
Abstract
Objective
This study compares the impact of surgical site infiltration of local anesthesia alone to surgical site infiltration plus suprazygomatic maxillary nerve block (SMB) in non-syndromic and syndromic children undergoing primary palatoplasty.
Design
Retrospective cohort study of intra- and post-operative outcomes and opioid utilization in children undergoing palatoplasty by a single surgeon.
Setting
Urban, academic, tertiary care children's hospital.
Patients, Participants
Children 24 months or younger undergoing primary palatoplasty were included (n = 102). Exclusion criteria were concurrent painful procedures, history of neonatal abstinence syndrome, and nurse-controlled analgesia (n = 30).
Interventions
All patients received epinephrine-containing local anesthetic infiltrated at the surgical site. Fifty-seven also underwent placement of ultrasound-guided SMB.
Main Outcome Measure(s)
Intra-operative opioid requirement, duration of anesthesia, time to wake up, post-operative opioid requirement, hypoxemic episodes, need for respiratory support, FLACC scores, and length of stay.
Results
When controlling for syndromic status and cleft phenotype, SMB was associated with a 57% reduction in intraoperative opioid requirements (95% CI = 15–81%, p = 0.024) but also with a 29% (∼5-min) increase in wake-up time post-surgery (95% CI = 3–50%, p = 0.048). Postoperatively, SMB was linked to a 18% reduction in hospital stay length (95% CI = 2–31%, p = 0.027) and a 88% reduction in opioid requirements within 24 h after surgery (p = 0.006). Desaturations and new respiratory support requirements were unaffected by SMB.
Conclusions
Compared to surgical site infiltration of local anesthetic alone, adding SMB reduces intra- and postoperative narcotic requirements and decreases length of stay. These benefits apply to both syndromic and non-syndromic children. SMB does not meaningfully affect respiratory outcomes.
Keywords
Introduction
Primary palatoplasty is an essential part of care for children with cleft palate but is widely considered to be painful. Perioperative pain can be severe enough to warrant intravenous opioids. 1 While opioids are potent in suppressing pain, their adverse effects on ventilatory and gastrointestinal functions increasingly warrant a multimodal, narcotic-sparing approach to pain control.2–4 To this end, regional anesthesia techniques, such as suprazygomatic maxillary nerve block (SMB), have emerged as valuable tools to manage pain in these children.5–7 Previous studies have demonstrated that SMB provides effective analgesia 8 and reduces narcotic requirements after palatoplasty compared to no intervention or placebo,6,9 and to other regional blocks. 10 However, studies comparing SMB to infiltration of local anesthetic at the surgical site, which is common practice for palatoplasty, have been less conclusive. Subgroup analysis of a small number of non-syndromic patients at our hospital suggested SMB provided superior analgesia to infiltration of local anesthetic in the surgical site alone, 7 however another similarly powered study did not demonstrate the same effect.11,12 Therefore, further exploration of the impact of SMB compared to surgical site infiltration of local anesthetic for palatoplasty is warranted.
Additionally, the efficacy of SMB in more medically complex syndromic children has not been thoroughly explored. Such children, including those with named syndromes and other major anomalies, constitute approximately half of all cases of cleft palate. 13 These individuals often present a more challenging physiological landscape and may have a history of narcotic exposure from previous interventions. For example, children with Robin sequence or CHARGE syndrome commonly exhibit preexisting airway and respiratory problems,14–17 and a history of prior operations potentially resulting in repeated narcotic exposure. Given these complexities, it is crucial to explore whether the opioid-sparing effect of SMB applies to this population and if that translates into improved respiratory function postoperatively.
We examined the impact of SMB on intraoperative and postoperative opioid usage and on respiratory outcomes in children undergoing palatoplasty, including both syndromic and non-syndromic cleft palate populations. Our hypotheses are that: 1) the addition of SMB delivers analgesia that is superior to that achieved solely with infiltration of local anesthetic at the surgical site, 2) SMB offers similar opioid-sparing benefits in syndromic children as has been reported in non-syndromic children,7,9 and, 3) the addition of SMB improves respiratory outcomes after palatoplasty, which is particularly meaningful for the syndromic population.
Methods
Eligibility Criteria
This retrospective cohort study, approved by the Institutional Review Board (IRB-P00033895), involved a chart review of children 24 months and younger who underwent primary palatoplasty by a single surgeon between September 2014 and May 2023.
Inclusion Criteria
Patients eligible for inclusion were those who received SMB administered either before or at the conclusion of surgery, as well as those who did not receive any form of regional anesthesia. All patients received infiltration of epinephrine-containing local anesthetic at the surgical site prior to incision. Patients undergoing concurrent minimally painful procedures (such as placement of myringotomy tubes, lingual frenectomy, or diagnostic laryngoscopy and bronchoscopy) were also included. Genesis of the cohorts with and without SMB arises from the fact that the surgeon incorporated SMB more often over time due to increasing availability of anesthesiologists skilled in this type of regional anesthesia. Thus, although there is temporal overlap between groups, the non-SMB group is largely earlier and the SMB group later in her practice.
Exclusion Criteria
Patients exhibiting non-standard cleft deformities (such as cleft palate in the context of a Tessier cleft) or those who underwent additional painful procedures (such as gastrostomy or circumcision) concurrently with their palate repair were excluded. To minimize confounding factors in analgesic utilization, patients with a history of neonatal abstinence syndrome or those who were administered post-operative narcotics through nurse-controlled analgesia (NCA) were excluded, as we previously found that NCA greatly increases narcotic administration in the cleft palate population. 7 Furthermore, patients who received regional anesthesia other than SMB (such as greater and lesser palatine nerve blocks and nasopalatine nerve block) were excluded from the analysis.
Surgical and Regional Block Techniques
In terms of palatoplasty technique, children with submucous cleft palate (SMCP) and Veau I cleft palate underwent either intravelar veloplasty (IVVP) or Furlow palatoplasty with or without relaxing incisions to mitigate tension. Children with Veau II, III, and IV cleft palate underwent two-flap palatoplasty with vomerine flaps and IVVP, with the extent of dissection varying based on size of the cleft.
