
Abstract
Objective
Disparities in insurance and socioeconomic status (SES) may impact surgical management and subsequent postoperative outcomes for patients with craniosynostosis. This systematic review summarizes the evidence on possible differences in surgical care, including procedure type, age at surgery, and differences in surgical outcomes such as complications, length of hospital stay, and child development based on SES.
Design
The databases Scopus, PubMed, and CINAHL were searched between May and July 2022. Following PICO criteria, studies included focused on patients diagnosed with craniosynostosis; corrective surgery for craniosynostosis; comparison of insurance, income, or zip code; and surgical management of postoperative outcomes.
Results
The initial search yielded 724 articles. After three stages of screening, 13 studies were included. Assessed outcomes included: type of procedure (6 articles), age at time of surgery (3 articles), post-operative complications (3 articles), referral delay (2 articles), length of stay (2 articles), hospital costs (2 articles), and child development (1 article). Of the studies with significant results, insurance type was the main SES variable of comparison. While some findings were mixed, these studies indicated that patients with public medical insurance were more likely to experience a delay in referral, undergo an open rather than minimally-invasive procedure, and have more complications, longer hospitalization, and higher medical charges.
Conclusions
This study demonstrated that SES may be associated with several differences in the management of patients with craniosynostosis. Further investigation into the impact of SES on the management of patients with craniosynostosis is warranted to identify possible interventions that may improve overall care.
Introduction
Craniosynostosis, the premature fusion of one or more cranial sutures, 1 is a common congenital condition with a global incidence of 5.2 per 10,000 live births. 2 The condition often results in aesthetic deformity of the cranium and can impair normal brain growth and cognitive development. Traditional management is surgical intervention, and the age at diagnosis and treatment may affect the choice of procedure used. Patients who are age 6 months or less at the time of treatment can be successfully managed using minimally invasive options, such as endoscopically-assisted strip craniectomy (SC) or spring-mediated distraction. These techniques utilize small incisions and limited dissection, with very low morbidity. 1 Conversely, patients who are older than 6 months at the time of surgery typically undergo open cranial vault remodeling (CVR), a more invasive procedure that requires a large open dissection and has significantly higher morbidity, cost, and hospital stay.1,3–6 Despite the dramatic differences in morbidity and cost between these two procedure types, the morphological and neurocognitive outcomes are virtually indistinguishable, and, in some aspects, SC provides better outcomes.7–9
Because early diagnosis, referral, and intervention have a major effect on the options available to families, the nature of the care a child with craniosynostosis may receive, and the overall cost of care, steps should be taken to identify and reduce the impact of these barriers. One factor that may affect the care received by patients with craniosynostosis is their socioeconomic status (SES). The American Psychological Association defines SES as factors that contribute to social status or class, including but not limited to income, insurance, occupation, and education. 10 SES factors are known to correlate with healthcare quality and accessibility, with individuals with lower SES experiencing lower quality of medical care and poor accessibility compared to those with higher SES. 11 Understanding the influence SES has on craniosynostosis care may be an important first step in addressing potential inequities and optimizing patient care.
Despite a recent surge of interest in comprehending socioeconomic inequalities in relation to craniosynostosis management, there is a paucity of comprehensive, systematic summaries of potential disparities in treatment. This review aims to evaluate existing literature to assess SES influences in surgical care, including type of procedure, age at surgery, surgical outcomes, complications, length of hospitalization, and child development. We sought to identify potential gaps in the care of craniosynostosis patients.
Methods
Search Methods
A review of the literature was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The primary outcome of interest was craniosynostosis management and surgical outcomes compared across socioeconomic statuses. Pubmed, Scopus, and CINAHL online databases were queried for all articles with the following Medical Subject Heading terms: (Craniosynostosis) AND ((socioeconomic) OR (insurance) OR (zip AND code) OR (disparity) OR (access) OR (access) OR (outcome) OR (quality of life). This systematic review does not involve human subjects, thus it was exempt from IRB review.
Selection Criteria
Inclusion criteria were articles published in English, data on craniosynostosis surgical management or outcomes, and SES stratifying variables such as insurance type, household income, or zip code. Excluding criteria were review articles, current clinical trials, commentaries, and abstracts/full-texts not available.
Data Extraction
Eligibility assessment was performed in a standardized manner by three independent reviewers using Covidence. First, the titles and abstracts of all articles were screened by two reviewers, and conflicts were resolved by a third reviewer. Similarly, full-text reviews were conducted by two reviewers, and conflicts were resolved by a third reviewer. From the final studies, the type of study, SES variable measured, and management or surgical outcome were measured, and results were extracted.
