
Abstract
Objective
To determine possible effects of unilateral alveolar cleft closure on internal nasal volume and external nasolabial surface.
Design
Retrospective, single-arm, cohort study.
Setting
Institutional, tertiary care.
Patients
Patients with complete unilateral cleft lip, alveolus, and palate (CUCLAP), who underwent closure of the alveolar cleft with autologous bone graft (ABG) at the age of 9–11 years, with cone beam computed tomography (CBCT) and/or three-dimensional (3D) stereophotogrammetry images taken before and one year after the ABG procedure.
Interventions
ABG-pocedure in patients with CUCLAP.
Main Outcome Measures
The influence of ABG on the internal and external nasal morphology.
Results
A total of 28 patients (21M/7F, 14R/14L) were divided into internal (CBCT) and external (3D-stereophotogrammetry) measurement subgroups. The external nasolabial surface showed a significant decrease of the angle alar curvature right–subnasale–alar curvature left (−1.99°; P = .02; 95% CI −2.61, −0.36) and an increase of the linear measurement between these points (+1.01 mm; P = .03; 95% CI: 0.11, 1.91). No significant differences were found when comparing the distance maps of the affected side with the non-affected side (P = .50, 95% CI: −0.20, 0.29).
Conclusions
Closure of the alveolar cleft in CUCLAP patients with ABG did not affect the internal nasal volume, but significantly affected the external nasal surface. The procedure resulted in the nose becoming wider because both alar curvatures moved caudally and laterally relative to the subnasale.
Introduction
Facial appearance plays an important role in an individual's life, and differences in facial growth and development may be perceived as a problem. Craniofacial malformations influence the facial appearance, and can thereby influence an affected person's well-being. The second most common congenital craniofacial malformations are orofacial clefts, with non-syndromic cleft lip with or without palate having a global prevalence rate of 7.9 per 10 000 births in the 1990s. 1 In the Netherlands, the prevalence of these malformations was 7.6 per 10 000 births. 2
Development of the nose, lip, and palate involves a complex process of differentiation and fusion, leading to merging of the medial nasal processes and the maxillary processes into the upper lip and primary and secondary palate. Normal fusion and differentiation processes are precisely timed, leading to normal orofacial development. Different cleft phenotypes arise during embryogenesis due to deranged fusion and/or differentiation processes. Fusion problems mainly lead to more severe cleft phenotypes, whereas differentiation problems lead to milder cleft phenotypes. 3 Orofacial clefts present with a variety of subphenotypes—ranging from an incomplete cleft lip to a complete cleft lip, alveolus, and palate, either unilateral of bilateral.4,5 Further subphenotyping can improve our understanding of cleft epidemiology and etiology. 6 In patients with unilateral complete cleft lip, alveolus, and palate (CUCLAP), several factors contribute to the stigmatizing asymmetry—including embryonic distortion and intrinsic growth deficiency, as well as surgical repair, which can interfere with a normal facial growth pattern and thereby lead to, for example, flattening of the nose.7,8 Patients with a cleft are usually treated in a multidisciplinary setting, and are followed from birth until adulthood. Depending on the type of cleft, treatment can include various surgical procedures performed during this period. 4 A standardized treatment protocol is often used, but the protocols often differ per hospital. 9 Surgical procedures are performed with the goal of rehabilitating anatomy and improving function. However, alongside the intrinsic differences in craniofacial growth among patients with an oral cleft, the surgical procedures may influence growth. Scar tissue formation may lead to asymmetrical development, which appears to be most prominent in patients with CUCLAP. 10
Even when surgical procedures are performed early in life, patients with CUCLAP will always have residual asymmetry of the face. The nasolabial and oral regions are most affected. 11 Ideally, the alveolar bone grafting procedure (ABG) could play a role in a further attenuation of this asymmetry. Secondary ABG can be divided into early (before eruption of permanent teeth), conventional (mixed dentition stage), and late (after permanent eruption) grafting. 12 During the bone grafting procedure, bone is added in the alveolar cleft to create a continuous maxillary/alveolar arch. The addition of bone in this region may change the shape of the upper lip and the nostril on the cleft side, and reduce asymmetry in the nasolabial area. 13 Furthermore, one could hypothesize that the compression of bone in the alveolar cleft might affect the nasal floor.
