
Abstract
Objective
Identify and describe factors associated with retention and attrition of patients during longitudinal follow-up at multidisciplinary cleft clinic.
Design
Retrospective cohort study.
Setting
Single, tertiary care center.
Patients, Participants
Patients born between 1995 and 2007 with a diagnosis of cleft palate with or without cleft lip attending multidisciplinary cleft clinic.
Interventions
None tested, observational study.
Main Outcome Measure(s)
Age at last clinical appointment with a multidisciplinary cleft team provider. Attrition was defined as absence of an outpatient appointment following 15 years of age.
Results
Six hundred seventy-eight patients were included. The average age at last appointment across the entire cohort was 13.1 years (IQR 6.6–17.2). Patients who were Black (HR 1.60, 95% CI 1.10–2.32, p = 0.014) and other races (HR 1.90, 95% CI 1.22–2.98, p = 0.004) were more likely to be lost to follow-up compared to white patients. Publicly insured patients were more likely to experience attrition than those who were privately insured (HR 1.30, 95% CI 1.03–1.65, p = 0.030). Estimated income was not significantly associated with length of follow-up (p = 0.259). Those whose residence was in the fourth quartile of driving distance from our center experienced loss to follow-up significantly more than those who lived the closest (HR 2.04, 95% CI 1.50–2.78, p < 0.001).
Conclusions
There is a high degree of follow-up attrition among patients with cleft lip and palate. Race, insurance status, and driving distance to our center were associated with attrition in a large, retrospective cohort of patients who have reached the age of cleft clinic graduation.
Introduction
Congenital orofacial clefts are associated with a burden of care which extends beyond primary lip and palate repair to include alveolar bone grafting, speech surgery, rhinoplasty, orthognathic surgery, and possibly revisional surgeries.1–4 While operative technique and secondary surgery practices vary widely between institutions, it is not uncommon for patients to undergo as many as ten procedures through their teen years, with variation based upon cleft severity and surgical outcomes.5,6 Due to ongoing surgical treatment needs and specialist care including speech therapy and psychosocial support, patients are commonly followed in multidisciplinary clinic at regular intervals throughout development. 7 Multidisciplinary cleft clinics consolidate multiple appointments into a single visit, and in this way attempt to lessen the burden of care which families experience.
While the goal of longitudinal follow-up is to provide sustained therapeutic treatment (speech, dental, orthodontic, etc) as well as surgical interventions both at standard intervals and based on specific needs, this is not achieved for all patients. Multiple studies have demonstrated delays to alveolar bone grafting for patients with public insurance and patients of racial minority groups.8–10 Additionally, there is evidence that patients who are Black undergo cleft rhinoplasty less frequently than peers. 11 Conversely, a separate study found that patients in the highest income quartile have increased odds of secondary cleft rhinoplasty. 12
It could be hypothesized that the lower rates of secondary cleft surgeries in patients of underserved groups is a by-product of loss to follow-up as patients age. Attrition from cleft clinic has been the subject of prior investigation, with attrition rates of 60% seen by age 16, and higher odds of attrition for black patients. 13 However, this study noted that almost 10% of patients characterized as lost to follow-up at the end of the study period returned to care within 18 months. This raises further questions about the true rate of attrition in this patient population. To that end, the present study was undertaken to comprehensively characterize retention and attrition from cleft clinic in a retrospective cohort of patients with cleft lip and palate who have reached facial skeletal maturity. We hypothesized that attrition varies based on sociodemographic factors, and that those of underserved racial/ethnic backgrounds, those with public insurance, and those with lower incomes will have higher rates of attrition over time.
Methods
This study was approved by the Institutional Review Board. Patients born between 1995 and 2007 with cleft palate with or without cleft lip who underwent palatoplasty were reviewed. Patients were excluded if they underwent surgery at an outside institution, if they had a syndromic diagnosis, or if they lived internationally.
Demographic information was collected for each patient. Cleft diagnosis was recorded as cleft palate only (CP), cleft lip and palate (CLP), or submucous cleft palate (SMCP). Insurance provider at the time of palatoplasty was recorded as either private or public. Each patient's last known address was used to calculate driving time to our institution in minutes using an application programming interface from Google Maps in Microsoft Excel Version 2022 (Redmond, Washington). Publicly available data from the United States Census Bureau was used to assign estimated income to each patient based on zip code median income in 2021 using their last known address.
Medical records were reviewed for clinical encounters with the patient's cleft surgeon and other members of the multidisciplinary cleft team. Virtual visits were included. The age at most recent clinical visit was recorded. Patients whose last visit date occurred prior to 15 years of age were categorized in the attrition group, whereas patients whose last visit occurred after that age were categorized in the retention group. The age cutoff was chosen based on surgeon experience rather than a ‘graduation’ cutoff because no standardized criteria is used at our institution.
