
Abstract
Autologous fat grafting for posterior pharyngeal wall augmentation has been described as a safe and effective treatment option for a subset of patients with mild to moderate velopharyngeal insufficiency (VPI). Reported complications including hyponasality and obstructive sleep apnea (OSA) are exceedingly rare. We describe the development of severe fat graft hypertrophy and subsequent OSA in a series of 3 patients several years after undergoing autologous fat grafting for VPI. All patients required revisional surgery for the removal of the engrafted fat. Although rare, OSA can result from hypertrophy of autologous fat grafted into the posterior pharyngeal wall for treatment of VPI.
Background
The velopharyngeal apparatus consists of the velum, the lateral pharyngeal walls, and the posterior pharynx. Incomplete closure of these component parts during speech production leads to velopharyngeal inadequacy (VPI) and can result in hypernasality, audible nasal emission, nasal turbulence, and compromised intelligibility. Velopharyngeal insufficiency is a common problem in patients with a cleft palate. Reported rates of VPI are variable and may be influenced by the size of the cleft and the repair technique.1–3
The severity of the associated speech disturbance often depends on the size of the velopharyngeal gap, the length of the palate, and the relative mobility of the oropharyngeal musculature during phonation. Common surgical treatments for VPI include revision palatoplasty, such as Furlow conversion, dynamic sphincter pharyngoplasty (DSP), posterior pharyngeal flap, and augmentation of the posterior pharyngeal wall with both alloplastic and autologous grafts.4–7 More recently, the use of the buccal myomucosal flap for palatal lengthening has been shown to be effective in treating VPI.8,9 The purpose of these procedures is to narrow the gap between the velum and the posterior pharyngeal wall so that complete closure can be achieved.
However, these surgical procedures can be associated with significant risks.10,11 Posterior pharyngeal flap has known associations with airway obstruction and we have previously shown that DSP can also lead to a clinically significant increase in obstructive sleep apnea (OSA) postoperatively. 12 In patients with small yet functionally significant velopharyngeal gaps, however, larger surgical intervention may not be warranted. In this subset of patients, autologous fat grafting has been shown to be an effective, less invasive alternative to achieving velopharyngeal closure and improving speech outcomes.13–18 Despite variability in technique and reported recipient sites, prior reviews have shown this technique to be safe with the development of hyponasality and OSA exceedingly rare.19–22
The objective of this case series is to report on 3 patients who developed significant late fat hypertrophy and severe OSA with airway compression several years after undergoing autologous fat grafting to the posterior pharynx for treatment of VPI.
Materials and Methods
All patients receiving care for cleft lip and palate at our institution are managed by a multidisciplinary treatment team. Velopharyngeal insufficiency is diagnosed via standard perceptual speech assessment and video nasoendoscopy performed by a certified speech and language pathologist. The videos are analyzed in conjunction with the craniofacial surgeon, and the surgical treatment is determined by the overall gap size and dynamic function of the velopharyngeal apparatus. As previously described, autologous fat grafting is typically chosen for small velopharyngeal gaps (0.5-2 cm2) in patients with mild to moderate hypernasality or in those with increased risk of developing OSA postoperatively. 19 All patients are evaluated postoperatively via repeat speech assessment and are screened for the development of OSA symptoms at 3 months and again at one year following surgery. Repeat nasoendoscopy is reserved for any patient that exhibits abnormal speech patterns postoperatively for visual inspection of the velopharyngeal port. Any patient presenting with OSA symptoms, including snoring, observed apnea events, daytime lethargy, and hyperactivity is referred to sleep medicine for a polysomnography study.
