
Abstract
Objective
This is a cross sectional study aimed to asses novel semi objectve compter assisted method to asses the symmetry amog unilateral cleft lip patients.
Design
using Standard inferior view nose photos that were uploaded to Digimizer© Version 4.6.1 (2005–2016 MedCalc Software) Image Analysis, symmetry percentage was calculated and compared between cleft and non-cleft neonates. This method was compared to two subjective methods of rating symmetry.
Setting
This a cross sectional pilot study performed in the Univresity Medical Center using standard inferior views of unilateral cleft patients which were compared to non-cleft neonates.
Patients
Photographs of 71 neonates with unilateral complete and incomplete cleft lip and 30 neonates without facial cleft, which were born at the university medical center, Beer Sheba, Israel, were analyzed in a standard manner to determine nasal symmetry.
Main measures
the novel method proposed produced a nominal value for percentage of symmetry.
Results
Using Pearson's correlation test we found intra-rater reliability of 91.2% (p < 0.001) and Inter-rater reliability of 82.9% (p < 0.001). The analysis correlated with the surgeons subjective scores in both the numerical ranking method at 73% (p < 0.001) and 72.6% (p < 0.001) and the Ordinal ranking method at 87.6% (p < 0.001) and 77.7% (p < 0.001). The ability of the method to discriminate healthy from Cleft Lip patients overall was 92.3% With high sensitivity and specificity.
Conclusions
This method accurately distinguishes healthy patients from cleft lip patients. We have achieved High levels of inter and intra-rater reliability. Significant correlations were found between our semiobjective method and the subjective scores.
Introduction
Physical and Facial attractiveness have important social consequences. Attractive people seem to lead a favorable life, have better and more abundant career opportunities, and more likely to be hired for a job. They also find it easier to find a spouse and enjoy social popularity. Symmetry is one of the main features of the attractive face, it reflects a normal development and function. 1
In humans’ complete union of the lip is usually accomplished at 35 days of embryo's life, as the lateral nasal, medial nasal and the maxillary mesodermal processes merge. A failure in merging of the maxillary processes produces unilateral, bilateral, or median cleft lip. These may be complete or incomplete clefts. 2 On the pathophysiological level this process represents a failure in mesenchymal proliferation and reduced FGF signaling, followed by breakdown and cleft formation. 3 Cleft lip and palate are the most common head and neck congenital deformities with an incidence of 1/1000 live births in the Israeli Negev population. 2
The classic features of the unilateral cleft lip deformity include deficiency of the maxillary alveolar ridge. The upper lip Cupid's bow is pulled into the affected recumbent nostril on the cleft side. 4 The wide piriform aperture causes the alar base to be situated laterally inferiorly and posteriorly. The anterior nasal spine, septum and columellar base deviate to the non-cleft side. 5
The surgical correction of the cleft lip is usually performed around the 3rd month of life aiming at restoring symmetry of the unilateral cleft lip and nose, attempting approximate normal anatomy. 4 Yet, the stigmata of the cleft lip persist with the affected children, and some must go through additional surgical procedures in order to improve lip and nasal appearance. Individuals affected by cleft lip and palate often experience social rejection, and may have trouble with social adjustment.6,7
There have been many attempts to assess and rate cleft lip surgery results. However, an optimal method to assess aesthetic outcomes accurately, is yet to be found. Saxby and Palmer tried using independent panel to assess long term results of cleft lip repair. Pairs of standardized photographs were presented to panel members which had to rank surgical results according to a scale running from “normal appearance” to “unacceptable result”. They also assessed the time factor as the photographs were assessed again after several months. 8
Laitung et al. compared panel assessment with computer-assisted analysis of upper nasal perimeter and alar margin based on standardized photographs, using a panel of cleft professionals and compared it with a computer analysis program. They concluded that the computer-based ranking offers a far more objective assessment while the panel assessment is subject to bias. But the computer assessment is not designed to evaluate overall esthetics. 9
Mosmuller et al. evaluated the effectiveness of SymNose© (Brian Pigott 2009 version 6.18 (2014)), which compared symmetry between the cleft side of CL patients with the non affected side of the same patient. The shape of ala, which in CL patient can vary and is inconsistent, influenced the used reference line for the nasal parameters. The study results showed low inter observer reliability when using the SymNose© program. 10
Bella et al. tried to evaluate percentage of symmetry by comparing left side of nose and lip to the right side assesing the mismatch areas using SymNose©. These were compared to subjective assesment of a panel of professionals. This research revealed a rather low inter-rater reiability using a Likert scale ranging from “excellent” to “very poor”. 11 Deall et al. also used SymNose© to compare an objective measurement with a Panel's subjective rates. They found that while the association of SymNose© and the panels lip rating was high, the association of nose scoring between the two systems was insignificant. 12
These studies emphasize the problem in assessing cleft surgery results. None of the methods can measure and score cleft surgery results by ultimate objective and accurate means.13,14
Our group is proposing a novel method to assess nasal symmetry using a worm's view photographs and an image analysis software. The objective of this study is to validate our novel method of symmetry analysis and to establish norms of nasal symmetry among newborns without facial cleft. Such norms were not set thus far.
