
Abstract
Objective
To document the impact of early follow-up by specialized cleft nurses (SCNs) provided to families affected by cleft lip and/or palate (CL/P) and the status of parental stress, infant feeding and well-being.
Design
Prospective inclusion of a control group, which only received standard care, followed by an intervention group that also received early SCN follow-up.
Setting
The cleft lip and palate team at Oslo University Hospital, Norway.
Participants
Seventy families (69 mothers and 57 fathers) distributed into an intervention group (n = 32) and a control group (n = 38).
Intervention
SCNs provided a consultation at the maternity ward and a follow-up conversation by phone or face-to-face at scheduled times for six months.
Outcome measures
Parental Stress Index (PSI), Perceived Stress Scale (PSS-14), feeding questionnaire, survey of infant diets, weight percentiles.
Results
The mothers reported higher stress scores than the fathers, but in the control group only in the PSI parent domain at T2 and T3 (P = .007, P = .018). Infants in the intervention group used pacifiers less frequently than in the control group (55.2% vs. 81.1%, P = .023). Otherwise, no significant differences were found between the groups. Overall, the infants received less breast milk than norms.
Conclusion
Contextual strategies for early follow-up of families affected by clefts need to be developed, with an emphasis on involving fathers and those parents reporting elevated stress and/or feeding difficulties. There is a need for diagnosis-specific guidelines about the use of pacifiers as well as collaboration between the health professionals involved to increase breastmilk feeding.
Introduction
It is well documented that a cleft lip and/or cleft palate (CL/P) have implications for the affected parents and their infants from birth and in the first year of life in terms of parental stress,1,2 infant feeding and well-being.3,4 Parents need information and benefit highly from support and guidance from health professionals (HPs) with competence in cleft care,1,5 but report unmet informational and supportive needs.6,7 More knowledge is needed about actions in nursing practice that have a positive impact on families’ processes of adjusting to everyday life with an infant with CL/P.
Oral clefts, including cleft lip (CL), with or without cleft palate (CL/P) or cleft palate alone (CP), are among the most commonly known birth defects. 8 Worldwide, this condition affects about one in every 600 newborns 9 and has a prevalence in the Norwegian population of about 2.1 per 1000 live births. 10 Some children born with CL/P have additional anomalies or underlying medical conditions. 11
In the field of CL/P, stress in parents has been studied from different perspectives, using different measures and associated definitions of stress. Psychological stress occurs when an individual perceives that environmental demands exceed his or her adaptive capacity. 12 Hence, parenting stress is defined as the discrepancy between the resources required for the parental role and parents’ perception of being able to cope with these demands. 13 Higher parenting stress levels in mothers of infants with CL/P compared to those without clefts have been reported,2,14 which also suggests that elevated stress may be related to feeding difficulties. 14 A study that also included the fathers found higher levels of perceived stress in both mothers and fathers of children with CL/P compared to normative scores. 1 In contrast, other studies have revealed less distress and parenting stress than norms 15 and lower psychosocial distress and a high degree of positive adjustment. 16 Because high levels of parenting stress are assumed to negatively affect parenting behavior and interaction between parents and their child, 13 it is important to explore the presence of parental stress in this population and whether interventions provided by nurses have an impact on stress levels.
An immediate concern in parents in the postnatal period is related to feeding the infant.7,17 Feeding difficulties, including breastfeeding difficulties, are known to occur more often in infants with CP and cleft lip and palate, with or without additional anomalies, than in infants with CL only due to the palatal anomaly.3,4,18 The infant's sucking pattern is shown to be less efficient14,19 and may involve distress during feeding, such as nasal regurgitation, coughing, choking, gagging and excessive air intake. 4 To ensure adequate nutritional intake in these infants, a variety of feeding bottles are used. No bottle seems to have advantages regarding weight gain,14,20 though Medela Feeder® seems to be widely used.21,22 The use of a nasogastric feeding tube is also frequently reported in this population.21,23 It is shown that infants with CL/P receive less breast milk than infants without clefts.23,24 Although breast milk is considered the best nutrition for newborns worldwide, 25 the difficulties caused by the cleft, as described above, and lack of advice on breast milk- and breastfeeding 18 might cause lower intake of breast milk in this population. Additionally, more knowledge is needed about the transition to solid foods and if early follow-up of families by cleft nurses influences aspects of feeding and nutrition in these infants.
Well-being in infants with CL/P might be affected by the above-mentioned excessive air intake, which is among the suggested causes of infant colic and is clearly demanding for infants and their parents. 26 Colic is defined as crying for three or more hours a day, three or more days a week for three weeks or more 27 and it occurs in 5-19% of healthy infants. 28 Even though there are descriptions of colic in infants with CL/P, 29 it is sparsely documented.
Another aspect of infant well-being is the use of a pacifier to meet the infant's non-nutritive sucking needs. Among the benefits are the calming effect used to prevent pain and anxiety. Potential negative effects are breastfeeding difficulties, an increased risk of otitis media and dental malocclusion, particularly with prolonged use.25,30 In the field of CL/P, studies report a wide range of usage of pacifiers, from 46.1% who found it beneficial 21 down to zero, 31 while lower usage than in children without CL/P has been demonstrated. 32 Knowledge-based recommendations for the use of pacifiers in infants with CL/P seem to be missing.
There are conflicting findings on birth weight and growth in infants with CL/P. Lower birth weight 33 and differences in neonatal weight gain between cleft types 22 have been reported. By contrast, others have found similar weight and growth in infants with CL/P as in the rest of the population and argue that these findings are due to the contribution of specialist cleft nurses 23 and that parental feeding education may have positive effects on growth. 34
Successful follow-up provided by HPs to families affected by clefts involves immediate support after birth and home visits focusing on information, support and feeding advice.24,35 Although some researchers have compared interventions in practice,21,36,37 there is still a need to enhance knowledge of how HPs best can help parents to adjust to the challenges of CL/P. The aim of the present study was to document the impact of an intervention provided to parents by specialist cleft nurses (SCNs) compared to a control group, in addition to providing an overview of the following parameters:
Stress in mothers and fathers Infant feeding, nutrition and growth Use of pacifiers and incidence of colic in the infants
Method and Measures
Design
This is a prospective, longitudinal study 38 of families with infants affected by CL/P. About half of the families received standard care, while the other half also received follow-up by an SCN.