The SMB was performed under ultrasound guidance in all cases. It is performed traditionally using the landmark technique by inserting a needle directly behind the orbital rim but above the zygoma. It is then advanced until the sphenoid bone is contacted. The needle is then re-oriented about 20 degrees anteriorly and 10 degrees caudally with the tip aimed towards the nose/philtrum. It is then advanced beyond the temporalis muscle and into the pterygopalatine fossa. Once negative aspiration is confirmed, local anesthetic is then delivered. The ultrasound-guided technique used here is essentially the same, with the exception that the needle is visualized out of plane as it guided to the pterygopalatine fossa. The probe is placed parallel and under the zygoma (Figure 1, Video 1). The ultrasound approach has the advantage of visual confirmation of spread and avoidance of vessel puncture.
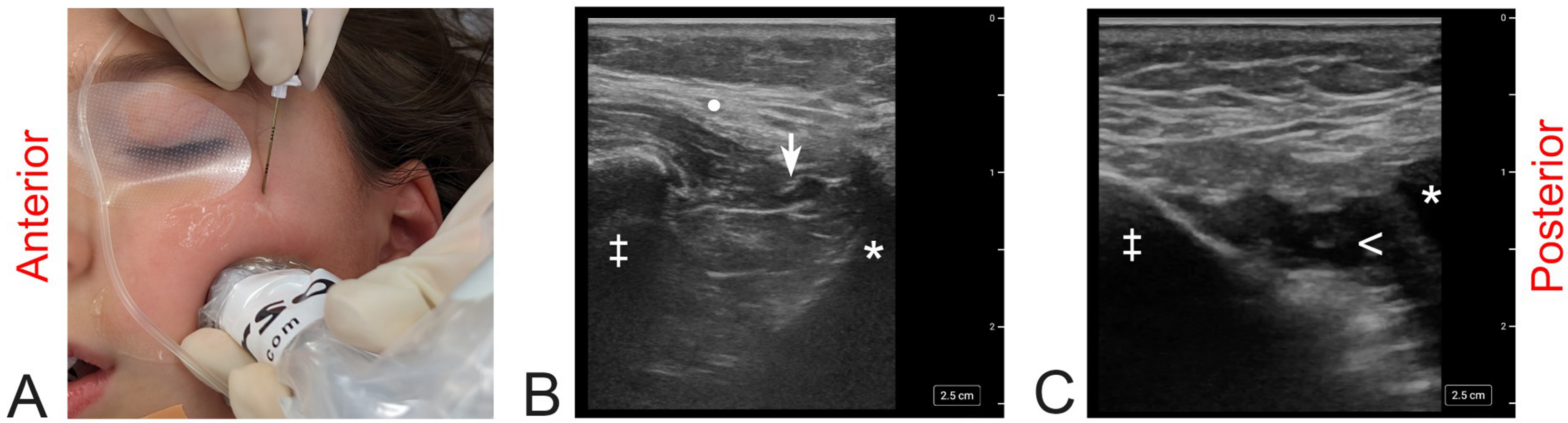
Technique for ultrasound-guided SMB.
Data Collection
Data was extracted from electronic medical records and Anesthesia Information Management Systems (AIMS), a comprehensive, prospectively-collected database of peri-anesthetic information. Collected variables comprised demographic details, Veau classification of cleft type, length of hospital stay, administration and timing of palate block, syndromic status, comorbidities, airway anomalies, and pre-existing respiratory support requirements.
Intraoperative measures included duration of anesthesia and normalized administered narcotics calculated in morphine equivalent units per kilogram per hour (MEU/kg/hr). To document the physiological response to painful stimuli, mean blood pressure and heart rate were recorded at incision and five minutes before and after. Minimal Alveolar Concentrations (MAC) of sevoflurane and isofluorane were recorded in a granular manner. The MAC isofluorane was converted to sevofluorane equivalent units. The area under the curve (AUC) of end-tidal sevoflurane concentrations was approximated using the trapezoidal rule. The analysis was performed for each third of the procedure's duration, as well as for the total duration. Furthermore, time-to-wake-up was determined by subtracting surgeon's end time from anesthesia end time.
In terms of postoperative care, patients are routinely extubated at the end of surgery and transported to the post-anesthesia care unit (PACU) either on supplemental oxygen or room air. In cases where any form of airway support was required beyond the operating room, patients were automatically taken to the intensive care unit (ICU), in accordance with hospital protocol. Airway support is defined here as nasopharyngeal airway (NPA), continuous positive airway pressure (CPAP), bilevel positive airway pressure (BiPAP), or mechanical ventilation via tracheotomy or intubation. We investigated the impact of SMB on postoperative respiratory outcomes by tracking episodes of hypoxemia, defined as instances where SaO2 levels fell below 92%, after the patient had left the PACU. We also evaluated the need for different levels of respiratory support, including supplemental oxygen administered beyond the PACU and airway support. Finally, ICU admission and the duration of stay were also recorded. Our analysis encompassed both the overall effect on any respiratory event, which includes both respiratory support needs and desaturation incidents, as well as an examination of each individual component of respiratory outcomes.
Normalized postoperative opioid (MEU/kg/hr) was calculated for the first 24 h following surgery. We chose this 24-h timeframe to minimize bias arising from the analysis of patients who were discharged early and received oral opioids, which we could not accurately quantify. We also recorded the amounts of non-narcotic analgesics, including acetaminophen, ibuprofen, and ketorolac. The highest pain scores using the Face, Legs, Activity, Cry, Consolability (FLACC) behavioral pain scale were recorded within the first 12 and 24 h after surgery, respectively.