Cone beam computed tomography (CBCT) is a reliable three-dimensional diagnostic and evaluation tool for optimizing the planning and execution of the ABG procedure, and for assessing the bone ingrowth after surgery. 12 Moreover, CBCT images are suitable for measuring the nasal airway volume. 14 For evaluating changes at the external nasolabial surface, three-dimensional (3D) stereophotogrammetry has been proven to be an adequate method for facial surface documentation and evaluation. The precision and accuracy are better than with other well-known methods, such as direct anthropometry or two-dimensional photography. 15
The goal of multidisciplinary oral cleft treatment is to reduce the patient burden and the stigma associated with clefts. Therefore, it is important to understand the outcomes of different steps within the total treatment. In this study, we used CBCT and 3D-stereophotogrammetry to assess the influence of ABG on the nasal airway volumes and the external nasolabial surface in patients with CUCLAP.
Materials and Methods
The study protocol was approved by the medical ethics committee of the involved institute (Radboud University Medical Center, Nijmegen, the Netherlands), and is in accordance with the 1964 Declaration of Helsinki and later amendments.
This study included patients with CUCLAP from the Cleft Palate Craniofacial Unit database of the Amalia's Childrens Hospital, Radboud Univeristy Medical Center in Nijmegen, The Netherlands. Due to a change in the primary surgery protocol since 2008, we excluded patients from this study if their date of birth was the 1st of January 2008 or later.
In this protocol, primary surgery for lip closure was performed at 4–6 months of age, the soft palate was closed at 12 months of age, and the hard palate was closed at the same time as the ABG procedure. Closure of the alveolar cleft (ABG procedure) was ideally performed before eruption of the permanent canine at the cleft side, using autologous bone from the mandibular symphysis. 16 This procedure was performed by one of two experienced surgeons, when the patient was 9–11 years old.