Setting
The study was conducted at Oslo University Hospital, which is the location of one of two multidisciplinary teams responsible for the treatment of CL/P in Norway. The Norwegian state covers most treatment expenses and traveling costs to hospital for patients and caregivers. In addition, patients and caregivers receive health care provided to all Norwegian citizens by law. 39 That includes pregnancy and maternity care, specialist health care if needed, and follow-up consultations at a child health clinic by public health nurses, midwives, general practitioners and other HPs. 40 Infants born with CL/P undergo surgical interventions one to three times during the first year depending on the cleft type, cleft lip surgery at the age of 3-5 months (often in two stages when the cleft is bilateral) and cleft palate surgery at one year.
Procedure
Parents of infants with CL/P who were referred to the cleft team in Oslo from one of 18 maternity wards under the South-Eastern Norway Regional Health Authority were asked to participate on an ongoing basis. The parents needed to speak, read, and write Norwegian and to be referred in time for T1 (one month after birth). Parents of infants with additional anomalies or other health problems were also included. Participants in the control group were included in 2015-2016, and those in the intervention group in 2016-2017. Participants in the control group were given written study information by mail, while the intervention group received this from the maternity ward staff. The primary researcher (1) then contacted potential participants and collected signed consent forms. The participating parents completed questionnaires at one month (T1), six months (T2) and 13 months (T3) after the birth (Figure 1). The questionnaires were sent in the mail to each participant, and completed questionnaires were returned to the primary researcher in a prepaid envelope. All participants were contacted by phone before each measurement point and after 3-4 weeks if a reminder was needed. The control group received standard care provided by cleft nurses, and the intervention group received an intervention in addition to standard care. Five cleft nurses, with 2-30 years of experience in the cleft team, performed the interventions. They took a three-day course in cleft care prior to the intervention. These SCNs documented the care actions they provided on a checklist. The data collection was completed by the end of 2018. This study is part of a larger study that has documented parents’ use of the internet, discharge information, response to follow-up care by HPs, coping difficulties and infant admissions to the neonatal intensive care unit. 41
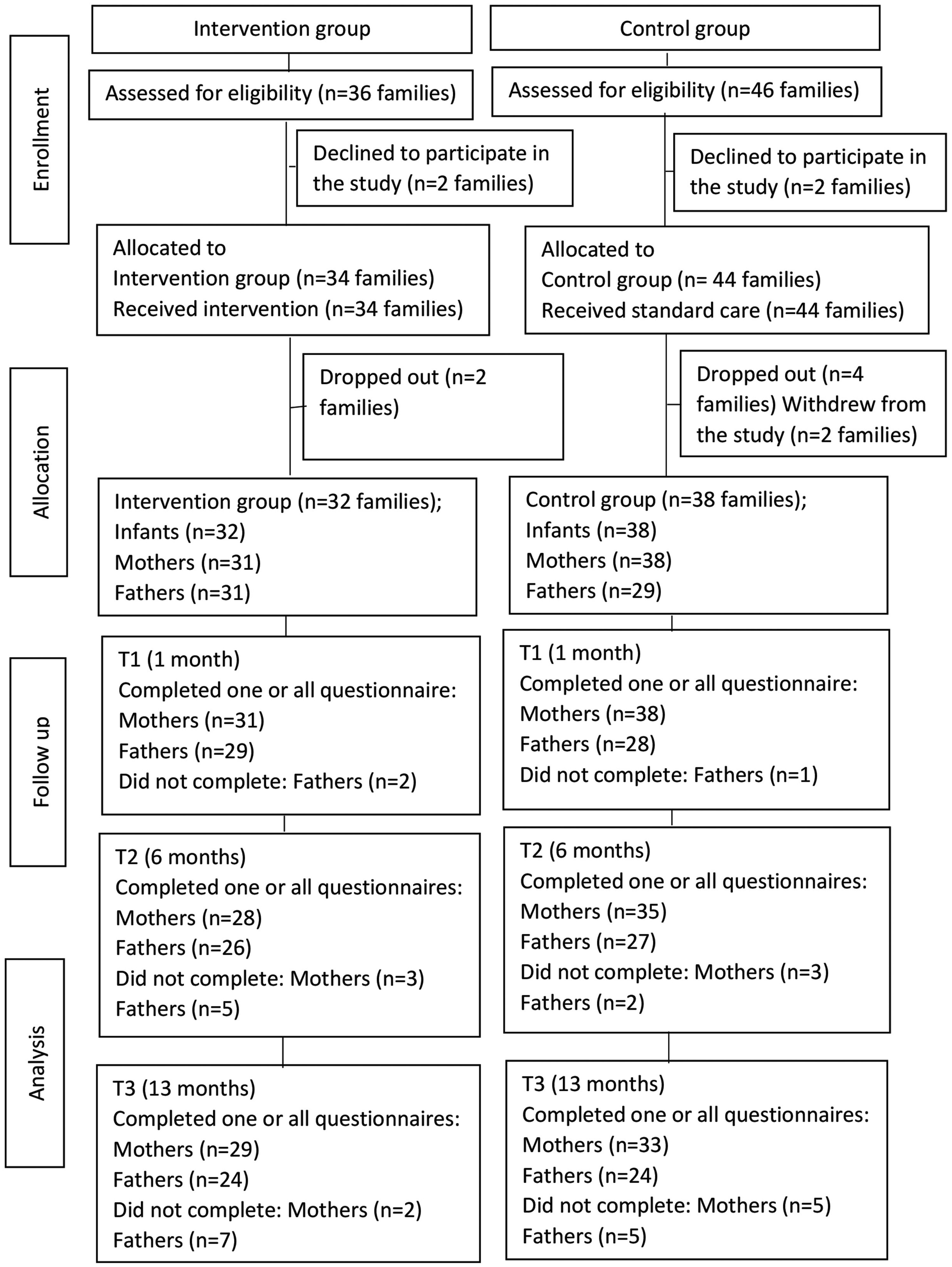
CONSORT flow chart.
