
Abstract
Objective
To examine ear and hearing clinical practices across American Cleft Palate-Craniofacial Association (ACPA) approved teams in the United States.
Design
Multi-site prospective, observational, longitudinal study.
Setting
Seventeen Cleft Palate Teams in the United States.
Patients, Participants
Children with cleft palate, with or without cleft lip (CP ± L), born between 2015 and 2022, evaluated by 18 months (n = 1246).
Interventions
None.
Main Outcome Measure(s)
Standard of care otolaryngology and audiology appointments evaluated in the context of whether otolaryngology and audiology services were provided as embedded care within the team visit or as ancillary services.
Results
Over 71% of infants passed newborn hearing screening (NBHS). By age 18 months, only 40% of infants received audiologic follow-up while 93.6% of children received otolaryngology care. Follow-up was significantly better for infants served by teams with embedded providers versus those who refer families for ancillary services; the odds of seeing an audiologist by 18 months were three times as high among participants seen by teams with embedded audiology (OR = 3.25; CI = 2.0, 5.2) while those seen by teams with embedded otolaryngologists had more than double the odds of seeing an otolaryngologist by 18 months (OR = 2.2; CI = 1.5, 3.2).
Conclusions
There is considerable variability across ACPA-approved centers in the US regarding the timing and completion of otolaryngology and audiologic follow-up for children with CP ± L. This study highlights the importance of following established standards of care and the impact that team composition and access to clinical services can have on equity of care.
Introduction
In the United States, the Centers for Disease Control and Prevention and the American Cleft Palate Craniofacial Association (ACPA) estimates 1/700 babies are born with cleft palate, with or without cleft lip (henceforth, CP ± L). In addition to the well-documented feeding and speech challenges, young children with CP ± L are at an increased risk for ear and hearing problems.1–3 This is largely attributed to eustachian tube dysfunction and otitis media with effusion (OME), an accumulation of serous or mucoid fluid in the middle-ear space. The incidence of OME in young children with CP ± L is upwards of 90%,1,4 and often presents within the first few months of life.2,4–7 Moreover, OME is far more common in children with CP ± L and persists far longer than in children without clefts.2,5–7
Eustachian tube dysfunction and OME can cause conductive hearing loss (CHL), which can be fluctuating or persistent, vary in severity, and be accompanied by infection or otalgia.8–11 Difficulty hearing can deleteriously impact speech and language development in children with clefts, a group already at increased risk for delays.12–14 The implications of OME are both immediate and long-term, affecting auditory processing, speech and language, cognitive development, and overall quality of life.15–18 Furthermore, children with syndromic diagnoses or other medically complex comorbidities, such as those with Stickler syndrome19–21 or Treacher Collins syndrome, 22 which are known to impact auditory structures and function, are at even greater risk of hearing loss.23,24 Placement of ventilation tubes prior to or at the time of palatoplasty has been shown to relieve OME and hearing loss in young children with CP ± L directly after tube surgery,25,26 yet some children have a greater prevalence of OME and CHL than typically developing peers until 5 years of age, indicating long-term outcomes can be more variable.2,5 Persistent middle ear dysfunction and/or OME despite patent ventilation tubes, and persistent hearing loss post-surgery suggests that early ventilation tube placement may not be sufficient to fully resolve auditory issues, or can be indicative of a more complicated etiology for hearing loss.1,2,5–7,27,28
Hearing evaluations and routine follow-up are critical for the timely and effective management of OME and other hearing-related issues29,30 and can lead to better long-term speech and language outcomes in children with CP ± L.12,31 Leading organizations, including ACPA, the Joint Committee on Infant Hearing, the American Academy of Audiology, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS), and the American Speech-Language-Hearing Association, have established clinical practice guidelines for ear and hearing care for children with CP ± L from birth through early childhood. Collectively these guidelines emphasize early evaluation, diagnosis, and monitoring of cleft-related ear conditions and hearing loss, with prompt referrals to specialists to optimize a child's hearing and communication.32–35
Routine ear and hearing care for all newborns with CP ± L in the United States includes several key steps within the first year of life and consistent follow-up until 5 years of age (Figure 1). All infants should have a hearing screening within the first month of life. If a child does not pass the newborn hearing screening for one or both ears, a diagnostic audiological evaluation via natural sleep auditory brainstem response is advised by 3 months of age. In cases where CHL is identified and remains unresolved by 6 months, the guidelines suggest considering amplification and referral to early intervention services to support speech and language development. Regardless of initial hearing results, all children with CP ± L should have an initial behavioral audiologic evaluation by 9 months of age. 32 Routine hearing evaluations are recommended every 6 to 12 months until the age of 5 years to monitor hearing status and speech development. Ear examinations by an otolaryngologist and management of OME throughout this period are crucial to address middle ear conditions and to prevent long-term complications.
