
Abstract
A true median cleft is an extremely rare congenital anomaly characterized by a midline vertical cleft and various deformities, also known as Tessier number 0 cleft. Here we report a case of a 5-year-old Asian boy with true median cleft associated with sinus tracts in the nasal septum, a phenomenon not previously reported in the literature. The tracts were identified as the cause of recurrent infections around the oral vestibule and upper lip. The tracts were resected successfully, and postoperative progress has been satisfactory. We discuss the importance of preoperative image evaluations and the selection of a suitable surgical approach.
Introduction
Median cleft is an extremely rare facial deformity and is embryologically classified as true median cleft or false median cleft, also known as Tessier number 0 cleft.1,2 A true median cleft often occurs as a result of frontonasal dysplasia, whereas a false median cleft occurs because of frontonasal agenesis and is thought to be included in holoprosencephaly. 3
This report presents the case of a 5-year-old boy with a true median cleft, which had been treated conventionally by cheiloplasty in early childhood. The patient presented repeatedly with abscess formation in the oral vestibule after undergoing cheiloplasty, the cause of which was found to be sinus tracts in the nasal septum. We report this case to underscore the importance of evaluating preoperative images in cases of true median cleft and considering the possibility of an associated sinus tract.
Case Report
A 5-year-old Asian boy presented with a true median cleft. He was delivered at full term without complications. His birth weight was normal and there was no history of exposure to risk factors. There was no family history of facial cleft.
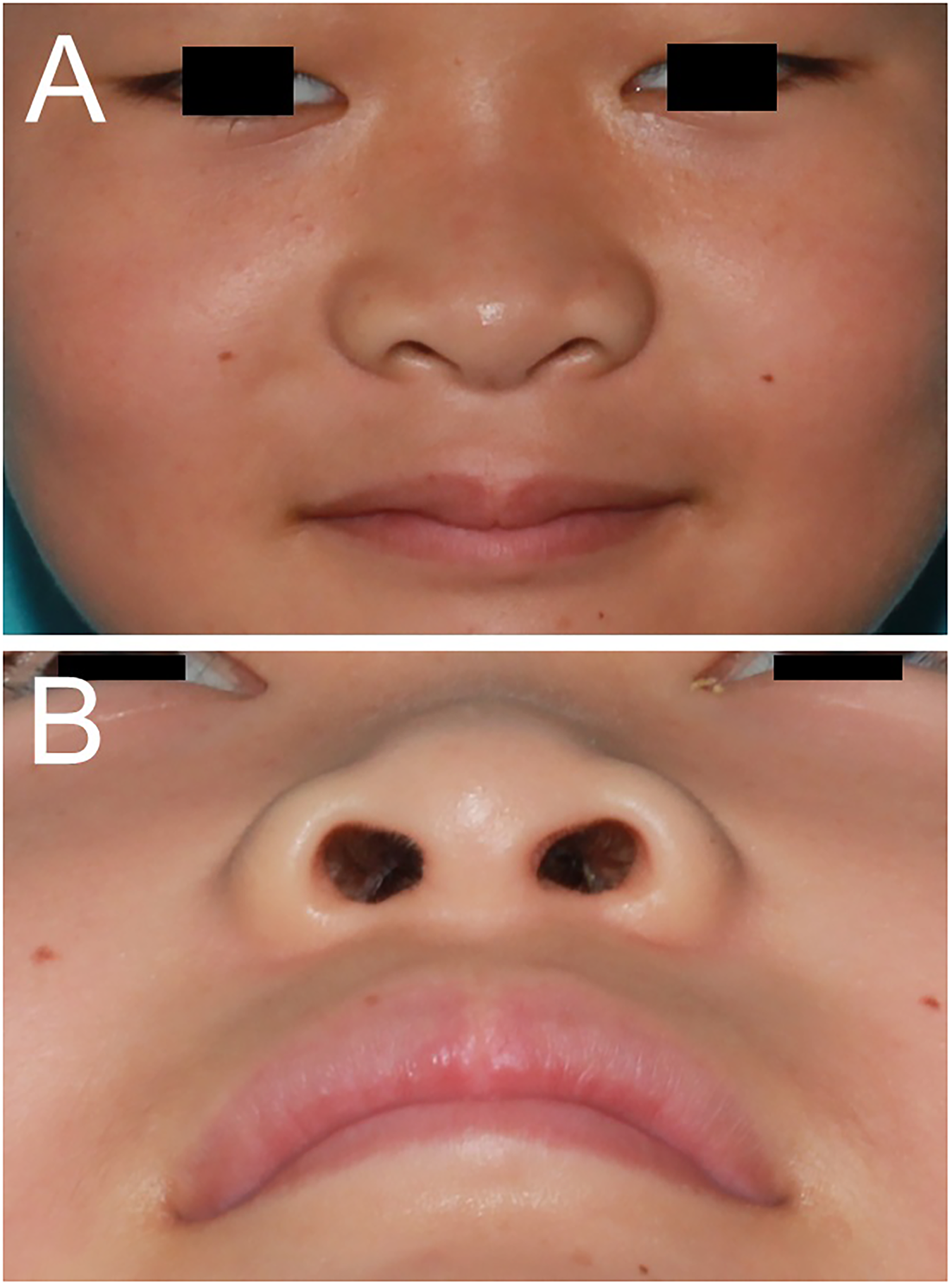
Physical examination revealed an incomplete median cleft of the upper lip. In the mucosal side of the upper lip, scar tissue extended through the center of the lip to the alveolar ridge. There was a pinhole-like fistula opening in the scar tissue of frenulum labii superioris. Vertical notch deformity was seen from the base of the columella to the nasal tip. There were no other noteworthy physical findings (Figure 1A and B). Computed tomography (CT) showed a slit-like midline cleft in the alveolus and no cleft palate was seen (Figure 1C and D).
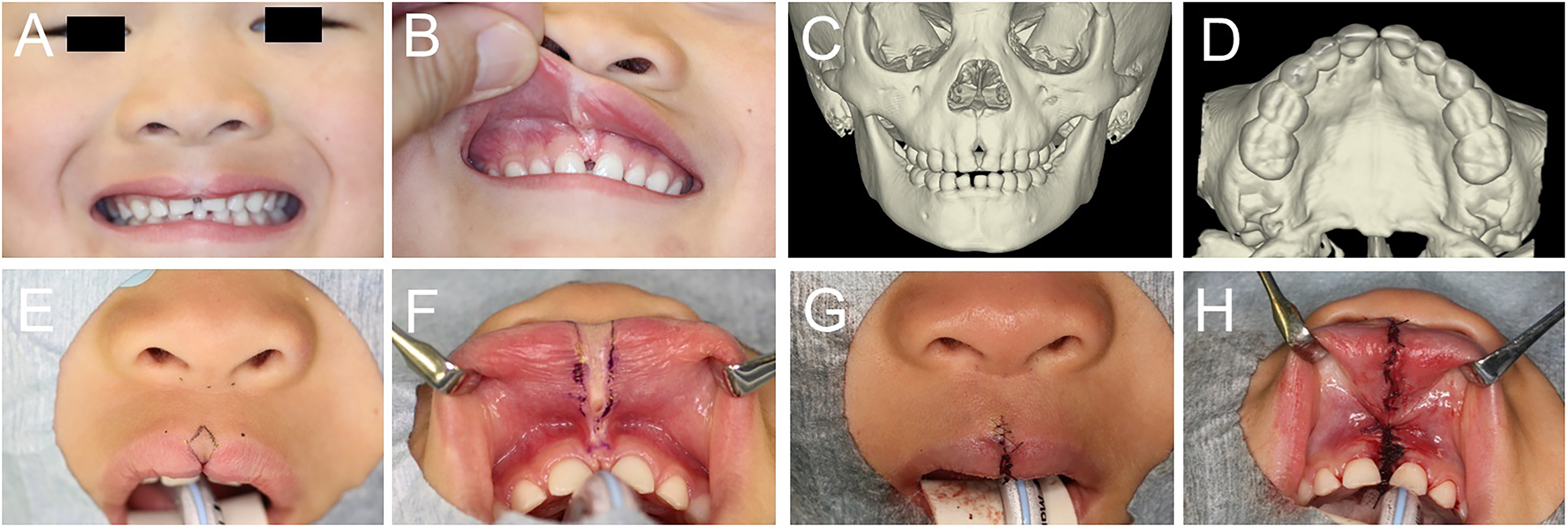
Preoperative and postoperative photographs and preoperative images were obtained at 5 years of age. (A) Preoperative close-up photograph of the nose and upper lip showing a median cleft of the upper lip and a notch deformity at the columella. (B) Preoperative intraoral photograph showing scar tissue extending to the alveolar ridge and a cleft alveolus. There was a pinhole-like fistula opening in the scar tissue of the frenulum labii superioris. (C) Three-dimensional (3D) image of the maxilla. A slit-like midline cleft in the alveolus