Inclusion criteria were non-syndromic patients with CUCLAP born between January 1st of 1994 until December 31st of 2007, with CBCT and /or 3D-stereophotogrammetry images available before and one year after bone graft. Patients were excluded if the cleft was bilateral or incomplete, if diagnosed with a syndrome, if the images were taken more than six months from the study time-points, or if the images were of insufficient quality. Patient data were pseudonymized prior to analysis of the acquired images.
Cone Beam CT
CBCT images were obtained using the KaVo 3D Exam cone beam CT unit (KaVo Dental, Biberach, Germany) with the following parameters: kV = 120, mA = 5, and voxel size = 0.3 mm. To evaluate the nasal airway volume in CBCT images, we used a custom in-house-made software program called the ‘Airway Segmentor’ (MATLAB 2017a; The MathWorks, Inc., Natick, MA, USA), as described and validated by Zhang et al. 14 Using this tool, the nasal cavity was semi-automatically segmented from the CBCT using a region of interest (ROI). The ROI was anteriorly delimited by a vertical plane through the most posterior point of the nasal nares, and posteriorly delimited by a vertical plane passing through the most anterior point of the posterior boundary of the nasal septum. The palate was the caudal border of the ROI, and the coronal border was indicated as a spline curve from the basion, via the ethmoid sinuses, to the nasion (Figure 1). 14 The maxillary and ethmoidal sinuses were manually removed, and then the resulting volume was extracted as a 3D model of the nasal airway (Figure 1). The volume of this airway was measured in mm3. The inter- and intra-rater reliability of this nasal airway volume measuring method was reported by Zhang et al. 14
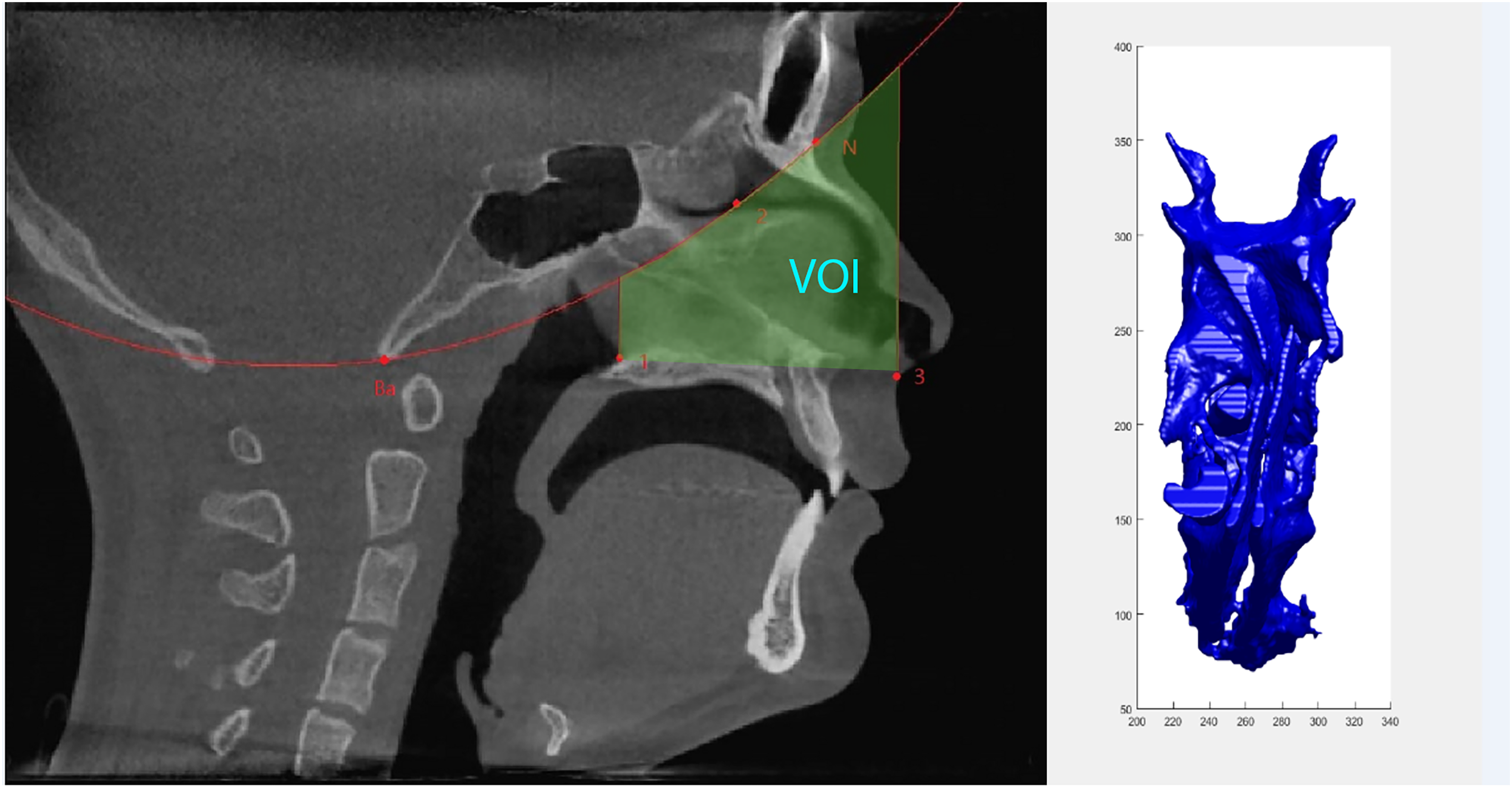
Sagittal view of a CBCT indicating the bouderies for creating the 3D nasal area volume (VOI area) (Zhang et al. 14 ), combined with a 3D-representation of the nasal airway volume rendered using Airway Segmentor in Matlab. Volume in mm3. View from cranial side.