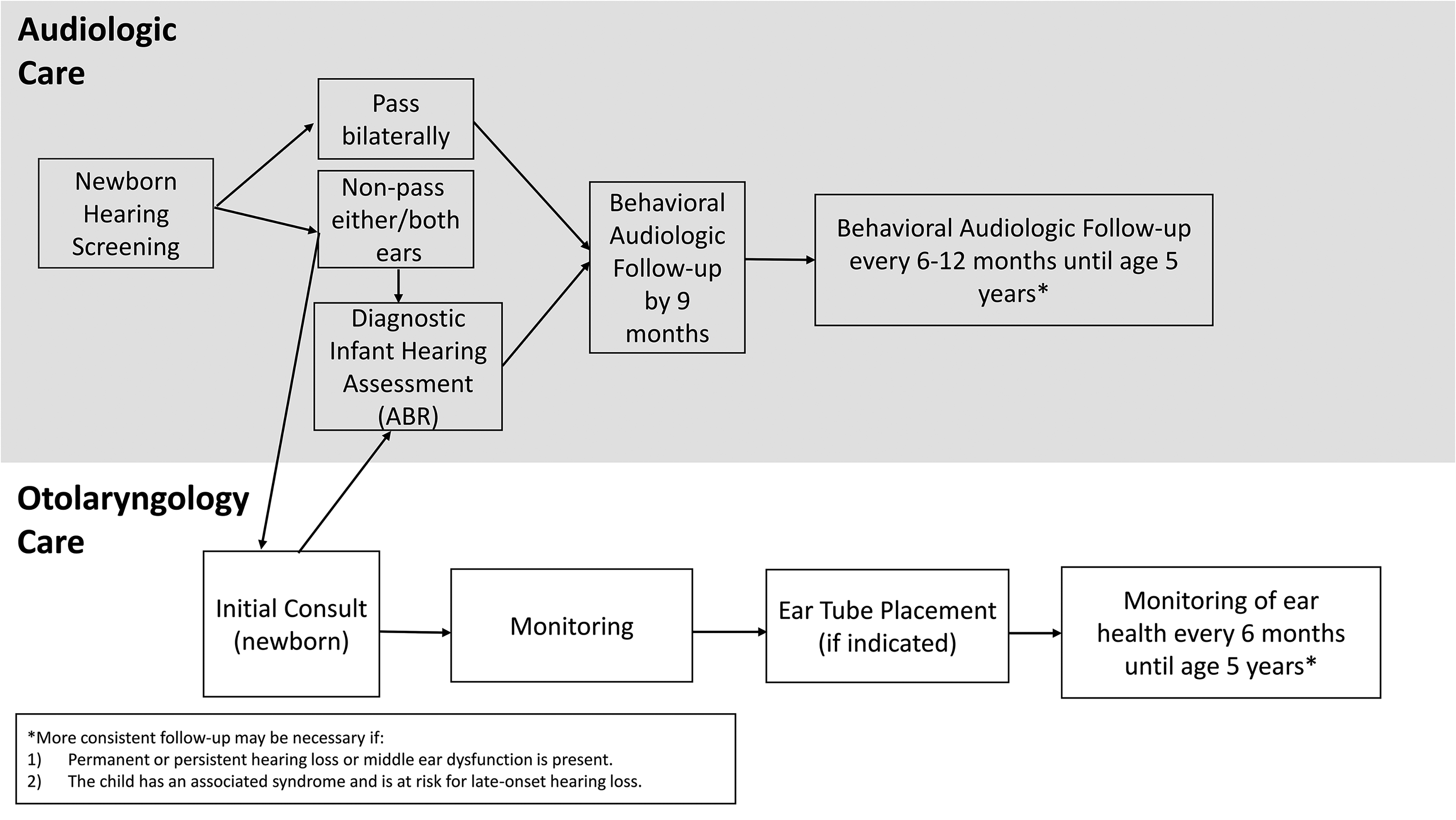
Recommended audiologic and otolaryngology care for children with CP ± L, based on synthesized guidelines from the American cleft palate craniofacial association, 34 joint committee on infant hearing, 32 the American academy of audiology, 36 and the American academy of otolaryngology-head & neck surgery. 35
Despite evidence-based guidelines and state regulations, there is well-documented variability in follow-up care for infants who do not pass the newborn hearing screening.37,38 Mahal et al. (2024) examined annual early hearing detection and intervention data reported between 2007 and 2016 from the Centers for Disease Control and found that although screening of infants across this time range was completed at a high rate of 98%, diagnostic evaluation was completed for only 55%, with a range across states from 1 to 100%. 37 Children with CP ± L are known to refer newborn hearing screening at a higher rate than infants born without medical conditions. Overall, the referral rate for children with CP ± L has been reported to be approximately 30%, but completed follow-up after newborn hearing screening referring (or non-pass) is largely unknown. 39
To facilitate ear and hearing care for children with CP ± L, ACPA recommends Teams provide access to audiology and otolaryngology services as part of team care 40 ; however, the current extent of this care received by young children with CP ± L in the United States is not well documented. Whittemore et al. (2018) 41 described outpatient otolaryngology service usage at one pediatric tertiary care facility that underscored the frequent use of otolaryngology services in this population; however, audiology services were not fully examined, and variability across centers with different approaches is likely and warrants further investigation. Findlen et al. (2022) found poor audiologic follow-up for a cohort of children with CP ± L at a tertiary pediatric center but also demonstrated the potential to improve adherence to recommended guidelines through formal quality improvement. Specifically for children aged 7-12 months, adherence to the recommended follow-up for audiometric testing significantly increased from 48% to 92%. The other care time points in the study, specifically audiologic follow up at 13-24 months,
25-36 months, 37-48 months, and 49-60 months, did not experience the same improvement in completion rates. 39 One intervention implemented as a part of this study was embedding an audiologist into a cleft feeding clinic for infants to ensure opportunity for hearing testing in the 7-12 month age range.