Statistical analysis was conducted in JASP (Version 0.16.3; JASP Team, 2020) and R 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/). Demographics were assessed with descriptive statistics. Categorical variables were assessed using chi-square tests. Continuous measures were assessed with median and interquartile ranges (IQR) and compared using the Mann-Whitney U test and Kruskal-Wallis test with Dunn post-hoc testing. The Benjamini-Hochberg method was used to correct for multiple post-hoc comparisons. Survival analysis was conducted using multivariable Cox proportional hazard modeling to assess for significant predictors of attrition by 15 years of age. Results were reported as hazard ratios (HR) and 95% confidence intervals (CI). To assess for trends in length of follow-up across the study period, patients were divided into two six-year groups based on date of birth (1995–2001, 2002–2007). For the purposes of statistical analysis, racial/ethnic groups included White, Black, Asian, Hispanic, and other. To our knowledge, the system for patient self-reporting race/ethnicity has not changed during the study period. Insurance was either private or public (Medicaid). Diagnoses included CP, CLP, and SMCP. Estimated income and travel distance were grouped by quartiles for analysis. Variance Inflation factors (VIF) were used to assess for multicollinearity among the variables tested with a threshold of VIF < 5 defined as acceptable. The model was stratified by diagnosis. Schoenfeld's test was used to test that the model met the assumption of proportional hazards. In the case where the assumption was not met, time-dependent coefficients were used as described in Therneau et al. 14
Results
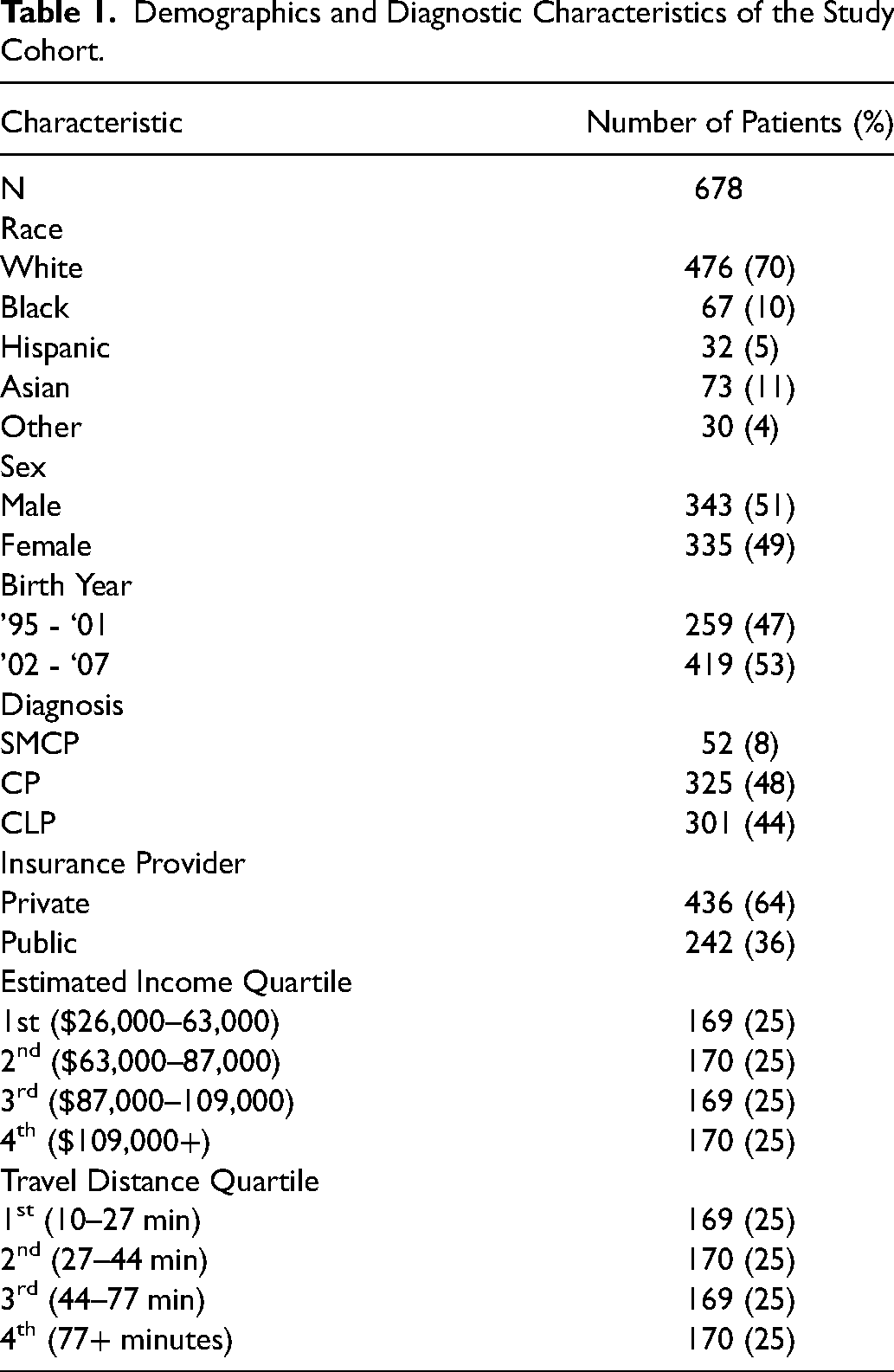
Six hundred seventy-eight patients were included. The cohort was majority white (70%), male (51%), and privately insured (64%). Three hundred twenty-five patients (48%) had CP, 192 (44%) had CLP, and 52 (8%) had SMCP. The lowest estimated income quartile ranged from $26,000-$63,000 and the highest income quartile included estimated incomes greater than $109,000. The first quartile of driving distance to our institution was 10–27 min and the fourth quartile included those traveling greater than 77 min (Table 1).