Content of standard care provided by cleft nurses
An experienced cleft nurse contacted the mothers by phone within 2-4 weeks of referral from the birth hospital to provide information on care, feeding and treatment unless the families or other HPs had made an earlier request. A contact phone number was available two hours a week for parents and other interested parties. The families attended a one-day course for families with infants with clefts 4-10 weeks after birth. The course is held by the cleft team and consists of an examination of the infants by a cleft surgeon and information and advice from a speech pathologist, psychologist, orthodontist, social worker, patient representative and cleft nurses.
Content of the intervention provided by SCNs
A visit to the maternity ward within 36 h of referral from the birth hospital with the presence of mother, father and the infant. The SCNs provided information about the diagnosis, treatment and feeding (orally and in writing) to the parents, to the staff at the maternity ward and to the health visitor at the child health clinic. The Medela Haberman® and Grieg Easyfeed® bottles were demonstrated and provided free of charge. Telephone conversations were provided at one, three, and eight weeks and at six months after birth to provide cleft-related information and support and to refer to specialists or arrange a visit to the hospital as needed. The SCNs were available on the phone in the daytime on weekdays for parents and HPs. This intervention was provided in addition to the standard care described above.
Ethical Considerations
The Data Protection Office of Oslo University Hospital approved the study (Reference number: 2014/17828). The study was discussed and exempt from review by the Regional Committee for Medical and Health Research Ethics, Section South-East C, Norway (2014/1947 C) and could be implemented without their approval. It was registered at ClinicalTrials.gov. (NCT02415361). The participants signed a consent form after receiving oral and written information about the study.
Measures
Statistical Analysis
Analysis was performed using SPSS 26 (IBM Corp., Armonk, NY) and Stata 17 (StataCorp LLC, College Station, TX). To calculate effect size, Cohen's d was used. 48 Due to expectations of a medium/strong effect for both mothers and fathers equivalent to an assumed mean difference between groups of 0.8 relative to the standard deviation, we needed to include 26 mothers and 26 fathers in each group to obtain 80% statistical power at the 5% significance level using an independent sample t-test. Descriptive statistics of means and standard deviations for the continuous variables and counts and percentages for the categorical variables were used to summarize the data. Group differences in the continuous variables were analyzed using the independent sample t-test. Pearson's chi-square test and Fisher's exact test were used for group comparison of categorical variables as appropriate. A two-sided P value of <.05 was considered statistically significant.
Results
Demographic and Baseline Data
Participants in this study consisted of mothers and fathers of 70 infants, where 32 families belonged to the intervention group and 38 to the control group. There were no significant differences between the parents in baseline data at T1. Apparent differences, albeit not significant, were found in the infants’ gender, cleft type and weight. The families in the intervention group had their first contact with the cleft team at 1.5 (SD 1.4) days after the birth, while for the control group it was at 8.8 (SD 7.9) days, P = .000 (Table 1).
Baseline and Clinical Characteristics: Numbers + % Unless Otherwise Stated.
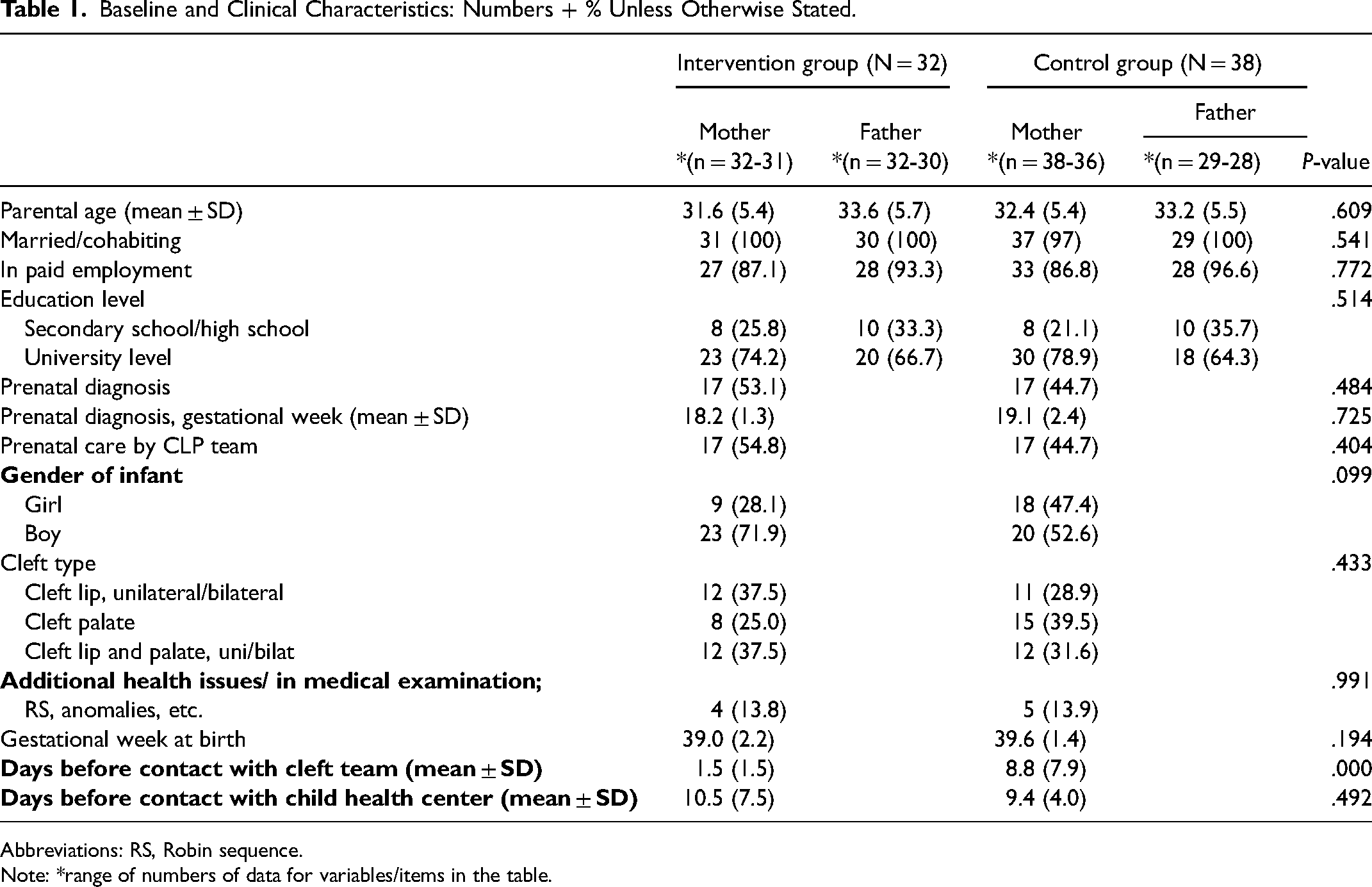
Abbreviations: RS, Robin sequence.
