
Abstract
Objective
This study aimed to investigate the prevalence of obstructive sleep apnoea (OSA) in patients with craniofacial microsomia (CFM) through polysomnography (PSG) and the relationship with the severity of CFM.
Methods
This study reviewed patients of CFM with pre-operative PSG data between January 2005 and September 2023. Patients were grouped according to the Pruzansky-Kaban classification. OSA was diagnosed and severity was assessed by the obstructive apnea-hypopnea index. The Pediatric Sleep Questionnaire was used to investigate OSA-related signs and symptoms. The χ 2 test and Fisher's exact test were used to compare between groups. Univariate logistic regression was used to identify risk factors associated with OSA. A p-value less than 0.05 was considered statistically significant.
Results
A total of 121 patients with CFM were included in the study with 3 bilateral and 118 unilateral patients. In total, 86 patients (71.07%) were diagnosed with OSA. The prevalence of OSA in type IIa, type IIb and type III was 72.97%, 78.33%, and 47.62%. There was no statistically significant difference in the prevalence of OSA between type IIa and type IIb (p > .05). The difference in the prevalence of OSA between type III and type II was statistically significant (p < .05). Snoring was the most common symptom among the patients of CFM with OSA.
Conclusions
Patients with CFM have a higher incidence of OSA based on PSG in type II and type III patients. The incidence of OSA did not correlate positively with the severity of CFM, with type III patients having certain particularities.
Introduction
Obstructive sleep apnoea (OSA) is a sleep-breathing disorder that affects the physical and mental health, growth, and cognitive function of children. 1 Most studies demonstrated that the prevalence of OSA in the pediatric population varies from 1%-5%. 2 A variety of causes can lead to OSA, including hypertrophy of the adenoids or tonsils, nasal polyps, deviated nasal septum, etc. In addition, abnormal craniofacial development is one of the risk factors of OSA. Children with craniofacial anomalies have a high prevalence of OSA.3,4 Craniofacial microsomia (CFM) is a congenital craniofacial deformity mainly characterized by hypoplasia of the mandible and ear deformity, with a prevalence of about 1 in 3600 to 5600, which makes CFM the second most common congenital craniofacial malformation after cleft lip and palate. 5 Other common malformations of CFM include facial nerve palsy, facial soft tissue dysplasia, macrostomia, spinal and cardiac abnormalities. Several studies have shown the narrowing of the upper airway in CFM and the high incidence of OSA. However, the incidence of OSA in CFM varied considerably between studies, ranging from 7% to 67%. 6 In addition, most previous studies have used questionnaires and charts, with only a few cases in which polysomnography (PSG) was performed to diagnose OSA. Therefore, this study aimed to investigate the occurrence of OSA in patients with CFM by PSG and the correlation between the severity of CFM and the risk of OSA.
Materials and Methods
In this study, patients who were diagnosed with CFM in the Maxillofacial Surgery Department of our hospital between January 2005 and September 2023 were reviewed. The study was reviewed and approved by the Ethics Review Committee of Plastic Surgery Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College (Beijing, China). Written informed consent was obtained from all participants.
Diagnosis of CFM was based on the patient’s history, clinical presentation, and radiographic examination of the craniofacial skeleton. The diagnostic criteria for CFM were congenital mandibular hypoplasia associated with auricular malformations or indirectly related deformities. Patients with pre-operative PSG data were included and those with body mass index (BMI) classified as obese according to Chinese criteria (http://www.nhc.gov.cn/) or with a history of maxillofacial surgery or the presence of respiratory or neuromuscular disease associated with OSA were excluded. Patients were classified according to Pruzansky-Kaban classification. 7 CFM is classified into four types based on mandibular morphology and temporomandibular joint function: Type I has a slightly shorter ascending ramus of the mandible with normal temporomandibular joint function; In Type IIa, the ascending ramus of the mandible is short, with abnormal condylar morphology and basically normal temporomandibular joint function; Type IIb has marked shortening of the ascending mandibular ramus, displacement of the condyle, and basic loss of temporomandibular joint function; Type III with complete absence of the mandibular ascending ramus and articular fossa without temporomandibular joint structures.