Statistical Analysis
The hypotheses for this study were determined a priori, before accessing the data, in line with the STROBE guidelines. All statistical tests were performed using Rstudio (Rstudio version 2023.03.1 + 446: Integrated Development for R. RStudio, PBC, Boston, MA, URL http://www.rstudio.com/). Descriptive statistics were used to summarize baseline patient characteristics. The main objective of the statistical analysis was examination of SMB's effect on intraoperative and postoperative outcomes, while controlling for syndromic status and cleft type. Secondarily, we elucidate the influence of syndromic status on these outcomes, a factor acknowledged for its established significant role in perioperative scenarios.
Univariate analyses for continuous variables were performed using Mann-Whitney U tests, and Fisher's exact tests for categorical variables to identify differences between patients who received SMB and those who did not receive a regional nerve block. To control for expected potent confounders, such as syndromic status and cleft phenotype, multivariate analyses were performed using logistic regression models for categorical outcomes and log-transformed linear regression models for continuous outcomes. For logistic regression models, the results are reported as odds ratios, along with their associated 95% confidence intervals (CIs). For continuous outcomes that have been log-transformed in linear regression models, results are reported as relative change coefficients, which represent the multiplicative effect on the dependent variable for each one-unit increase in the independent variable. These relative change coefficients are obtained by exponentiating the estimated beta coefficients, and the associated 95% CIs are obtained by exponentiating the lower and upper bounds of the CIs for the beta coefficients. Finally, the effect of SMB and syndromic status on pain scores was analyzed using ordinal regression. A p-value threshold of 0.05 was used to determine statistical significance.
Results
Baseline Characteristics
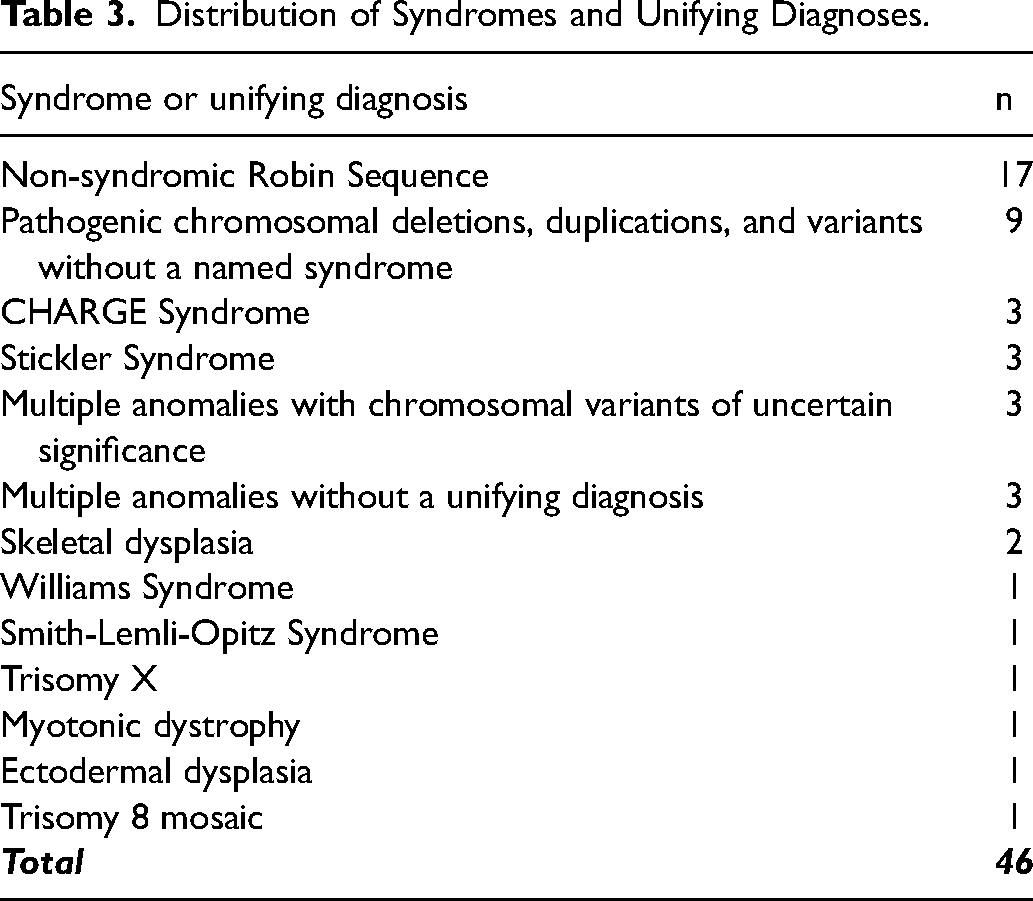
Of 132 patients who underwent primary palatoplasty within the selected timeframe, 30 were excluded based on the previously defined criteria. Out of the 102 patients who met the inclusion criteria, 57 (55.9%) underwent an ultrasound-guided SMB (Table 1). Among these 57 patients, SMB was administered at the beginning of the surgery for 49, while 8 received SMB at the end of the procedure due to lack of availability of an anesthesiologist skilled in regional anesthesia at the start of the case. Consequently, these 8 patients were not considered in the intraoperative outcome analyses but were considered in the postoperative outcome analysis. Sensitivity analysis revealed no difference in postoperative outcome with inclusion of these 8 children. All children, including those who received SMB, underwent surgical site infiltration of local anesthetic with epinephrine. Local anesthetic solutions used pre-incision included 0.25% bupivacaine with 1:200,000 epinephrine, 0.5% lidocaine with 1:200,000 epinephrine, or a mixture of 0.25% bupivacaine, 0.5% lidocaine, and 1:200,000 epinephrine. The specific quantity of local anesthetic varied, adhering to each patient's weight-based maximum dose limits, while also accounting for the amount administered as part of the SMB (detailed in Table 2). Where necessary, straight epinephrine 1:100,000 was used to augment vasoconstriction. It is noteworthy that, in one patient, the administration of local anesthetic was documented in the intraoperative anesthesia report; the specific anesthetic used and dose was not recorded in the Medication Administration Record resulting in missing data. Choice of local anesthetic combination in the regional block was at the discretion of the anesthesiologist; all blocks were ropivacaine-based (Figure 2). Median age was 10 months, with no difference observed between the SMB and non-SMB groups (p = 0.78). Syndromic cleft palate was present in 45.1% (n = 46) of the sample (Table 3), with the most common conditions being Robin sequence (n = 17, 37.0%), chromosomal anomalies without a named syndrome (n = 9, 19.6%), Stickler syndrome (n = 3, 6.5%), and CHARGE syndrome (n = 3, 6.5%). Active airway issues (laryngomalacia, tracheomalacia, persistent obstructive sleep apnea) were present in 28 patients at the time of palate repair (27.5%). Nine (8.8%) of these children required baseline respiratory support such as supplemental oxygen, CPAP, BiPAP, or tracheostomy.