This study examined ear and hearing clinical practice across seventeen ACPA-approved Cleft Palate Teams in the United States, including the impact of having otolaryngology and audiology providers fully embedded into team visits compared to those providing ancillary care. For the purposes of this study, ancillary care referred to Otolaryngologic and/or Audiologic care provided (a) as a service on a separate day and/or at a separate department (or facility/practice) from the core cleft team evaluation, or (b) when Otolaryngology and/or Audiology services were not consistently available at all cleft team clinics held (eg, services were only available at two of four monthly team clinics). We hypothesized that differences in provider integration impacted the type and timing of ear and hearing care received by children with CP ± L.
Methods
The study was reviewed and approved using a Single Institutional Review Board (SIRB) model with the primary institution as the Institutional Review Board of record (IRB#00105205). Seventeen ACPA-approved Cleft Lip and Palate Teams in the United States collected data by parent report and electronic medical record review at multiple points of standard care as part of a prospective longitudinal study of palatoplasty outcomes. Written informed consent was obtained from a parent or legal guardian of each participant. Children were enrolled prior to palatoplasty and followed until at least age 3 years in the primary study. Data was collected for this observational sub-study through a combination of chart review and parent report at enrollment, palatoplasty, post-surgery, and at 16 months of age. Study data were collected and managed using REDCap electronic data capture tools.42,43 REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources. When possible, data collection coincided with regularly scheduled Team visits, surgery, or other clinic visits at the enrolling site.