was seen. (D) 3D image of the maxilla. There was no cleft palate. (E) Frontal photograph showing the preoperative design. An inverted V-shape incision was used. (F) Intraoral photograph showing the preoperative design. An incision was made around the scar tissue and the pinhole-like fistula. (G) Frontal photograph obtained postoperatively. A straight-line repair technique was used. (H) Intraoral photograph obtained postoperatively. The scar tissue penetrating into the slit-like cleft of the alveolus was resected.
The upper lip was repaired with excision of the scar tissue when the patient was 5 years old. The epithelium and scar tissue extending from the cleft of the red lip to the alveolar ridge were excised together using an inverted V-shaped excision. The scar tissue in the oral vestibule and that penetrating into the slit-like cleft of the alveolus were also excised as far as possible. The pinhole-like fistula opening in the scar tissue extended through the scar tissue and seemed to end inside the scar tissue near the alveolar ridge. During the resection of the scar tissue in the oral vestibule, the fistula was not exposed and therefore we judged that the fistula was resected along with the scar tissue. The anterior nasal spine and alveolar bone were not treated. After performing orbicularis oris muscle plasty, the skin and mucosal sides were closed separately (Figure 1E to H).
Three years later, the patient presented with swelling and discharge of pus in the midline of the oral vestibule. Ultrasonography revealed a cyst in the oral vestibule. The cyst and the scar tissue around it were resected (Figure 2). Histological examination revealed a fistula accompanied by chronic inflammation.
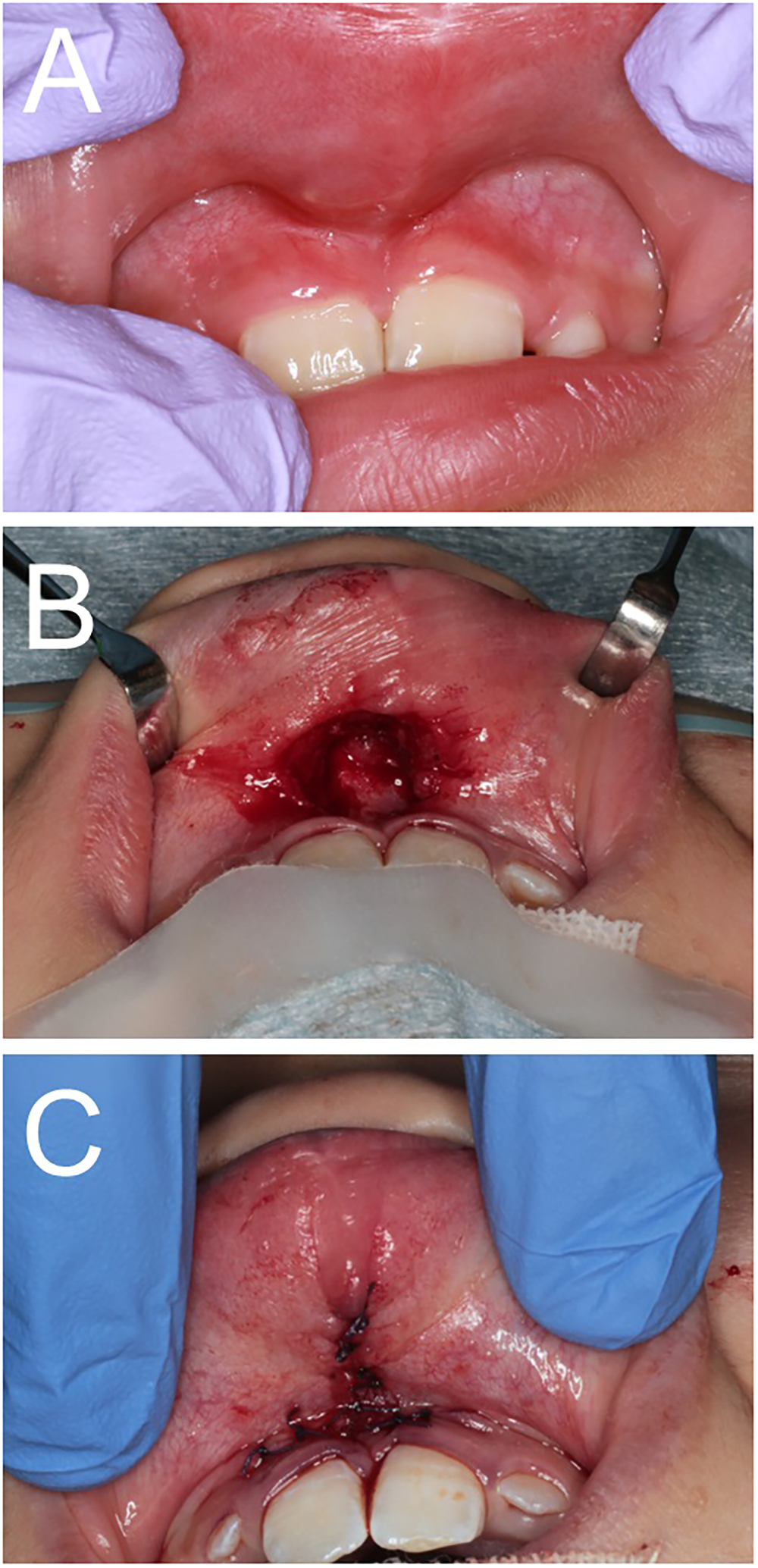
(A) Photograph obtained 3 years after the first surgery. Infection is present in the oral vestibule. (B) Intraoral photograph was obtained at the time of the second surgery. A resection of the cyst was performed. (C) Intraoral photograph obtained postoperatively. Straight-line closure was performed.
Discharge of pus recurred 3 months after the second surgery and was treated conservatively using oral antibiotics. However, there were repeated cycles of remission and recurrence of infection in the following 6 months. Enhanced magnetic resonance imaging (MRI) showed a large subcutaneous fluid collection measuring 1 cm in the upper lip, which raised suspicion for abscess formation. There was also a lesion extending from the fluid collection to the nasal septum through a small fistula near the anterior nasal spine. The lesion was duct-like, extended craniocaudally within the nasal septum, and showed high signal intensity on T2-weighted imaging. The lesion connected to the right nasal cavity on the cranial side. No connection with the cranial cavity or other fistula was seen (Figure 3). The lesion in the nasal septum was suspected to be a sinus tract and the cause of infection.