Note: *range of numbers of data for variables/items in the table.
Parenting Stress Index (PSI)
A total of 334 PSI questionnaires, distributed at T1, T2, and T3, were completed by the participants (Table 2). Four questionnaires were excluded in accordance with the manual because of missing items and subscales. The mean defensive score was above the cutoff of 24 in both groups at all measurement points, indicating that the participants responded in a non-defensive manner. In the control group, mothers had higher PSI scores than fathers in the parent domain at T2 (P = .007) and T3 (P = .018) (Supplemental Table S1), but otherwise no significant differences were found between the groups (Table 2). The mean total stress scores were below the 50th percentile for both parents in both groups at all measurement times, with a decrease from one (T1) to six months (T2) and an increase at thirteen months (T3). The child domain and life stress scores were below the 65th percentile, while the parent domain was below the 50th percentile.
Parenting Stress Index (PSI) and Perceived Stress Scale (PSS-14): Comparison of Means and SD Between Groups and Parents.
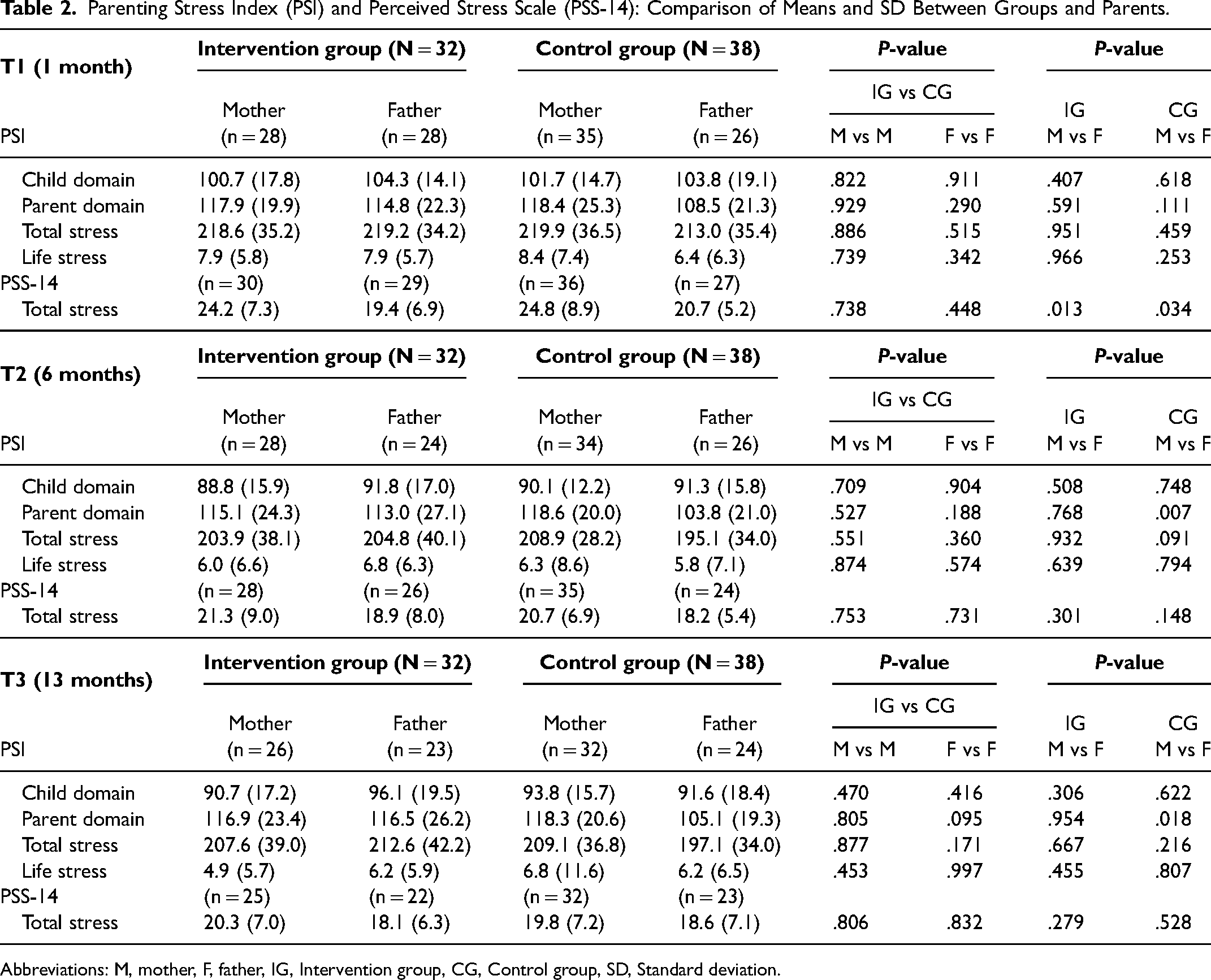
Abbreviations: M, mother, F, father, IG, Intervention group, CG, Control group, SD, Standard deviation.