For the purposes of this study, data collected between the time of enrollment and at the 16-month study visit (visit window of 14-18 months) were included in the data analysis. Participants enrolled included infants born between 2016 and 2022 served by one of the 17 Cleft Teams between 2018 and 2023. Demographic data recorded included sex, race, ethnicity, rurality, insurance payor, and Veau classification (Veau I- soft palate only, Veau II- soft and hard palate, Veau III- unilateral cleft lip and palate, Veau IV- bilateral cleft lip and palate). Audiologic data collected included newborn hearing screening results, history of hearing problems, and whether audiologic testing was completed by 18 months of age. Otolaryngology data collected included in-clinic consults or evaluations completed by 18 months of age, age at first otolaryngology appointment, and timing of tympanostomy tube placement. As an observational study, no directives were provided for sites to follow a specific protocol; rather, all data reflected the care provided to children enrolled in the study at each site.
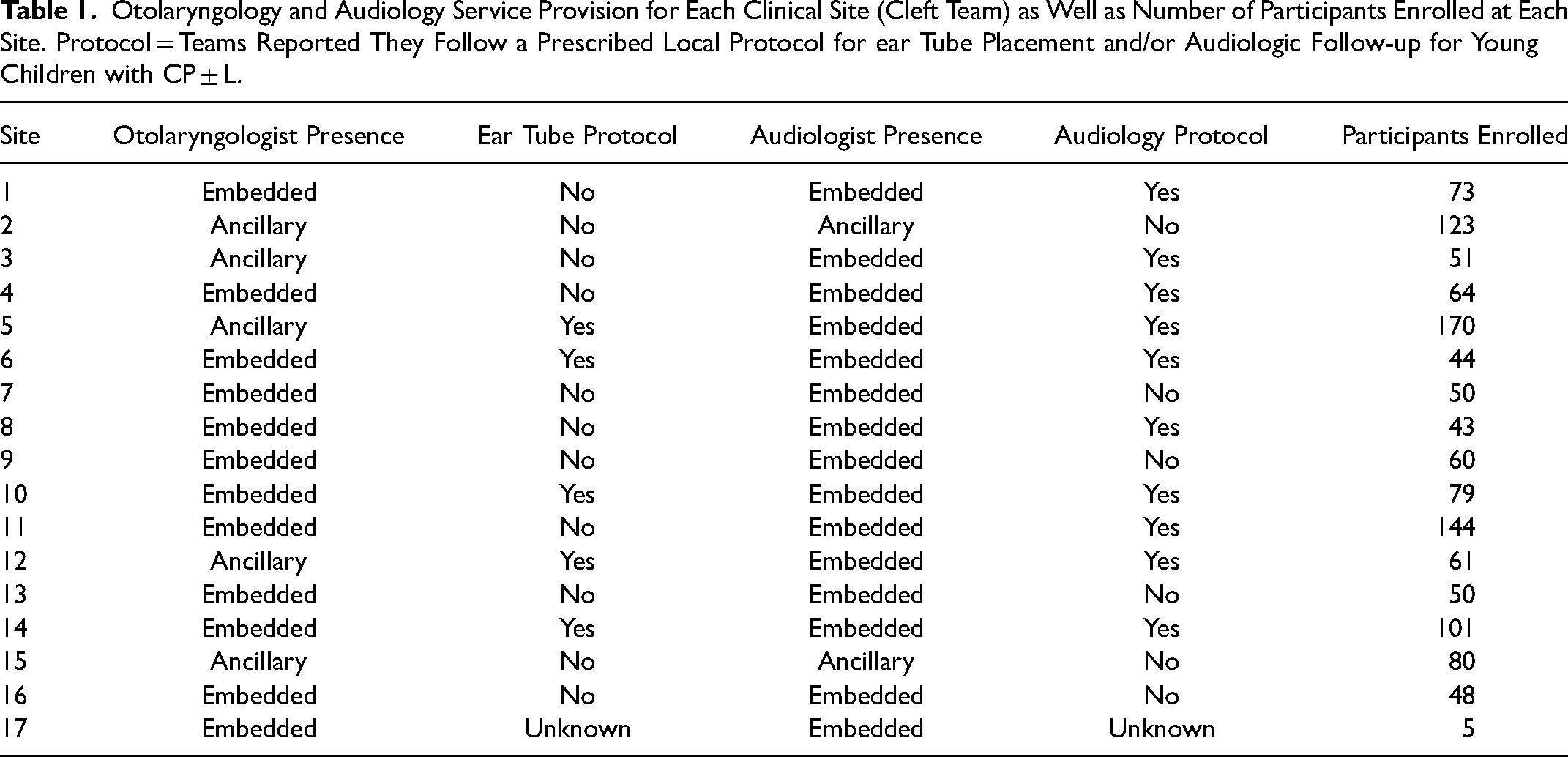
Children enrolled in this study received care from ACPA-approved cleft centers with a variety of team leadership and composition. Most Cleft Team leaders or co-leaders were plastic surgeons (10 sites) while other leaders included a nurse/nurse practitioner, otolaryngologist, pediatric dentist, geneticist, speech-language pathologist, and a pediatrician. Clinical sites were asked to confirm how otolaryngology and audiology services are provided to children with CP ± L during typical Cleft Team appointments at their center. Sites were asked to confirm whether they have an otolaryngologist and/or audiologist present in the clinic during Team visits, or if services were provided ancillary to team appointments by referring patients for outpatient consultations (same day or different day), and whether they follow specific protocols for tympanostomy tube placement timing and ongoing audiologic follow-up at their center. Based on the reported provider involvement, each site's Cleft Team was categorized as either having services embedded in the clinic or as ancillary to team visits. Each service was categorized in this manner based on each site's responses in Table 1.
Otolaryngology and Audiology Service Provision for Each Clinical Site (Cleft Team) as Well as Number of Participants Enrolled at Each Site. Protocol = Teams Reported They Follow a Prescribed Local Protocol for ear Tube Placement and/or Audiologic Follow-up for Young Children with CP ± L.
