
Abstract
Objectives
To objectively quantify results of sagittal lip changes following Abbe flap reconstruction in patients with bilateral cleft lip.
Design
Retrospective, observational study.
Setting
Single institution, 8-year retrospective review.
Patients/Participants
In total, 17 patients with bilateral cleft lip that underwent Abbe flap reconstruction were included in this study.
Intervention
Patients had lateral photographs taken prior to Abbe flap reconstruction and at least 8 months post-Abbe flap.
Main Outcome Measurements
Vegter's index, Sushner's S2 line and Burstone's B line reference lines were used for evaluation of sagittal lip changes. Wilcoxon signed rank tests were used in analysis.
Results
The mean pre-Abbe flap upper to lower lip ratio, defined as Vegter's Lip Index, was 0.906 compared to a mean of 0.946 following Abbe flap reconstruction. The mean upper to lower lip ratio for Sushner's S2 and Burstone's B line exhibited an increase in upper lip sagittal projection from −0.164 to 1.459 and 0.259 to 0.957, respectively (P < 0.001).
Conclusions
This study quantifies sagittal changes to upper and lower lip position after Abbe flap reconstruction. These findings may aid in operative planning and patient/caregiver expectations during counseling.
Introduction
The Abbe flap was first described by Dr. Robert Abbe in 1898 as a method of addressing the secondary correction of a bilateral cleft lip deformity. 1 This technique addresses upper lip deformities associated with a bilateral cleft lip by restoring the philtrum, Cupid's bow, and central tubercle. Furthermore, upper to lower lip apposition can be improved through horizontal reduction of the lower lip which can address excessive lower lip vermillion projection. 2
Studies have evaluated the soft tissue profile and frontal photographs in repaired complete bilateral cleft lip and palate, reporting on differences in comparison with the non-cleft population. 3 Additionally, it has been recorded that Abbe flap reconstruction increases vermillion lip length and Cupid's bow width, providing adequate bulk to the middle of the lip in the frontal plane. 4
Despite its common use, there is a paucity of literature quantifying results on the sagittal projection of Abbe flaps in patients with bilateral cleft lip. Lip position is an important factor for achieving facial harmony 5 and patients with cleft lip and palate have been found to have a thicker, more everted lower lip as compared to noncleft controls. 6 Furthermore, as the Abbe flap is a significant procedure for a patient to endure and patients commonly request predicted results of proposed reconstructive procedures, a thorough understanding of the benefits of the reconstruction are critical to making an informed decision. Therefore, this study objectively quantifies results of sagittal lip changes following Abbe flap reconstruction in patients with bilateral cleft lip using lateral view 2D photographs.
Method
Patient Cohort
Following approval from the Institutional Review Board (IRB), a single institution, 8-year retrospective review was performed of all patients with a bilateral cleft lip who underwent Abbe flap reconstruction between 2015 and 2022. Patients with lateral photographs taken prior to Abbe flap reconstruction and at least 8 months after division and inset of Abbe flap were included. Patients were excluded if they underwent lip revision surgery prior to their follow-up lateral photograph or if Abbe flap reconstruction was performed for an iatrogenic defect such as a skin cancer excision.
Photograph Selection and Standardization
All lateral standardized photographs were taken in a dedicated medical photography suite by one of two photographers with formalized training in medical photography and analyzed using Dolphin software (Imaging and Management Solutions, Chatsworth, Calif, USA). Lateral photographs were included if they were taken in natural head position, and clearly included the ears, forehead, and neck. Photographs were taken from the same side of the patient.
Photograph Measurements Protocol
For this study, Vegter's Lip Protrusion Index 7 along with Sushner's S2 line 8 and Burstone's B line 5 were chosen as reference lines for evaluation of sagittal lip changes following Abbe flap reconstruction in patients with bilateral cleft lip. These measurements are standard lateral view lip measurements which are independent of nasal tip position, especially important as many study patients underwent simultaneous rhinoplasty at the time of division and inset of the Abbe flap. Furthermore, the subnasale and nasion reference points used in Burstone's B line and Sushner's S2 line, respectively, are not expected to change following concomitant rhinoplasty, ensuring that these points are stable references for this patient cohort.
Vegter's Lip Protrusion Index is defined as the ratio of the distance of the labiale superius (Is), the mucocutaneous limit of the upper lip, to the tragion (t), the notch above the tragus, over the distance of the labiale inferius (li), defined as the mucocutaneous limit of the lower lip, to the traigon (Figure 1a).