OSA was diagnosed and classified based on the obstructive apnea-hypopnea index (OAHI). OAHI ≥ 1 was diagnosed as OSA, mild OSA was defined as 1 ≤ OAHI < 5, moderate OSA as 5 ≤ OAHI < 10, and severe OSA as OAHI ≥ 10.8–10 We used the Pediatric Sleep Questionnaire (PSQ) 11 to investigate the signs and symptoms of patients of CFM with OSA.
SPSS version 26.0 was used for statistical analysis. A chi-squared test and Fisher’s exact test were used to compare the prevalence rates of OSA between different types of patients with CFM. Univariate logistic regression was used to assess gender, affected side, and symptoms such as snoring to identify risk factors associated with OSA. Statistical significance was defined as a p-value less than .05.
Results
There were 121 patients with CFM included in the study. In these patients, the mean age was 7.92 years with a range from 5 to 14 years, 74 were males and 47 were females, 3 cases were bilateral, 53 cases of right-sided mandibular hypoplasia, and 65 cases of left-sided hypoplasia. Three cases of bilateral CFM were a combination of type IIa and IIb with micrognathia (Figure 1). In unilateral cases, 37 patients were classified as type IIa, 60 were classified as type IIb, and 21 were classified as type III by the Pruzansky-Kaban classification system.
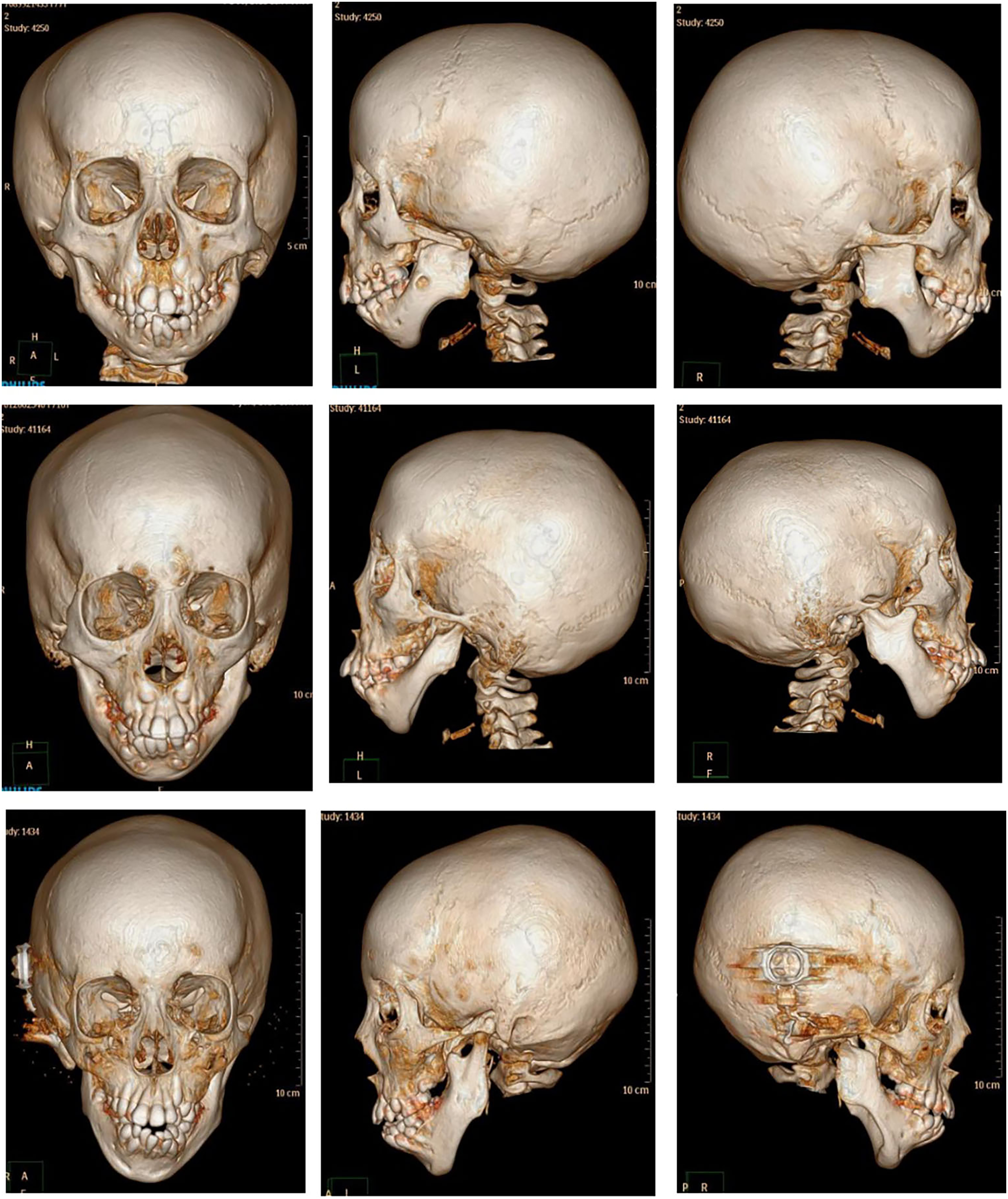
Three cases of bilateral patients with CFM with micrognathia. (Above) No OSA; (Middle) Mild OSA; (Below) Severe OSA.