Data were analyzed using descriptive statistics, Student's t-tests, and logistic regressions to evaluate differences in outcomes across Teams with embedded vs. ancillary services in Microsoft 365 Excel using the Analysis ToolPak (Microsoft Corporation, Redmond, WA) and Stata 14.2 (StataCorp, College Station, TX).
Results
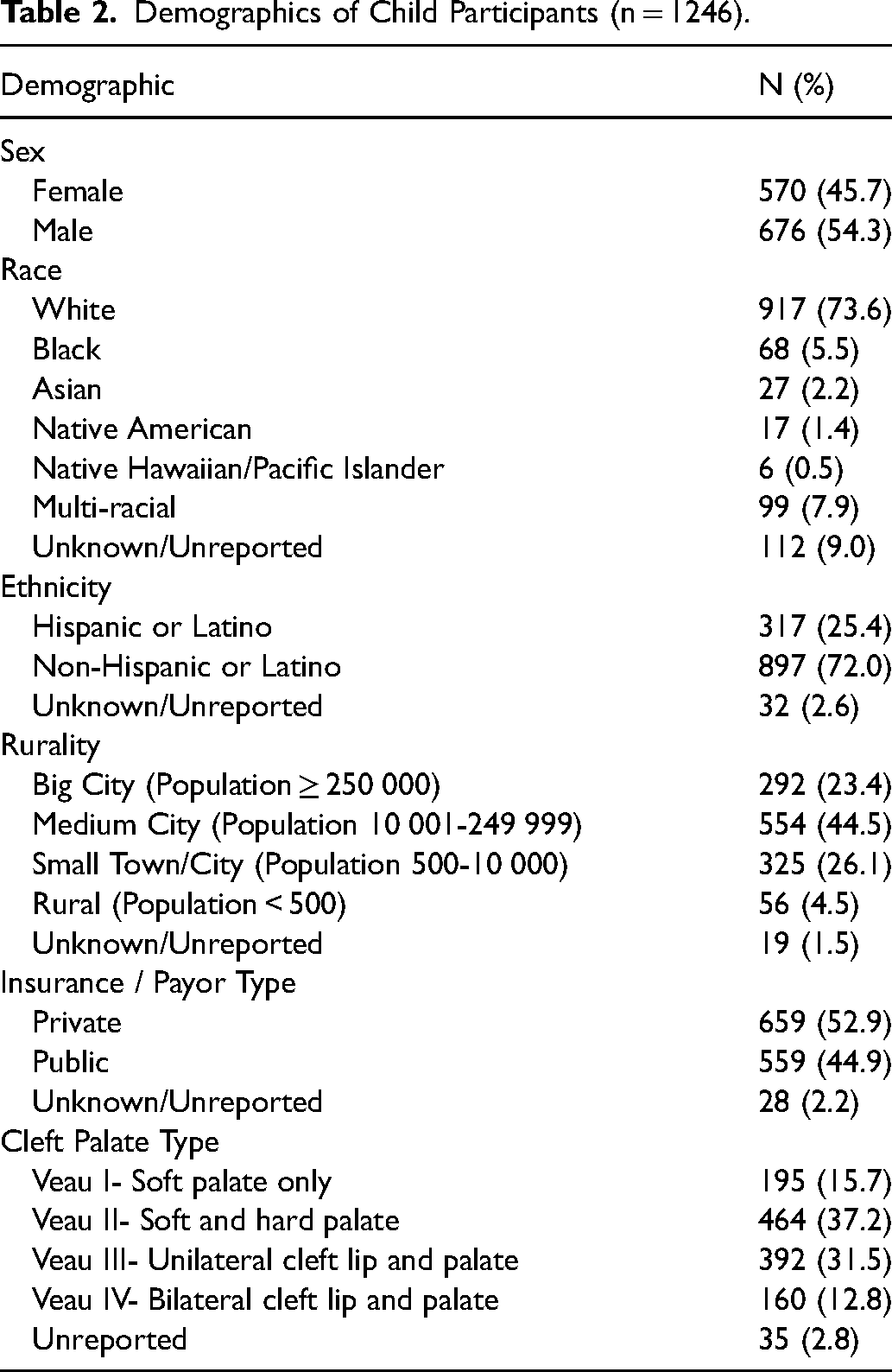
Across the 17 centers, 1246 children with CP ± L were included in this analysis (Table 2). Within this cohort, 892 infants (71.6%) passed their newborn hearing screening (NBHS), 295 (23.7%) infants did not pass, and 59 (4.8%) had missing data or status was unknown. Hearing problems were frequently reported by parents/caregivers, including 849 (68.1%) infants with problems related to CP ± L (eg, CHL due to middle ear effusions) and 89 (7.1%) with additional hearing problems (eg, sensorineural hearing loss associated with a syndrome). The remaining 24.8% (n = 268) of infants had no parent-reported or documented ear or hearing concerns by 18 months of age.
Demographics of Child Participants (n = 1246).
Of those infants who did not pass the NBHS, only 125 (42.4%) had received audiologic follow-up by 18 months of age. Follow-up after referred NBHS was significantly better for sites with audiology embedded into the team visit (45.6%, n = 113) versus sites with ancillary services (26.1%, n = 12); participants at sites with embedded audiologists had odds more than three times as high of receiving audiology follow-up by 18 months as did participants without embedded audiologists (Odds Ratio [OR] 3.25, 95% confidence interval [CI] 2.0-5.2, P < .001; Table 3). For infants who passed the NBHS, 318 (35.7%) had follow-up audiologic evaluation by 16 months of age. Collectively, audiologic follow-up by 18 months of age regardless of NBHS result was40.0% (n = 415) for embedded vs 20.2% (n = 41) for ancillary services(P < .01; Figure 2).
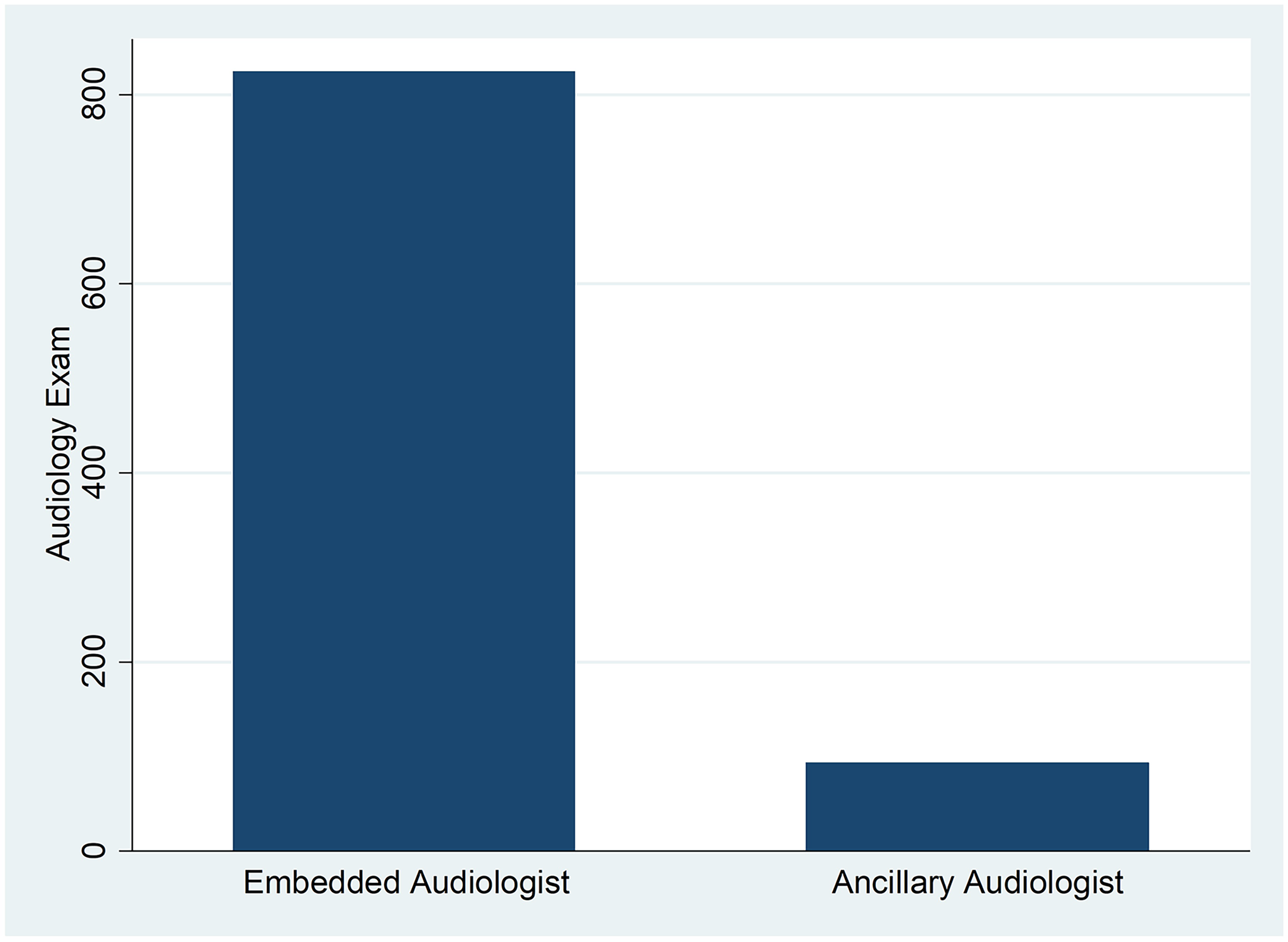
Number of children who completed audiology follow-up by 18 months of age, parsed by embedded or ancillary services. The difference between embedded and ancillary services was statistically significant, P < .001.