Material and Methods
This is a cross sectional pilot study. Approval from institutions ethical committee was obtained before commencing the research. Photographs of 71 neonates with unilateral cleft lip and 30 neonates without facial cleft, which were born at the ‘Soroka’ university medical center, Beer Sheba, Israel, were analyzed in a standard manner to determine nasal symmetry. The results were examined for inter and intra-rater reliability and were compared to two methods of expert panel rankings to validate the method.
The research included all the children who were born with unilateral cleft lip and underwent a surgical repair at the ‘Soroka’ university medical center between 2004–2018. As a control group 30 newborns without facial cleft between the ages of 1 day to 1 month, who were born at the ‘Soroka’ University medical center, and their parents consented for their participation. The participating neonates were excluded for any known nasal or lip deformity except for unilateral cleft lip (such as hemangiomas, dermoid cysts, nasal trauma). All participating neonates in the CL group had available photos before and after CL surgery.
Demographic data of birth date and gender were collected for all participants and for cleft patients also the type of deformity.
Symmetry Analysis Using the Novel Method
Standard inferior view nose photos were uploaded to Digimizer© Version 4.6.1 (2005–2016 MedCalc Software) Image Analysis. The analyzer defines the alar curvature (ac) points on each side of the nose and draws a straight line between them (ac-ac line) (Figure 1a and b) which is the reference line. 14 The analyzer outlined the nostril circumference, and the software determines the nostril center according to it. The analyzer then draws a perpendicular line from the nostril center to the reference line (ac-ac) (Figure 1b) and then divides the nostril area into 8 sectors with a 45° angle between them. Each sector area is determined by the software and is compared to the mirror sector in the other nostril (the smaller area is being deducted from the larger area). Each sector symmetry is defined according to the percentage of symmetry (deduction of the smaller sector area from the larger sector area and dividing the result by the larger sector area). Then the overall symmetry is defined by the mean symmetry of all sections.
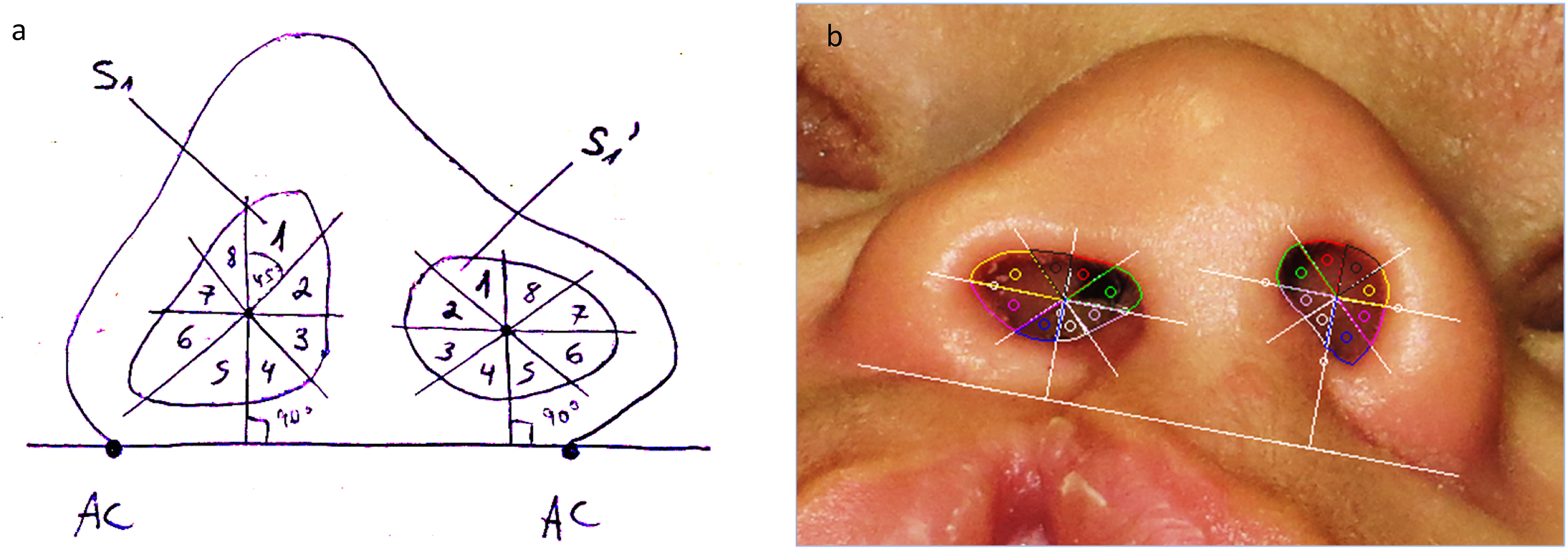
(a) An illustration of our novel method to determine nasal symmetry analysis. (b) Example of our semi objective method for nasal symmetry analysis using Digimizer© software.