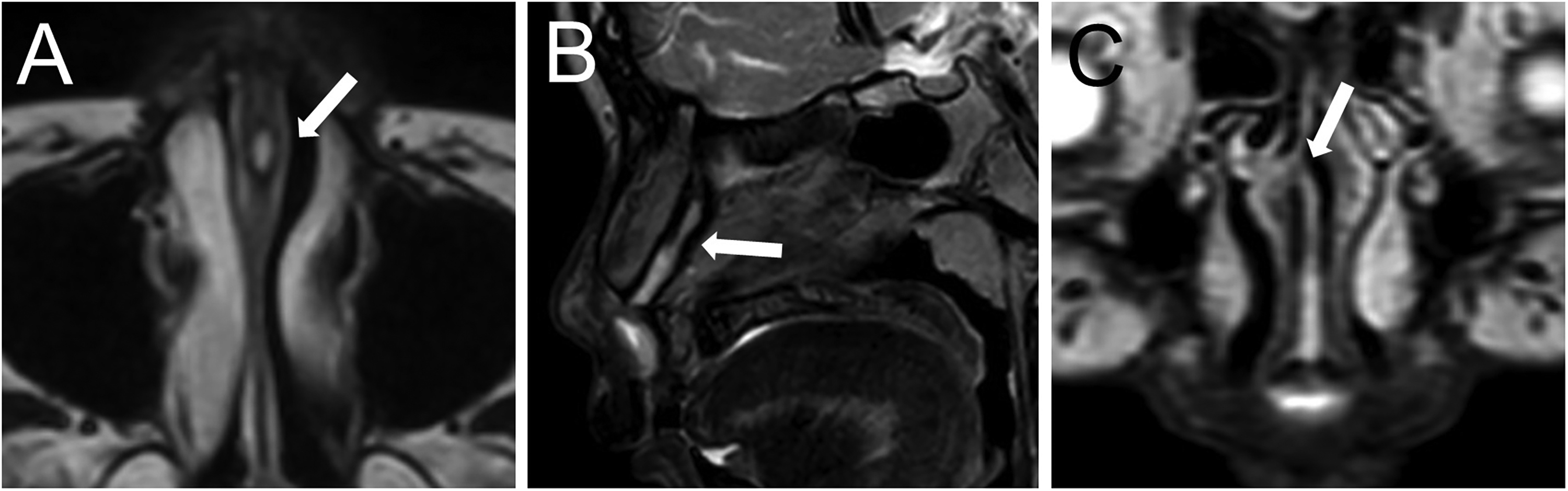
Findings on contrast-enhanced magnetic resonance images obtained 9 months after the second surgery. The arrow indicates the sinus tract. (A) Axial T2-weighted image showing a tract between the septal cartilages. (B) Sagittal T2-weighted image showing the tract extending craniocaudally through the septal cartilage. (C) Coronal T2-weighted image showing the tract connected to the right nasal cavity.
The plan was to perform resection of the sinus tract using two approaches, one via the oral vestibule and the other via the nose. The approach from the oral vestibule was performed via a horizontal spindle-shaped incision that was designed to include the scar tissue. The approach from the nose was performed by open rhinoplasty using a mid-columellar inverted V-shaped incision and an infracartilaginous incision on both sides. Incision of the oral vestibule revealed another sinus tract with a diameter of 2 mm near the anterior nasal spine. Dissection was performed along the tract, which extended between the medial crus of the lower lateral cartilages. This tract, which was not evident on MRI, was resected by pulling it through the nose to the oral vestibule. The tract shown on MRI was on the dorsal side of this tract and extended into the bifid septal cartilages. This tract was dissected through to the opening in the right nasal cavity and excised near the nasal mucosa. As a result, the resected lesions extended from the vestibule and bifurcated into two tracts, one extending between the medial crus of the lower lateral cartilages and the other extending between the bifid septal cartilages (Figure 4). The tract extending between the medial crus of the lower lateral cartilages was 2 mm in diameter and 8 mm in length, and the tract extending between the bifid septal cartilages was 7 mm in diameter and 25 mm in length. After resection of the tracts, the lower lateral cartilages were sutured together to close the dead space. Finally, the nose and oral vestibule were closed individually. Histological examination revealed a lumen covered by stratified squamous epithelium, which was diagnosed as a sinus tract (Figure 5).