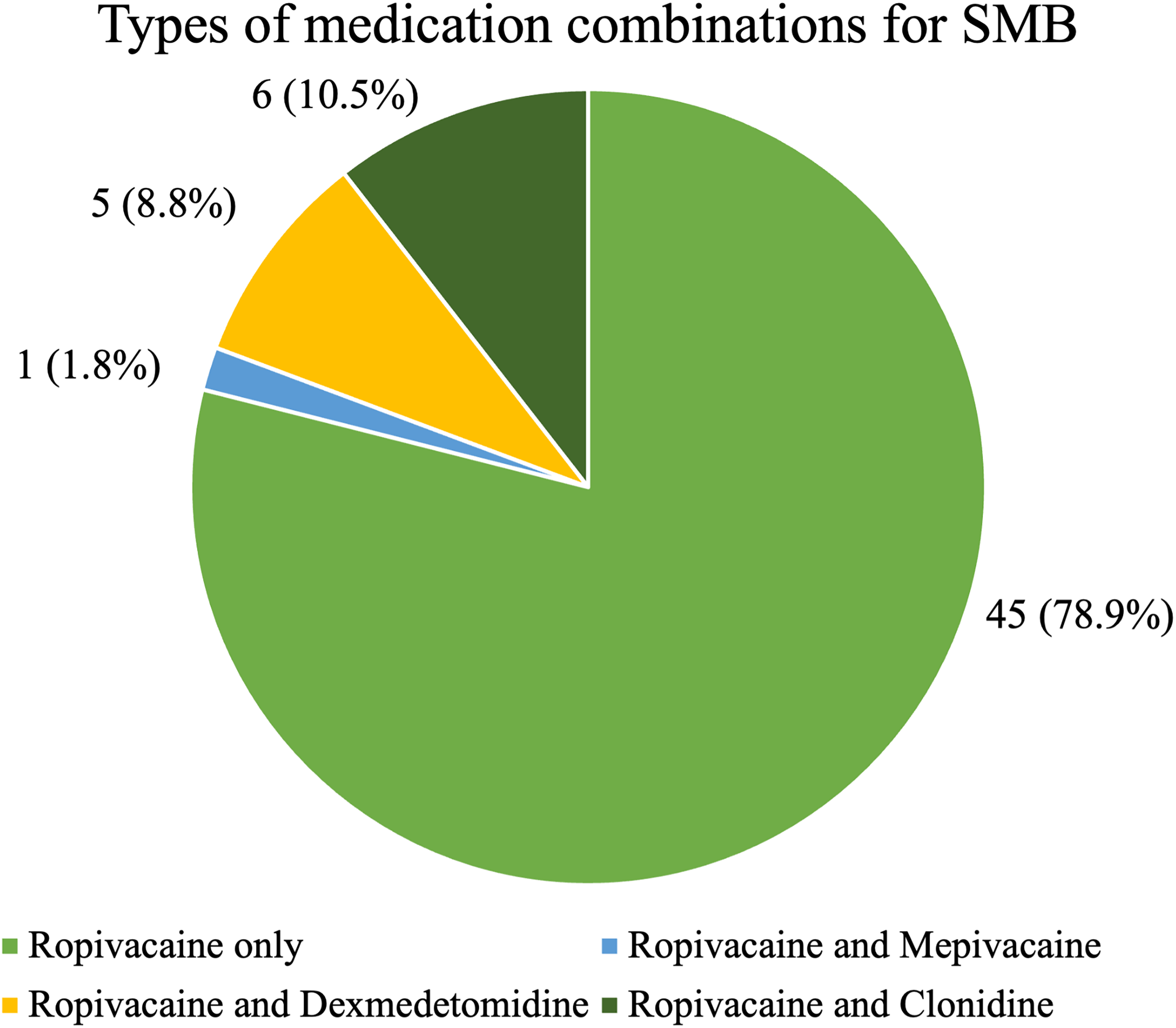
Distribution of local anesthetics. Suprazygomatic maxillary nerve block: proportions of patients administered each local anesthetic.
Baseline Demographic and Clinical Characteristics of the Study Cohort.