Symmetry Percentage is determined by the following equation:

Comparing the Novel Method to Subjective Methods
Method A: Two senior surgeons scored 20 photos of a mixture of 5 children without facial cleft and 15 unilateral incomplete cleft lip patients using a rating scale: 1 – Excellent symmetry 2 – Good symmetry 3 – Fair symmetry 4 – Poor symmetry 5 – Very poor symmetry.
The examiners rated the photo images subjectively and separately without being exposed to a predetermined scale. Two other team members analyzed nasal symmetry in the same photos using the Digimizer© software. The use of incomplete unilateral cleft cases for comparing between the subjective and the novel method will able to establish the efficacy of the method in distinguishing between cleft and non cleft cases even in rather subtle deviations of symmetry.
Method B: Two senior surgeons ranked a collection of the same 20 photos of babies without facial cleft and cleft lip patients with incomplete cleft lip in an ordinal way from the best to the least symmetrical baby (Figure 2). Photos were displayed simultaneously on one screen, allowing a macro view for relative assessment. The photo chosen by the surgeon to be first represents best nasal symmetry, and the last photo in line represents worst nasal symmetry.
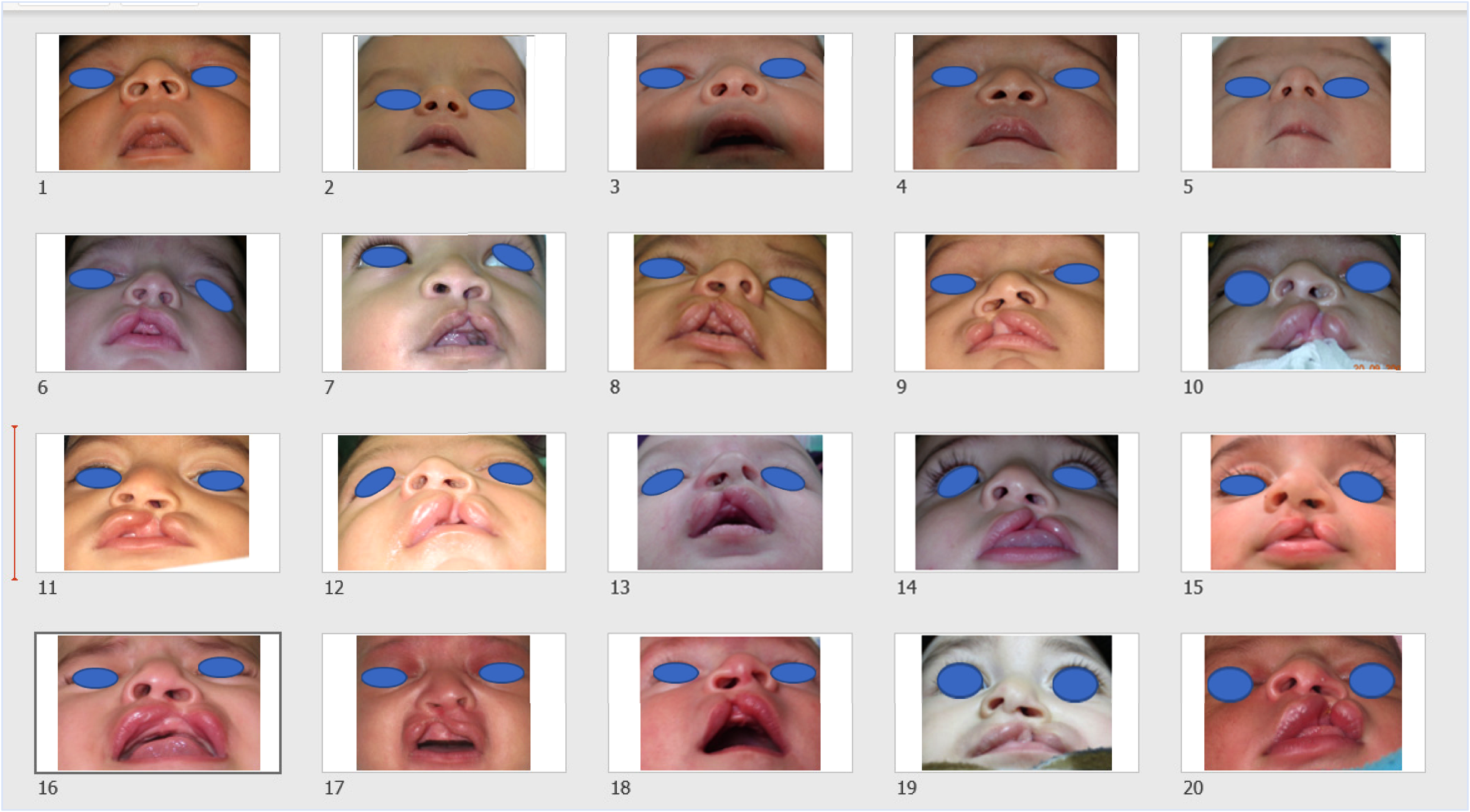
Example of method B – a subjective ordinal rating method.