3D-Stereophotogrammetry
We acquired 3D images of the face using the 3dMD system (3dMD; V3.0.1; Atlanta, GA, USA) with two pods with a special resolution of 0.2 mm. Patients were instructed to look forward with a neutral facial expression, and to keep their eyes open while the images were acquired. All images were taken by an experienced operator, and the system settings were calibrated every morning.
The acquired images were loaded into 3DMedX® version 1.2.13.1 (version 1.1.8 3D Lab Radboudumc, Nijmegen, the Netherlands). Measurements were performed using a custom-made workflow. Linear and angular measurements were taken using the point alar curvature (most caudolateral point of the transition between the nostril and cheek) left and right, and subnasale in between. The following variables were defined:
ALR: alar curvature right–alar curvature left ASN: affected alar curvature–subnasale NSN: non-affected alar curvature–subnasale NB: nasal base (alar curvature right–subnasale–alar curvature left AN: angle of alar curvature right–subnasale–alar curvature left
The results were subdivided into an affected and a non-affected side. After these measurements, a distance map was created to visualize the inter-surface difference of the nose and upper lip. This distance map was generated by matching the image acquired before grafting to the image acquired one year after ABG. These images were aligned using a rigid iterative closest point (ICP) algorithm. ICP alignment has been proven to be an accurate and reliable method for superimposing similar surfaces.
17
The image acquired before ABG was aligned towards the postoperative image using the ICP algorithm. The images were superimposed on the area between the soft tissue glabella, endocanthion left and right, and point V.
18
The distance maps were used to measure the facial changes following the ABG procedure. On the 3D image, the ROI was delineated by the right and left cheilon, right and left alar point (most lateral point of ala of the nose), and the midpoint of a line drawn between the subnasale and soft nasion. The line through the subnasale and soft nasion was also used to distinguish between the affected and non-affected side. All cleft sides were clustered in one group, and the non-affected sides were clustered into another group. For each patient, the mean and the standard deviation for that distance map were used as the outcome. All measurements were conducted twice by the first author, with a 10-day interval, to determine the intra-rater reliability. A second author (LK) also performed the measurements to determine the inter-rater reliability.
Statistical Analysis
All data were statistically analysed using SPSS statistics (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0.0.1; Armonk, NY, USA). Changes of internal volume were analysed using a paired samples T-test. The linear and angular measurements on the 3D image were analysed using a paired samples T-test, whereas an independent samples T-test was used to analyse the mean values from the distance maps. To determine the inter- and intra-rater reliability of the 3D-stereophotogrammetrical data, reliability analysis was performed using the intraclass correlation coefficient (ICC).
Results
During the study period, 241 patients were identified as having a CUCLAP. 215 Patients were identified. 18 patients were excluded, because of a syndrome (n = 18) . Additionally, 116 patients were excluded due to lacking data, 20 patients because the images were taken more than six months away from the desired time-points, and 33 patients due to suboptimal image quality. Thus, our analysis included a total of 28 non-syndromic patients (21 male, 7 female) with CUCLAP. The patients were of mixed race (Asian and Caucasian). The mean age at the time of surgical intervention was 10.30 years (min. 8.25; max. 12.08; SD 0.86). The left side was affected in 14 patients (50.00%), and the right side in 14 patients (50.00%). Patients were divided into two groups: available CBCT data and available 3D-stereophotogrammetry data. Both kinds of data were available for some patients, while other patients had only one kind of data available due to incomplete data, e.g., small field of view for CBCT, facial expressions in 3D-stereophotogrammetry, artifacts (surface data loss or scalp hair), or inadequate timing of scan/image acquisition before or after the ABG procedure.