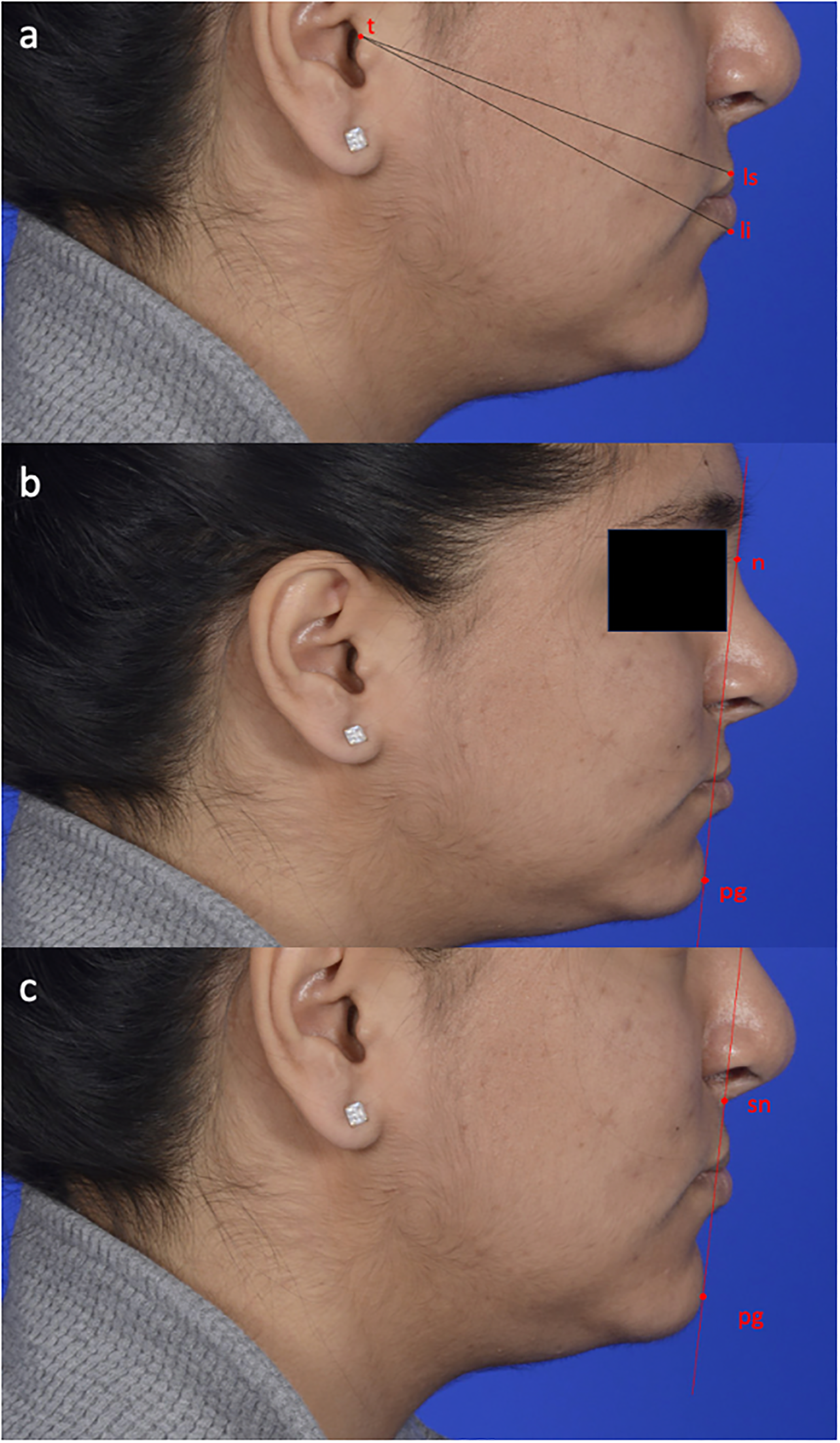
Lip Reference Ratios a. Vegters lip index b. Sushner's S2 Line c. Burstone's B Line. Patient of DAS.
Sushner's S2 reference line is drawn from the soft tissue pogonion (pg), the most anterior point on the soft tissue chin, to the soft tissue nasion, the point of greatest concavity in the midline between the forehead and the nose (Figure 1b).
Burstone's B reference line is drawn from the soft tissue pogonion (pg), the most anterior point on the soft tissue chin, to the subnasale (sn), the point where the columella (nasal septum) merges with the upper lip in the mid-sagittal plane (Figure 1c).
Measurements at pre-operative and at least 8-month post-operative time-points for each patient comprised of the horizontal distance from the most anterior point of the upper lip, to both Sushner's S2 line and Burstone's B line, as well as from the most anterior point of the lower lip to Sushner's S2 line and Burstone's B line. Positive distances were noted if position of the lips were anterior to the reference lines, while negative distances were noted if position of the lips were posterior to the reference lines. The ratio of the upper lip horizontal distance to the lower lip horizontal distance was calculated for Sushner's S2 line and Burstone's B line. Two independent measurements were taken by two different examiners to obtain intraclass correlation coefficient.