Statistical Analysis
Univariable analysis was performed in order to evaluate the characteristics of the study group and the control group. The univariable analysis included T-test for the continuous variable.
In order to evaluate the differences between the 3 categorical groups – 2 subgroups of the study group and the control group, we used One-way ANOVA test.
Bonferroni test was performed for multiple comparisons with the dependent variable to examine the differences between the categorical subgroups and control group.
Logistic regression was performed to estimate how the independent nominal variable affect the dependent variable, using the Omnibus test to determine the difference in significance.
ROC (Receiver operating characteristic) analysis was performed to determine the sensitivity and specificity of our novel method, and evaluated our method's predictability by measuring the Area Under the Curve.
20 photographs were analyzed by 2 independent team members. 20 photographs were analyzed twice by the same team member without knowing what the previous score was. To evaluate Intra-rater and Inter-rater reliability we used Pearson's and Spearman's correlation tests. We also performed non-parametric Kendall's tau b to measure the strength of the correlations.
To evaluate the association between the two senior surgeons’ scores in method A and B, and to assess whether these methods correlated to the analysis determined by our novel method we used Pearson's correlation coefficient test.
All analyses were performed using IBM® SPSS® statistics software (version 23).
Results
During the 15 years of the study period there were 71 Cleft lip patients who met the inclusion criteria, 30 Females (42.2%) and 41 Males (57.7%). 59 were patients with Incomplete Unilateral Cleft Lip (IUCL) and 12 were patients with Complete Unilateral Cleft Lip (CUCL). The control group included 30 patients without facial cleft, 21 Females (70%) and 9 Males (30%) who were chosen randomly from the maternity department in 2019.
Using logistic regression, we found that the ability of our new method to discriminate neonate without facial cleft and CL patients overall was 92.3% (OR 0.727, p < 0.001, 95% CI 0.63–0.84). ROC analysis found that our model accurately predicted neonates without facial cleft and CL patients (AUC 0.97 p < 0.001, 95%CI 0.942–0.998).
Using Pearson's correlation test we found an intra-rater reliability of 91.2% (p < 0.001), and inter-rater reliability of 82.9% (p < 0.001).
Using Pearson's correlation test we found that the correlation between the two senior surgeons scores was 87.1% (p < 0.001) in method A and 86% (p < 0.001) in method B. The correlation between the two different subjective methods performed by the same surgeon was 85.3% (p < 0.001) for the 1st surgeon and 78.7% (p < 0.001) for the 2nd surgeon.