Demographics and Diagnostic Characteristics of the Study Cohort.
The average age at last appointment across the entire cohort was 13.1 years (IQR 6.6–17.2). Age at last appointment varied by diagnosis as patients with CLP were older at their last visit (16.2 years, IQR 11.4–18.5) than patients with CP (8.5 years, IQR 3.4–15.3) or patients with SMCP (9.9 years, IQR 6.6–14.8, p < 0.001, Table 2). The average age at last appointment for males was 14.5 years (IQR 7.4–17.7), which was greater than the age at last follow-up for females (10.8 years, IQR 5.1–16.7, p = 0.002). Males made up a larger proportion of patients with CLP (n = 189, 63%) than females (n = 112, 37%), and females were more likely to have CP (n = 191, 59%) than males (n = 134, 41%, p < 0.001). Patients born between 1995 and 2001 were followed for an average of 11.7 years (IQR 7.0–18.2) compared to those born between 2002 and 2007 who were followed for an average of 13.8 years (IQR 5.9–16.6, p = 0.049).
Age at Last Appointment Based on Each Diagnostic and Demographic variable. P-Values Calculated via Mann-Whitney U Test and Kruskal-Wallis Test.
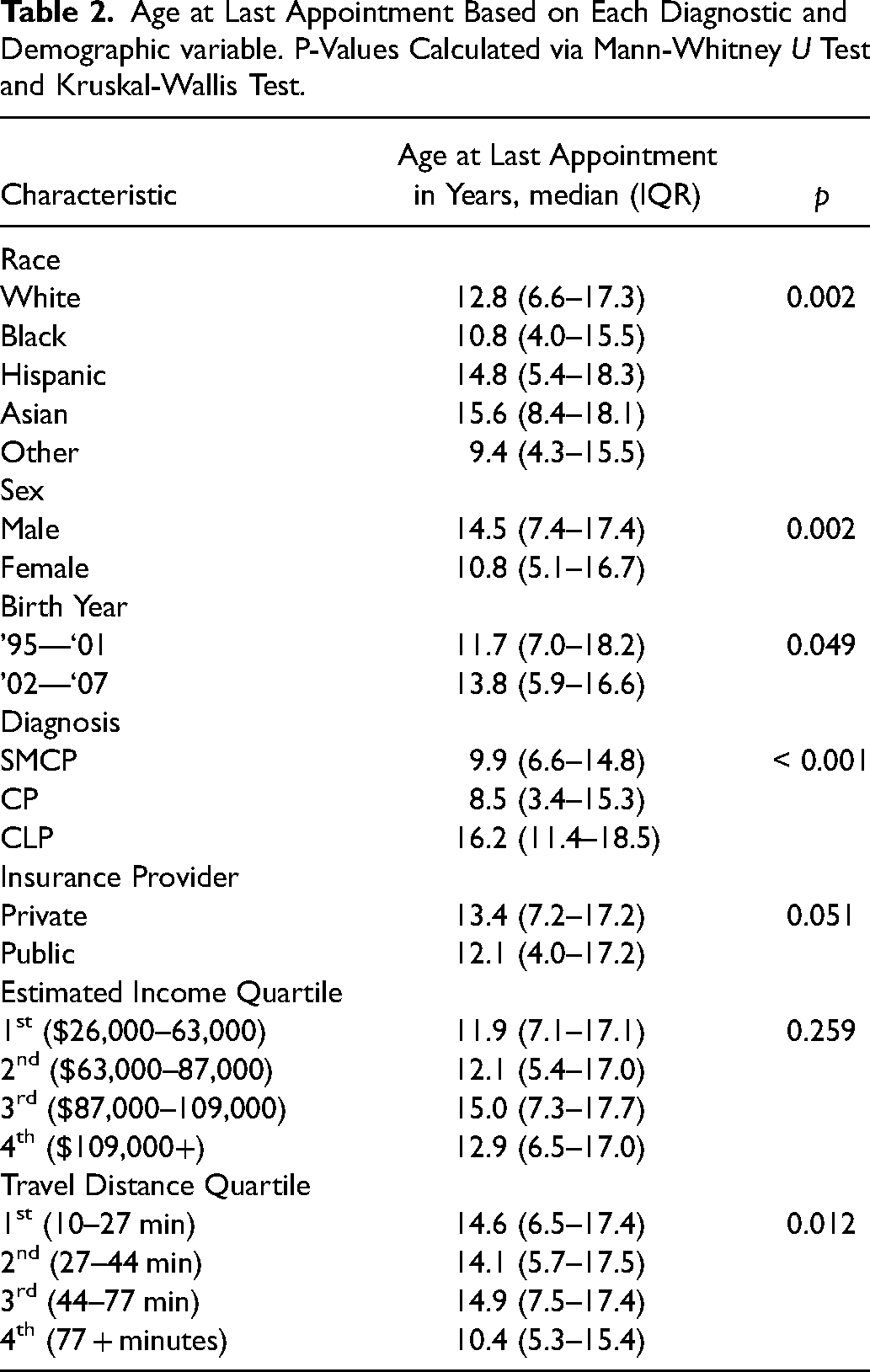
Asian patients had the longest median follow-up (15.6 years, IQR 8.4–18.1) whereas Black patients (10.8 years, IQR 4.0–15.5) and patients of other racial and ethnic groups (9.4 years, IQR 4.3–15.5) had the shortest follow-up (p = 0.002, Figure 1). Post-hoc testing showed that Asian patients had significantly longer follow-up than both Black patients (p = 0.006) and other patients (p = 0.008, Supplemental Table 1). There was no significant difference in age of last appointment between patients with private insurance (13.4 years, IQR 7.2–17.2) and public insurance (12.1 years, IQR 4.0–17.2, p = 0.051).
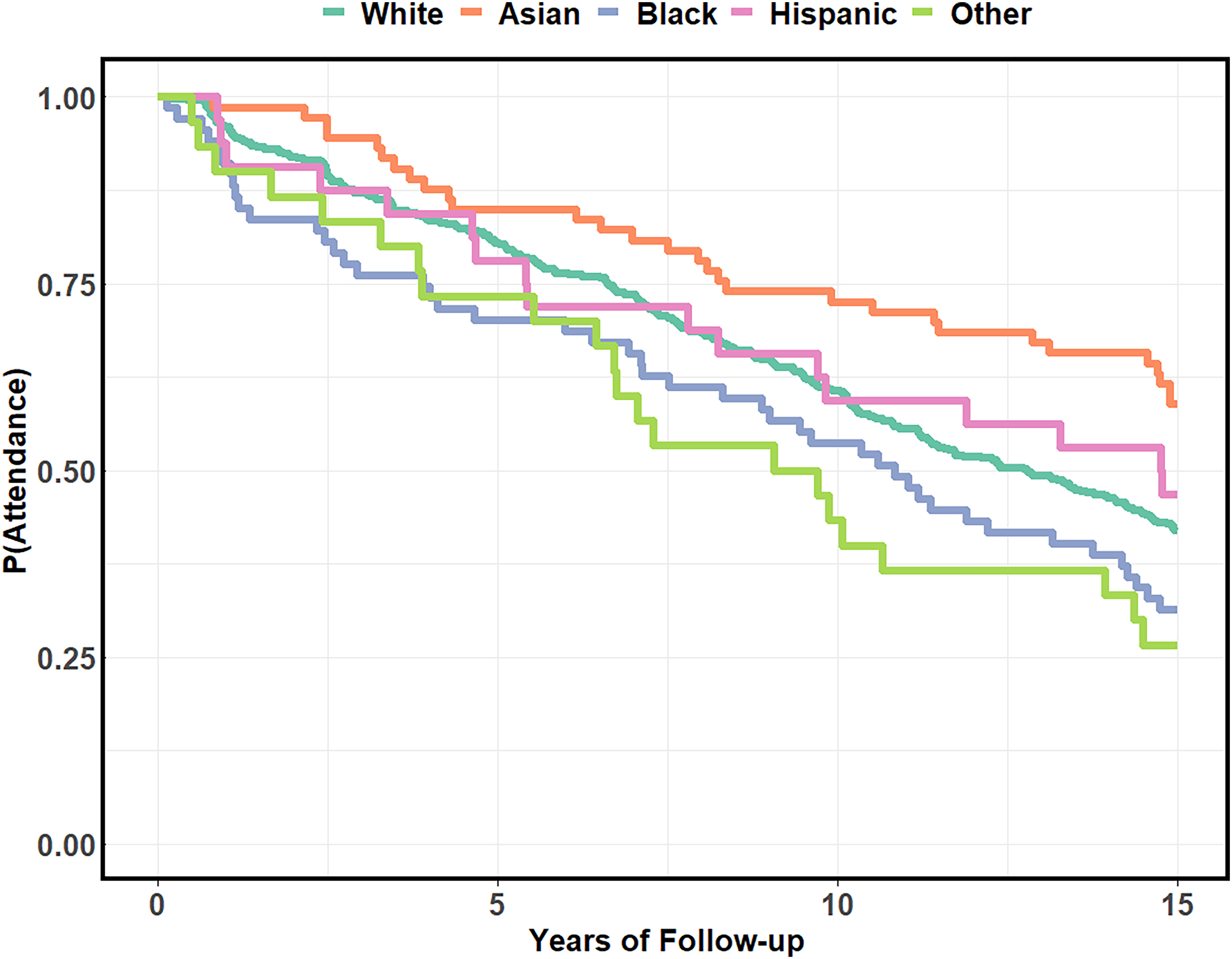
Kaplan-Meier curve of cleft clinic attendance attrition across the first 15 years of life separated by race.