Data Collection
Demographic characteristics collected from the electronic medical records of the study population included sex, age at surgery, age at preoperative and post-operative photograph, and time between surgery and pre-and postoperative photographs. Characteristics related to Abbe flap reconstruction of cleft lip repair surgery included presence of comorbidities, prior alveolar bone grafting, orthognathic surgery, operative time for Abbe flap reconstruction, presence of a complication associated with Abbe flap creation and division (dehiscence, wound breakdown, flap loss, infection), date of division, length of time to division, operative time of division, concurrent cleft rhinoplasty at time of division, any revision surgery and length to follow-up.
Statistical Analysis
Wilcoxon signed rank tests were utilized to analyze the pre-and post-Abbe flap measurements. Mann-Whitney U tests were conducted to analyze pre- and post-Abbe flap differences between patients who received a concomitant rhinoplasty at time of Abbe flap creation and those who did not. P values less than 0.05 were considered statistically significant. An intra-class correlation coefficient analyzed reliability of measurements between two examiners. Statistical analyses were calculated in Stata/SE (Version 14.2; StataCorp LLC, College Station, TX).
Results
Patient Demographics
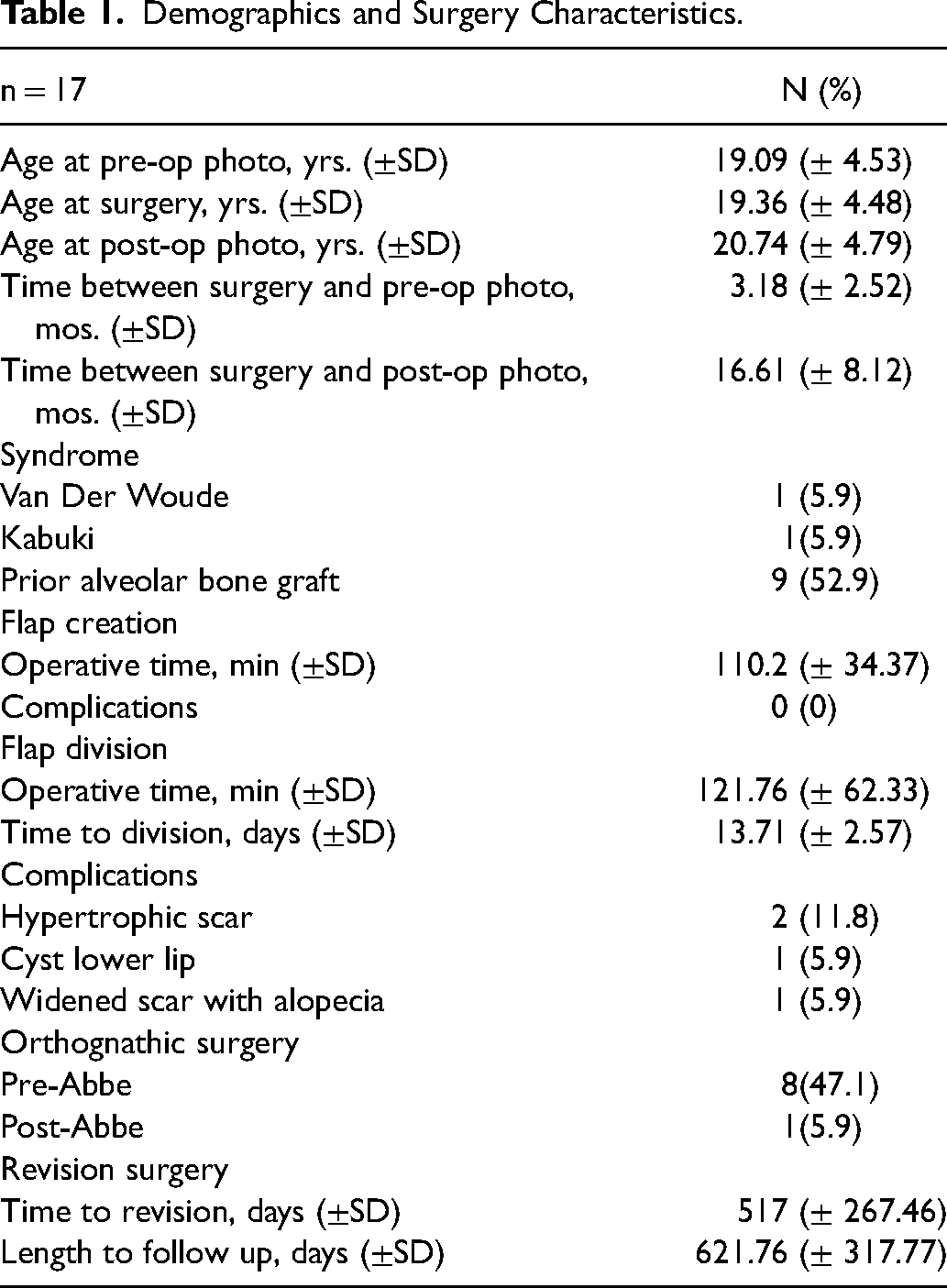
A total of 17 patients that underwent Abbe flap reconstruction for bilateral cleft lip were included in this study. The mean age at surgery was 19.4 years (range 12.6–33.4 years). The mean time from the pre-operative photograph to time of surgery was 3.2 ± 2.6 months and the mean time from surgery to the post-operative photograph was 16.6 ± 8.1 months (Table 1).