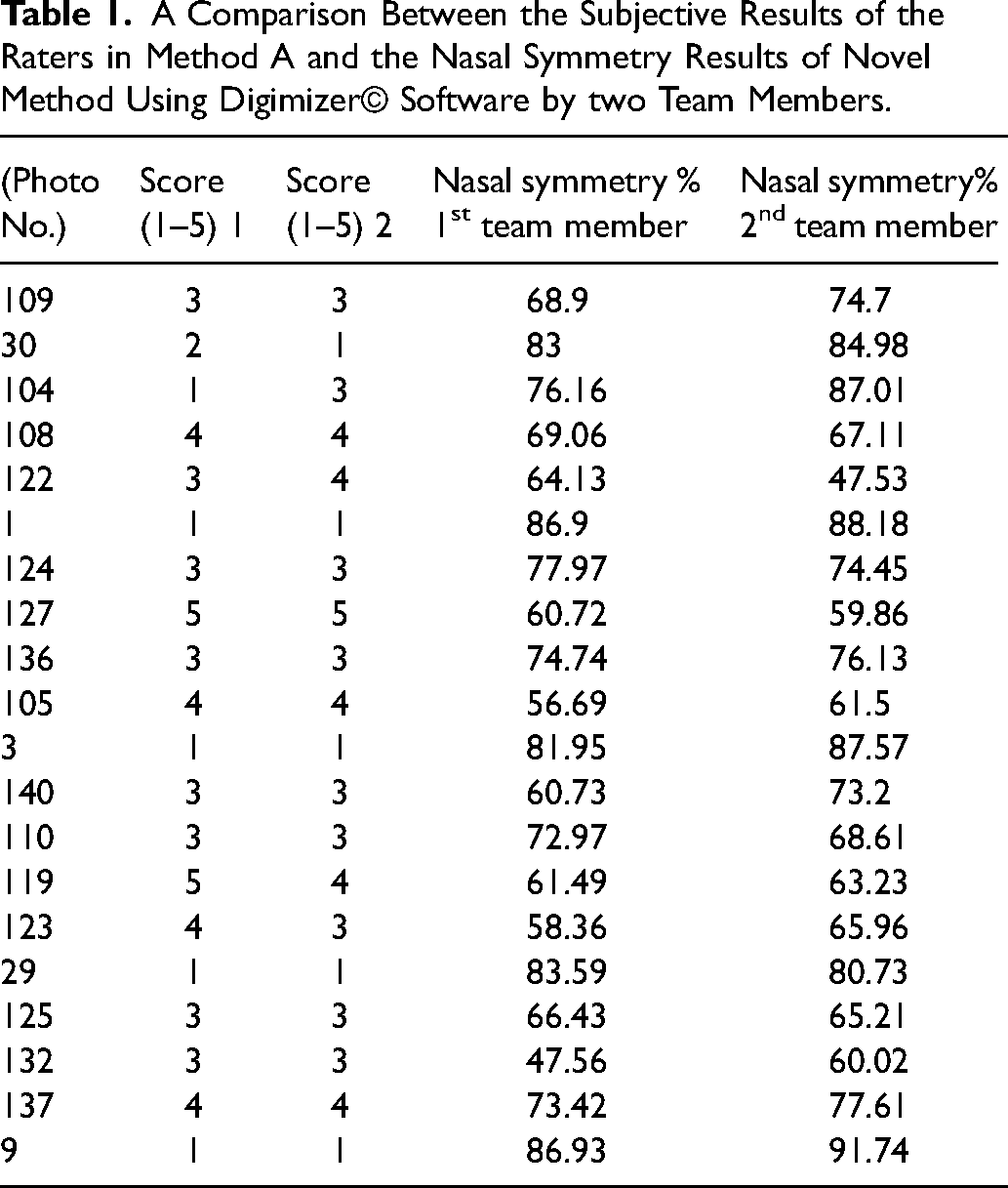
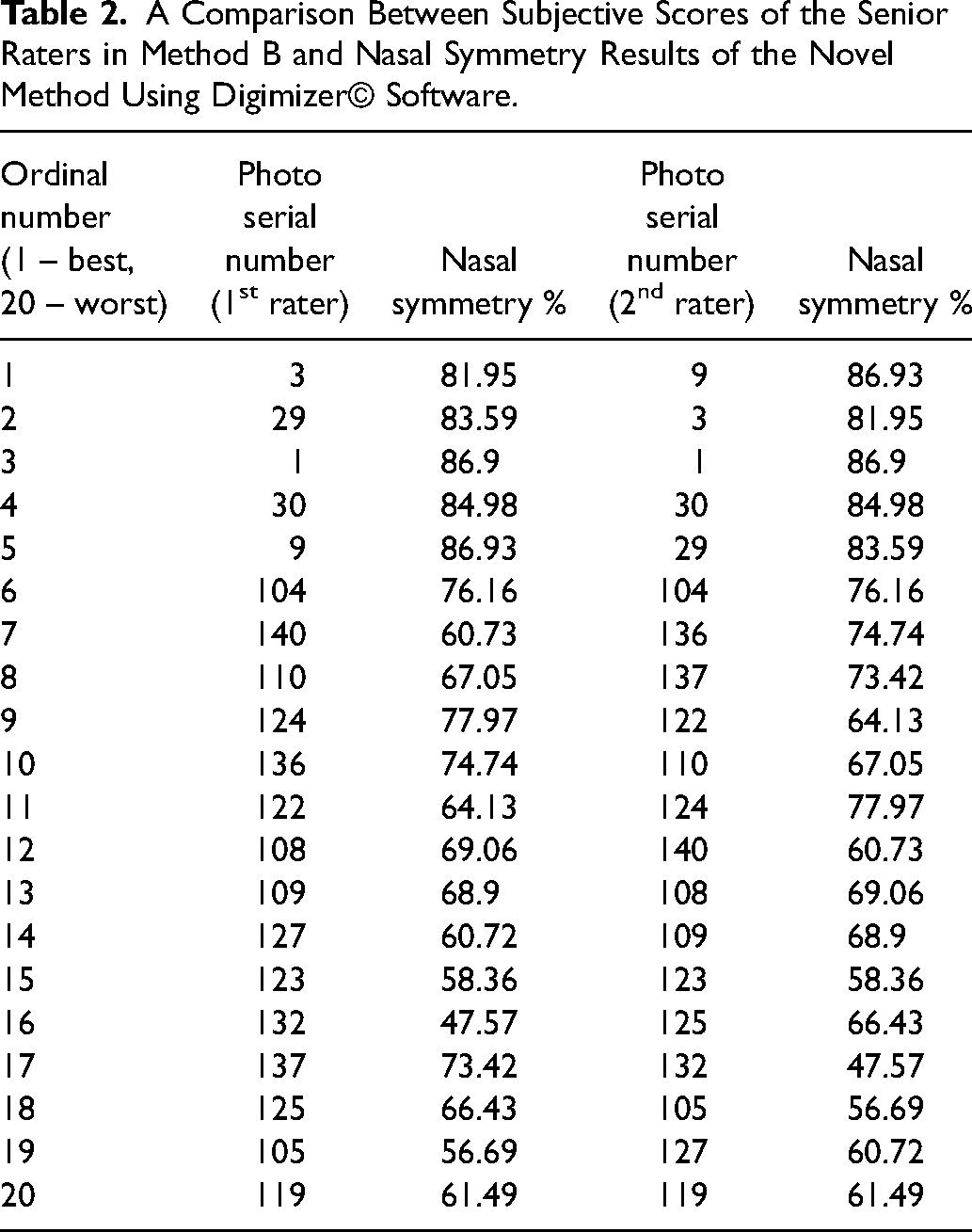
The nasal symmetry analysis correlated with the surgeons’ subjective ratings in both the Numerical ranking method (Method A) at 73% for the 1st surgeons’ scores (p < 0.001) and 72.6% for the 2nd surgeons’ scores (p < 0.001, Table 1) as well as in the arrangement as spectrum method (Method B) at 87.6% for the 1st surgeons’ scores (p < 0.001) and 77.7% for the 2nd surgeons’ scores (p < 0.001, Figure 3, Table 2). After stratifying for deformity