Perceived Stress Scale (PSS-14)
A total of 337 PSS-14 questionnaires, distributed at T1, T2, and T3, were completed by the participants (Table 2). Mothers in both groups reported higher total stress scores than fathers (intervention group, P = .013; control group, P = .034) and an average score slightly above 24 at T1. Otherwise, no significant differences were found between the groups at any measurement time (Table 2). The total stress scores decreased at T2 and T3 for both mothers and fathers; here, the mothers had generally higher scores, but below the score of 24.
Feeding Questionnaire
Fewer infants in the intervention group used a pacifier than those in the control group (P = .023) at T1. No significant group differences were found for the other variables included in the feeding questionnaire (Table 3). None of the infants were fed by nasogastric tube alone at any measurement points.
Aspects of Feeding: Comparison of Number + % Between the Groups.
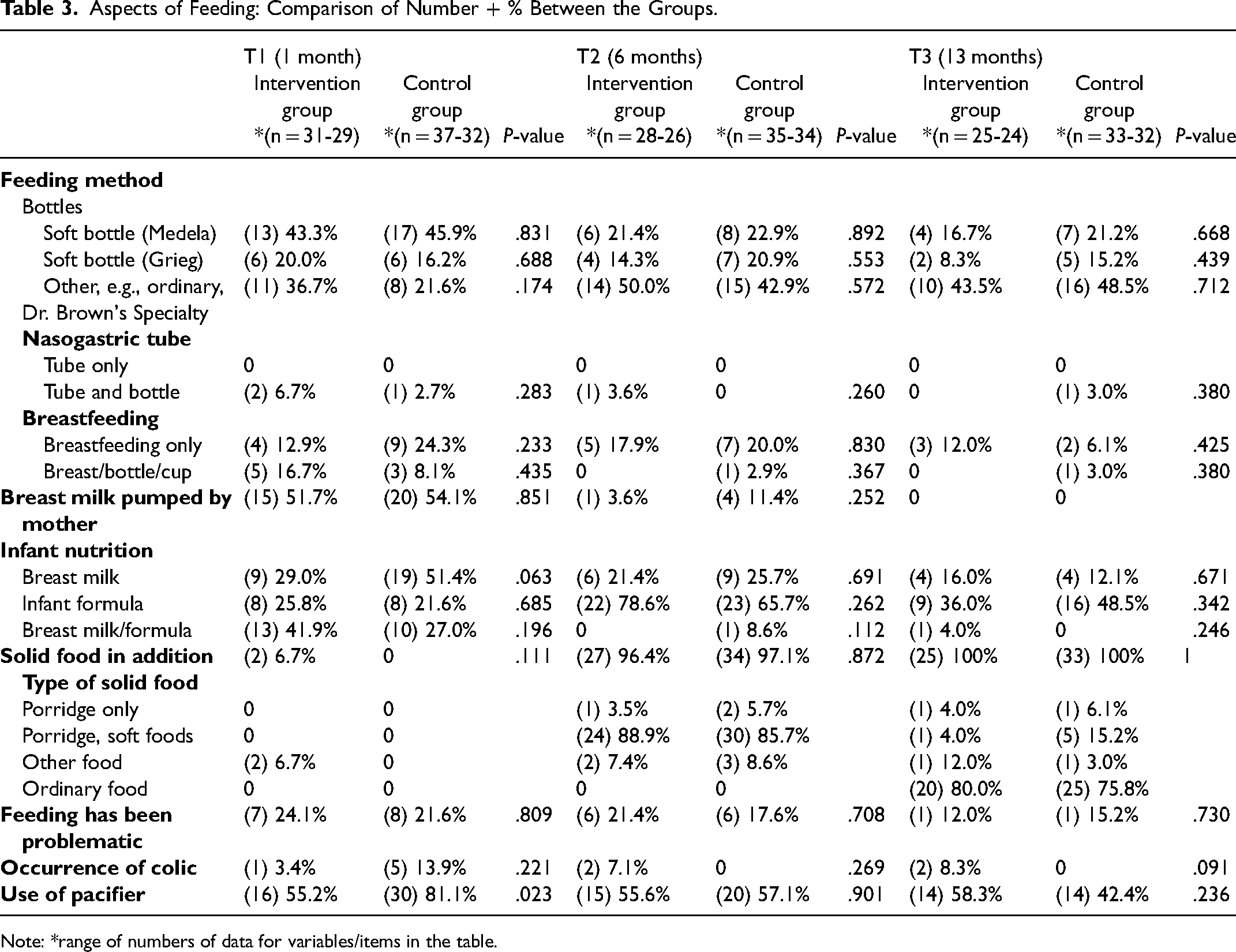
Note: *range of numbers of data for variables/items in the table.
Survey of Infant Diets
A total of 59 parents, 58 mothers and 1 father, completed the questionnaire at T3, representing 26 infants in the intervention group and 33 in the control group. The groups were not significantly different for any variable measured. At the maternity ward, 9 (34.6%) infants in the intervention group and 10 (32.3%) in the control group received breast milk alone while 22 (84.6%) and 29 (93.6%), respectively, received breast milk supplemented by other liquids, mostly infant formula.