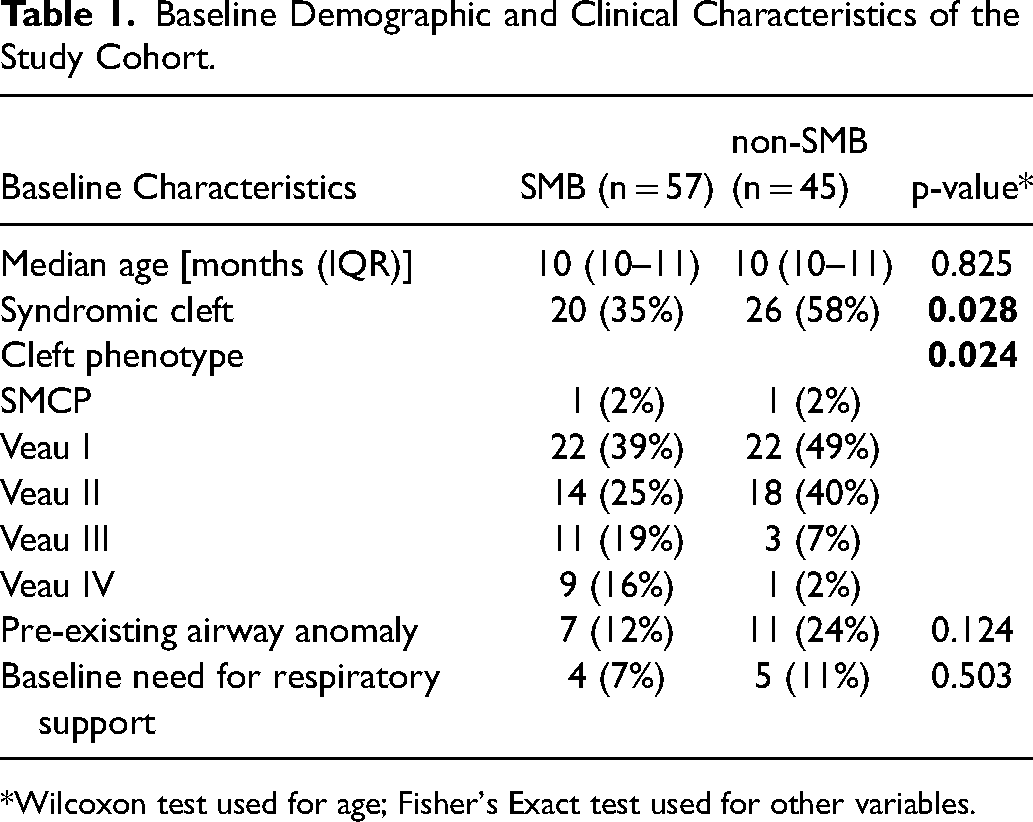
*Wilcoxon test used for age; Fisher's Exact test used for other variables.
Summary of Local Anesthetic Dosages: The Table Summarizes the Median Doses (in mg/kg) of Local Anesthetics Administered at the Surgical Site and at the SMB Site. Doses are Reported As Medians With Interquartile Ranges (IQR) in Parentheses. P-values from the Comparison of Median Doses between SMB and Non-SMB Groups, Obtained Using the Wilcoxon Test, are also Reported.
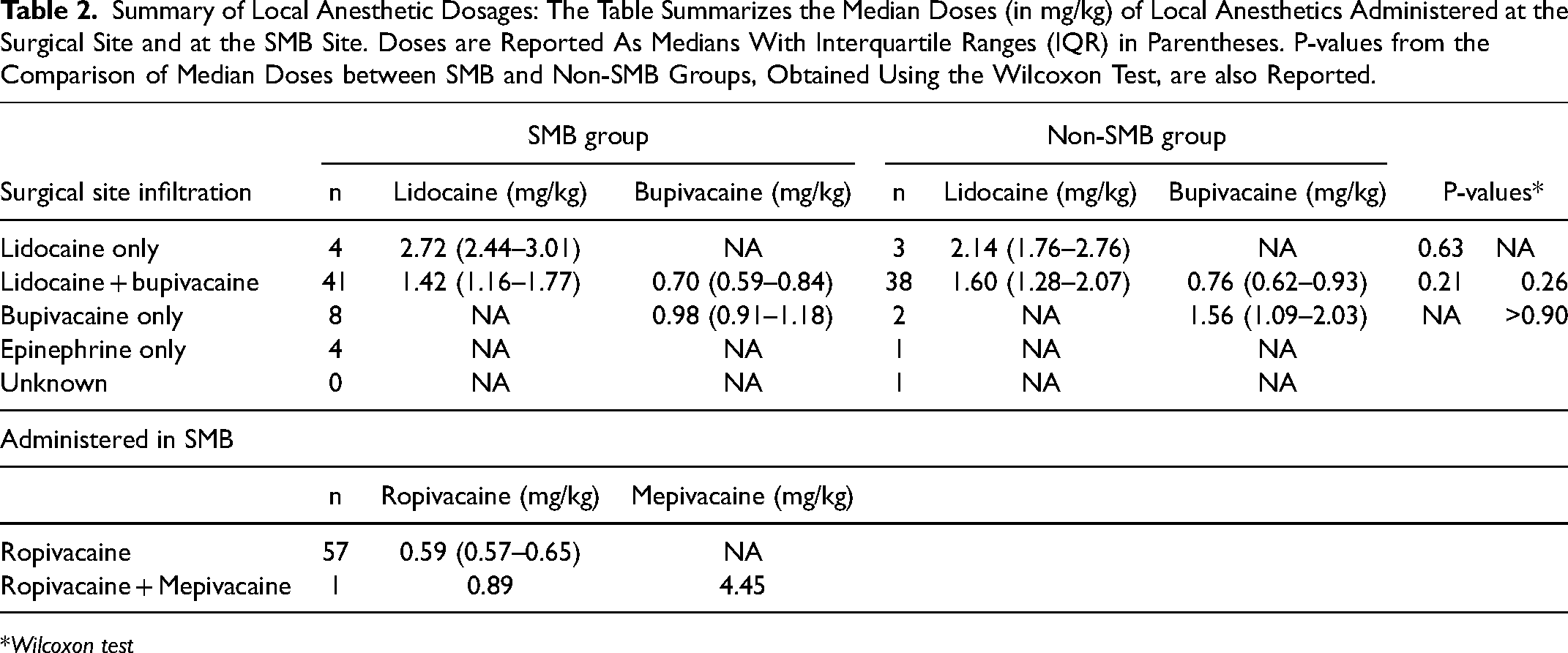
*Wilcoxon test
Distribution of Syndromes and Unifying Diagnoses.