Surgical Technique
Autologous fat harvest and grafting was performed with the patient under general endotracheal anesthesia in the supine position. Fat was harvested from the abdomen, buttock or thighs, depending on availability, and processed using the Coleman technique. 23 The volume and injection sites were determined by the specific size and gap location identified on preoperative nasoendoscopy. Following graft harvest and processing, the posterior pharyngeal wall was exposed, and a blunt injection catheter was placed through the mucosa and submucosa to introduce the fat into the retropharyngeal space using 1cc syringes. A red rubber catheter can be passed though the nose and sewn to the uvula to invert and retract the soft palate to better expose the region of the Passavant's ridge. Manual pressure was applied directly below the injection site to prevent undesired migration of the fat. The endpoint for injection was determined based on visual inspection of the velopharyngeal port by the senior surgeon. Overcorrection was routinely performed taking into account partial fat graft resorption expected postoperatively. As needed, a single suture (4-0 Vicryl) can be used to seal the injection site and prevent extrusion of the injected fat.
Results
In total, 76 patients were treated with fat grafting for VPI by 3 craniofacial surgeons at our institution between 2007 and 2022. The mean fat injection volume was 10.4cc (range 2.0-31.5cc). Fifteen patients (19%) received multiple rounds of fat grafting for persistent velopharyngeal gaps. Of these, 2 patients developed fat hypertrophy and OSA. One additional patient developed OSA after a single fat injection.
Case Examples
Details of each case are summarized in Table 1.
Patient Demographics and Surgical Details.
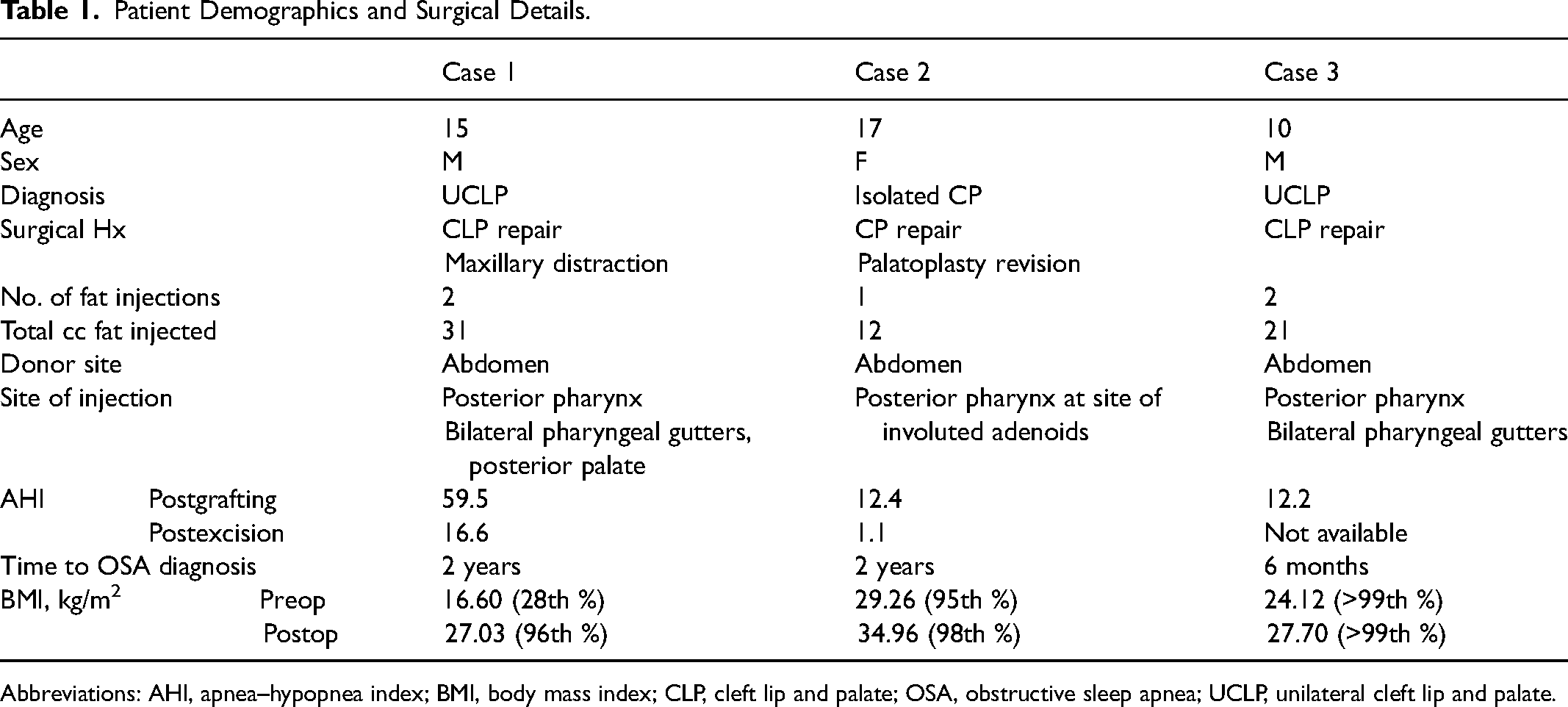
Abbreviations: AHI, apnea–hypopnea index; BMI, body mass index; CLP, cleft lip and palate; OSA, obstructive sleep apnea; UCLP, unilateral cleft lip and palate.