Logistic Regression Results.
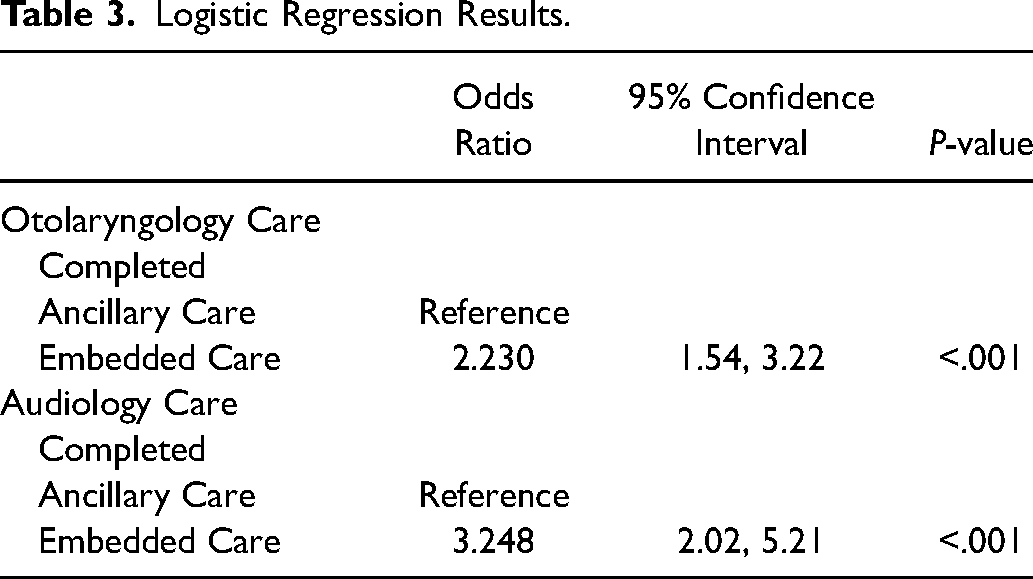
Otolaryngology follow-up was better than audiologic follow-up, with 1114 infants (89.4%) having received otolaryngology care by 18 months of age. These results varied, however, between teams with embedded (92.3%, n = 698) and ancillary (84.7%, n = 411) otolaryngology providers. Those participants seen by teams with embedded otolaryngologists had odds more than twice as high of seeing otolaryngology by 18 months as did children without embedded otolaryngologists (OR 2.23, CI 1.5-3.2, P < .001; Figure 3).
