 Oncogene (rs987525) as shown in Table 4, which coincides with our findings. Interestingly, the SNP LOC102724968 was part of the investigated variants in the mentioned study, but contrary to our findings, there was no significant association. The differences in these findings could be attributed to the difference in the genetic makeup of both populations.
This study had laid the foundation to further secondary projects, such as whole exome sequencing of selected consanguineous families. Furthermore, it demonstrates the role of genetic variants in the development of orofacial clefts that can be further investigated by examining other gene variants to determine their interaction and by possibly employing In vitro functional analysis. It also allowed the development of a registry for orofacial clefts, the first of its kind in Kuwait, and sets an example for possible other epidemiological and genetics studies focusing on diseases understudied in the region. Finally, this had opened an opportunity to consider establishing a GCC consortium. The limitations of this study were mainly related to the small sample size and lack of functional role/analysis of the identified SNPs. The limitation in the sample size prevented further analysis into genotype to genotype correlation which would had provided some insight on the interaction of SNPs at different gene loci and their combined role in the etiology of NSCL/P. Furthermore, it is recommended that animal studies be designed to investigate the role of the significant SNPs on the development pathway of orofacial clefts. This will provide a better understanding of the molecular etiology of NSCL/P.
Conclusions
Genetic variations are associated with the occurrence of oral clefts. Customized Next Generation Sequencing (NGS) panel to the Arab ethnicity is encouraged. In Addition, national preconception genetic carrier screening tests should expand to include common craniofacial anomalies. Findings of this investigation emphasizes the need for genetic counseling, especially to families with a history of OFCs. Our findings encourage further investigation into the functionality of the associated polymorphisms in order to shed light into their involvement in the molecular mechanism of development of NCL/P, and to conduct polygenic risk scores studies in the Kuwaiti and Arabian Peninsula population with the utility of a bigger sample and a larger number of high-risk SNPs.
Footnotes
Acknowledgements
The authors also acknowledge the use of the Kuwait University general facility project (GS01/02) and the Biotechnology center at the Faculty of Science, Kuwait University.
Authors’ Contributions
Availability of Data and Material
Data supporting the findings of this study are available from the corresponding author [LK] on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
All participants agreed to a written informed consent to an institutional review board–approved protocol (Ministry of Health, Kuwait: IRB# 2017-562)
Funding
This work was supported by the Kuwait Foundation for the Advancement of Sciences (grant number #PR17-13DS-01).