Risk of Bias Assessment
Two independent reviewers used a modified Newcastle-Ottawa Scale (NOS) to measure the risk of bias for each study (Supplemental Digital Content 1). 12 This scale scores three different domains: selection, comparability, and outcome. The maximum score of nine stars is associated with the least possible risk of bias. Any discrepancies between the reviewers were resolved by reaching a consensus. Final star scores were converted to qualitative values, with 0 to 4 stars considered a high risk of bias, 5 to 6 stars as a moderate risk of bias, and 7 to 9 stars as a low risk of bias. 13
Results
Study Selection
The initial search yielded 724 results. After excluding duplicates (n = 74), 650 papers remained. From these papers, 608 were excluded based on title and abstract, resulting in full-text retrieval for the remaining 42 papers. A full-text review for inclusion and exclusion criteria removed 28 papers with reasons shown in Figure 1. The remaining 13 papers were included in the data extraction and analyses.
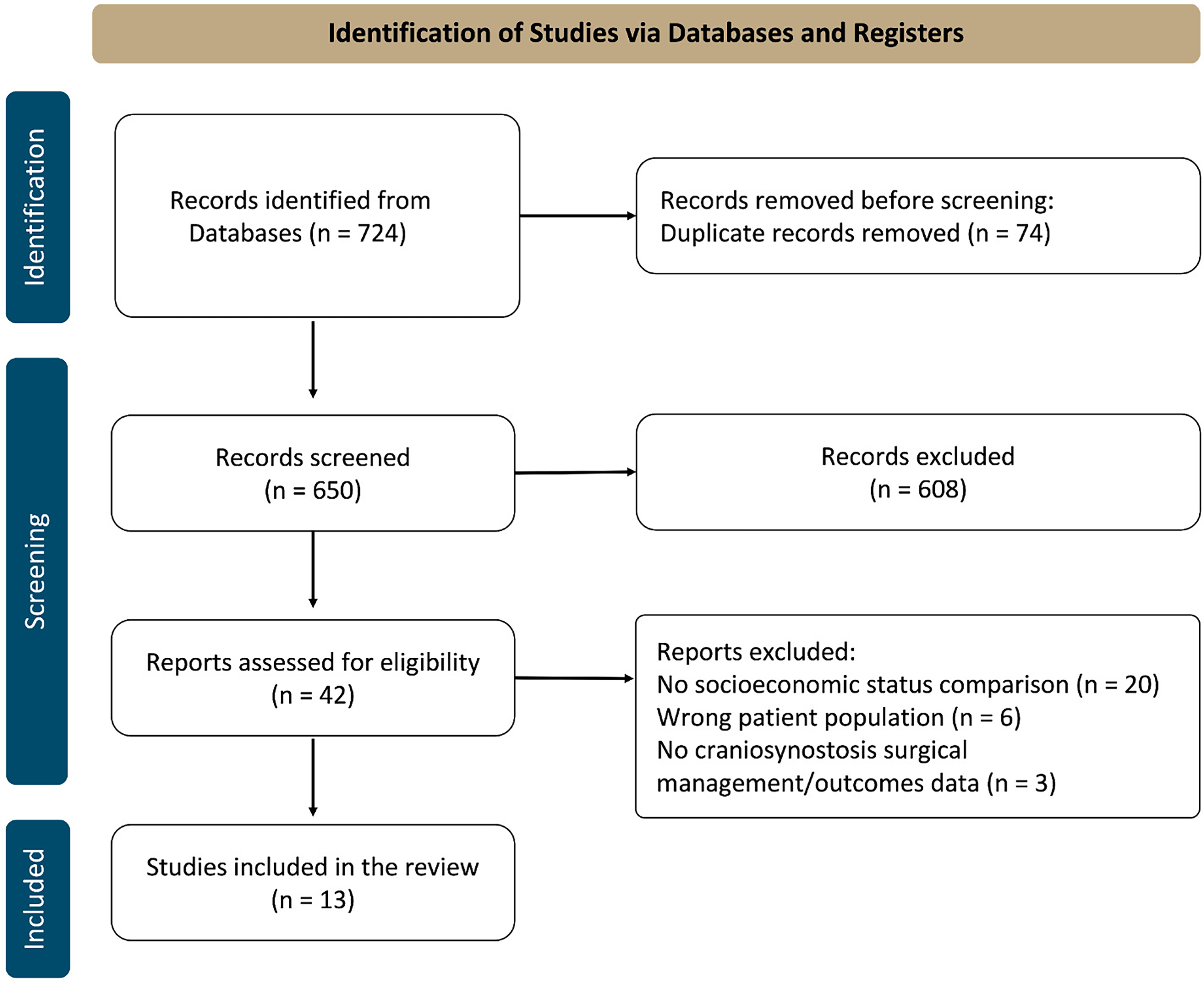
Preferred reporting items for systematic reviews and meta-analyses search methodology. Three independent reviewers screened 724 articles in a standardized manner resulting in 13 studies included in this systematic review.