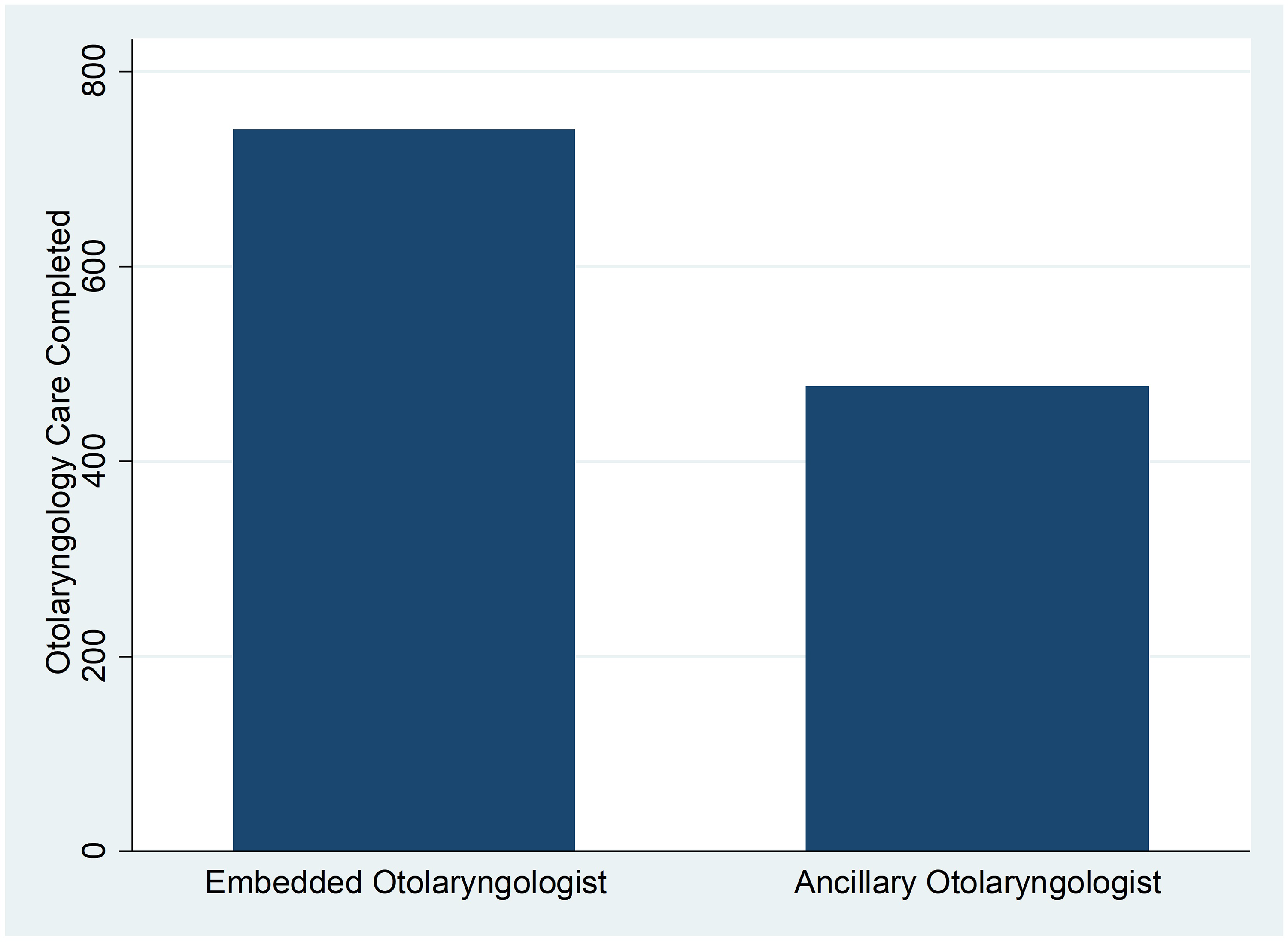
Number of children who completed otolaryngology follow-up by 18 months of age, parsed by embedded or ancillary services. The difference between embedded and ancillary services was statistically significant, P < .001.
Average age at first otolaryngology care was similar for teams with embedded (8.4 months) and ancillary (8.5 months) providers (P = 0.83). Most infants (n = 1166, 93.6%) had tubes placed before 18 months of age, with 809 (64.0%) having their first set of tubes placed at the time of palate repair. The average age at tube placement was slightly but not significantly younger for children with Veau III and IV clefts (11.9 months) versus those with Veau I and II (12.1 months; P = 0.63).
Discussion
The purpose of this study was to examine ear and hearing care received by children with CP ± L in the US across multiple ACPA-approved Cleft Palate Teams, through evaluation of adherence to published clinical guidelines.32–35 Secondarily, we set out to understand whether embedding otolaryngology and audiology providers into the Team visit has an impact on adherence. The ACPA Standards for Approval of Cleft Palate and Craniofacial Teams 40 requires that “the team demonstrates access to professionals in the disciplines of psychology, social work, audiology, genetics, general and pediatric dentistry, otolaryngology and pediatrics/primary care.” The term “access” does not prescribe whether these services are embedded or ancillary to team care and allows for flexibility in how teams ensure access to this type of care. This language stands in contrast to that regarding team composition including the “core” specialties of speech-language pathology, surgery, and orthodontics, which must “participate in team meetings.” 40
Our results suggest that there is considerable variability across ACPA-approved cleft teams regarding how otolaryngology and audiologic care is accessed and provided within the first 16 months of life. Although 89.3% of children in this study received timely otolaryngology care, based on guidelines from AAO-HNS, 35 audiologic follow-up was more limited and fell below reported rates in the greater population of infants who do not pass the NBHS.37,38 The results of this study are consistent with a previous study examining the likelihood of audiologic care provision depending upon whether care was provided in the context of a team versus individual providers. 44 This limited audiologic follow-up presents a particular challenge for this population given that the current recommendation for infants with CP ± L is to have an audiologic evaluation by 9 months of age regardless of newborn hearing screening outcome. 32 Additionally, parents in this study reported hearing issues in 75.2% of children, which constitutes another risk factor for hearing deficits warranting timely follow-up by 9 months. 32
Overall, the provision of otolaryngology care (89.4%) was better than audiologic follow-up (36.6%) for centers involved in this study, though both disciplines had differences across teams who had embedded providers versus those ancillary to the team. For both otolaryngology and audiology, provision of services was significantly better for those children served by teams with embedded otolaryngologists or audiologists. These findings should not be surprising, given that multidisciplinary coordinated care for patients with complex health issues has been shown to improve adherence to recommended follow-up and overall health outcomes across many complex health conditions.44–46
Although there is no international consensus on the management of OME in children with CP ± L,16,47 93.6% of the children in this study had documentation of ear tube placement, with most having placement completed at the time of palate repair. Shaffer et al. (2019) 48 also reported widespread tympanostomy tube placement in a cohort of children with CP ± L (98.6%), with 96.5% of children having otitis media at the time of tube placement. Unfortunately, complications with early tube placement (ie, at time of lip repair as opposed to at time of palate repair) have been reported, including myringosclerosis (35.2%), granulation (22.8%), perforation (17.9%), retained tubes (5.5%), and cholesteatoma (1.4%), with ultimately 67.4% of children requiring tube replacement for ongoing middle ear dysfunction.41,48 Despite noted complications, accelerated treatment of middle ear dysfunction in children with CP ± L via tympanostomy tube placement is recommended by the AAO-HNS 35 given the increased risk for speech-language delays in this population. Additionally, early tube placement has been shown to reduce prevalence of CHL. 26