Demographics and Surgery Characteristics.
Comorbidities and Prior Surgeries
Two patients were noted to be syndromic: one patient with Kabuki syndrome and one with Van Der Woude Syndrome. Nine patients (52.9%) underwent alveolar bone grafting and 8 patients (47.1%) underwent orthognathic surgery prior to Abbe flap reconstruction (Table 1).
Surgical Characteristics and Complications
The mean operative time for Abbe flap creation was 110.2 (± 34.4) minutes. The mean time to division was 13.7 (± 2.57) days. No patients experienced complications between Abbe flap creation and division. The mean operative time for Abbe flap division was 121.8 (± 62.3). Nine patients (52.9%) underwent concurrent rhinoplasty at time of Abbe flap division and inset, thus explaining the longer operative time. Anterior nasal spine was not taken down in any of these patients. One patient had orthognathic surgery post Abbe flap. Post-operative photos were analyzed prior to orthognathic surgery in this patient. Four patients (28.6%) experienced minor postoperative complications after division and inset of the flap which required revision surgery. This included 2 patients (11.8%) with hypertrophic scars, 1 patient (5.9%) with a lower lip cyst and 1 (5.9%) patient with a widened scar with alopecia. Photographs were taken prior to revision surgery and the scar/cyst did not affect the position of the lower lip. Revision surgery was conducted at a mean time of 517 ± 267.5 days after Abbe flap surgery and included 2 fat-grafting procedures and 2 scar excisions. The mean length of follow-up for all patients was 621.8 ± 317.8 days (Table 1).