Study Characteristics
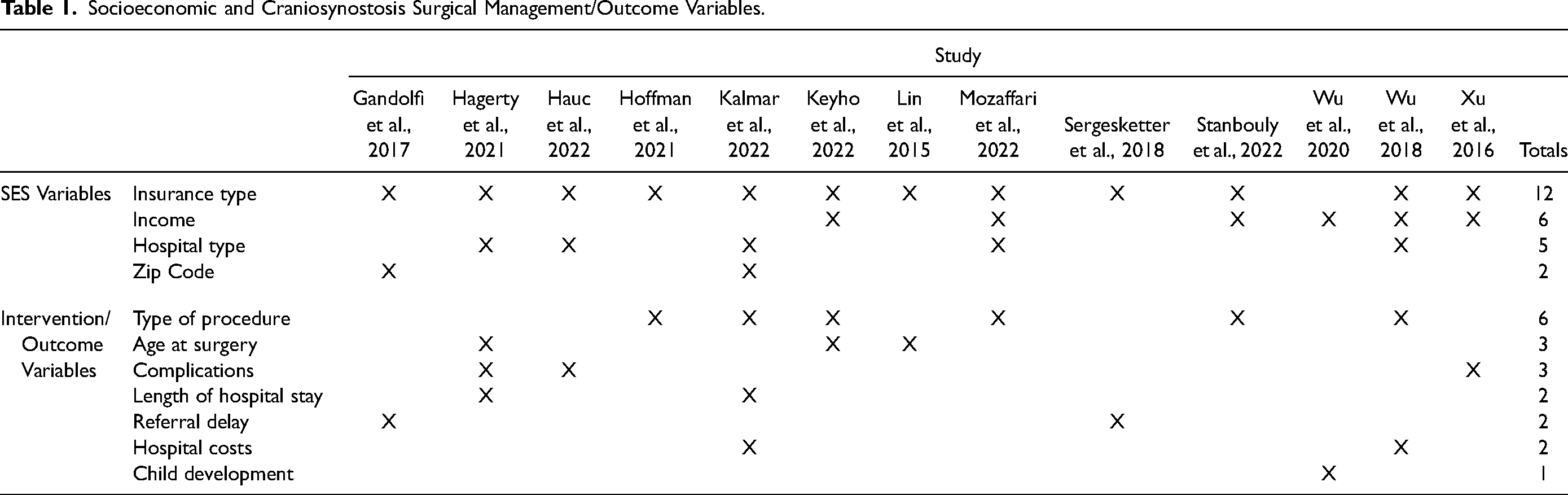
The studies included were published between 2015 and 2022, all from the United States. Among these, twelve were retrospective cohort studies,14–25 and one was prospective. 26 The primary variables measured are detailed in Table 1, were insurance type (N = 12) and type of surgical procedure (N = 6). Detailed results for these variables are presented below and in Table 2. Regarding hospital administration types, Wu et al. (2018) and Hagerty et al. highlighted that a majority (>90%) of the included hospitals were teaching institutions situated in urban areas, while Mozaffari et al. specified that the majority (>90%) of hospitals in their study were non-teaching institutions in urban settings.15,21,24 Hagerty et al. was able to further identify that almost 50% of the analyzed hospitals were children's units in general hospitals, almost 40% were freestanding children's hospitals and the rest were not children's hospitals. 15 Moreover, none of the articles that examined multiple socioeconomic variables investigated the interrelationships among those variables.
Socioeconomic and Craniosynostosis Surgical Management/Outcome Variables.
Summary of Included Studies.
