
Abstract
Objective
This study aimed to determine the efficacy of gingivoperiosteoplasty (GPP) in preventing alveolar bone grafting (ABG) among children with cleft lip and palate (CLP).
Design/Setting
Retrospective university hospital single center study.
Patients
Children with CLP treated with GPP from 2000-2015 were included. Those under eight years of age, without definitive conclusions regarding need for ABG or with incomplete data were excluded.
Interventions
Included patients were analyzed for demographics, cleft type, age at GPP, associated cleft surgery, use of nasoalveolar molding (NAM), indication for ABG, operating surgeon and presence of residual alveolar fistula. T-tests and Fisher's exact tests were utilized for statistical analysis.
Main Outcome Measure
The need for ABG.
Results
Of the 1682 children identified with CLP, 64 underwent GPP and met inclusion criteria. 78% of patients with CLP who underwent GPP were recommended for ABG. Those who received GPP at a younger age (P = .004) and at the time of initial cleft lip repair (P = .022) were less likely to be recommended for ABG. Patients with complete CLP were more likely to be recommended for ABG than patients with cleft lip and alveolus only (P = .015). The operating surgeon impacted the likelihood of ABG (P = .004). Patient gender, race, ethnicity, laterality, and NAM were not significantly associated with recommendation for ABG.
Conclusion
GPP does not preclude the need for ABG. Therefore, the success of ABG after GPP and maxillary growth restriction should be analyzed further to determine if GPP is a worthwhile adjunct to ABG in cleft care.
Introduction
Alveolar clefts are present in approximately 75% of patients with orofacial clefts. 1 The goals of reconstruction are to restore the position and bony continuity of the maxillary arch, facilitate a satisfactory periodontal environment for dental eruption, achieve closure of the oronasal fistula and minimize damage to surrounding dentition and maxillary growth. The optimal treatment strategy to accomplish these goals remains a point of controversy among providers in cleft care.2–7 Gingivoperiosteoplasty and alveolar bone grafting are the main approaches utilized to reconstruct the alveolar cleft.6,8–10
Gingivoperiosteoplasty (GPP) is performed at either the time of primary cleft lip repair or cleft palatoplasty in an effort to minimize the number of secondary surgeries for patients with clefts.11–15 It relies on the osteogenic capacity of the child's periosteum to bridge the alveolar defect.13,14 GPP is undertaken with the goals to eliminate the nasolabial fistula early in life, simplify subsequent alveolar bone grafting, minimize inferior descent of the premaxilla in bilateral complete cleft lip and ultimately reduce the need for alveolar bone grafting (ABG).15–17 The alveolar cleft repair technique and/ or extent of GPP performed, implementation of nasoalveolar molding (NAM), width of the cleft, and operating surgeon have variable impacts on the success of GPP and its effects on facial growth.6,18–23 Success rates following GPP range greatly from 0%-90%.11,13,24–26
Secondary alveolar bone grafting (SABG) is the most common technique for alveolar reconstruction in patients with clefts of the alveolus and was first described in 1972. 27 This is due to its predictability, minimal impact on maxillary growth, provision of sufficient bone quantity, and closure of the oronasal fistula.8,28 Complications of SABG include donor site morbidity, potential need for overnight hospitalization, risk of graft infection and/or insufficient graft take and need for repeat operations.29–31 Despite these challenges, SABG for the treatment of alveolar clefts has a reported success rate of over 90% and is considered the treatment of choice at most cleft centers.14,24,32,33
Many published studies examine a single surgeon's experience with GPP and the need for SABG following GPP as a measure of success.13,15,34–36 The primary goal of this study aims to determine what percentage of children with a cleft alveolus, who had undergone GPP, were recommended for secondary or tertiary alveolar bone grafting performed by multiple surgeons at one institution. The secondary goal of this study is to establish predictors of requiring ABG following GPP.