Weight of the Infants
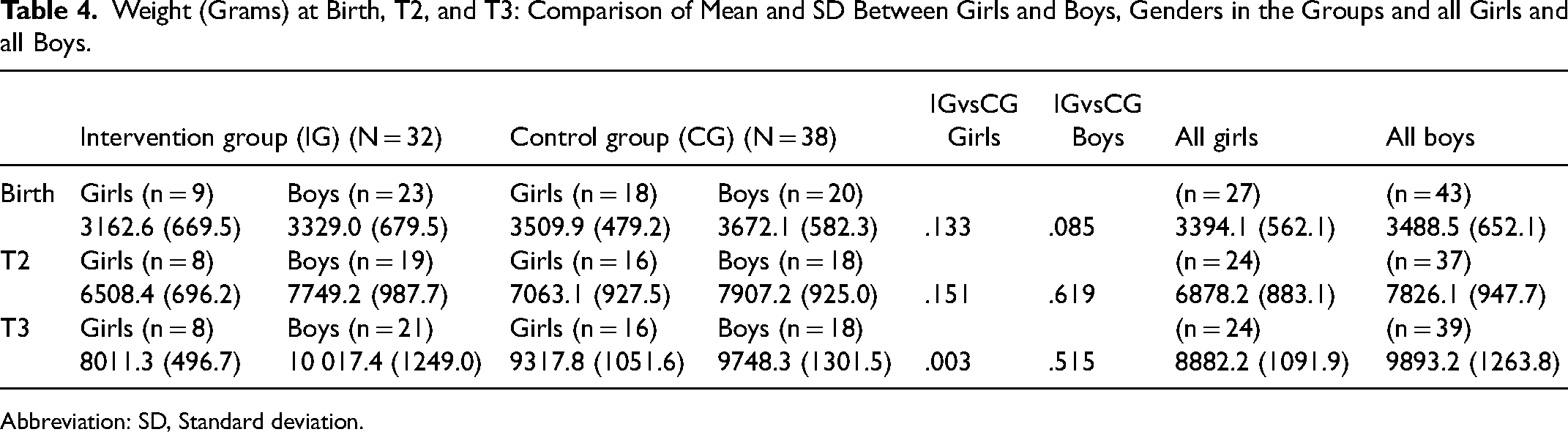
Parents of 57 infants, 24 in the intervention group and 33 in the control group, reported their infants’ weight at T3. The number of reported measurements of each infant varied. Most infants were 12 months old at the last measurement point, except for seven in the intervention group (one was 11 months and six were 13 months) and five in the control group (two were eleven months and three were 13 months). The girls in the intervention group had a lower birth weight than those in the control group, and weighed less at T2 and significantly less at T3 (P = .003) than the girls in the control group. Compared to the boys in the control group, those in the intervention group weighed less at birth and at T2 but more at T3, though not significantly (Table 4). Overall, the weights of the study participants were close to the 50th percentile 47 at birth, T2, and T3, except for girls in the intervention group at T2 (Figure 2).
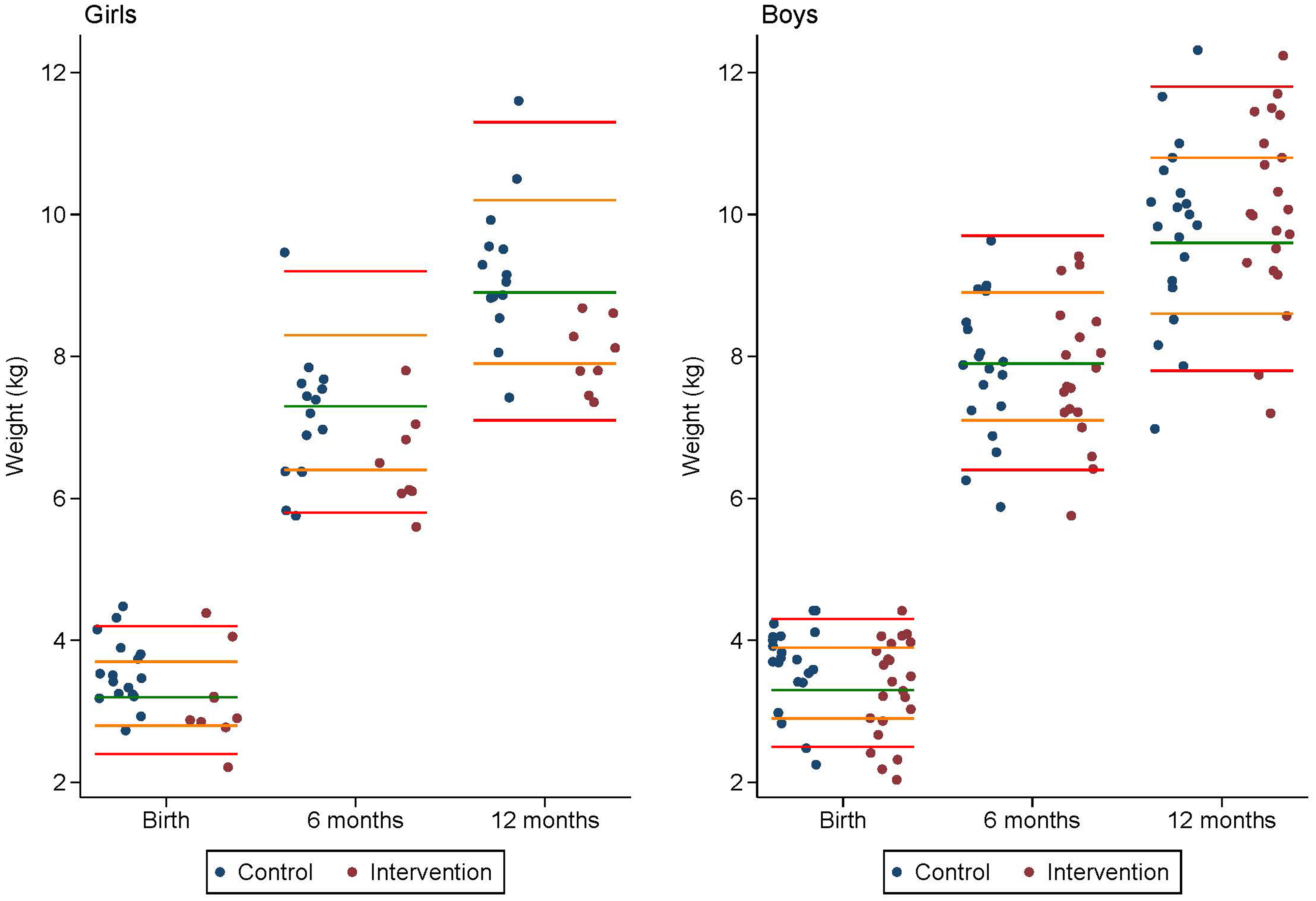
Illustration of weight for girls and boys in relation to WHO growth percentiles at the 3rd, 15th, 50th, 85th and 97th percentile.