Sagittal Lip Measurements Pre-and Post-Abbe Flap
The mean preoperative upper to lower lip ratio as defined by the Vegter's index was 0.906 (0.888–0.925, 95% CI) with a range from 0.842 to 0.976. The mean postoperative upper to lower lip ratio was 0.946 (0.932–0.959, 95% CI) with a range from 0.89 to 0.986 (Figure 2). The upper to lower lip ratio post-Abbe flap was found to be statistically different as compared to the pre-Abbe flap ratio (p < 0.0001) consistent with an improvement in sagittal lip position of the upper lip compared to the lower lip (Table 2).
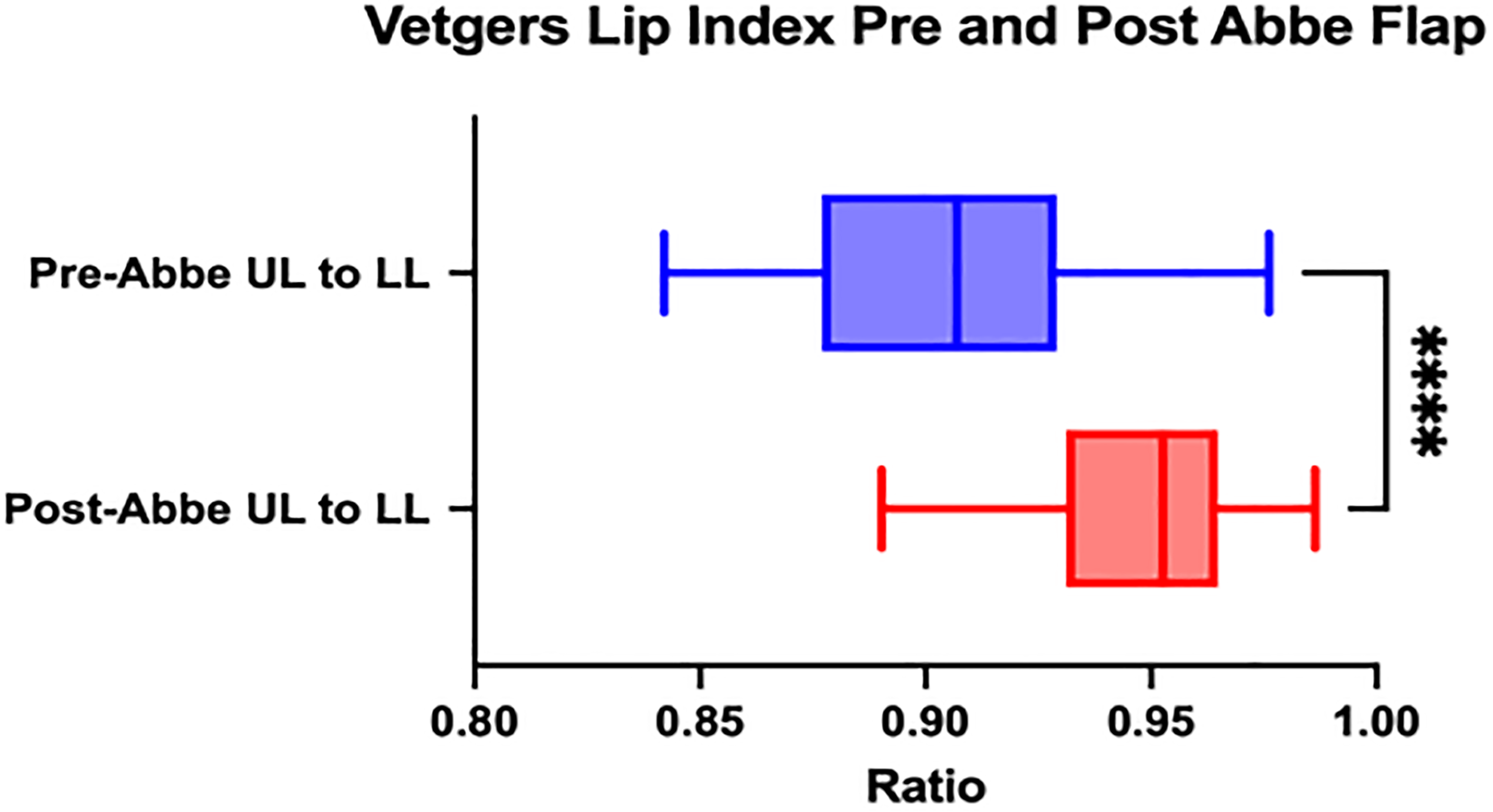
Vegters lip index pre-and post- Abbe Flap (p < 0.0001).
Descriptive Statistics for Burstone's B Line, Sushner's S2, and Vegters Lip index pre- and Post- Abbe Flap Reconstruction.
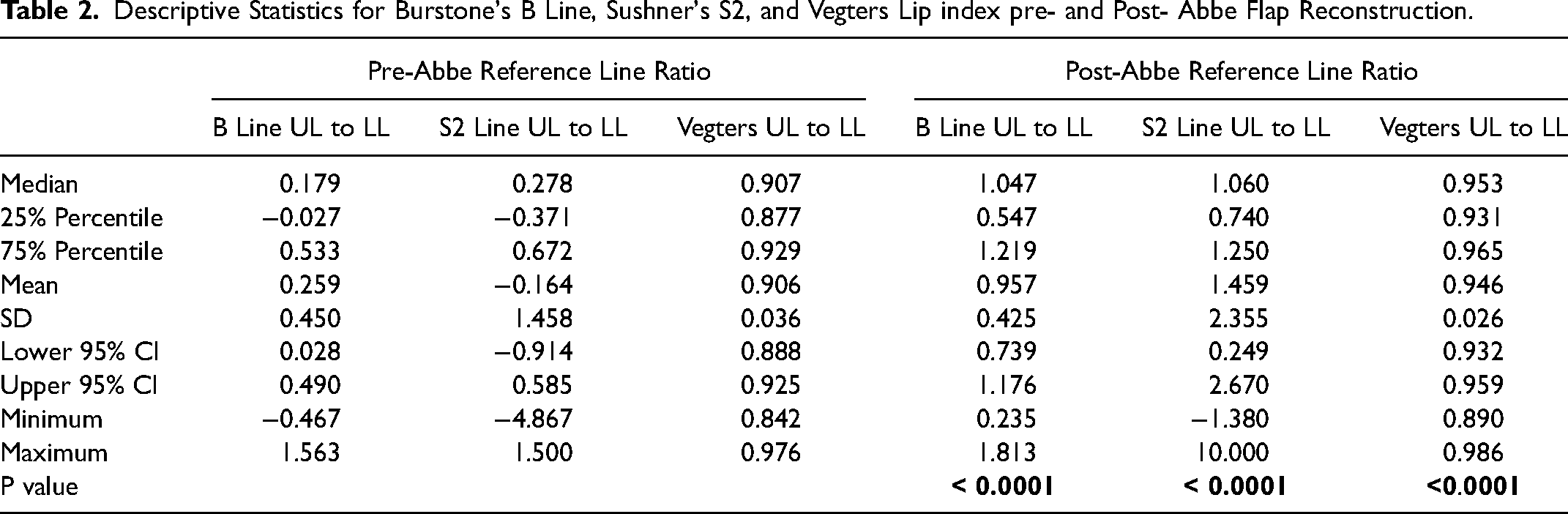
The mean pre-Abbe flap lip ratio regarding Sushner's S2 Line was −0.164 (−0.914–0.585, 95% CI) with a range from −4.867 to 1.500. Post-Abbe flap reconstruction, the mean upper to lower lip ratio was 1.459 (0.249–2.670, 95% CI) with a range from −1.380 to 10.000 (Figure 3). The lip ratio post-Abbe flap was statistically different when compared to the pre-Abbe flap lip ratio with a P value of <0.0001 (Table 2).