Methods
Following approval by the institutional review board at Oregon Health & Science University, all patients treated with cleft lip and palate at our academic institution from 2000-2015 were identified utilizing current procedural terminology (CPT) coding. Patients under eight years of age at last visit were excluded as we do not indicate patients for ABG before this age at our institution. A retrospective chart review was performed to identify all patients who had undergone GPP. Electronic health records (EHR) were then searched for all medical, dental and orthodontic records. Patients with a confirmed recommendation either for or against ABG were included for analysis, while those with unknown or unconfirmed need for ABG were excluded. Patients lost to follow-up or with incomplete EHR documentation were excluded. Data analyzed included demographics, cleft type, timing of GPP repair, age at GPP, associated cleft surgery at the time of GPP (primary cleft lip repair, cleft palatoplasty, other), NAM, indication for ABG, surgeon and the presence of a residual alveolar fistula.
Demographic and clinical characteristics of patients were analyzed. An independent samples t-test was used to compare the mean age at GPP between the groups. For all categorical variables, Fisher's exact tests were used. A 5% significance level was used. Given the retrospective nature of this study, need for patient consent for use of their information was waived by the institutional review board.
A complete comprehensive treatment description of a patient with a cleft is beyond the scope of this paper. However, our historical, institutional cleft protocol related to NAM, GPP and alveolar bone grafting are as follows. At initial evaluation, usually within the first few weeks of life, the patient with a cleft is evaluated by our multidisciplinary team including the craniofacial surgeon, nurse practitioner, and craniofacial orthodontist. Adequate weight gain and familial support are prioritized and candidacy for NAM is evaluated. At our center, NAM is typically recommended for children with wide (alveolar cleft greater than 6 mm), unilateral, complete clefts and bilateral complete clefts when medically safe and geographically feasible. Primary cleft lip repair occurs around 3-6 months of age. Generally, primary repair is closer to 6 months of age for those completing NAM. Historical criteria for performing GPP at our institution were a small bone gap, non-collapsed arch, and well-aligned bone segments, although there is variability to the significance of these criteria per surgeon. Additionally, if this criteria was felt not to be met at the time of primary lip repair, but met at a later time, either during palate repair or revision surgery, four surgeons performed GPP at these time frames. GPP was attempted with the dissection limited to the tissues