Patient 1
A 15-year-old male with history of left unilateral cleft lip and palate who underwent age-appropriate lip and palate repairs with subsequent LeFort I maxillary advancement via rigid external distraction for severe maxillary hypoplasia and Class III malocclusion at 10 years old. Two years following distraction, he presented with hypernasality and nasoendoscopy revealed a moderately sized central velopharyngeal gap with a circular closure pattern. The decision was made to perform posterior pharyngeal wall augmentation via autologous fat grafting (13cc) harvested from his abdomen and injected just below the adenoid pad and into Passavant's ridge. Repeat nasoendoscopy performed 6 months postoperatively demonstrated a persistent small velopharyngeal gap, and the decision was made to repeat fat grafting to the central posterior pharynx (13cc), bilateral pharyngeal gutters (2cc's each), and the posterior palate (1cc) as guided by the closure pattern. The patient had significant improvement in nasometry scores postoperatively with increased intelligibility.
Two years following the second grafting surgery, he developed increased snoring and daytime fatigue and polysomnography revealed an AHI of 59.5 consistent with severe OSA. This coincided with an increase in body mass index (BMI) from 16.6 kg/m2 (28th percentile) to 27.03 kg/m2 (96th percentile). Nasoendoscopy at that time showed a competent velopharyngeal mechanism with mild intermittent gapping. A CT neck was obtained, which revealed the source of his OSA as a giant retropharyngeal lipoma, extending 7.6 cm in craniocaudal dimension with internal septations (Figure 1). The lipoma nearly occluded the inferior nasopharyngeal airway with significant narrowing of the posterior oropharynx. The patient was taken to the operating room for excision of the lipomatous mass, which was found underlying the posterior pharyngeal wall with significant impingement on the airway down to the level of the epiglottis. He had significant improvement in his OSA (postop AHI 16.6) and maintained his excellent speech outcome.