Patients in the third income quartile were oldest on average at their last appointment (15.0 years, IQR 7.3–17.7), but this was not significantly different from patients in other estimated income quartiles (p = 0.259). Age at last follow-up was significantly associated with travel time from our institution, with patient whose address mapped in the fourth quartile having the shortest average follow-up (10.4 years, IQR 5.3–15.4, p = 0.012, Figure 2). On post-hoc testing, patients in the first (p = 0.029) and third (p = 0.008) quartiles for travel time were followed longer than those in the fourth quartile. There was no difference between length of follow-up for patients in the first, second, or third quartiles (p > 0.05 for all, Supplemental Table 1).
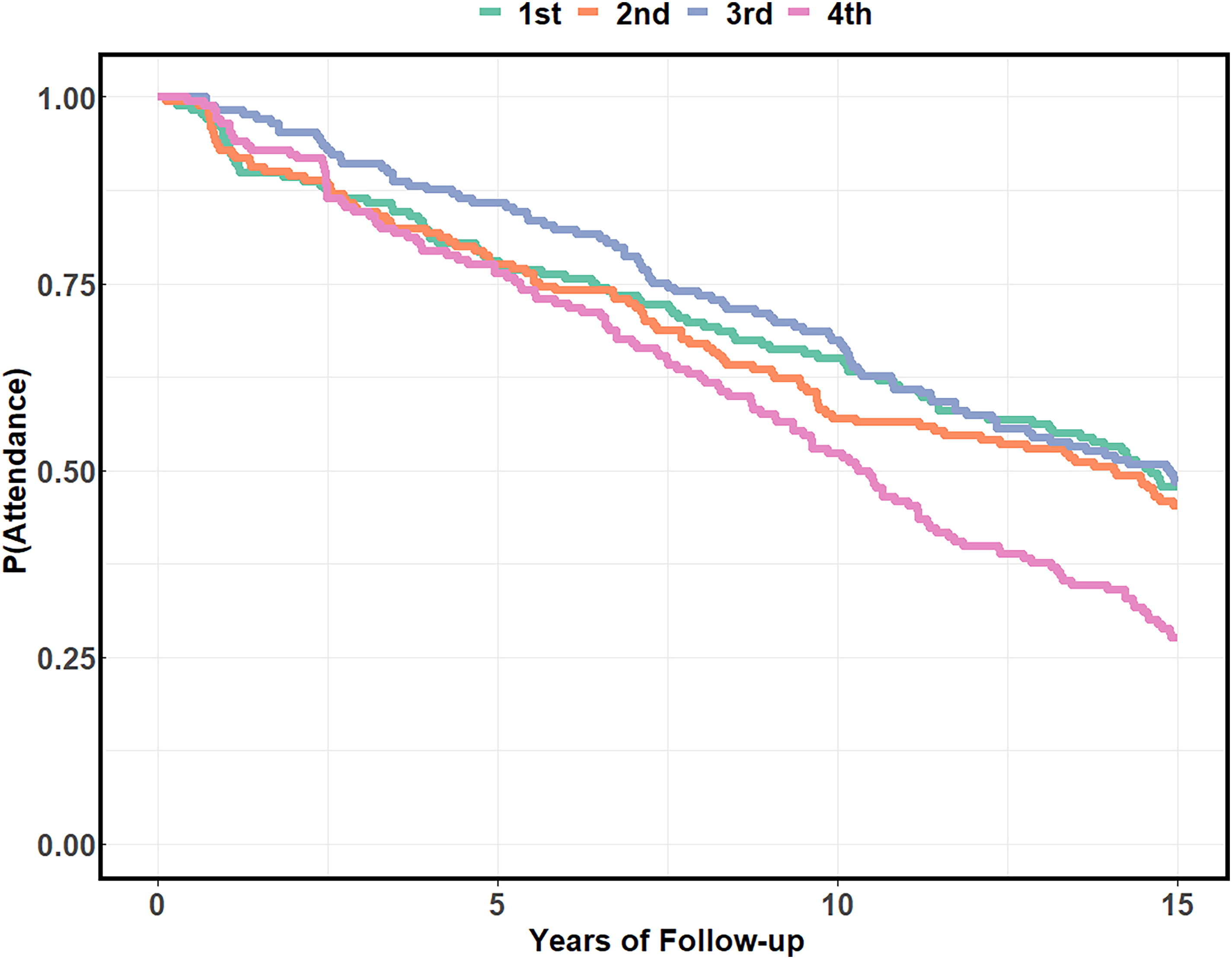
Kaplan-Meier curve of cleft clinic attendance attrition across the first 15 years of life separated by travel distance quartile.