Intraoperative Outcomes
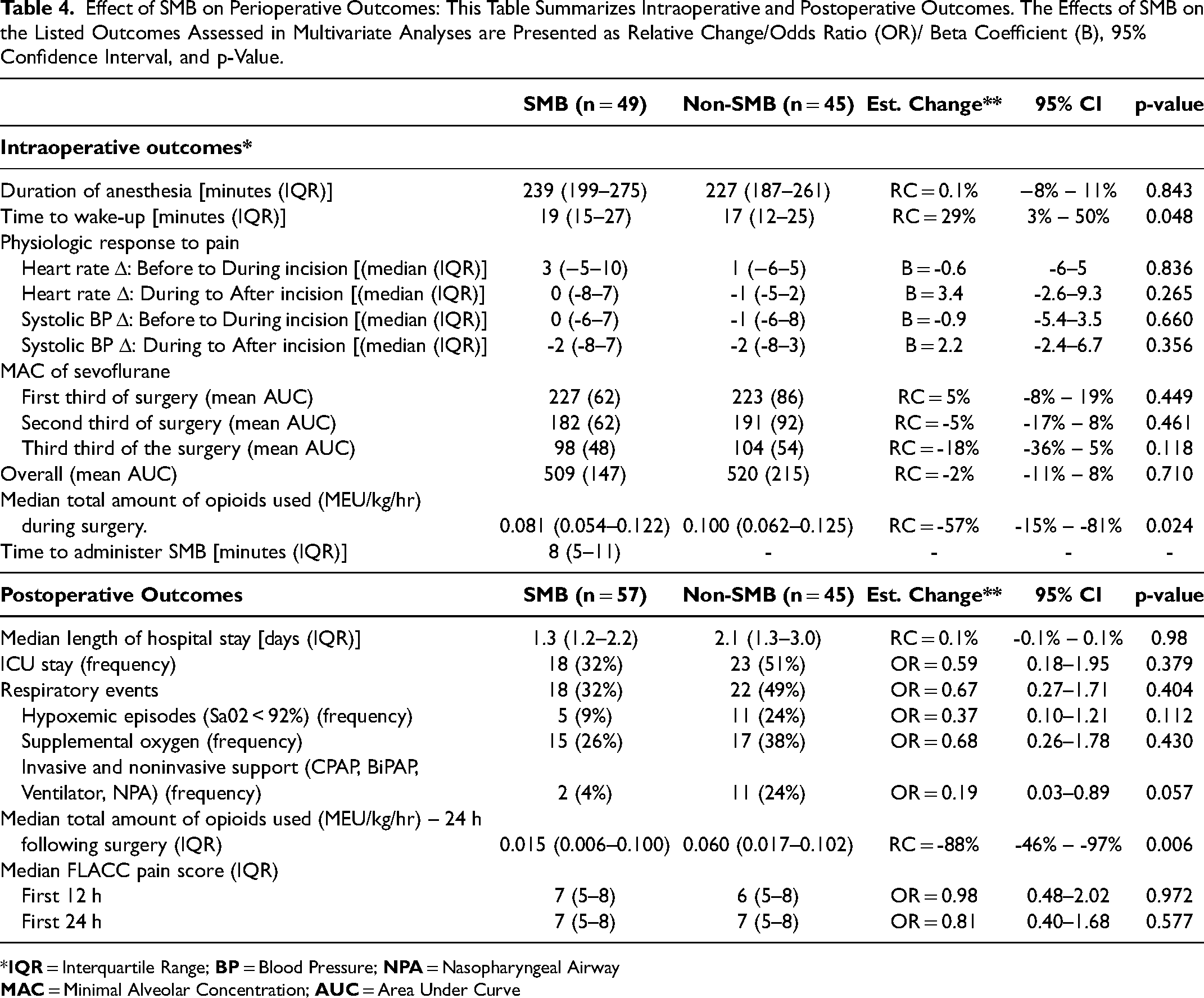
Forty-four different attending anesthesiologists participated in the procedures and all cases were primarily inhalational anesthetics with sevofluorane or isofluorane. The minimal alveolar concentration (MAC) of isofluorane was converted to sevofluorane-equivalent MAC. The median duration of anesthesia was 232 min (IQR = 199- 269), and did not differ between the SMB and non-SMB groups when adjusting for cleft phenotype (and thus the extent of the operation) (Table 4). Median time to complete bilateral SMB was 8 min (IQR = 5–11). Median intraoperative consumption of opioids was 0.08 MEU/kg/hr (IQR = 0.054–0.124). Notably, SMB was significantly associated with a 57% reduction in total intraoperative opioid requirements (95% CI = 15%—81%, p = 0.024), while controlling for syndromic status and cleft phenotype. However, there was no difference in physiological response (including heart rate and blood pressure) to surgical incision between SMB and non-SMB groups. We found no difference between groups in the MAC of sevoflurane used, and it was also unaffected by SMB in any of the observed time frames, when adjusted for syndromic status, cleft phenotype, and duration of anesthesia. Median wake-up time post-surgery was 18 min (IQR = 13–27). Notably, SMB was significantly associated with a 29% (5 min) increase in median wake-up time post-surgery (95% CI = 3% – 50%, p = 0.048), when controlling for syndromic status and cleft phenotype.
Effect of SMB on Perioperative Outcomes: This Table Summarizes Intraoperative and Postoperative Outcomes. The Effects of SMB on the Listed Outcomes Assessed in Multivariate Analyses are Presented as Relative Change/Odds Ratio (OR)/ Beta Coefficient (B), 95% Confidence Interval, and p-Value.