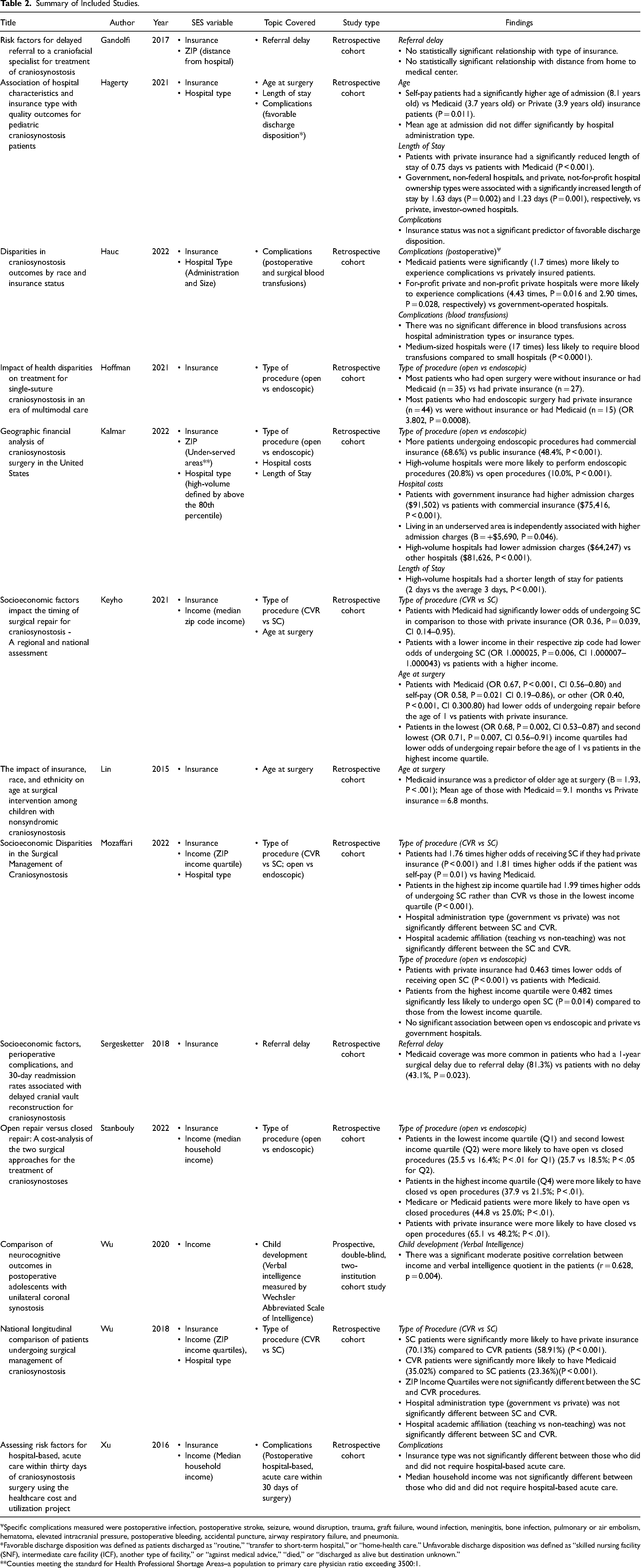
Specific complications measured were postoperative infection, postoperative stroke, seizure, wound disruption, trauma, graft failure, wound infection, meningitis, bone infection, pulmonary or air embolism, hematoma, elevated intracranial pressure, postoperative bleeding, accidental puncture, airway respiratory failure, and pneumonia.
*Favorable discharge disposition was defined as patients discharged as “routine,” “transfer to short-term hospital,” or “home-health care.” Unfavorable discharge disposition was defined as “skilled nursing facility (SNF), intermediate care facility (ICF), another type of facility,” or “against medical advice,” “died,” or “discharged as alive but destination unknown.”
**Counties meeting the standard for Health Professional Shortage Areas–a population to primary care physician ratio exceeding 3500:1.