Fifty-eight percent (391/678) of patients did not have a visit after the age of 15. The rate of attrition by 15 years of age was lowest among patients with CLP (38%), followed by patients with CP (73%) and patients with SMCP (75%, p < 0.001). Attrition prior to 15 years did not differ between patients born from 1995 to 2001 compared to those born from 2002 to 2007 (p = 0.794). Attrition was lowest among Asian patients (41%) and highest among black patients (69%) and patients of other racial and ethnic groups (73%, p = 0.005, Table 3). The rate of attrition among privately and publicly insured patients did not differ significantly (57% versus 59%, p = 0.692). The rate of attrition for the first through fourth income quartiles were 61%, 58%, 50%, and 62% (p = 0.097). Those who lived the farthest from our institution had a higher rate of attrition (72%, p < 0.001).
Attrition Rates at 15 Years of age for Each Diagnostic and Demographic Group. P-Values Calculated with the chi-Square Test.

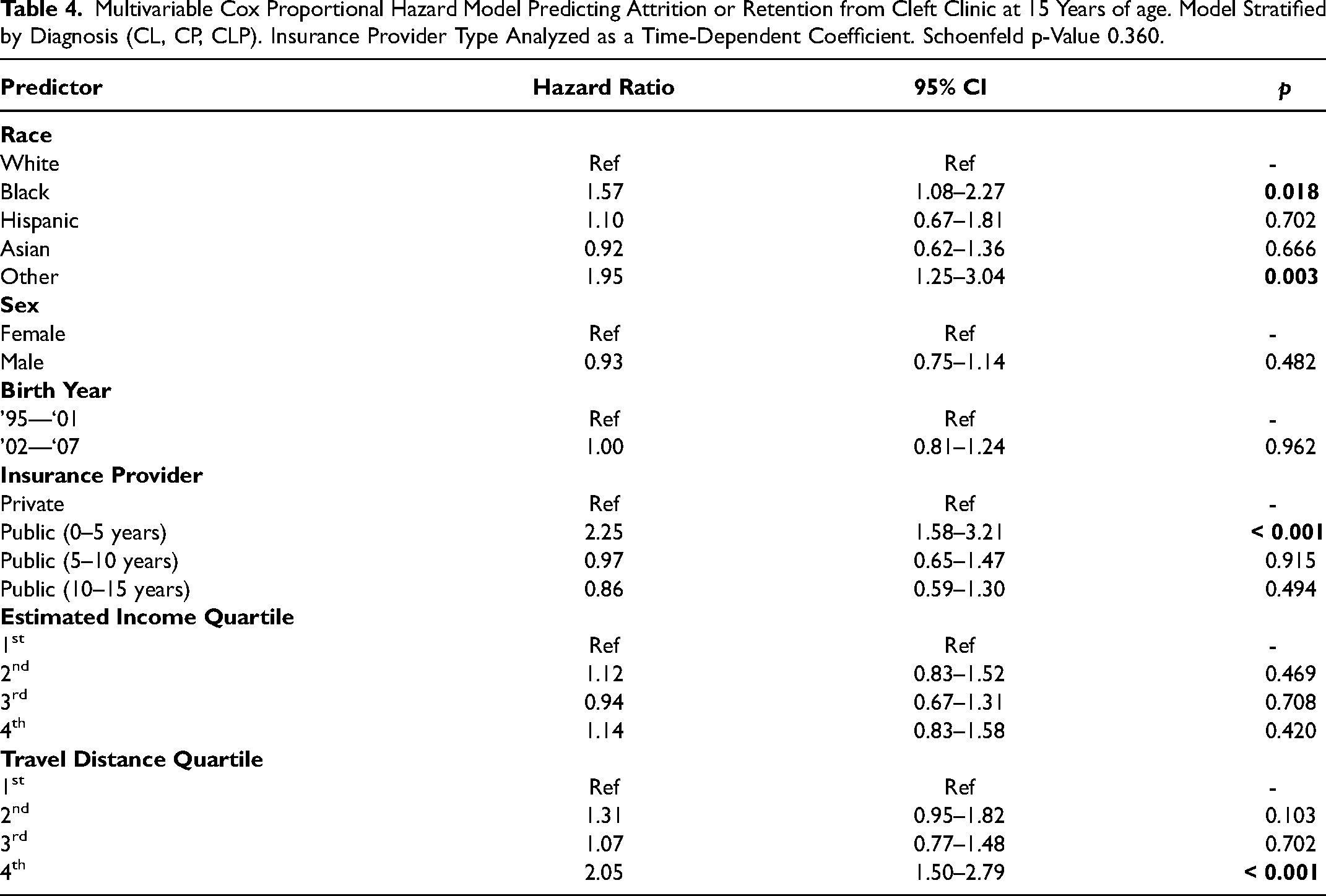
Multivariable Cox proportional hazard modeling stratified by diagnosis was carried out and tested for the proportional hazards assumption with Schoenfeld's test. In the initial null model incorporating each demographic factor, all variables met the proportional hazard assumption (p > 0.05) except for insurance provider (p < 0.001), and the global model did not meet the assumption (p = 0.006). Insurance provider was converted to a time-dependent coefficient with independent coefficients for 0–5 years, 5–10 years, and 10–15 years. This resulted in model which met the global assumption of proportional hazards (Schoenfeld p-value 0.360). In this model, Black race (HR 1.57, 95% CI 1.08–2.27, p = 0.018) and other race/ethnicity (HR 1.95, 95% CI 1.25–3.04, p = 0.003) were significant predictors of loss to follow-up compared to white patients (Table 4). Patients with public insurance were more likely to experience loss to follow-up than patients with private insurance specifically in the 0–5-year time interval (HR 2.25, 95% CI 1.58–3.21, p < 0.001) and not in the 5–10- or 10–15-year intervals (p > 0.05). Attrition was more likely in patients living in the fourth quartile of driving distance from our institution compared to the first (HR 2.05, 95% CI 1.50–2.79, p < 0.001). Variance inflation factors were < 5 for all variables tested.
Multivariable Cox Proportional Hazard Model Predicting Attrition or Retention from Cleft Clinic at 15 Years of age. Model Stratified by Diagnosis (CL, CP, CLP). Insurance Provider Type Analyzed as a Time-Dependent Coefficient. Schoenfeld p-Value 0.360.
Discussion
In the longitudinal care for patients with cleft lip and palate, multidisciplinary team care through skeletal and psychological maturity is advised to detect late presenting sequalae and deliver indicated interventions. This study was conducted to assess the degree to which sustained follow-up is achieved, and to investigate the rate of attrition from clinic among different sociodemographic groups. The results demonstrate high rates of attrition overall which vary significantly by presenting diagnosis. Patients of racial/ethnic minority groups, those who are publicly insured, and those residing the farthest form our institution were the most likely to experience early termination of follow-up with the multidisciplinary team.