within the cleft when feasible.25,28 However, if unachievable with gingivoperiosteal flaps adjacent to the cleft, maxillary subperiosteal dissection was performed to create the mucoperiosteal bridge. Patients with an alveolar cleft are seen by both the craniofacial surgeon and craniofacial orthodontist yearly to monitor dental development. We utilize clinical examination, panoramic x-rays and periapical x-rays starting at age 7 to determine the subjective need and timing for alveolar bone grafting. Primarily, we look at the formation of bone spanning the cleft, adequate bone to support relative dentition, and assessment of residual alveolar fistula. Cone beam computed tomography (CBCT) is not available at our institution (Table 1).
Treatment Protocol.
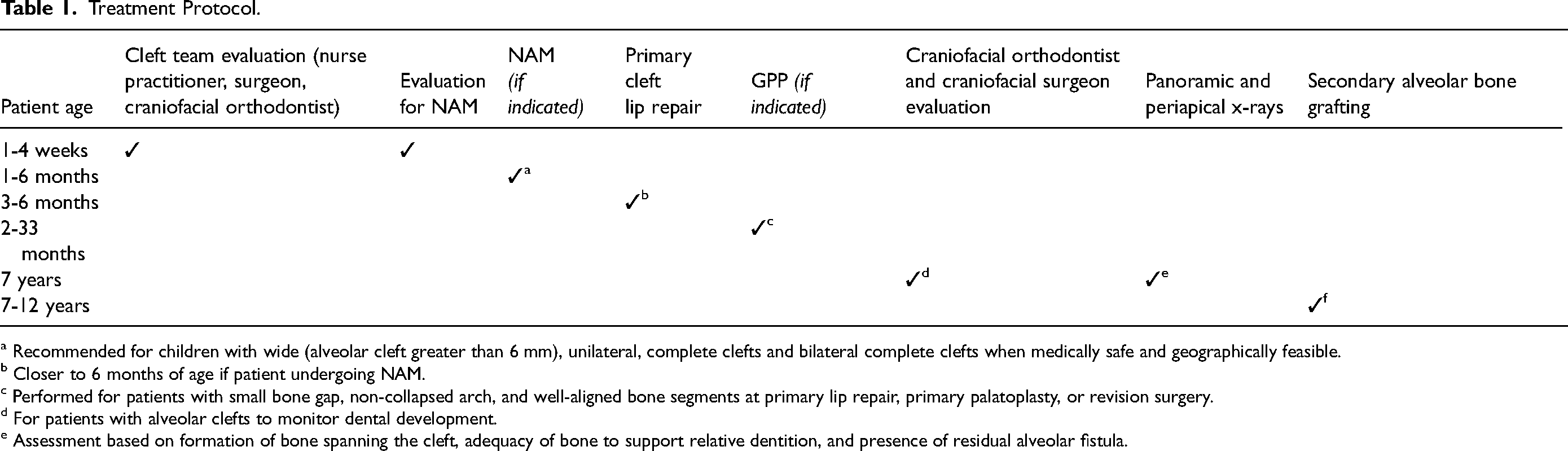
a Recommended for children with wide (alveolar cleft greater than 6
b Closer to 6 months of age if patient undergoing NAM.
c Performed for patients with small bone gap, non-collapsed arch, and well-aligned bone segments at primary lip repair, primary palatoplasty, or revision surgery.
d For patients with alveolar clefts to monitor dental development.
e Assessment based on formation of bone spanning the cleft, adequacy of bone to support relative dentition, and presence of residual alveolar fistula.
Results
Out of 1682 patients with cleft lip and palate (CLP) identified during the study period, 87 (5.17%) patients underwent GPP. 10 patients without definitive conclusion of need for ABG and 13 who were lost to follow up were excluded from analysis. The 64 remaining patients with definitive conclusions regarding the need for ABG at the time of the study were included in the analysis. Of these patients, 21 were female and 43 were male. Patient demographics are summarized in Table 2. Of the 64 included patients, 16 (25%) had unilateral cleft lip and alveolus (UCLA), 2 (3.1%) had bilateral cleft lip and alveolus (BCLA), 38 (59.4%) had unilateral cleft lip and palate (UCLP) and 8 (12.5%) had bilateral cleft lip and palate (BCLP). For analysis, they were grouped into those patients who had cleft lip and alveolus (n = 18) and those patients with complete cleft lip and palate (n = 46). Fifty-nine patients (including all patients with unilateral clefts and three patients with bilateral clefts) had unilateral alveolar clefts treated with GPP. Five patients with bilateral cleft lip and alveolus were treated with bilateral GPP. GPP was undertaken at the time of primary lip repair in 34 patients (53.1%), primary palatoplasty in 27 patients (42.2%) and other revision surgery in three patients (4.7%) (Table 3). Of those who underwent GPP at revision surgery, this consisted of cleft lip revision with a complete takedown for 2 patients (one at 14 months and another at 34 months) and cleft palate revision for one patient (at 19 months).
Patient Demographics.