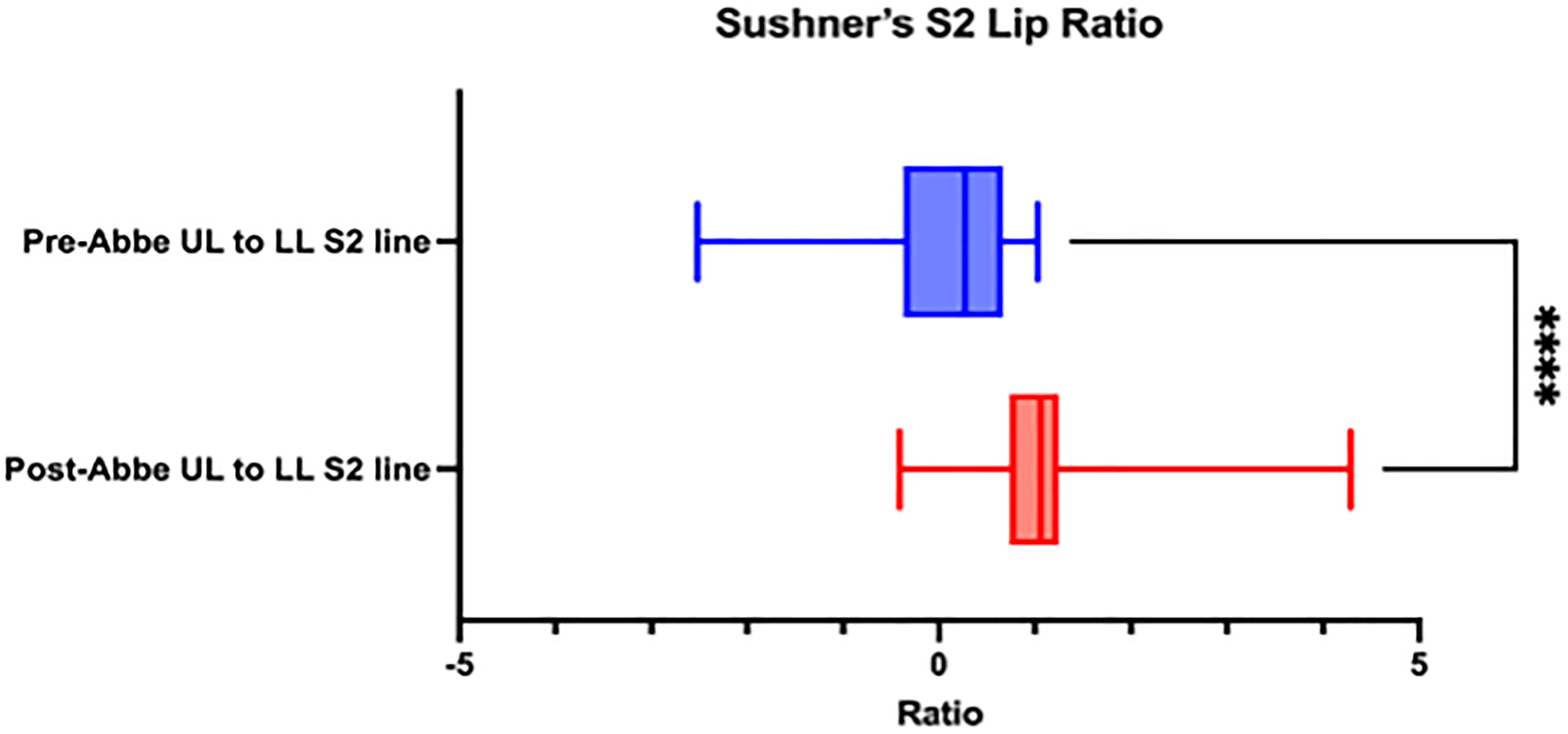
Sushner's S2 Line upper to lower lip ratio pre- and post- Abbe reconstruction (p < 0.0001).
The mean pre-Abbe upper to lower lip ratio regarding Burstone's B Line was 0.259 (0.028- 0.490, 95% CI) with a range from - 0.467 to 1.563. Post- Abbe flap reconstruction, the mean upper to lower lip ratio was 0.957 (0.739–1.176) with a range from 0.235 to 1.813 (Figure 4). The lip ratio post-Abbe flap was statistically different when compared to the pre-Abbe flap lip ratio with a P value of <0.0001 (Table 2).