Black patients and patients of other racial minority groups were followed an average of two less years than white patients, and these racial identities were independent predictors of attrition in a multivariable model controlling for other factors. While this study was not designed to investigate access to secondary surgery, it has been established that minority racial groups are more likely to experience delayed secondary surgery, including alveolar bone grafting.9,15,16 Patmon et al. demonstrated that both Black and Hispanic patients were significantly more likely to undergo bone grafting later than 12 years of age. 16 This is notable in the context of existing evidence suggesting that complications are lower and bone graft success is greater when performed earlier.17–19 Taken together, it appears that there is evidence for delays in care, risk for inferior outcomes, and decreased retention among minority patients. There are many possible factors which may influence follow-up rates and rates of secondary surgeries in minoritized populations including health literacy, cultural preferences, referral patterns, and distrust of the healthcare system, all of which have been studied extensively in other contexts within plastic surgery, notably breast reconstruction.20–24 These factors considered, it is possible that targeted outreach for patient education, flexible appointment scheduling, and cultural humility may aid in narrowing this existing gap.
The present study found that relative to other factors, income level was not a predictor of attrition. However, prior research has shown that income level does interact with disparities in access to secondary cleft surgery. For example, Badiee et al. found that patients of families making below $50,000 per year had a 15-month relative delay to alveolar bone grafting. Similarly, there is evidence that patients of families in the top income quartile have higher odds of undergoing secondary rhinoplasty. 12 Results from this study suggest surgical access disparities on the basis of income are less likely the result from increased attrition from cleft clinic in these groups.
Patients who are publicly insured experience challenges across the spectrum of cleft care, including delays in primary surgery,25–27 higher frequencies of missed appointments,28,29 and lower odds of receiving timely secondary surgery.12,30 These disparities are certainly tied to the large demand for health care services and high health care costs among patients with orofacial clefts, which has been demonstrated in both privately and publicly insured populations.31,32 It is perhaps unsurprising that these inequities were recapitulated here with publicly insured patients having higher odds of attrition in the present cohort, as compounding costs across patient development place the most strain on these patients. Interestingly, the difference in attrition rate between privately and publicly insured patients seemed to be greatest from birth to 5 years of age, after which rates did not significantly differ. This perhaps implies that particular attention should be paid towards young publicly insured patients, especially considering that surgical interventions including alveolar bone grafting have likely not yet been completed.