Type of Procedure
Of the six studies that analyzed the relationship between SES and type of surgical procedure, four compared open and endoscopic procedures.17,18,21,23 Hoffman et al. found a significant association between patients undergoing open procedures having public insurance and association between patients undergoing endoscopic procedures having private insurance. 17 Kalmar and associates also identified more patients undergoing endoscopic procedures had private insurance. 18 Similarly, patients with private insurance had significantly lower odds of receiving open SC rather than endoscopic SC compared to patients with Medicaid, as documented by Mozaffari and colleagues. 21 Stanbouly et al. found that publicly insured patients were significantly more likely to be treated through an open approach whereas privately insured were significantly more likely to be treated endoscopically. 23 Additionally, Mozaffari et al. found that patients from the highest income quartile were significantly less likely to undergo open, compared to those from the lowest income quartile. 21 Stanbouly et al. found that patients in the highest income quartile were more likely to be treated by the endoscopic approach, whereas the lowest two income quartiles were significantly more likely to be treated by the open approach. 23 Furthermore, Mozaffari et al. found no significant association between endoscopic and open procedures when comparing hospital types such as government or privately owned nor when comparing hospital teaching status. 21 Kalmar et al., on the other hand, did find that high-volume hospitals were significantly more likely to perform endoscopic procedures. 18
Three papers specifically compared SC and CVR across different SES.19,21,24 Keyho et al. found that patients with public insurance had lower odds of undergoing SC than those with private insurance. 19 Mozaffari et al. found that patients with private insurance and those who were self-paying had significantly higher odds of undergoing SC compared to patients with public insurance. 21 Wu et al. found that CVR patients were significantly more likely to have public insurance compared to SC patients, and SC patients were significantly more likely to have private insurance compared to CVR patients. 24 Additionally, Keyho et al. found that patients with lower income levels had significantly lower odds of undergoing SC compared to patients with higher incomes. 19 Mozaffari et al. also found that patients with the highest zip income quartile had significantly higher odds of undergoing SC rather than CVR compared to patients with the lowest income quartile. 21 Wu et al. did not find a significant difference between SC and CVR when comparing income quartiles. 24 Similarly, hospital type and hospital teaching status did not significantly influence the choice between SC and CVR.21,24
Age at Surgery
A total of three papers analyzed the relationship between SES and age at the time of surgery.15,19,20 When looking at insurance type, one study by Lin et al. found that public insurance was a statistically significant predictor of older age at surgery, with mean ages of 9.1 months for those with public insurance and 6.8 months for those with private insurance. 20 Keyho et al. found that patients with public insurance and self-pay had significantly lower odds of having surgery before one year of age than private insurance. 19 This paper also found that the patients in the lowest and second lowest income quartiles had significantly lower odds of undergoing repair before the age of 1 than those in the highest income quartile. 19 Hagerty et al. found a significant difference in age across insurance types, with self-pay having the highest age (8.1 years), followed by private insurance (3.9 years), and then public insurance (3.7 years). 15 This study also found that age was not significantly different by hospital type. 15
Complications
Three studies measured post-operative complications or complication-adjacent variables such as hospital-based acute care within 30 days of surgery and favorable discharge disposition.15,16,25 Hagerty et al. defined favorable discharge disposition as patients discharged as “routine,” “transfer to short-term hospital,” or “home-health care,” whereas unfavorable discharge disposition was defined as discharged to “skilled nursing facility (SNF), intermediate care facility (ICF), another type of facility,” “against medical advice,” “died,” or “discharged as alive but destination unknown.” This study found insurance not to be a significant predictor of favorable discharge disposition. 15 Similarly, Xu et al. found no significant difference in insurance type or income between those who required hospital-based acute care within 30 days of surgery and those who did not. 25 Hauc et al. looked at the following postoperative complications: postoperative infection, postoperative stroke, seizure, wound disruption, trauma, graft failure, wound infection, meningitis, bone infection, pulmonary or air embolism, hematoma, elevated intracranial pressure, postoperative bleeding, accidental puncture, airway respiratory failure, and pneumonia. This study did find that patients with public insurance were significantly more likely to experience postoperative complications compared to privately insured patients. 16 This study also found that surgeries at for-profit and non-profit private hospitals were significantly more likely to experience postoperative complications than those at government-operated hospitals. 16 Huac et al. additionally measured the surgical complications of blood transfusions. They found that patients at medium-sized hospitals, compared to small hospitals, were significantly less likely to require blood transfusions during the procedure. However, there was no significant difference in transfusion rates across hospital administration types or insurance types. 16
Referral Delay
Two studies looked at the relationship between SES and referral delay.14,22 Gandolfi et al., defined referral delays by the age at time of referral whereas Sergesketter et al. defined delays by age at surgical intervention as being greater than 12 months of age.14,22 Sergesketter et al. found that public insurance was significantly more common in patients with a one-year surgical delay due to referral delay. 22 Conversely, Gandolfi et al. found no significant relationship between type of insurance or ZIP (distance from hospital) and referral delay. 14 Beyond socioeconomic factors, both articles identified a significant association between delayed referral or intervention and patients belonging to a racial/ethnic minority group. Sergesketter et al. additionally found delays associated with having a primary language other than English, and Gandolfi et al. associated delays with patients who underwent radiographic imaging before referral.14,22 Furthermore, Gandolfi et al. established a connection between early referrals and pediatricians as the referring provider in contrast to other medical providers. 14
Length of Hospital Stay
Two studies analyzed the association between the length of hospital stay following surgery with SES.15,18 Hagerty et al. found that patients with private insurance had a significantly reduced length of stay compared to those with public insurance. 15 This study also found that non-federal government hospitals and not-for-profit private hospitals were associated with a significant increase in the length of stay compared to investor-owned private hospitals. 15 Another study by Kalmar et al. found that high-volume hospitals had significantly shorter lengths of stay. 18
Hospital Costs
Two studies analyzed the association between SES and hospital costs for craniosynostosis surgery.18,24 Kalmar et al. found that patients with government insurance had significantly higher admission charges than patients with commercial insurance. Also, living in an underserved area was significantly associated with higher admission charges. This paper additionally found that high-volume hospitals had significantly lower admission charges than other hospitals. Wu et al., however, found no significant association between hospital costs and insurance type or income.