Cone Beam CT
The CBCT group comprised seventeen patients (13 male/4 female; 9 left/8 right) with a mean age of 10.24 years (min. 8.25; max. 11.92; SD 0.83) at the time of the ABG procedure. Internal nasal volume was measured before the ABG procedure (mean +9677.59 mm3; SD 4033.13) and after (mean + 10 820.71 mm3; SD 3642.42) (Table 1). The internal nasal volume did not significantly change as an effect of the autologous bone grafting procedure (mean volume change +1143.11 mm3; P = .08; 95% CI: −155.44, 2441.66) (Table 2).
Internal Nasal Volumes (mm3)of the Patients as Measured on CBCT-Scans Before and After the Alveolar Bone Grafting Procedure.

Effect of the Alveolar Bone Graft on the Internal Nasal Volume (mm3).

3D-Stereophotogrammetry
The 3D-stereophotogrammetry group included sixteen patients (12 male/4 female; 8 left/8 right) with a mean age of 10.33 years (min. 8.25; max. 12.08; SD 1.02) at the time of the ABG procedure. The external nasolabial surface significantly changed after the alveolar bone grafting procedure, on both the angle of the alar curvature right–subnasale–alar curvature left, and the linear measurement between these three points (Table 3). The angle decreased by 1.99° (P = .02; 95% CI: −2.61, −0.36) and the distance increased by 1.01 mm (P = .03; 95% CI: 0.11, 1.91). These findings indicate that the ABG procedure caused the nostril to become wider, while the upper lip remained the same. We did not find significant changes in the width between alar curvature left and right, alar curvature of the affected side and subnasale, and alar curvature of the non-affected side and subnasale.
Comparison of Linear Measurements on 3D-Stereophotogrammetry Before and After Alveolar Bone Grafting Procedure.
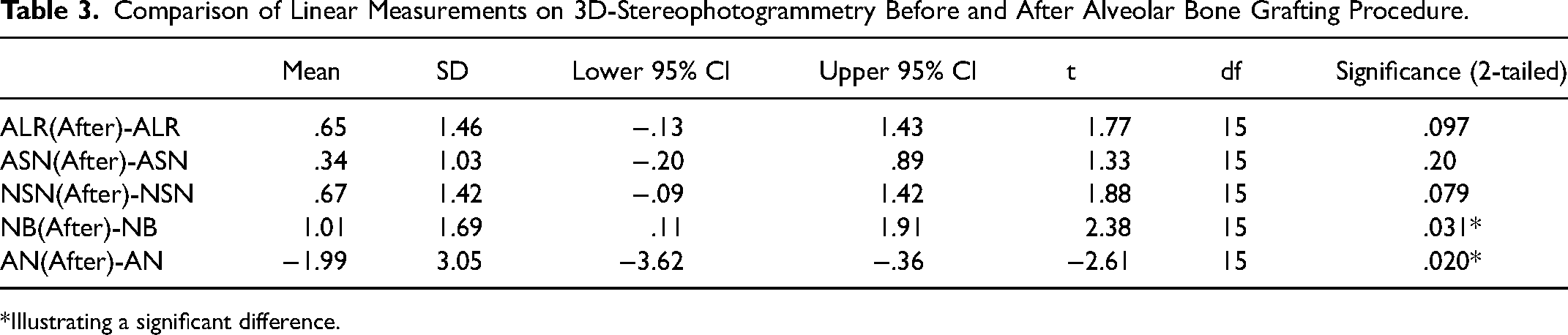
*Illustrating a significant difference.
Inter- and intrarater reliability of the used method proved to be good or excellent for most linear measurements as well as for the distance maps, with ICC-values ranging from .79 to .99. Exceptions are the interrater reliability of the width of the non-affected side before and after the ABG-procedure (resp. ICC .71; .55), the width of the affected side after the ABG-procedure (ICC .73) and the intrarater reliability of the non-affected side after the ABG-procedure (ICC .59).
When comparing the affected side (mean intersurface distance 0.04 mm; SD 0.83) with the non-affected side (mean intersurface distance 0.016 mm; SD 0.81) on the distance maps of the nasolabial surface no significant difference was found (P = 0.79; 95% CI: −0.20, 0.29) (Figure 2).