In total, 86 patients (71.07%) were diagnosed with OSA (OAHI range 1-26.6, average OAHI 4.86), with 56 cases of mild OSA (OAHI range 1-4.7, average OAHI 2.36), 19 cases of moderate OSA (OAHI range 5-9.5, average OAHI 6.24) and 11 cases of severe OSA (OAHI range 10.5-26.6, average OAHI 16.57). Of the 3 bilateral patients with CFM, 1 patient had no OSA, 1 had mild OSA and the other had severe OSA.
Among the different groups of unilateral CFM, 27 patients were diagnosed with OSA in type IIa, 47 patients with OSA in type IIb, and 10 patients with OSA in type III. The prevalence of OSA in type IIa, type IIb and type III was 72.97%, 78.33%, and 47.62% respectively. There was a statistical difference in the prevalence of OSA among the three groups of patients with CFM (p = .023). The prevalence of OSA was not statistically different between type IIa and IIb (p > .05), and there was a statistically significant difference in the prevalence of OSA between type III and type II (p < .05) (Table 1).
Comparison of Clinical Data and Prevalence of OSA Between Different Groups of CFM Patients.
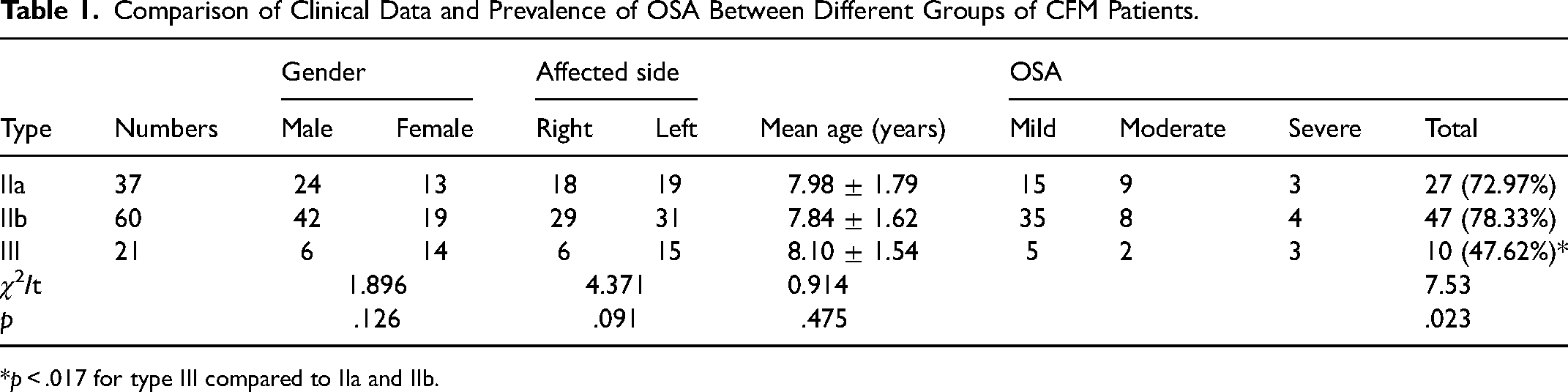
p < .017 for type III compared to IIa and IIb.