Weight (Grams) at Birth, T2, and T3: Comparison of Mean and SD Between Girls and Boys, Genders in the Groups and all Girls and all Boys.
Abbreviation: SD, Standard deviation.
Discussion
In this study, we have documented the impact of an intervention provided by an SCN after the birth of an infant with CL/P compared to a control group who received standard care only. The findings revealed that the infants in the intervention group used a pacifier less than the infants in the control group. There were no group differences regarding parental stress but there were differences in the parent domain of the PSI between mothers and fathers in the control group, with mothers reporting higher stress. Higher perceived stress in mothers was also found at T1, although overall stress seemed to be within the normal range. The groups did not appear to differ in aspects of feeding, type of nutrition and colic. However, the group as a whole received less breast milk than the norm.
Impact of the Intervention and status of Stress in Parents
One key finding in this study is that mothers scored higher than fathers in the control group on the parent domain of the PSI (on items related to their physical health, freedom restricted by the infant, depression symptoms and lack of emotional and active support from their partner). This is in line with findings in the general population showing more stress (and less well-being) in mothers than fathers, especially when children were of young age. 49 This contrasts with the scores in the intervention group, where the difference between mothers and fathers was minor. The findings may indicate that the intervention strengthened fathers’ participation in the child's care by being included in the visit at the maternity ward and by being invited to take part in the dialogue with the CNS. This might have led to an equalization of stress between mothers and fathers, up to the mothers’ level, but still within the 50th percentile. A greater similarity in stress score between genders may lead to a better understanding of the situation and parental role. Overall, findings in this study reveal a total stress score of mothers and fathers of infants with clefts within the 50th percentile in both groups at all measurement times for PSI, thus suggesting that the parents in this study reported parenting stress within a normal range. Further, the study findings may underline the importance of HPs developing strategies to include fathers in the child's care. Solberg et al. (2018) found that fathers want to play a more active role and to be more included in care. That requires a greater focus on fathers as independent and equal caregivers. 50
Impact of the Intervention and status of Feeding
Findings did not reveal significant differences between the groups in feeding method (breastfeeding, bottle-feeding, nasogastric tube feeding), type of nutrition (breast milk, formula, solid food) or parents’ perception of feeding difficulties. Even though the intervention consists of follow-up immediately after birth, which is considered valuable,23,35 the intervention might have been too marginal or insufficient to make a difference or solve all the feeding difficulties. Further, subsequent care was provided by telephone, which some perceive as unsuitable for advice on feeding. 20 However, other researchers have revealed that despite early team care and feeding interventions, mothers of infants with CL/P reported more challenges with feeding and growth (and stress) than those without clefts. 14 Since feeding difficulties are more frequent in infants with additional problems, 4 some parents might find infant feeding demanding despite follow-up. Although, parents in both groups reported fewer feeding difficulties than others,21,51 it is worth noting that the comparison is challenging because feeding difficulties might be defined differently and are not specified in this study. Nevertheless, the participants in this study were generally well educated, in paid employment and living together. These factors might increase parents’ ability to access the help they need, either from the cleft team or from others. Mothers’ strength and determination to seek information from different sources when they meet challenges has been reported. 7 More knowledge is needed on how to support parents who report feeding difficulties in their infants.
Impact of the Intervention and status of Nutrition
The findings in this study correspond with those of studies reporting that infants with clefts receive less breast milk than those without clefts.23,24,52 At the maternity ward, 34.6% of infants in the intervention group and 32.3% in the control group were breast milk fed with supplements of other liquids, while normative data is 68%. 46 This entails that infants with clefts do not reach the goals and recommendations for breast milk feeding in an WHO guideline. 25 Since breast milk is the best nutrition for infants, HPs should provide evidence-based information, including practical advice, in order to increase breast milk intake. 18 On the other hand, the stress that might occur in parents, particularly mothers, 14 must be acknowledged. Further, parents should make knowledge-based decisions based on their particular resources, and receive non-paternalistic and supportive care and advice from HPs. Overall, infants in the present study seemed to be introduced to solid food by six months of age and receive the type of nutrition that is recommended to infants in general. 53
Impact of the Intervention and status of Colic and the use of a Pacifier
Based on the lower usage of pacifier in the intervention group (55.2%) than in the control group (81.1%) at T1, the intervention may have increased parents’ knowledge about the cleft, e.g., infants’ ability to keep a pacifier in the mouth as well as postoperative restrictions. The cultural aspect of pacifier use as well as recommendations given to parents are argued to have a great impact on use.21,31 More knowledge is needed on risks and benefits of the use of pacifiers in infants with CL/P in order to provide parents with evidence-based recommendations. Parents in the control group reported more colic at T1 than those in the intervention group. Although the numbers are small, one may speculate that the SCNs’ information about feeding might have led to less air intake because of better feeding positions, bottles, etc. Overall, the small numbers of parents who reported infant colic might suggest that infants with CL/P suffer less from colic, but more knowledge is needed.