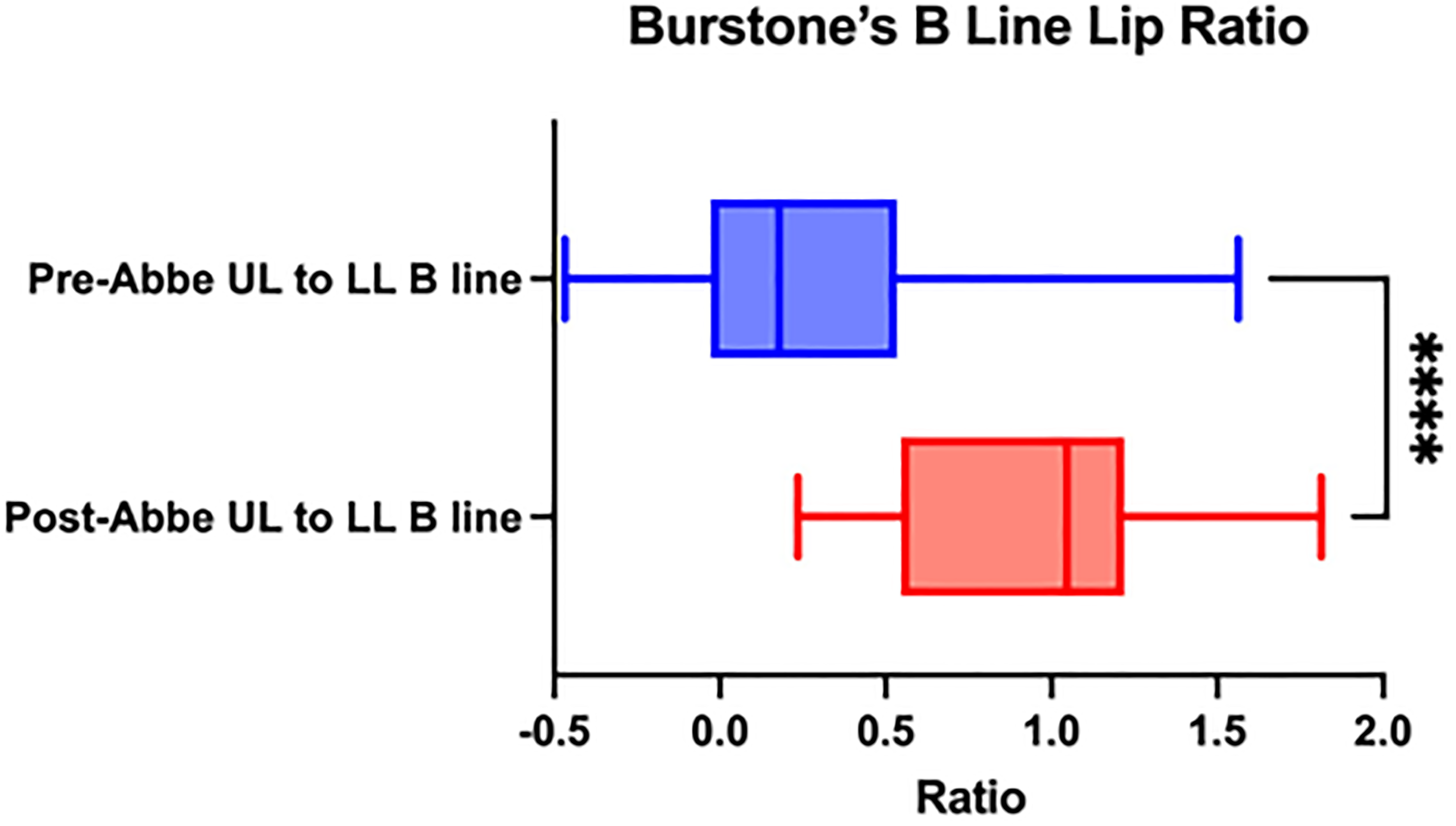
Burstone's B Line upper to lower lip ratio pre- and post- Abbe reconstruction (p < 0.0001).
Furthermore, there were no differences in Vegter's index, Burstone's B Line or Sushner's S2 Line measurements when comparing patients that received or did not receive rhinoplasty at the time of Abbe flap creation (p > 0.05).
Discussion
This study details the sagittal lip changes following Abbe flap reconstruction. Regarding the Vegter's protrusion index, there was a significant increase in upper lip sagittal projection as compared to lower lip projection, from 0.906 to 0.946, following Abbe flap reconstruction. The mean upper to lower lip ratio for Sushner's S2 and Burstone's B and line similarly demonstrated an increase in sagittal projection from −0.164 to 1.459 and 0.259 to 0.957, respectively. These results help quantify changes in lip sagittal projection following Abbe flap reconstruction to help improve facial harmony for these patients.
Anteroposterior lip position has long been regarded a significant factor in achieving facial harmony and thus an aesthetically pleasing facial profile.5,9 The presence of a lower lip deformity following primary cheiloplasty in patients with a bilateral cleft lip has been well described. 10 Recent studies have further quantified lower lip abnormalities in CLP patients, finding that those with maxillary hypoplasia have a significantly thicker lower lip and outward rotation of the vermillion border compared to noncleft controls, with patients with a bilateral cleft lip exhibiting a thicker lower lip as compared to patients with unilateral cleft lip. 6 While Abbe flap reconstruction has been described as an effective means of addressing significant secondary lip deformities,4,11 few studies have objectively quantified sagittal lip changes in this population.