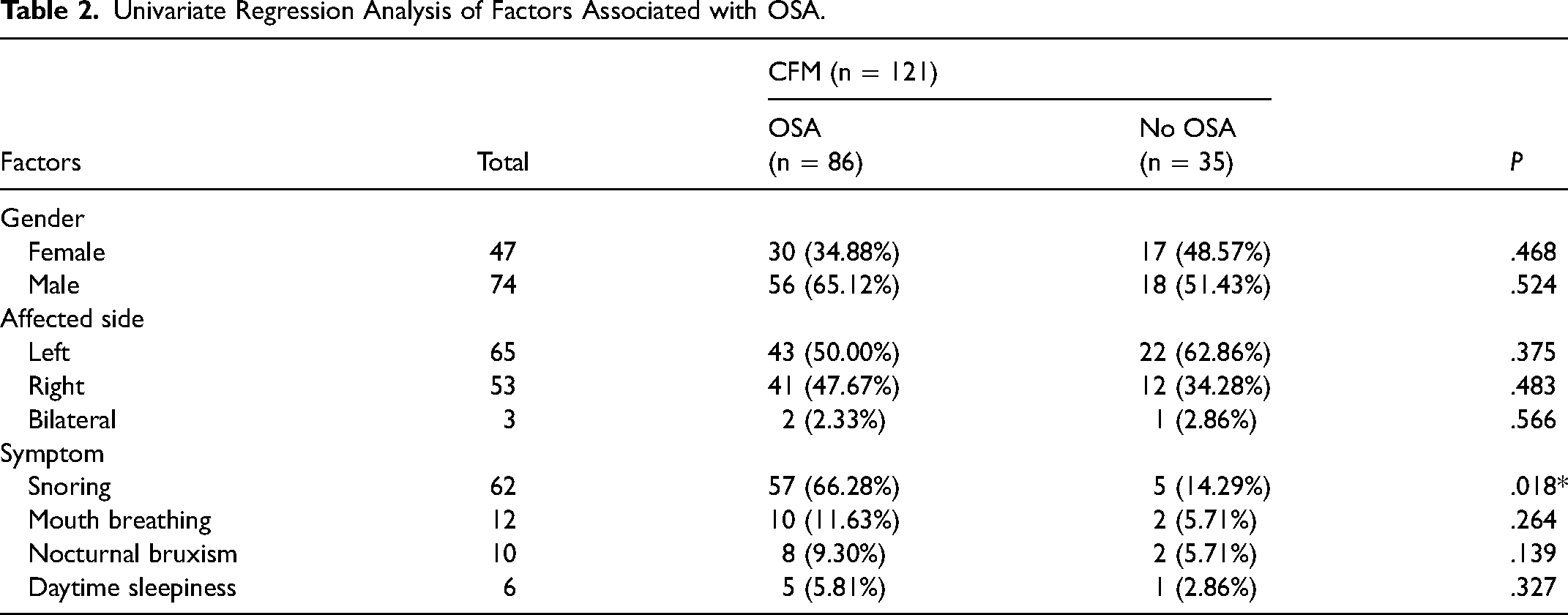
Among our study cohort, patients of CFM with OSA present with multiple clinical manifestations. Snoring (66.28%) was the most common symptom, followed by mouth breathing (11.63%), nocturnal bruxism (9.30%), daytime sleepiness (5.81%), nocturnal sweating (4.65%), and inattention (2.32%). Univariate logistic analysis showed that snoring was significantly correlated with the occurrence of OSA (p < .05). There was no significant correlation between the patient's gender, affected side, and other symptoms and the prevalence of OSA. (Table 2).
Univariate Regression Analysis of Factors Associated with OSA.
Discussion
The structural narrowing of the upper airway is a significant pathological factor in the development of OSA.12,13 To date, several studies have demonstrated that the upper airways of patients with CFM are narrow. 14 Theoretically, patients with CFM have a greater risk of airway obstruction and a higher prevalence of OSA. The prevalence of OSA in patients with CFM was highly variable (7%-67%), the reason for this difference may lie in the different study methods. When diagnosing and evaluating OSA, evaluation of children's symptoms mostly requires parental help, and mild symptoms may not be brought to their attention.Thus some indicators of PSG monitoring in some children may exist independently of subjective symptoms. The previous studies used mostly subjective measurement tools, such as questionnaires, and medical charts.15–17 There were only a few studies based on objective measurements and data. Szpalski et al. 18 investigated the incidence of OSA in unilateral patients with CFM according to the apnea hypopnea index (AHI) of PSG, they reported an OSA incidence of 11.3% in unilateral CFM. However, in their study, only patients with signs or symptoms related to OSA performed PSG. Thus, the incidence of OSA may have been underestimated when the signs and symptoms of OSA are not obvious in some patients. Caron et al. 19 found the prevalence of OSA was 17.6% in patients with CFM. In their study, only patients with suspected OSA who present with breathing difficulties were further reviewed for OSA on PSG results. Therefore, the incidence of OSA may have also been underestimated.