Is there a clinical impact to attrition earlier in adolescence? We believe there are several reasons to suspect so. First, because Phase 2 orthodontics are performed typically at 14–18 years of age and approximately 1/3 of patients are candidates for orthognathic surgery, 33 earlier loss of follow-up foregoes these interventions. Second, we find that secondary cleft rhinoplasty, also performed at skeletal maturity, imparts high patient satisfaction due both to improved facial aesthetics and nasal function, 34 and would likewise be foregone with early cessation of care. This would predominantly affect those patients with a diagnosis of cleft lip and palate, who more frequently require these secondary interventions. Third, with increased attention to psychological health such as through use of the CLEFT-Q, 35 we note the importance of mental health support through adolescence. These factors contrast with attrition in patients with nonsyndromic craniosynostosis, for instance, where the tail end of treatment is primarily about screening for rare cases of relapse or regression.
To be sure, it may be possible to predict at an earlier age, such as 12 years of age, who is likely to need the above services and who may be a reasonable candidate for “early graduation.” Part of our observed attrition may have been medically reasonable “graduates,” and thus stand as falsely positive cases of attrition. However, this would not be expected to occur more frequently in those with socioeconomic factors associated with barriers to care, and in fact we would expect the opposite due to documented delays of care and increased complication rates.27,36,37 Nonetheless, given the family-born costs of continued cleft team attendance, 13 we are interested in conceptually developing an “early graduation” assessment. This could have the dual benefit of reducing unnecessary visits in some patients through early graduation, while reinforcing the rationale for and importance of continued attendance for those in whom it is indicated.
Attrition by the age of 15 among patients with cleft lip and palate in the present study was 38%. This is a notable contrast from prior research investigating cleft clinic patient retention which reported that 62% of patients with cleft lip and palate were lost to follow-up prior to cleft clinic graduation, although the graduation year in this study was set at 16 years of age. 13 This is likely owing to the fact that this study included patients who were not yet old enough to have graduated, and indeed the authors noted that nearly 10% of patients initially characterized as lost to follow-up represented to clinic after gaps in care of 2 or more years. The present study spans nearly 30 years of clinical encounters and all patients who were included are currently 15 years or older, thus it is less likely that this methodology is not capturing patients with large lapses in follow-up who will later return to clinic. This could also reflect success of efforts our program has placed on emphasizing the importance of continuity through high school age. Still, it is important to reinforce that the goal of the study was not to establish an ideal target for clinic attendance rates by a particular age range, but rather, to compare attrition across groups which may otherwise be expected to display similar attendance patterns.
There are a number of limitations to the present study. First, the data collection was retrospective and can only assign associations between sociodemographic factors and length of follow-up. Second, while the results suggest a mechanism of understanding disparities in the timing and delivery of secondary cleft surgeries, rates of the secondary surgeries were not included in this cohort. Multiple studies referenced here have used national databases to address these disparities, but those databases are not well-suited to investigate longitudinal patient follow-up. Travel distance and income estimates were based on patient address and zip code which may or may not reflect patients who have changed address across the study period. While patients may generally be expected to change address to new locations with similar median income estimates, the distance from our institution is certainly subject to change and adds variability to the results.
Still, this analysis of a large, diverse population of older patients with orofacial clefts has demonstrated several factors which were significantly associated with long-term attrition from cleft clinic. Targeted outreach may be particularly beneficial toward narrowing observed gaps in alveolar bone grafting, rhinoplasty, and orthognathic surgery among marginalized sociodemographic groups.
Conclusions
This study was conducted to investigate whether long-term attrition from cleft clinic follow-up may be a plausible mediator of observed socioeconomic disparities in secondary cleft surgery. We report that race, insurance coverage, and travel distance were associated with early cessation of care in multidisciplinary cleft clinic. Attrition rates in these groups were high, and vulnerable populations may be hypothesized to benefit from targeted outreach regarding adolescent and teenage cleft clinic attendance.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241234804 - Supplemental material for Sociodemographic Factors Predict Long-Term Attrition from Multidisciplinary Cleft Clinic
Supplemental material, sj-docx-1-cpc-10.1177_10556656241234804 for Sociodemographic Factors Predict Long-Term Attrition from Multidisciplinary Cleft Clinic by Connor S Wagner, Sarah L Barnett, Dominic Romeo, Carrie Z Morales, Lauren K Salinero, Carlos E Barrero, Matthew E Pontell, Rachel A McKenna, Nancy Folsom, Jesse A Taylor and Jordan W Swanson in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
None.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.