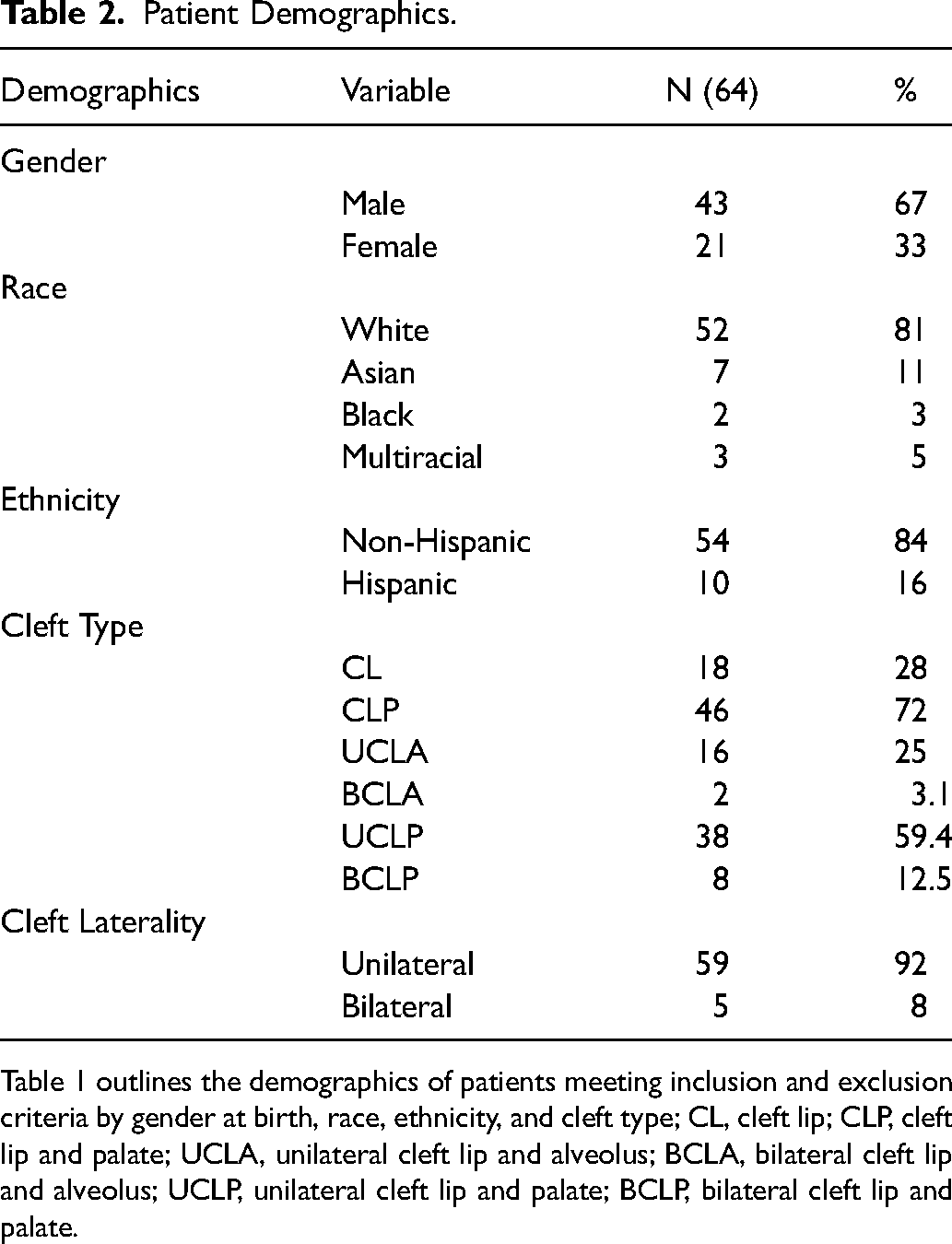
Table 1 outlines the demographics of patients meeting inclusion and exclusion criteria by gender at birth, race, ethnicity, and cleft type; CL, cleft lip; CLP, cleft lip and palate; UCLA, unilateral cleft lip and alveolus; BCLA, bilateral cleft lip and alveolus; UCLP, unilateral cleft lip and palate; BCLP, bilateral cleft lip and palate.
Timing of GPP.