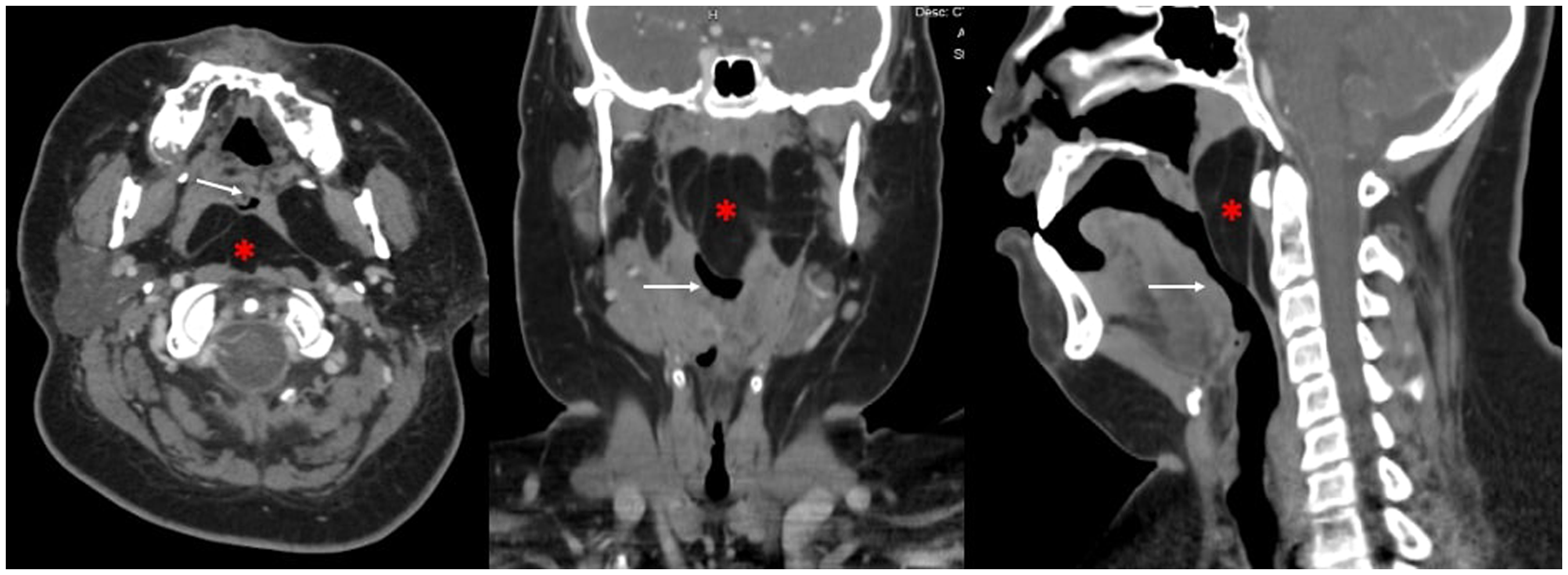
CT scan of patient 1 demonstrating the lipomatous mass (*) in the posterior pharyngeal wall compressing the upper airway (white arrow).
Patient 2
A 17-year-old female with history of isolated cleft palate with age-appropriate repair who developed VPI during adolescence and underwent a Furlow conversion palatoplasty at age 14. This improved her speech significantly but she had persistent hypernasality with a small velopharyngeal gap on nasoendoscopy at age 15. Autologous fat grafting was chosen as the least invasive procedure to improve her speech and 12cc of fat was subsequently harvested from her abdomen and injected along with the posterior pharynx at the site of the involuted adenoids. This resolved her hypernasality.
Two years following surgery, she presented with symptoms of OSA and difficulties swallowing. This was associated with an increase in BMI from 29.26 kg/m2 (95th percentile) to 34.96 kg/m2 (98th percentile). A polysomnography was obtained and revealed an AHI of 12.4 with repeat nasoendoscopy demonstrating a large lipomatous mass (Figure 2). An MRI head and neck revealed a midline retropharyngeal lipoma with extension into the right parapharyngeal space and superiorly to the level of the skull base. There was an increased mass effect on the posterior wall of the oropharynx at the level of the soft palate, which was significantly narrowed (Figure 3). She was taken to the operating room on 2 separate occasions for debulking of the adipose mass. This resolved her OSA (postop AHI 1.1) and did not affect her speech.

Nasoendoscopy of patient 1 demonstrating large lipomatous mass pushing against the posterior pharyngeal wall obstructing the velopharyngeal sphincter.