Neither patient signs nor symptoms are good predictors of OSA in children compared to PSG.20,21 PSG is recognized as the gold standard for diagnosing and assessing the severity of OSA. 22 PSG can record changes in a wide range of physiological signs and sleep conditions, and can also identify obstructive, mixed, or central sleep apnoea. Airway obstruction and narrowing are the primary causes of OSA. Therefore, the obstructive apnea-hypopnea index (OAHI) is mainly used as an indicator for the assessment of OSA. In this study, all patients had undergone PSG prior to the operation, and we diagnosed and assessed the severity of OSA according to OAHI. The prevalence of OSA in patients with CFM in this study was 71.07%, higher than in previous studies. This may be caused by the following factors. Firstly, PSG was performed regardless of the presence or absence of OSA-related signs and symptoms, which may increase the detection rate of OSA. Secondly, all patients in this study were type Pruzansky II and III, but no type I patients. Notably, the majority of patients with CFM diagnosed with OSA were mild, this may be easily ignored by the child's family and clinician.
Several studies reported that patients with more severe CFM had a higher risk of OSA.15,16 However, both studies by Cloonan et al. and Cohen et al. classify the severity of CFM only based on medical records and photographs, without imaging data. In the present study, the prevalence of OSA was 72.97%, 78.33%, and 47.62% for type IIa, type IIb and type III in unilateral CFM respectively. Our results showed that the incidence of OSA was greater in type IIb than in type IIa, but the difference was not statistically significant. The prevalence of OSA in type III was less than in type II and the difference was statistically significant, which is consistent with our previous findings. In our previous research, 23 we studied the upper airway morphology of patients of CFM with different clinical types using 3D models. The results showed that the mean cross-sectional area (mean-CSA) of the laryngopharynx was not statistically different between subtypes, mean-CSA of the oropharynx gradually decreased from type I to IIb, while the mean-CSA of the oropharynx in type III was larger than in type II, suggesting that type III patients have less airway resistance than type II according to Poiseuille law. 24 Due to the specificity of type III patients, we conclude that the prevalence of OSA in patients with CFM may not be positively correlated with the degree of mandibular deformity.
Type III CFM is characterized by the absence of the ascending mandibular ramus on the affected side, with different morphology of the stump and varying degrees of mandibular movement. Morphologically, type III patients with CFM have micrognathia (Figure 2). However, we found that some type III patients did not have OSA associated with micrognathia functionally. The three patients with bilateral CFM with micrognathia in this study had concomitant OSA ranging from none to severe, with large individual differences. OSA correlated with the severity of micrognathia, but the sample size was too small to be statistically significant.