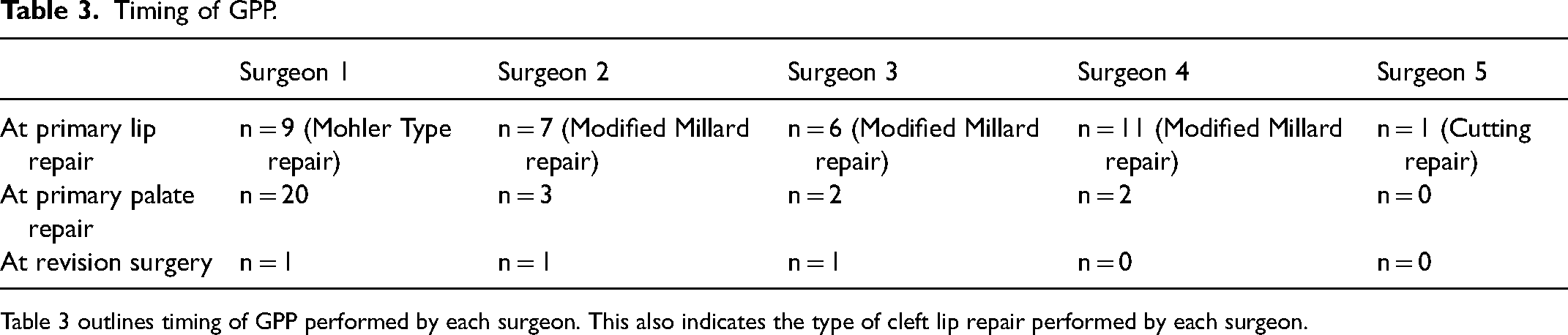
Table 3 outlines timing of GPP performed by each surgeon. This also indicates the type of cleft lip repair performed by each surgeon.
The mean age at GPP was 9.6 months with a range of 2.5 to 33.7 months. Fifty patients (78.1%) were indicated for secondary or tertiary alveolar bone grafting while 14 patients (21.9%) were deemed to have satisfactory bone formation without the need for ABG. Of the five patients with bilateral alveolar clefts treated with bilateral GPP, three (60%) required ABG to bilateral cleft sites and two did not need subsequent ABG. Among those indicated for bone grafting, 21 patients (42%) had undergone secondary or tertiary bone grafting at the time of the study. The mean age at SABG was 10.5 years. Two patients underwent tertiary bone grafting given eruption of their canines into the cleft prior to completion of SABG.
Twenty-seven patients (42.2%) completed NAM treatment prior to GPP. Eight patients were recommended NAM but did not complete treatment. Additionally, nineteen patients had no record of indications for or against the need for NAM. Of the 27 patients who completed NAM, 22 (81.5%) were indicated for ABG. Those who underwent NAM and subsequently required ABG comprised 44% of the 50 total patients indicated for ABG. For those recommended NAM who did not complete treatment, 100% required ABG. Details regarding final alveolar cleft width after NAM at time of cleft lip repair were not readily available for this patient cohort.
Those patients who received GPP at a younger age and those who received GPP at the time of initial cleft lip repair were less likely to be recommended for ABG, P = .004 and P = .022, respectively. Five surgeons were compared and the operating surgeon whom performed the highest number of GPPs was also more likely to have ABG recommended for their patient cohort (P = .004). Patients with a complete cleft lip and palate were more likely to have ABG recommend than patients with cleft lip and alveolus alone (P = .015). Of note, and as stated above, the alveolar cleft width was not assessed. Patient gender, race, ethnicity and laterality were not significantly associated with being more likely to be recommended for ABG. Residual nasolabial fistulae after GPP were noted in ten patients included in the analysis (15.6%).