type, we found no significant correlations between methods in the control group. In the IUCL group we found Intra-rater reliability of 82.4% (p < 0.001), Inter-rater reliability of 64.8% (p = 0.009) and a correlation of 72.9% with method B (p = 0.002) and 52.5% (p < 0.05) with method A.
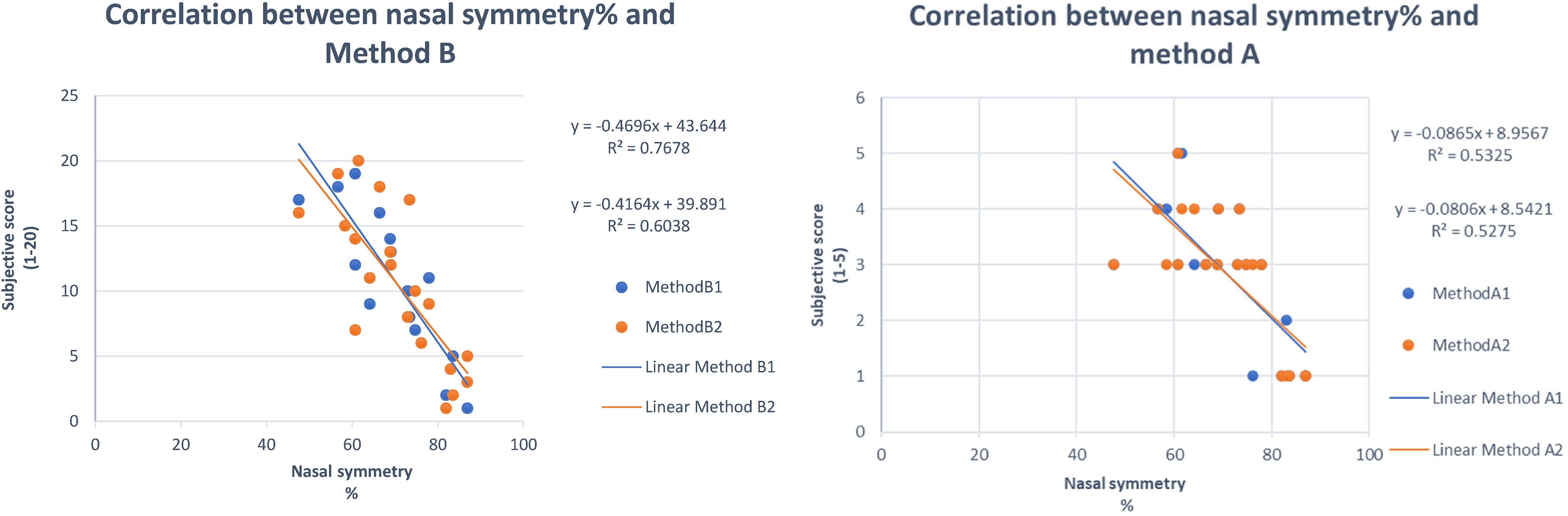
Shows the correlation between the scores of the two senior surgeons who evaluated nasal symmetry using subjective method A and B and the results of symmetry analyses using our novel method, respectively.