Child Development
One study analyzed the relationship between SES and child verbal intelligence using the Wechsler Abbreviated Scale of Intelligence. 26 This paper by Wu et al. (2020) found a significant moderate positive correlation between household income and verbal intelligence quotient in the patients (r = 0.628, p = 0.004). 26
Risk of Bias Assessment
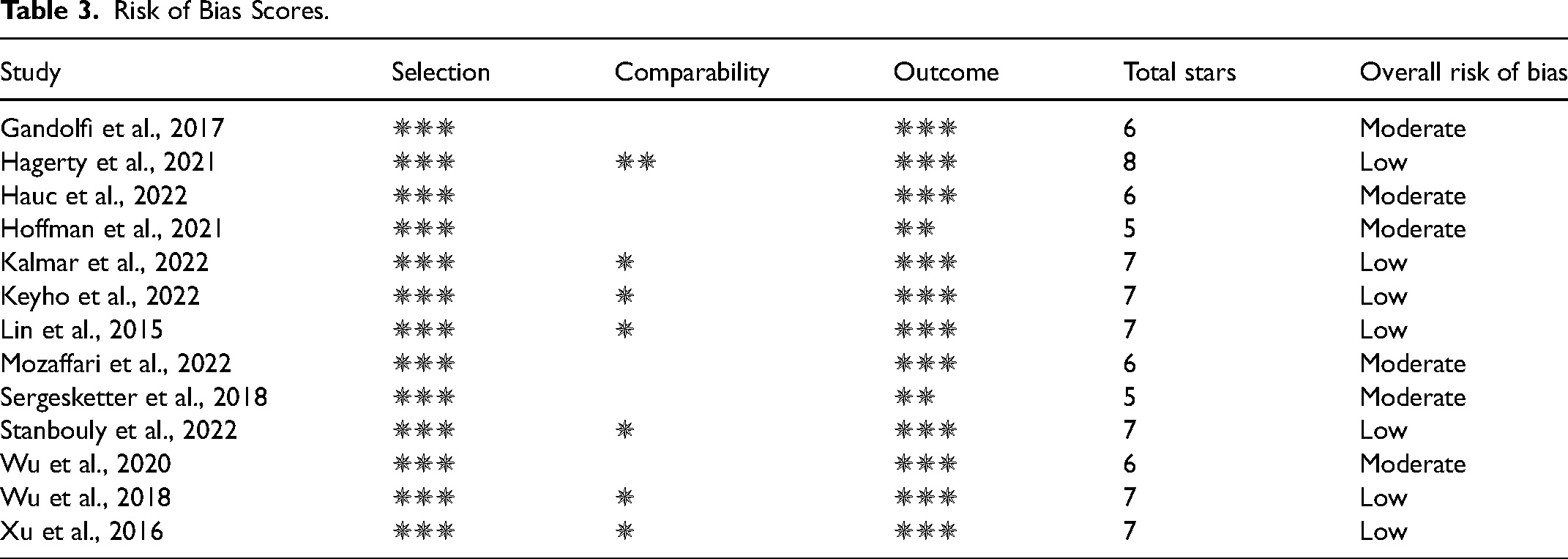
Risk of bias scores were recorded in Table 3. The majority of studies scored at least three out of four stars for the selection domain, with most stars lost due to the retrospective nature of studies, causing the outcome of the study to be present at the start of the study. The scores for the compatibility domain ranged from 0–2 stars. Stars in this section were lost when papers did not account for pre-defined confounding variables described in Supplemental Digital Content 2. For the outcome domain, most papers scored three out of three stars. The papers that scored fewer stars in this domain were often due to the exclusion of participants, introducing possible bias. When converting these scores to qualitative values, seven studies were low risk of bias and six were moderate risk of bias.
Risk of Bias Scores.