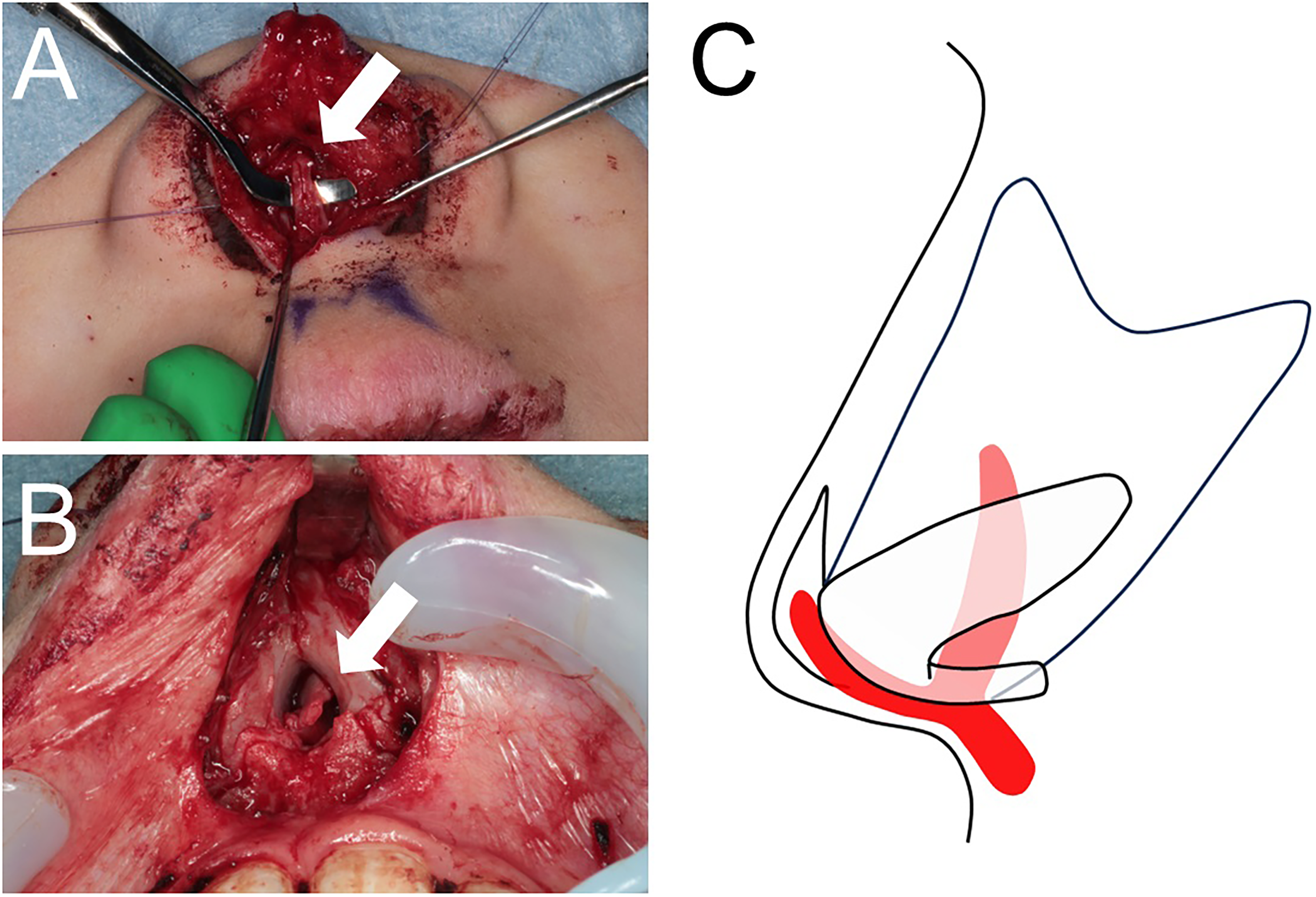
Intraoperative findings. (A) Close-up photograph of the lower lateral cartilages. The arrow indicates the tract extending between the medial crus of the lower lateral cartilages. (B) Close-up photograph of the bifid septal cartilages. The arrow indicates the tract extending between these cartilages. (C) Schema of the nose and tracts. One tract extends between the lower lateral cartilage and the other between the bifid septal cartilages.