*
Postoperative Outcomes
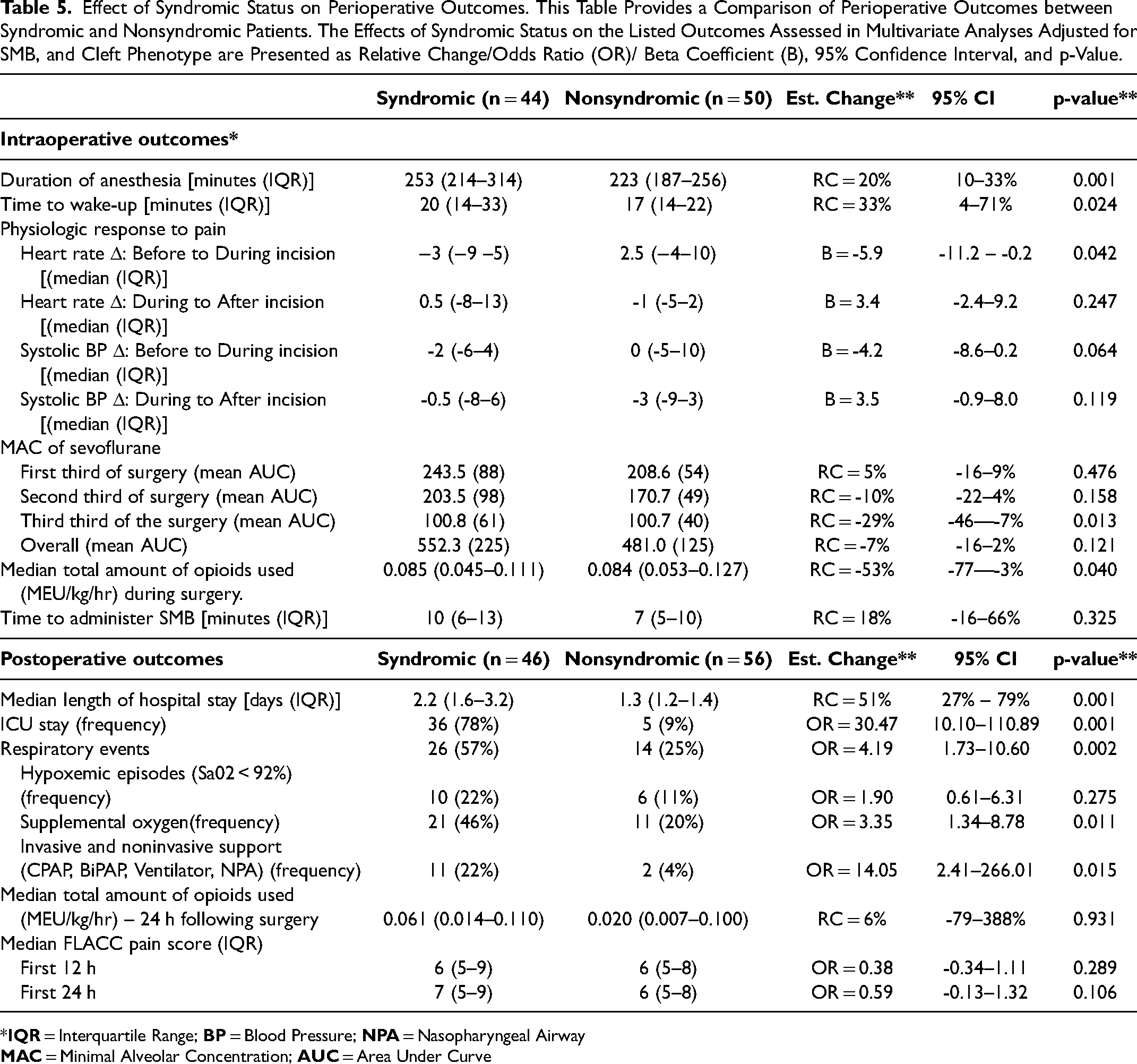
When accounting for syndromic status and cleft phenotype, many of the observed postoperative outcomes were not influenced by SMB administration (Table 4). This includes ICU admission, incidence of hypoxemic episodes, and need for either new supplemental oxygen or airway support. SMB also had an insignificant effect on pain as measured on the FLACC scale, both in the first 12 and first 24 h. However, we found that SMB was significantly associated with a 18% reduction in length of hospital stay (95% CI = 2–31%, p = 0.048), when adjusted for syndromic status and cleft phenotype. Furthermore, the median total amount of administered opioids in the first 24 h after surgery was 0.039 MEU/kg/hr, with the SMB group requiring significantly less than the non-SMB group. Specifically, SMB administration was associated with an 88% (95% CI = 46% – 97%, p = 0.006) reduction in total opioid consumption within 24 h after surgery, while controlling for syndromic status, cleft phenotype, and non-narcotic pain medications (ibuprofen, acetaminophen, ketorolac). Comparison of both intraoperative and postoperative outcomes between syndromic and non-syndromic patients is provided in Table 5 to illustrate the rationale for controlling for syndromic status when evaluating the impact of SMB.
Effect of Syndromic Status on Perioperative Outcomes. This Table Provides a Comparison of Perioperative Outcomes between Syndromic and Nonsyndromic Patients. The Effects of Syndromic Status on the Listed Outcomes Assessed in Multivariate Analyses Adjusted for SMB, and Cleft Phenotype are Presented as Relative Change/Odds Ratio (OR)/ Beta Coefficient (B), 95% Confidence Interval, and p-Value.
*
Discussion
Several prospective studies have demonstrated that compared to no analgesia or to other regional blocks, SMB significantly reduces opioid consumption during cleft palate repair and hastens recovery and resumption of feeding after surgery.6,9,18 However, studies comparing SMB to infiltration of local anesthetic at the surgical site, a common practice in palatoplasty, have been more limited and less convincing. For this reason, SMB is not universally employed by all cleft surgeons. Moreover, a substantial proportion of children requiring primary palatoplasty have cleft palate as part of a broader, unifying diagnosis. Patients with CHARGE syndrome, chromosomal anomalies, or Stickler syndrome often have a complex medical history precluding their participation in clinical trials. Yet, they still stand to benefit from better perioperative analgesia. Moreover, they are more likely to have pre-existing airway anomalies that could benefit from a narcotic-sparing approach. Consequently, understanding SMB's effect for this population is important.