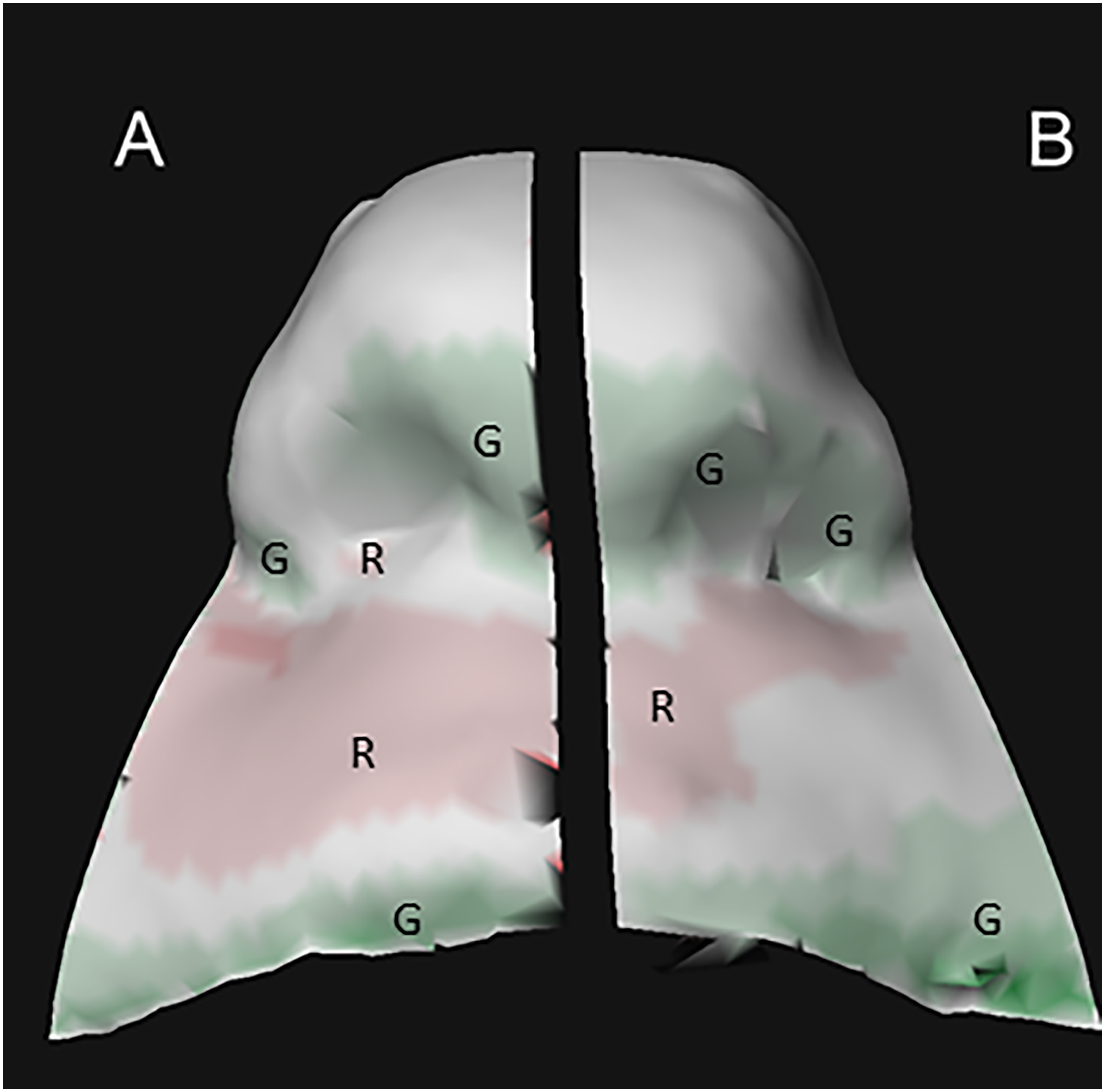
Changes of the soft tissues after alveolar bone graft (A non cleft side, B cleft side). Distance map of the caudofrontal view of the lower half of the nose and the upper lip/philtrum showing the upper lip surface after surgery to be slightly, however non significant, behind the upper lip surface before surgery (red areas) in the non-cleft side (A). At the cleft side (B) there is a slight forward position, however non significant, mainly of the alar base after surgery. Areas marked with R represent a negative difference, areas marked with G represent a positive difference, range −10 mm to +10 mm.