A Comparison Between the Subjective Results of the Raters in Method A and the Nasal Symmetry Results of Novel Method Using Digimizer© Software by two Team Members.
A Comparison Between Subjective Scores of the Senior Raters in Method B and Nasal Symmetry Results of the Novel Method Using Digimizer© Software.
We found that the mean nasal symmetry of the non cleft neonates was 83.9% (±5.373, 95% CI 81.893–85.906), 61.815% for the IUCL group (±12.391, 95%CI 58.586–65.044) and 46.664% for the CUCL group (±12.374, 95%CI 38.801–54.526) (Table 3A). No significant variances were found when stratifying for Gender.
(A) Normal Ranges and Mean Nasal Symmetry Percentages in Healthy and CL Patients According to the Novel Method. (B) Mean Differences in Nasal Symmetry Between Non-Cleft and CL Patients According to the Novel Method.
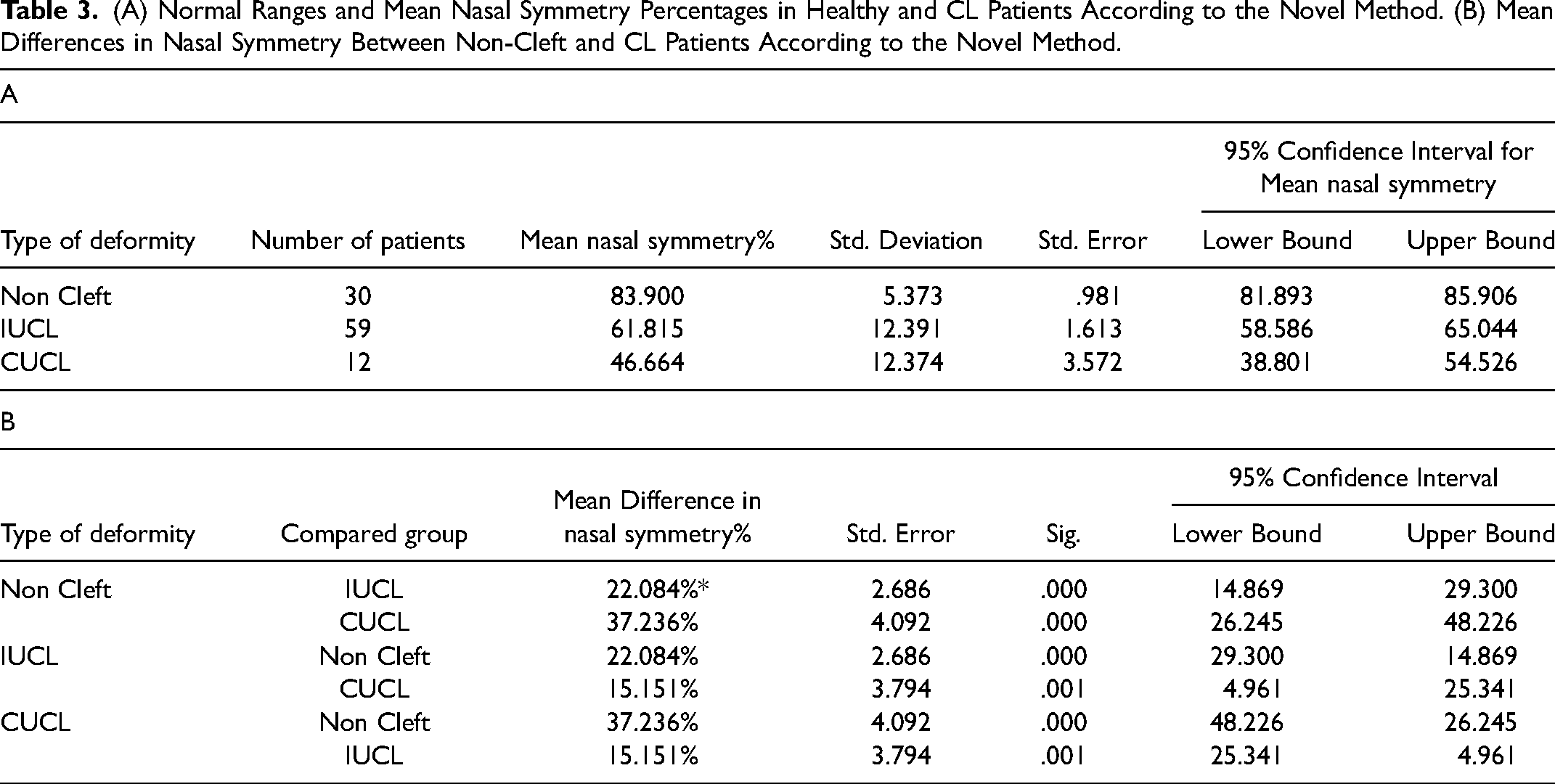
The mean difference in nasal symmetry between the control group and the IUCL group was 22.084% (p < 0.001, 95% CI 14.87–29.3). A mean difference of 37.236% (p < 0.001, 95% CI 26.24–48.22) was found between the control group and the CUCL. The mean difference between the CUCL and the IUCL groups was 15.151% (p = 0.001,95% CI 4.96–25.34) (Table 3B).
Discussion
The Assessment of the surgical results of Cleft lip Surgical repair have been a subject to much debate in the literature.7–12 Various methods were proposed and examined in the attempt to validate a reproducible way of scoring the aesthetic outcome of lip and nasal repair. Subjective methods using evaluation of photos by a panel of professionals varied in the background of the people scoring the results, the portion of the face they were exposed to and had to assess, and the scale according to which they were asked to evaluate the results.15,16 Semi objective methods described, varied in the software used and in the actual method and reference points according to which surgical results were analyzed.17,18 These methods, were compared to subjective methods for validation. There is no consensus of the optimal way of evaluation of esthetic outcome among cleft patients. The subjective methods are biased by the personal perception of beauty and esthetics of the person doing the evaluation, along with his past exposure to surgical results and cleft patients. On the other hand, objective methods require specialized equipment and software, and rely heavily on the quality of the picture provided. In both methods, we evaluate three-dimensional structures through two-dimensional photos. Standardization of the photos used is difficult since the population investigated is small in age and inherently uncooperative. We used photos of incomplete cleft lip where the malformation should be considerabley milder when compared to complete unilateral cleft lip, as to set a higher bar for distinguishing between the cleft and the non cleft subjects.