Photographs and histologic findings of the tracts. (A) The resected tissue (white arrow) and tract (black arrow) extending between the lower lateral cartilages. (B) The resected tract extending between the bifid septal cartilages. The left side of the image corresponds to the caudal side of the tract. (C) Histologic findings of the lumen of the tract covered by stratified squamous epithelium in a low-power field. (D) Histologic findings of the lumen of the tract covered by stratified squamous epithelium in a high-power field.
Eighteen months after the surgery, the patient has a satisfactory esthetic result and has had no recurrence of infection (Figure 6).
Photographs were obtained 18 months after resection of the tracts. (A) Frontal view of the face. The vertical scar is not visible and the result is satisfactory. (B) Close-up view of the nose and upper lip. The scar in the columella is unremarkable and there is no postoperative deformity.
Discussion
A craniofacial cleft is a fissure in the face and/or head that affects both bones and soft tissues. It is a rare congenital anomaly with an incidence in the range of about 1.4 to 4.9 per 100 000 live births. 4 One of the main methods used to categorize craniofacial clefts is the number system devised by Tessier, 5 who classified facial clefts based on localization of the fissure, referred to as cleft number 0 to 14 or 30. A midline vertical cleft is classified as Tessier number 0 and number 14 and is known as a median cleft, which is extremely rare. The prevalence of cleft lip in Asian populations has been reported to be 1.33 per 1000 births. 6 Median clefts are rare among the cleft population, with a reported prevalence of 0.43% to 0.73%. 7 There have been few reports on the prevalence of true median cleft, which is reported to be 0.17% among the cleft population. 8
The most widely accepted embryological explanation for Tessier number 0 cleft is the incomplete merging of both medial nasal prominences because of inhibition of mesenchymal penetration. 9 The typical phenotype of Tessier number 0 cleft includes a median cleft of the upper lip and a bifid nose deformity, and is the most common of the craniofacial clefts. 10 They might also be accompanied with hypo- or hypertelorism, intracranial anomalies such as frontonasal encephalocele, and cranial base deformity. 11 In true median cleft, the fissure tends to be broad horizontally and the tissue volume may be excessive or normal. The deformity in true median cleft lip may include broad or short columella and philtrum columns, hypertelorism, bifid frenulum, bifid septal cartilages, and cleft of the alveolus. 1 Due to the broad range of deformities, the surgical treatment needed is extensive. Surgical correction of cleft lip in median clefts is often needed, which involves a reconstruction of the Cupid's bow, labial philtrum, vermillion, and buccal mucosa. 12 If the nasal malformation is severe and unappealing, they may need rhinoplasty in the future. 13 They may also have issues with the eruption of incisors and may need orthodontic treatment in the future. 10
In our case, sinus tracts were found to be the cause of repeated episodes of infection. A comprehensive literature search about median cleft was performed using Pubmed and Google Scholar but we could not find any previous reports of median cleft with sinus tracts in the nasal septum. There have been reports of a similar congenital fistula-like midline lesion associated with median cleft, midline upper lip sinus, and nasal dermoid sinus cyst (NDSC).14,15 Congenital upper lip sinus is a congenital lesion that presents as a pit in the frenulum or in the vermillion of the upper lip and the tract is usually lined by stratified squamous epithelium. Many theories have been put forward to explain the cause of midline sinuses.16–19 These include failure of ectodermal invagination of the nasal placodes, failure of mesodermal merging of the medial nasal processes, failure of complete fusion of the maxillary process, and breakdown of the epithelium. NDSC is a congenital lesion that presents as a pit in the median line of the nasofrontal area from the glabella to the columella and may extend to the nasal cartilages, nasal bone, or sometimes intracranially. 20 This lesion is lined by stratified squamous epithelium associated with adnexal structures, including hair follicles, sebaceous glands, and eccrine glands. The predominant embryological theory is that it is caused by the failure of separation of early embryological communication between the projected dura and nasal dermis. 21 Another theory suggests that early ectodermal inclusion events in the median fusion area might be the cause. 22
The etiology of the sinus tracts in our case is not clear. There has been some discussion about the cause-and-effect relationship between median clefts and midline lesions. In a report on a case of midline upper lip sinus associated with a median cleft, it was suggested that thin tissue or lack of muscle in the cleft lip might have caused the breakdown of the epithelium. 16 On the other hand, a report on a case of NDSC associated with a median cleft mentioned that the cleft might have been a secondary event that occurred as a consequence of NDSC. 15 Therefore, we can consider two possibilities for the pathogenesis in our case. One is that the median cleft occurred first and caused the breakdown of the epithelium and the formation of a fistula. Another is that a tract occurred first by early ectodermal inclusion and caused the median cleft. If there are future case reports of other median clefts with sinus tract in the nasal septum, perhaps a more definite cause can be determined.