Discussion
In the present study, we found that the compression of bone in the alveolar cleft of patients with CUCLAP during the ABG procedure resulted in significant changes of the external nasal surface, especially the characteristics of the nasal base.
Facial growth is influenced by a combination of intrinsic and extrinsic factors, such as surgery (scar tissue), which contribute to the characteristic lip and nasal imbalance, 19 as well as to a reduced mean volume of the nasopharyngeal airway. 20 Compared to healthy individuals, patients with CUCLAP exhibit reduced facial soft tissue growth in all dimensions—vertical, sagittal, and transversal. 21 In our present study, the mixed race population (Asian and Caucasian) could have led to a potential racial bias, as race may also have an influence on facial characteristics and growth. This potential risk of bias was overcome by comparing the results per individual before pooling the data and analysing the results in the subgroups. Furthermore, comparing the results per individual highlights the changes that resulted from ABG rather than those affected by the patients’ ethnic backgrounds.
Patient inclusion occurred based on all of the available data at the Cleft Palate Craniofacial Unit. Due to the definite available number of patients with a cleft and the retrospective nature of this study, no sample size calculation was performed. The consequential small and heterogenous (ie, race, gender) sample is a limitation of not only this cleft study but is seen more generally in this field of research. The dental age of the patients – in contrast – is comparable, due to the inclusion of patients based on the eruption of the upper canines.
When surgically treating patients with CUCLAP, the goal is to restore function and to thereby reduce the characteristic cleft features and associated stigma. Understanding how the ABG procedure affects the nasolabial area is important to maximize the potential benefits of the necessary surgical operations. The procedure tends to decrease the asymmetry of the nasolabial area,22,23 although the available research is not conclusive regarding the improvement in symmetry. 13 Our present findings revealed no significant beneficial external dimensional change on the affected side compared to the non-affected side. Therefore, our study adds to the current knowledge of how the ABG procedure influences external dimensional changes in the nasolabial area and nasal volume, which will facilitate the possibility of optimizing the forward planning of the operation.
Here we used CBCT and 3D-stereophotogrammetry to assess differences in nasal volume and nasal and lip shape. CBCT is a useful tool for evaluating the bone grafting and tooth position, and is thus often used to plan treatment for patients with a cleft. These readily available data are suitable for analysis of the nasopharyngeal airways, 24 and the representation of the airways is similar to those in CT scans. 25 Notably, differences in the grayscales in the available CBCT images required that we made minor changes to the selected threshold value. This could potentially lead to overestimation or underestimation of the measured airway volume. However, in other similar programs, minor changes in threshold values have not significantly changed the measured values, therefore proving this method to be reliable. 26
Furthermore, in this study, we measured the nasal volume as well as lip and nasal changes after ABG. The ABG procedure is performed when the patient is between 9–11 years of age, just before canine eruption. This means that the procedure is performed in growing patients, and growth may also induce nasal volume and lip and nose changes. However, nasal airway volumes do not seem to change during the growth spurt in patients with CUCLAP, whereas the volumes tend to increase during growth in non-affected patients. 27 Therefore, the slight changes in nasal volume found in our present study might be attributed to modifications in the nasal area induced by the compression of bone into the cleft during the ABG procedure. In this study patients participated who were treated according to our former protocol in which closure of the hard palate occurred at the same time of the bonegraft procedure. Late closure of the hard palate was done to achieve better growth of the maxilla. This may cause differences in the maxillary apical base and nasal base when compared to earlier closure of the hard palate. A comparison between early and late hard palate closure of patients treated in our cleft palate team was not possible yet.