Our study confirmed the primary hypothesis that addition of SMB significantly reduces administration of opioid medications during and after surgery compared to surgical site infiltration of local anesthetic only. This is an important addition to our understanding of SMB efficacy in palatoplasty because the current literature making this comparison has been limited by lower power and has yielded conflicting results.7,11 Our department previously evaluated palatoplasty pain management practices as a whole, including a small subanalysis of non-syndromic children receiving SMB. 7 This study demonstrated a reduction in post-operative opioid-utilization with SMB. Subsequent to this, Jacobs-El et al. 11 evaluated the impact of SMB on narcotic requirements after palatoplasty and found no effect, in addition to finding no effect on other parameters. Here, in a larger population of children operated on by a single surgeon (standardizing technique in a phenotype-specific manner), we demonstrate a significant reduction in not just postoperative, but intraoperative opioid requirement with SMB. Moreover, the opioid-sparing benefits persists when controlling for cleft type and syndromic status. This confirms our secondary hypothesis and suggests comparable efficacy of SMB in both syndromic and non-syndromic groups. Although we did not find a difference in post-operative FLACC scores, hospital length of stay was significantly less with SMB when accounting for phenotype and syndromic status. This suggests a general improvement in post-operative analgesia and return to baseline functional status in a way that cannot be accounted for by measures like FLACC.
Chiono's et al. 9 proposition that SMB could potentially reduce postoperative respiratory complications compared to placebo inspired us to investigate the respiratory implications of SMB compared to surgical site infiltration of local anesthetic. This stemmed from the notion that if SMB curtails the amount of administered narcotics—known contributors to respiratory depression 19 — it could lead to enhanced respiratory mechanics during and after surgery. We felt this was particularly important to consider for the syndromic cleft population because they are often at higher risk of negative respiratory outcomes related to their underlying diagnoses and potential pre-existing airway anomalies. However, our tertiary hypothesis that SMB improves respiratory outcomes after palatoplasty was not supported. Consistent with several other recent studies,10,20 our findings showed no SMB advantage in diminishing respiratory complications, nor in other measures such as requirement for airway support. However, it is important to note that these episodes occurred infrequently in the population as a whole. Thus, the present study may be underpowered to detect an effect. Moreover, the syndromic cleft population is highly heterogeneous. Binary categorization of syndromic v. non-syndromic is an oversimplification and a different distribution of syndromes with more baseline predisposition to airway issues may yield different results.
The finding of reduced narcotic requirements both during and after surgery is clinically meaningful. Opiate use in infants and children can be associated with pruritus, emesis, and ileus. 21 Those latter side effects are particularly important to avoid after palate repair. Emesis is undesirable after intraoral surgery. Ileus may hinder oral intake in the days after surgery, impacting hydration and nutritional status after an operation that already makes oral intake challenging. Therefore, exploration of opiate alternatives is a priority. Moreover, literature demonstrates that infants can exhibit unpredictable susceptibility to opiates,22–24 especially morphine, leading to an increased occurrence of respiratory complications. This risk is further potentiated by inherent threat to the airway posed by cleft palate repair itself. 25 Given this background, despite finding no effect on respiratory outcomes, the theoretic respiratory benefits remain of interest. We advocate for larger studies to evaluate for more subtle differences in these infrequent, but serious adverse events.
Anecdotally, cleft surgeons may refrain from incorporating SMB in their practice due to concerns about prolonging time under anesthesia. To this point, although duration of surgery and anesthesia significantly increased with syndromic status and Veau phenotype severity as would be expected, it was not significantly impacted by placement of SMB. The time needed to perform bilateral SMB was approximately 8 min. Thus, the additional time needed for this effective intervention is negligible and should not discourage its use. An unanticipated finding was that SMB significantly increased wake-up time after completion of surgery by approximately 5 min. Related to this, in our population, the minimal alveolar concentration (MAC) of sevoflurane did not differ between groups. Thus, the prolonged wake-up time in the setting of children being maintained at equivalent MAC speaks to the potent analgesic effects of SMB. This level of analgesia may lead to deeper sedation despite less narcotic utilization. Prolonged wake up time could be mitigated by tailoring MAC to account for use of SMB and may improve with increasing familiarity of the primary anesthesiolgist with the effect of regional anesthesia. Additionally, better communication between surgeon and anesthesiologist about anticipated procedure end time may better inform when to reduce the amount of volatile anesthetics being administered.
A key strength of our study is its single-surgeon design, which promotes a consistent surgical approach within a given cleft phenotype, enhancing homogeneity of our data. The fact that there were 44 different anesthesia attendings involved in the procedures is both a weakness and a strength. Although it precludes our ability to control for anesthesiologist, the large variability in anesthesiologists helps mitigate individual biases in administration of narcotics and volatile anesthetics. However, limitations of our study include its retrospective, non-randomized design, the constraints of our sample size (particularly the relatively small sample of those who had adverse respiratory outcomes), and the fact that frequency with which SMB was used was dictated by time period. Although our cohort is comparatively larger than those in most other studies on this topic, the sample size still poses limitations due to the demanding statistical requirements of our analysis. Moreover, a substantial number of cases were excluded due to combined operations. Patients needing additional painful procedures, such as gastrostomy, may be more likely to have underlying diagnoses. Thus, excluding these patients may have blunted our ability to detect an effect on respiratory complications that the syndromic population is more prone to having. Additionally, stratification of non-syndromic and syndromic as a binary variable is a rudimentary way of categorizing a heterogenous population. Larger numbers of each unifying diagnosis are needed to better understand the benefit of SMB in the context of each condition. Finally, the frequency with which SMB was used was highly correlated with later years in the study (R = 0.76, p < 0.001). This makes it difficult to determine whether the decreased length of stay seen in the SMB group was attributable to SMB alone or due to changing discharge practices over time. To these ends, prospective randomized trials are needed to definitively ascertain the efficacy of SMB compared to surgical site infiltration of local anesthetic alone in diverse clinical contexts.
Conclusions
SMB reduces intra-operative and post-operative narcotic requirements after palatoplasty in both non-syndromic and syndromic children. Respiratory outcomes are no different with SMB, when accounting for syndromic status and cleft phenotype.
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.