Discussion
Gingivoperiosteoplasty remains a controversial treatment approach in alveolar cleft repair. The success rate of GPP is variable depending on the center and operating surgeon, with reported success rates ranging from 0%-90%.13,24–26,37 Several centers have found sufficient alveolar bone stock is achieved in 40%-70% of patients with CLP who underwent GPP with 20%-40% of those patients ultimately requiring ABG for definitive closure of the alveolar defect.13,24 Due to its unreliable results, some centers have abandoned the practice of GPP completely to avoid sequelae such as maxillary growth restriction, while others with higher success rates of alveolar cleft closure and adequate bony formation continue to advocate for its efficacy.13,14,38 Those in the cleft care community advocating for primary GPP cite eliminating the need for SABG at the time of mixed dentition as the major benefit of GPP. 16
Given the vast anatomical variations in patients with cleft lip and palate, not all infants are candidates for GPP. The success of GPP is inversely dependent on the size of the alveolar cleft.18,39 To reduce the alveolar width prior to GPP, presurgical molding or NAM can be performed.37,40 Additionally, NAM can facilitate alignment of the alveolar arch and prevent collapse.3,25,41 NAM followed by GPP has been reported to increase success of GPP after the alveolar cleft is narrowed to less than 6 mm in width.13,23,25,34,35 Other centers have more stringent criteria and recommend a well-aligned maxillary arch without bony step-off, an alveolar cleft width of less than 2 mm with gingival mucosa contact as a prerequisite for surgical success. With this more stringent criteria, they report up to 80% of unilateral clefts developing bone formation. 25 Wang et al. reported performing GPP on children with alveolar cleft gaps ranging from 0 mm - 0.5 mm. 13 They discuss that their success rate of 78% was due to small gaps with well-aligned arches and surgeon experience. However, both small and large gaps present surgical challenges for GPP. When small (<1 mm), elevating the subperiosteal flaps in very narrow alveolar defects is quite difficult and sometimes insufficient. 14 Significantly larger (>6 mm) alveolar gaps, usually encountered in cases where NAM is not completed, require extensive subperiosteal dissection.23,34,42 The larger alveolar gap exceeds the osteogenic potential of the pediatric periosteum to generate a significant alveolar bone bridge, resulting in poor alveolar bone quality and quantity. 42 As such, a narrow gap, close to 2 mm but ideally >1 mm, seems to be the ideal cleft width prior to GPP. 25
At our center, NAM is typically recommended for children with wide (alveolar cleft > 6 mm) unilateral clefts and bilateral complete cleft lips when medically safe and geographically feasible. However, due to various concerns including travel distance to treating center and challenges of treatment adherence, only one third of the children included in this study underwent NAM prior to GPP. While cleft widths were not obtained, it is conceivable that many patients in this study's cohort presented with alveolar clefts wider than 2 mm prior to undergoing GPP. This introduces a possible selection bias that may have negatively skewed the reported efficacy of GPP in this patient cohort.
GPP is a technically complex procedure with variable success rates that have been shown to vary significantly depending on the operating surgeon. 42 In our patient population, five surgeons performed GPP during the study period. Surgical provider was found to be a statistically significant contributor to the likelihood of being recommended for ABG (P = .004) with the operating surgeon performing the highest number of GPPs being more likely to have ABG recommended for their patients. This differs from other reports arguing that those with more experience have higher success rates and reduced need for subsequent ABG.13,14 One explanation for this finding could be selection criteria. Those with stricter criteria may have fewer patients requiring secondary procedures. Another possible explanation is variability in different surgeons’ definition of GPP. For example, a direct approach utilizes GPP dissection limited to the tissue within the cleft and creates an oral, nasal and labial bridge for the periosteal tunnel with readily adjacent tissue. This differs from wide dissection along the maxilla to advance mucoperiosteal flaps seen in an indirect approach.20,28 Therefore, two institutions describing GPP, unless defined, may not be discussing the same procedure. As such, patient selection, surgical technique and the operating surgeon are key determinants of the outcome.
There is no consensus on ideal timing of GPP within cleft treatment protocols.12,14,43,44 Most centers perform GPP at the time of cleft lip repair around 3-6 months of age.13,14,34 At this age, alveolar cleft closure is believed to provide optimal access to close the defect at the earliest and safest opportunity. 45 The use of NAM prior to cleft lip repair to decrease the alveolar cleft width makes GPP a feasible approach.4,12,23,25 GPP has also been reported at the time of cleft palate repair.12,42,45 In nearly all circumstances, the cleft lip repair precedes palatoplasty by several months. The cheiloplasty coupled with nasal floor closure in children with an alveolar cleft narrows the defect in the alveolus and anterior hard palate allowing for GPP to be performed. 45 In this study, patients who had GPP at the time of cleft palate repair were more likely to be recommended for ABG compared to those who had it at cleft lip repair (P = .022). This finding is contrary to that of Losquadro et al. who reported superior results following GPP at palatoplasty “with secondary alveolar bone grafting being unnecessary” in their patient population. 12 Currently, there are no large studies comparing outcomes of GPP done at the time of cleft lip repair versus cleft palate repair.