Of the published literature reporting objective measurements on treatment outcomes of Abbe flap reconstruction on aesthetic improvement, most available studies delineate a quantitative method for photographic evaluation in the frontal view.3,12 Using computer-assisted anthropometric analysis of frontal photographs, Ramanathan et al. found that Abbe flap reconstruction consistently improved symmetry for horizontal and vertical lip lengths, Cupid's bow width, and vermillion length. 4 Additionally, a recent study performed by Long et al. utilized a combination of frontal and lateral measurements based on classical soft tissue landmarks established by Farkas13–15 to quantify the treatment effect of nasolabial reconstruction in Abbe flap patients. 16 Long found a significant difference in lip protrusion angle, nasolabial angle, and columellar-labial angle, among other parameters, following reconstruction in cohorts stratified by level of lip deformity severity. This quantitative analysis allows for the identification of sensitive indicators and reference parameters to aid in patient selection for Abbe flap reconstruction, suggesting the importance of performing both frontal and lateral measurements involving the lips to better characterize Abbe flap results. 16
The Vegter protrusion index was described as a quantification method of the forward protrusion of the upper lip to the lower lip in patients that had undergone an Abbe flap procedure from lateral photographs. 7 Our results of increased sagittal projection of the upper lip compared to the lower lip are consistent with Vegter's initial analysis, where he defined a normal lip index as 0.97–0.99 in noncleft patients, where CLP patients consistently had a less than normal preoperative lip ratio that was improved following Abbe flap reconstruction. 7 Our group found a relative increase in upper lip projection and decrease in lower lip projection that is consistent with the subjective direct facial observation method of the Abbe flap procedures for correction of lip deformities in patients with bilateral cleft lip. 11
These findings are replicated in our study when performing the analyses using the Sushner's S2 reference line and Burstone's B reference line. Currently, the 5 most commonly used reference lines that evaluate lip position to aid in orthodontic treatment planning include the Sushner's S2, Burstone's B line, Holdaway's H line, Ricketts E line, Steiner's S1 line.5,8,9,17,18 Steiner's S1 line, that runs from the soft tissue pogonion to the curvature of the nose, Rickett's E line, that runs soft tissue pogonion to the most anterior point of the soft tissue nose, and Holdaway's H line, that runs from the soft tissue pogonion to the outer prominence of the upper lip all depend on nasal growth and/or lip position. We chose to use Sushner's S2 line and Burstone's B line for lip evaluation due to their independence of nose and lip position. This was an important consideration as many of our patients underwent rhinoplasty at the time of Abbe flap division and inset, which would skew the reference line on the postoperative image for Steiner's S1 line and Rickett's E line and not allow for comparison of quantitative changes in lip position pre-and post-Abbe flap reconstruction. Multiple studies have used Burstone's B line and Sushner's S2 line to describe lip protrusion and retrusion to quantify sagittal lip changes following orthodontic treatment19,20 as well as identifying differences across skeletal malocclusions and populations.21–23 Additionally, studies show that Sushner's S2 line and Burstone's B line demonstrate the smallest coefficient of variance with respect to upper and lower lip as compared to the other reference lines, showing consistency and reliability in the assessment of the horizontal position of lips in the lateral view across different populations.23,24
Methods that have been used for facial aesthetic evaluation include photogrammetry,25,26 cephalometry, 27 and the development of cone-beam computed tomography. 28 While Sushner's S2 and Burstone's B line were initially established for cephalometric analyses, 8 patients with CLP not undergoing orthodontics treatment may not have these forms of analyses available, relying on the use of 2D digital photographs as the only means of objective evaluation of facial profile pre- and post- CLP repair. As previous studies have conducted the analyses of these reference lines using 2D photographs,24,29 and the Vegter's index was established specifically for photographic analyses, our study was conducted using this method of soft tissue profile analysis. Furthermore, we chose to display the Burstone's B line and Sushner's S2 line measurements as upper to lower lip ratios, as this eliminates the need for magnification standardization required to determine absolute measurements. 12
This study provides an objective analysis of sagittal lip changes after Abbe flap reconstruction in patients with a bilateral cleft. These data will aid in preoperative patient counseling, prediction of surgical results and patient indication. Limitations of this study include a small sample size. Additionally, this is a retrospective study at a single institution. As there were no rulers present in the photographs used, absolute measurements for the reference lines chosen could not be conducted, so the values achieved for Sushner's S2 line and Burstone's B line were unable to be compared to the normative values established across different populations in previous work. Future studies may include a larger patient population over multiple institutions and should seek to replicate these results to increase reliability of the methods described.
Conclusion
Abbe flap reconstruction in patients with a bilateral cleft can increase upper lip sagittal projection as well as decrease lower lip sagittal projection. These findings provide cleft teams with objective data to better aid in operative planning and patient/caregiver expectations during counseling.
Footnotes
Acknowledgements
This study received ethical approval from the institutional IRB. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.