Through our case, we recognized the importance of preoperative image examinations and ensuring a broad operative field. In our case, we did not recognize the sinus tract extending further than the anterior nasal spine when performing the first cheiloplasty. Retrospectively observing the computed tomography (CT) images obtained before the first surgery, an indistinct shadow can be seen in the nasal septum (Supplemental Figure 1). This finding indicates that the sinus tract was present when the first surgery was performed. We could not confirm the connection of the tract and fistula in the CT images, but it is natural to think that the sinus tracts were connected to the pinhole-like fistula opening in the scar tissue which we thought to have resected completely. Therefore, we can conclude that the sinus tracts were overlooked at the first surgery. The presence of the fistula in the scar tissue was one of the reasons for the oversight, but it could also be due to the absence of appropriate preoperative imaging examinations which made the full extent of the lesion unknown. As previously mentioned, median clefts can present with various types of deformity and associated lesions. Therefore, it is important to perform thorough imaging examinations, such as MRI and ultrasonography, to investigate the full extent of the lesion and the possibility of other lesions. On the other hand, our patient also had a tract between the lower lateral cartilages that was not visible on MRI. Therefore, preoperative imaging might not be sufficient for resection of all sinus tracts, and intraoperative broadening of the operative field may be important. In our case, we added an open rhinoplasty to the incision of the oral vestibule for the purpose of ensuring a broad field of view in the nasal area. Given that we found a tract that was not visible on MRI, we conclude that the addition of an open rhinoplasty can allow observation of the entire lesion.
In the 18 months since our patient's last surgery, he has had esthetically satisfactory results and no recurrence of infection. Given that the first infection occurred 3 years after the first surgery, it is uncertain whether or not the infection will recur during long-term follow-up. Furthermore, he is only 12 years old at present, so long-term follow-up is necessary to determine whether there will be problems with the growth of the nose. We plan to continue with follow-up, keeping in mind that there might be other lesions that we have not detected in imaging studies.
Conclusion
We have encountered a case of true median cleft with sinus tracts in the nasal septum. These tracts were the cause of repeated episodes of infections. We believe that detailed imaging examination to exclude the existence of sinus tracts is important in the case of the median cleft. However, given that a tract was not found on preoperative imaging, ensuring a broad operative field is also important when performing surgery on tract-like lesions in patients with a median cleft.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241298133 - Supplemental material for True Median Cleft With Sinus Tract in the Nasal Septum: A Case Report
Supplemental material, sj-docx-1-cpc-10.1177_10556656241298133 for True Median Cleft With Sinus Tract in the Nasal Septum: A Case Report by Sho Suzuki, Kosuke Kuwahara, Mutsumi Okazaki and Hideaki Kamochi in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent Statements
Our institution does not require ethical approval for reporting individual cases or case series. We obtained the informed consent of the patient and his parent using the institutional consent form.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.