Discussion
In this systematic review, we examined recent literature on SES and its relationship to surgical management, procedure types, age at surgery, and postoperative outcomes (complications, hospital stay length, child development)–for patients with craniosynostosis. While many studies have focused on SES and race in relation to craniosynostosis outcomes,16,20,27 far fewer studies have focused on other indicators of SES. However, the complex interplay between race and SES variables leads to disparities; therefore, the goal of our systematic review was to obtain a holistic picture of SES to better understand trends in surgical outcomes.
SES Proxy Variables
This systematic review investigated the proxies used by existing studies to measure SES, which included insurance type, hospital type, income, and zip code. We found the proxy most often used was insurance type, which we deemed to be an appropriate area of focus due to its ties with household income. Those with public or government insurance must be below a state income threshold in order to qualify for coverage, thus falling into the low SES category, whereas those with private insurance are considered of a higher SES. Hospital type was also measured by several studies due to the range of publicly funded versus privately funded institutions. Resources allocated to hospitals depend on available funding, which may limit patient options. Larger hospitals and hospitals with private funding were associated with a higher SES, while smaller and publicly funded hospitals were considered associated with lower SES. Both household income and zip-code income quartiles fell under the income variable. Household income and zip code income quartiles are important measures as they directly relate to the patient's SES. The studies that analyzed access to care based on patient distance from the hospital and county patient-to-physician ratio were combined in the zip-code variable. Patients located in areas with greater access to health care are associated with higher SES. 11 These variables ultimately act as proxies for SES when comparing outcomes across different studies.
Craniosynostosis Management and Outcome Trends
The management and outcome variables measured by the included studies are crucial for identifying socioeconomic-based differences in care. Among the management variables examined in three or more papers, similarities were observed in procedure type and age at surgery. Higher SES was associated with endoscopic surgeries and SC, while lower SES was linked to open procedures and CVR.17–19,21,23,24 These similarities were expected, as SC is typically performed endoscopically, while CVR involves an open procedure. 1 Age can potentially explain the differences in the procedures received by different SES groups. The optimal age for SC and CVR varies due to the risks associated with anesthesia exposure at different ages: SC procedures are commonly performed at 3–6 months, while CVR is typically performed later, between 6–12 months of age. 1 We found that patients with lower SES underwent surgery later, while those with higher SES had surgery at younger ages.19,20 Low SES patients who are older at the time of surgery will ultimately be managed with an open procedure. Hoffman et al. were able to draw this association between procedure type and age as they found patients undergoing open procedures, in addition to having lower SES, were older at presentation and older at the time of surgery compared to the patients undergoing minimally invasive procedures. 17 Thus, providing plausible causality that patients of lower SES may be missing the timeframe for minimally invasive treatment. One factor that may result in a later age of surgery, measured in two studies, was referral delay. However, none of the studies analyzing procedure type investigated referral times, and of the studies that did analyze referral delays there was a lack of consensus in the results. Later age of surgery can be impacted by many other factors, such as socio-demographic barriers to care, and warrants further investigation.
Furthermore, outcome variables such as complications, length of hospital stay, hospital costs, and child development are influenced by age and type of surgery. Although no SES trends were noted for these outcome variables due to lack of consensus or insufficient data, one can expect poorer outcomes for those with lower SES because the child will likely be of an older age at the time of surgery. Older age at time of surgery is associated with restraint-related brain injury and adverse neurocognitive outcomes. 28 Delaying craniosynostosis surgery, regardless of the procedure type, can result in increased complications, prolonged hospital stays, and healthcare costs. 29 These older patients also miss the time window to receive the endoscopic procedures that are associated with less operative risk and minimal postoperative morbidity compared to the open CVR procedures.7–9,29 Additionally, endoscopic craniosynostosis repair has been found to be a more cost-effective option when compared to the open,4–6 which brings up the concern that patients of low SES may be experiencing further economic burden as a result of craniosynostosis care when compared to their higher SES counterparts. In addition to surgical expenses, it is essential to consider the accessibility and costs associated with helmet therapy as well as insurance coverage of these treatment options, aspects overlooked in the studies under review. While earlier research has suggested that the combined expenses of endoscopic craniectomy and helmet therapy, encompassing hospital charges, professional and helmet fees, and clinic visits, were lower compared to those of CVR, there exists a gap in the literature regarding the varying insurance coverage for helmet therapy. 4 Moreover, the lack of assessment of billing data in current studies restricts our understanding of whether higher reimbursement payers might incentivize the utilization of more costly open procedures, highlighting the necessity for further investigation in this field. Despite the limited results on the direct relationship between SES and outcome variables, potential health disparities in these variables may exist, emphasizing the need for future studies to prioritize their investigation.