In this study, 78% of patients with CLP who underwent GPP did not forego the need for ABG. Sato et al. reported increased mesial and distal crest height in children with initially insufficient bone stock following GPP who eventually underwent SABG. They noted that the smaller residual alveolar bone defects in these children appear to allow for secondary bone graft survival with decreased chances of infection, especially in the absence of fistulae. 8 In our patient population, residual nasolabial fistulae was noted in only 10 patients (15.6%), similar to the low rates of residual fistulae reported by Grayson et al. 34 Although GPP may not preclude bone grafting, one goal of GPP could be to increase the success of bone grafting, as often there is bone formation at the occlusal level and a closed nasoalveolar fistula at the time of ABG. Whether or not there is higher success of ABG in those patients who underwent GPP compared to those who did not and if this outweighs the risk of maxillary growth restriction is a question still in need of an answer at our institution. When this patient cohort reaches an age of skeletal maturity, a follow up study will be performed.
The success of GPP should be weighed against the success of ABG when considering it as a part of the comprehensive cleft paradigm. ABG for the treatment of alveolar clefts has a reported success rate of over 90% and is considered the treatment of choice at most cleft centers.14,24,32,33 Additionally, although most centers, including ours, perform late secondary alveolar bone grafting (8-12 years of age prior to the eruption of permanent canines), some suggest that early secondary alveolar bone grafting (4-7 years of age before the eruption of lateral incisors) may provide better residual bone volume outcomes at the cleft site.5,7,31,46,47 In 2014, Pepper et al. evaluated symptomatic oronasal fistula rates before and after SABG. The percent of patients experiencing symptoms related to the fistula dropped from 45% to 10% after ABG. There was no statistically significant difference in these rates between patients who underwent early versus late ABG. 48 For those advocating for earlier intervention, early secondary bone grafting may be an alternative to GPP with similar goals. However, this is beyond the scope of this paper.
This study has several shortcomings including being a retrospective review of a small cohort without comparative groups. Given that the success of GPP is inversely related to cleft width, the lack of inclusion of width in this study represents another significant limitation. Additionally, our institution, like most cleft centers, does not have a systematic method to assess graft success. 49 We utilize experienced cleft surgeons and craniofacial orthodontists who make recommendations for ABG after review of x-rays rather than cone beam computed tomography imaging. Given the results of a recent study by Briss et al. discussing Standardized Way to Assess Grafts (SWAG) ratings compared to 3D imaging, utilizing SWAG for group comparisons may have aided in comparing our results to other institutions and is a step we are considering moving forward. 50 However, for individual treatment planning, SWAG alone does not predict treatment recommendations and it is the treatment of these patients we are most concerned about. Nonetheless, the strength of this study lies in its reporting of GPP at the time of cleft lip repair and palatoplasty and outcomes of five surgical providers.
Conclusion
Gingivoperiosteoplasty does not preclude the need for ABG. 78% of our patients with cleft lip and palate who were initially treated with GPP were recommended for ABG. Those who had GPP at a younger age (P = .004) and at the time of initial cleft lip repair (P = .022) were less likely to be recommended for ABG. Patients with complete clefts were more likely to be recommended for ABG compared to patients with cleft lip and alveolus only (P = .015). Additionally, patient selection and the surgical provider are key determinants of the outcome given the complexity of GPP. A follow up study on this population, looking at success of ABG following GPP compared to ABG alone and effects of GPP on maxillary growth restriction will be conducted at skeletal maturity to determine if GPP is a worthwhile adjunct to ABG in cleft care.
Footnotes
Acknowledgements
Stephanie Radu M.D., M.S., Zbigniew Sikora B.S. The work contained in this manuscript was presented at Plastic Surgery The Meeting in Boston, MA, October 2022.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.