One major limitation of this study included the use of retrospective chart review and parent report to document adherence to ear and hearing follow-up, and difficulties with documenting this care when it occurred outside of the enrolling site (eg, otolaryngology private practice). Reporting of otologic and audiologic care was documented on forms that relied on parent report and electronic medical record review, thus, it cannot be ruled out that there could be some discrepancies in if and how care was documented, as is a limitation of any retrospective study, or due to limited parent recall of outside care, etc. Another limitation is that the Joint Committee on Infant Hearing (2019) 32 recommendation for audiologic follow-up by 9 months of age was introduced in December of 2019. Although 85% of children enrolled in this study would have reached 9 months of age after this date, there is often a lag in adopting evidence-based recommendations that may have impacted site and provider implementation. Additionally, some care was likely impacted by the COVID-19 pandemic, in which some medical services (including ENT and audiology) were temporarily restricted during 2020 and 2021, which may have contributed to why some follow-up rates at sites in this study were lower than expected. Lastly, adherence to ear and hearing care recommendations may also have been impacted by other barriers in access to care and family choice. Findlen et al. (2022) previously documented that non-adherence to recommended follow-up is multifactorial and can be attributed to provider non-adherence, family choice, or a combination of both provider non-adherence and family choice. 39 Although previous reports suggest that families with unfavorable social determinants of health (SDOH) 49 do not experience additional barriers once connected to interdisciplinary cleft teams, 50 further study is needed within this cohort to determine whether unfavorable SDOH increase barriers to accessing otolaryngology and audiology services, and how SDOH needs may impact long term outcomes. Future studies planned include analyses of discrete audiometric evaluation data for all participants across the site, up to 36 months of age, which will define the prevalence, type, and degree of hearing loss experienced by this population, as well as continue to explore causes of variation in follow-up care rates.
Conclusions
Many factors can influence a Cleft Team's approach to team member composition, including practicality of discipline location, clinic size/setting, required time for full team appointments, and physical access to specialized otolaryngology and audiologic equipment, as well as the availability of the providers themselves. Although it may not always be possible to have otolaryngologists and audiologists present at each child's Team visit, the results of this study suggest inferior access to ear and hearing care when these services are provided as ancillary to the core team. For teams who may not be able to embed otolaryngologists and/or audiologists within their teams, it will be critical to create and maintain feasible referral pathways with bi-directional communication and to minimize any barriers to care access to ensure children and families receive the ear and hearing care needed to maximize speech-language outcomes.
Supplemental Material
sj-pdf-1-cpc-10.1177_10556656241283535 - Supplemental material for Current Ear and Hearing Care Practices for Infants and Toddlers with Cleft Palate in the United States
Supplemental material, sj-pdf-1-cpc-10.1177_10556656241283535 for Current Ear and Hearing Care Practices for Infants and Toddlers with Cleft Palate in the United States by Ursula M. Findlen, Anna Meehan, Gregory Allen, Deborah S.F. Kacmarynski, Jonathan Grischkan, Emily C. Nightengale, Lauren C. Alexander, Sarah Hatch Pollard, Adriane L. Baylis and in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements:
The authors would like to acknowledge the clinical sites, cleft team providers, study coordinators, and children and families participating in the Cleft Outcomes Research NETwork (CORNET) Consortium, in alphabetical order: Ann & Robert H. Lurie Children's Hospital; Phoenix Children's Hospital; Boston Children's Hospital; Children's Hospital of Alabama; Children's Hospital Colorado; Children's Hospital Los Angeles; Children's Hospital of Philadelphia; John Hopkins University; Lancaster Cleft Palate Clinic-Penn State/Milton S. Hershey Medical Center; Nationwide Children's Hospital; Rady Children's Hospital; Seattle Children's Hospital; Shriners Hospital for Children – Chicago; Texas Children's Hospital; University of Iowa; University of Wisconsin – Madison. We would also like to acknowledge Kathy Chapman, PhD, Principal Investigator at the University of Utah, for her leadership over the CORNET project. This work will be presented at the 81st American Cleft Palate Craniofacial Association (ACPA) Annual Meeting, April 10-13, 2024, Denver, CO.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Institute of Dental & Craniofacial Research of the National Institutes of Health under Award Number R01DE027493.The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.