In the basis of this research, is the assumption that setting nominal values for symmetry both in neonates without facial cleft and in cleft patients, will help to create an objective scale for surgical results according to which it will be possible to evaluate different surgical techniques and aesthetic outcomes. The method offered and examined in the article can become a useful tool for evaluation of pre surgical condition and post-surgical outcome and provide a nominal value of change.
The research used cropped worm's view photos that presented the nasal and lip regions. The worm's view or basal view has already been established as a superior method in evaluating surgical results in cleft lip patiets. 3 The high correlation found between nostril area proportions and subjective surgeon scores of surgical results, indicates that this specific parameter is of essential importance in evaluating aesthetic outcome of surgical cleft lip repair. The limited region of the face exposed for evaluation also reduces the bias in the panel scoring.3,15
At the research at hand nasal symmetry was evaluated for neonates without facial cleft and unilateral cleft patients. A mean nasal symmetry of 83.9% was found in the control group, 61.8% in the incomplete unilateral cleft and 46.6% in the complete unilateral cleft group. The semi-objective method was able to distinguish between cleft patients and patients without any facial cleft with high sensitivity and high specificity. All finding were statistically significant. The research also revealed high inter-rater and intra-rater reliability and good correlation to surgeons’ subjective evaluations even while comparing non-cleft and incomplete cleft lip cases. Upon stratification and comparison of separate groups significance of correlation between the methods of evaluation could not be reached, on account of the small groups of patients. Further investigation is planned on greater number of patients and as a mean to compare aesthetic outcome of different surgical techniques.
Conclusions
This research presents a valid and reproducible method for evaluation of aesthetic outcome and symmetry among cleft patients. The research sets a value of symmetry percentage through which the operator will be able to evaluate surgical results and compare different surgical techniques. Further validation on larger groups of patients is advised to solidify the statistical significance of this method when stratifying for each and every group of patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.