3D-stereophotogrammetry is useful for treatment planning, and for assessing 3D changes resulting from growth and surgical interventions. This technique offers the advantages that it is fast and does not involve radiation exposure. These features make it easily applicable for evaluating facial growth and treatment in younger patients. Superimposition of 3D-stereophotogrammetry images from patients with a cleft provides reliable results regarding the changes of facial structures over time. 28 Despite advancements in recent years, clinicians must be alert to avoid artifacts in these images. In the present study, special attention was required for the subnasale region, since it is prone to data loss because of the direct lighting needed, and since this region is sensitive to reflection due to a shiny surface (snotty nose). Minor instances of this artifact were observed in some of the images used. For future research aimed at obtaining the most usable data, it is recommended to have the subject slightly tilt their head backward with the forehead free from scalp hair. 27
In our study, a substantial portion of the available 3D-stereophotogrammetrical images included irregularities (ie, scalp hair and acne on the forehead); therefore, a smaller region was used for superimposition. For the stereophotogrammetric analysis we superimposed the images before and after bone grafting on the area of the soft tissue glabella, endocanthion left and right, and point V. We choose this region as it is relatively stable in this young age group while the length of the follow-up period was only one year. As is widely accepted there are no true stable regions in the cranium or the face. Farkas et al. 29 using direct anthropometry and Ainuz et al. 30 using stereophotogrammetry performed longitudinal studies assessing growth changes. In the latter study measurements were performed longitudinally using 3D stereophoto-grammetry from the age of 6 to 11 years in a group of 194 children in Dallas (USA). Their research showed that in our specific age group (bone graft at the age of 10.3 years, follow-up 1 year) growth is limited in this part of the face. Furthermore, superimposition of 3D images is less susceptible to errors due to small growth changes as it is not a superimposition based on landmarks but it is based on the best fit of two surfaces. Additionally, the Iterative Closest Point (ICP) method was employed for image superimposition. One significant advantage of ICP is that it incorporates a more extensive dataset for superimposition, as opposed to relying on a few manually selected landmarks.
Additionally, in younger patients with a cleft, facial mimicry can lead to distortion of the rendered 3D-images, especially in the nasolabial region. 31 However, previous studies show that 3D-stereophotogrammetry with modern technology is an adequate and reliable imaging technique, and superimposition of these images is proven to be accurate.32,33 The presently utilized 3DMD software includes the option to pick an image from a short video capture. When combined with well-trained staff, this feature enables the clinician to select the best 3D image without the need to continuously take new pictures.
As mentioned above, 3D-stereophotogrammetry images were acquired in growing individuals, which may influence facial shape. Measurements may show an effect of growth and surgery. However there is not a lot of growth during the one year follow up on our specific age group. Larger changes do occur during growth spurt.29,30,34 Altogether, the available data suggest that growth may have had a negligible influence on our findings, meaning that the observed change in alar curvature left via subnasale to alar curvature right could be a result of the ABG procedure. Thus, it can be suggested that the ABG procedure reduces the flattening of the nose, and thereby reduces the cleft stigma. Further research is needed to explore the possible correlation between the external and internal nasal changes, and to compare the CUCLAP group with another cleft subphenotype.
In conclusion, our present findings indicate that closure of the unilateral alveolar cleft with ABG in the context of our treatment protocol has a significant effect on the external nasal surface. The alveolar bone grafting procedure results in the nose becoming wider because the alar curvature left and right move caudally and laterally relative to the point subnasale. In contrast, internal nasal volume did not significantly change after alveolar cleft closure. These findings can improve the information provided to patients regarding the ABG procedure.
Footnotes
Data Availability Statement
The data underlying this article will be shared upon reasonable request to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.