Impact of the Intervention and status of Weight
This study found that girls in the intervention group had (non-significantly) lower birth weight than those in the control group, even lower weight at T2 and significantly lower weight at T3 (P = .003). In light of this, the contribution of the SCN might not have had a positive impact on weight gain. On the other hand, there were few girls in the intervention group, which makes comparison difficult. Additionally, they may have had undetected additional issues 11 or feeding difficulties that needed a more comprehensive approach. The weight of the whole study population compared to WHO growth standards (Figure 2) shows that the infants were close to the 50th percentile at all measurement times, apart from girls in the intervention group at T2. This is in contrast to another study that reported lower birth weight in newborns with clefts than in those without clefts. 33
Strengths and Limitations
The study design, consisting of an intervention and comparison of the results with a control group in a longitudinal perspective, provides an insight into the impacts of early follow-up as well as the status of aspects of parental stress, infant feeding and well-being in families affected by CL/P. The study was conducted in a centralized treatment setting with a sample that appears to be representative because most potential participants who met the inclusion criteria gave their consent to participate. The high number of participating fathers needs to be highlighted, as research often includes mothers, not both parents. 50
Among the limitations that need to be acknowledged is the lack of heterogeneity between the infants in the groups in terms of birthweight, cleft types and gender distribution. The fact that more of the infants in the control group were born with CP than those in the intervention group could have affected the results because a CP is reported to increase feeding difficulties 4 and occur with higher incidence of other anomalies than in those with CL or cleft lip and palate. 11 In addition, other factors that are not documented may influence infant feeding, well-being and parental stress in a longitudinal perspective, e.g., how infants and parents experience surgical interventions with potential stress and complications, travel distances to hospital and parents’ psychosocial status. The characteristics of this study sample is a well-documented methodological challenge described in craniofacial research because samples do not contain large enough subgroups. 54 Analysis was performed without differentiating between the infants’ cleft types and with limited knowledge about the impact of the cleft type.
We considered that a randomized controlled trial was not a suitable method for this study, despite the strength of this method in comparing groups. 38 By studying the control group before the intervention group, we aimed to avoid potential bias related to contamination of the groups. 38 In hospital settings where many HPs are involved, it might be challenging to distinguish between the groups, with a risk of providing part of the care for the intervention group to the control group and vice versa. By leaving out the process of randomization, we also avoided the ethical challenge of some families receiving early follow-up while others did not, when such care could be most needed. On the other hand, the fact that the control group was studied one year before the intervention group could have meant that the groups were explored in different contexts. However, there were no structural changes in the organization of health care in that period.
The use of multiple statistical tests needs to be acknowledged as a limitation. The risk of drawing the wrong conclusion is present with multiple testing due to a greater probability of false positive findings. 55 It is possible to adjust for multiplicity, but there is no consensus on if, how or when. 56 In this study, we chose not to adjust for multiplicity and kept the significance level at 5% despite the limitations. We also reported results at the item level because of clinical relevance, e.g., awareness and knowledge of potential differences between mothers’ and fathers’ is of great interest in improving care strategies.
Among the measures used in this study, the PSI long version is a long and comprehensive questionnaire. Some participants commented that certain items were difficult to answer, unsuited to their infant's age and complicated to fill in. This concurs with experiences from another study in the field of CL/P. 57 On the other hand, measuring stress from different perspectives might provide knowledge of individual experiences and interventions that might be effective, and using similar instruments across different studies should be prioritized for methodological reasons to enable findings to be compared. 54 PSI may be one among other relevant and validated tools for the measurement of parental stress, but the PSI long version could be replaced by the PSI short version to lessen the burden for the participants. The feeding questionnaire was developed for the purpose of the study and included patient- reported data on feeding. Although it is considered to be relevant and easy to complete, it has not been tested for internal or external validity, which thus limits the value of the results. 38
All participants who responded at at least one of the three measurement points were included. They were also included if they responded up to two months after a measurement point, which might have led to recall bias. 38 On the other hand, this was considered an acceptable time frame for the participants to recall.
To our knowledge, there is no exact definition of a “feeding difficulty” in the cleft literature. Some refer to functional challenges in infants 58 while others include psychosocial difficulties and practical strains.17,59 Participants may therefore have different criteria for what a feeding difficulty consists of, which may lead to imprecise comparison between participants and between studies.
The present study was conducted in a high-income country where the health service is regulated by guidelines and laws and mostly free of charge. Therefore, the findings may not be generalizable to other countries where health and cleft care are organized differently.
Summary
This study provides an important insight into the impacts of initial follow-up by SCNs as well as an overall status on aspects of stress in parents, infant feeding and well-being in a Norwegian population of families affected by CL/P. More attention should be paid to parents, both mothers and fathers, who report elevated stress and/or feeding difficulties in their infants, in order to create efficient and context-dependent strategies to meet their needs. Strategies are also needed to provide parents with evidence-based advice on pacifier use and to increase breastmilk feeding.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241231524 - Supplemental material for Parental Stress, Infant Feeding and Well-being in Families Affected by Cleft Lip and/or Cleft Palate: The Impact of Early Follow-up
Supplemental material, sj-docx-1-cpc-10.1177_10556656241231524 for Parental Stress, Infant Feeding and Well-being in Families Affected by Cleft Lip and/or Cleft Palate: The Impact of Early Follow-up by Nina Ellefsen Lindberg, Nina Margrethe Kynø, Kristin Billaud Feragen, Are Hugo Pripp and Kim Alexander Tønseth in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656241231524 - Supplemental material for Parental Stress, Infant Feeding and Well-being in Families Affected by Cleft Lip and/or Cleft Palate: The Impact of Early Follow-up
Supplemental material, sj-docx-2-cpc-10.1177_10556656241231524 for Parental Stress, Infant Feeding and Well-being in Families Affected by Cleft Lip and/or Cleft Palate: The Impact of Early Follow-up by Nina Ellefsen Lindberg, Nina Margrethe Kynø, Kristin Billaud Feragen, Are Hugo Pripp and Kim Alexander Tønseth in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
Many thanks to the mothers and fathers who took their time to participate in this study. Special thanks to the SCN's; Linn-Beate Ask, Wenche Nyborg Mongstad, Barbro Skogfelt, Ann Magritt Semmingsen and Ida Johansson Ringvold who conscientiously carried out the intervention. Thanks to the Cleft lip and Palate Organization in Norway for the enthusiasm for the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.