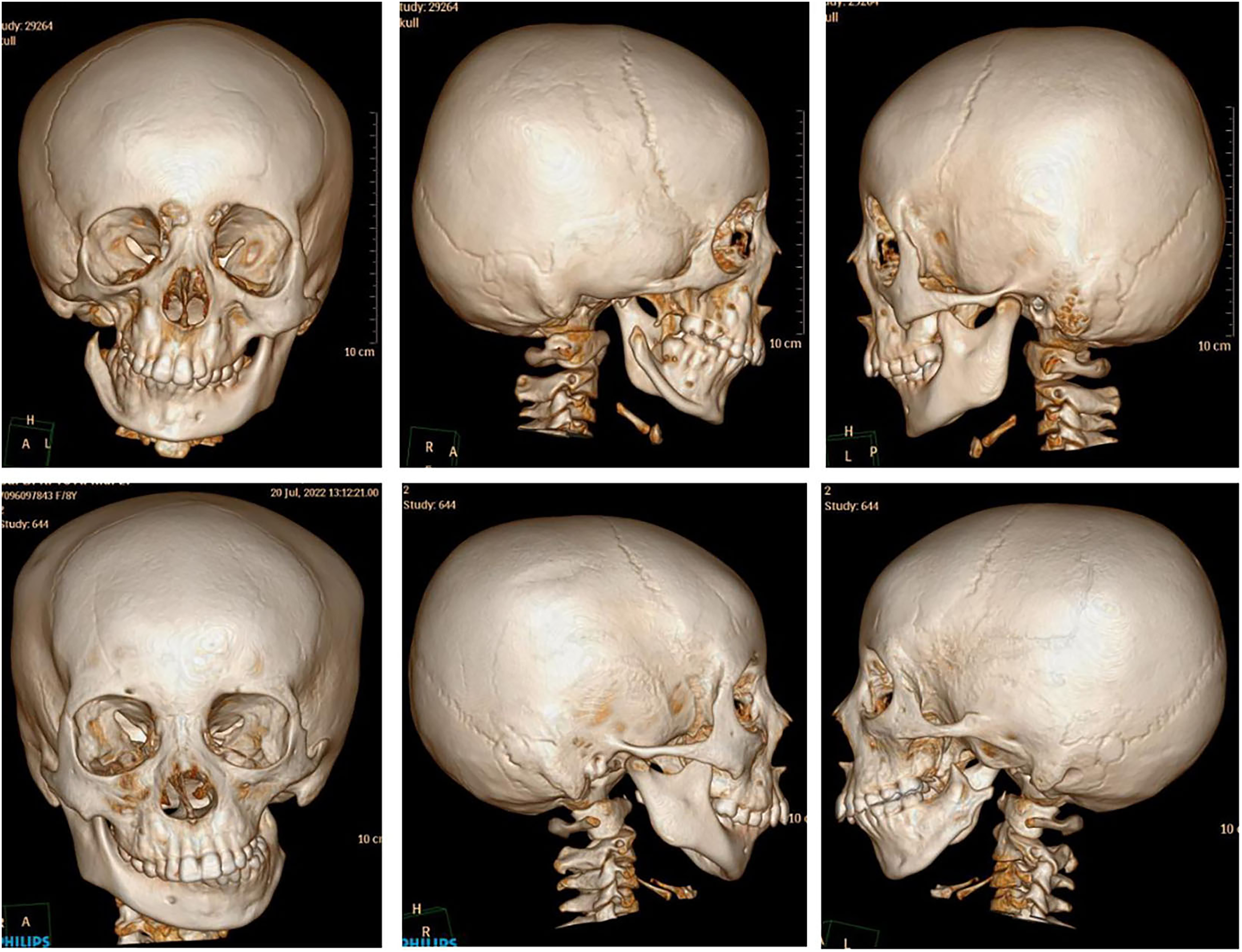
Type III patients with CFM with micrognathia.
We use the Pediatric Sleep Questionnaire (PSQ) to assess OSA-related symptoms and signs in patients with CFM. The questionnaire consists of several questions about the physical characteristics, sleep, and daytime symptoms of the investigators. In our patients’ cohort, snoring is the most common symptom, accounting for 66.28% of all patients of CFM with OSA, which is generally consistent with the previous study. 18 Notably, neither symptoms nor signs can be used as diagnostic tools for OSA. Snoring was significantly associated with the presence of OSA. Patients with snoring symptoms need to be alerted to the occurrence of OSA and, if necessary, have PSG performed to clarify the diagnosis.
However, this study lacked type I patients with CFM, and further research on type I patients is needed in the future.
Conclusion
In conclusion, this study showed that patients with CFM have a higher incidence of OSA based on PSG, with a 71.07% prevalence of OSA in type II and type III patients. However, the incidence of OSA did not correlate positively with the severity of CFM by the Pruzansky-Kaban classification. The prevalence of OSA in type III CFM is lower than in type II. Further research is still needed on the specificity of type III patients. Snoring was the most common symptom among the patients with OSA in this study and was significantly correlated with the occurrence of OSA. Patients with CFM who present with snoring symptoms need to be alerted to the occurrence of OSA and have a PSG examination completed if necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Special Research Fund for Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, the CAMS Innovation Fund for Medical Sciences, (grant number YS202033, 2021-I2M-1-068)