Limitations
Our systematic review revealed trends, but no associations due to a lack of studies and underwhelming data. There currently lacks a standardized method to measure SES as different variables are used across studies as proxies for SES. A particular variable that warrants further standardization and exploration is referral delay in relation to SES. While the current studies evaluated delays primarily based on the age at referral and the age at the time of surgery, a more comprehensive approach could involve examining the duration between the initial diagnosis and the age at the time of surgery. This approach could offer richer data for identifying patients requiring closer monitoring during the referral process. Another variable that could be further analyzed is the billing of open and minimally invasive procedures by different insurance companies to better understand if higher reimbursement payers create incentives for larger billed procedures such as CVR. Additionally, by primarily focusing on SES variables, our study does not investigate other variables that potentially contribute to health inequities, such as the primary language spoken, limitations in transportation, work flexibility, and mistrust in the medical system. Furthermore, our risk of bias assessment revealed numerous publications to have a moderate risk of bias. Papers with a moderate bias score fell short in the comparability category due to a lack of study controls. Ultimately, more robust variables and further investigations into the relationship between SES, craniosynostosis management, and outcomes are indicated.
Future Directions
In addition to improving data quality to better understand care disparities, interventions that improve patient care can be enacted in the interim to help mitigate possible inequities. As proposed by Hagerty et al., financial incentives such as the Delivery System Payment Reform Incentive Payment Program (DSRIP), implemented in California 2010, have exhibited notable improvements in care quality, patient outcomes, and healthcare expenditure reductions.15,30 Establishing financial incentives, whether through private investment or government funding, could aid in the early identification and intervention of patients with craniosynostosis. Furthermore, the implementation of tailored Enhanced Recovery After Surgery (ERAS) protocols for craniosynostosis repair has been shown to reduce hospitalization duration and costs, presenting an avenue for enhanced care across all patient demographics. 31 Overall, initiatives aimed at earlier identification of patients with craniosynostosis and efforts to enhance the overall quality of care can enhance management for all affected patients, while we continue to identify specific factors contributing to care disparities.
Conclusion
The findings of this systematic review indicate a potential association between SES and various aspects of craniosynostosis management. Of note, there was consensus among several studies that patients of higher SES were associated with SC or endoscopic procedures and younger age at surgery, while patients of lower SES were associated with CVR or open procedures and older age at surgery. However, the available literature on SES's impact on referral delay, complications, length of hospital stay, hospital costs, and child development is limited and lacks consensus. There is also a lack of exploration of other impactful variables relating to primary language, transport, work flexibility, and patient trust/mistrust in the healthcare field. These findings underscore the importance of further research to gain a comprehensive understanding of the impact of SES on the management and outcomes of individuals with craniosynostosis.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241261838 - Supplemental material for Socioeconomic Influence on Surgical Management and Outcomes in Patients with Craniosynostosis - A Systematic Review
Supplemental material, sj-docx-1-cpc-10.1177_10556656241261838 for Socioeconomic Influence on Surgical Management and Outcomes in Patients with Craniosynostosis - A Systematic Review by Melanie Bakovic, Lilliana Starsiak, Spencer Bennett, Ryan McCaffrey, Esperanza Mantilla-Rivas, Monica Manrique, Gary F Rogers and Albert K Oh in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656241261838 - Supplemental material for Socioeconomic Influence on Surgical Management and Outcomes in Patients with Craniosynostosis - A Systematic Review
Supplemental material, sj-docx-2-cpc-10.1177_10556656241261838 for Socioeconomic Influence on Surgical Management and Outcomes in Patients with Craniosynostosis - A Systematic Review by Melanie Bakovic, Lilliana Starsiak, Spencer Bennett, Ryan McCaffrey, Esperanza Mantilla-Rivas, Monica Manrique, Gary F Rogers and Albert K Oh in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Compliance and Informed Consent Disclosure
This systematic review does not involve direct participation of patients, human samples, or study participants. Consequently, obtaining individual informed consent from patients is not applicable in this context. As the study solely relies on the analysis of existing literature and data, and there is no involvement of personal identifiers, the need for informed consent is waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Presentation
The work contained in this manuscript was presented at the International Society of Craniofacial Surgery (ISCFS), 20th Congress, Poster presentation. September 2023. Seattle, WA. As well as at the George Washington University Medical Student Research Day, Poster presentation. April 2023. Washington, DC.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.