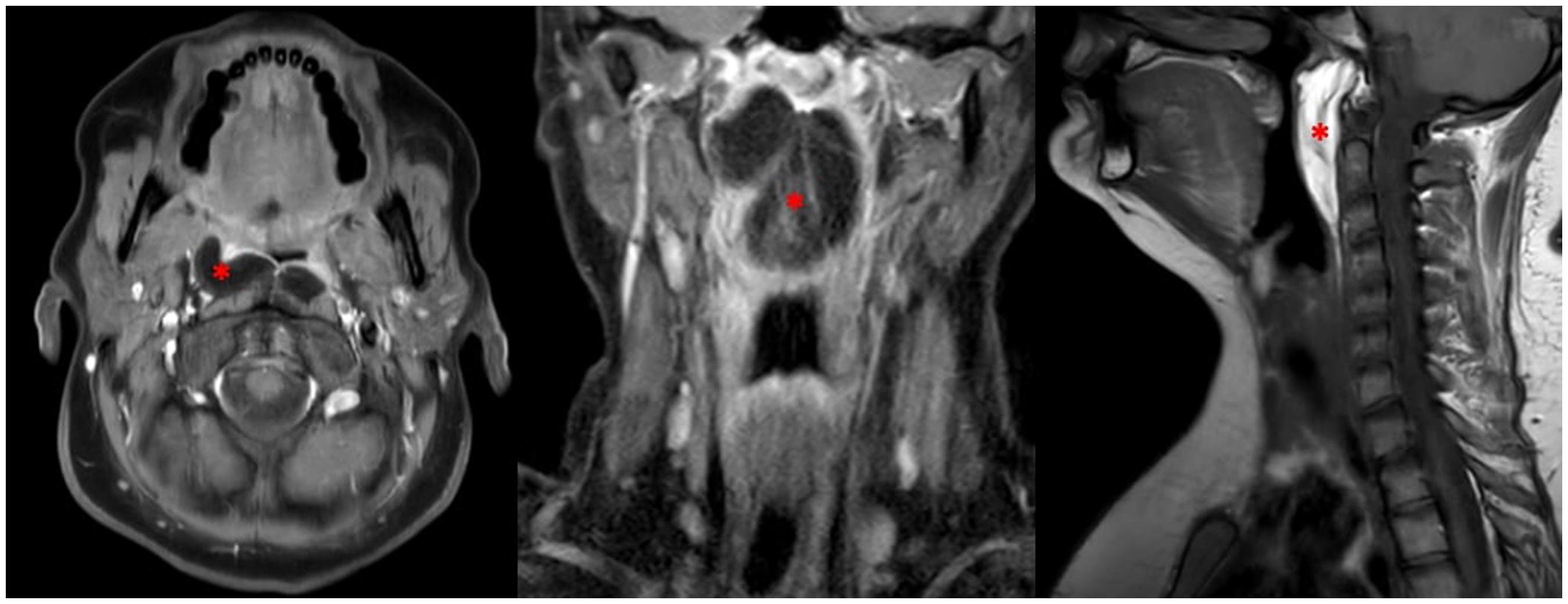
MRI of patient 2 revealing a multilobulated lipomatous mass (*) in the posterior pharyngeal wall with extensive craniocaudal extension from the skull base to the epiglottis with compression of the upper airway.
Patient 3
A 10-year-old male with history of right unilateral cleft lip and palate who underwent age-appropriate repairs and subsequently developed VPI. Nasopharyngoscopy showed a circular closure pattern with a central velopharyngeal gap. On speech assessment, he had audible nasal air emission and severe hypernasality. He underwent autologous fat grafting. A total of 17cc of fat was harvested from his abdomen and injected into the right (6cc), left (8cc), and central (3cc) posterior pharynx at the base of the adenoid pad. He had persistent hypernasality 2 years following surgery with a small central gap in his velopharyngeal port and no symptoms of OSA. Repeat fat grafting was performed with 4ccs injected into the central posterior pharynx. He had improvement in speech but subsequently developed symptoms of OSA and a polysomnography recorded 6 months postoperatively revealed an AHI of 12.2. His BMI increased from 24.12 kg/m2 (>99th percentile) to 27.7 kg/m2 over the same time period. He underwent a tonsillectomy and adenoidectomy without improvement in his OSA symptoms. A repeat nasoendoscopy one year after his second grafting procedure revealed a significantly enlarged fat graft obstructing his pharyngeal airway. He was taken to the operating room for excision of the fat mass from his posterior pharynx (Figure 4). This improved his OSA and did not impact his speech outcome.
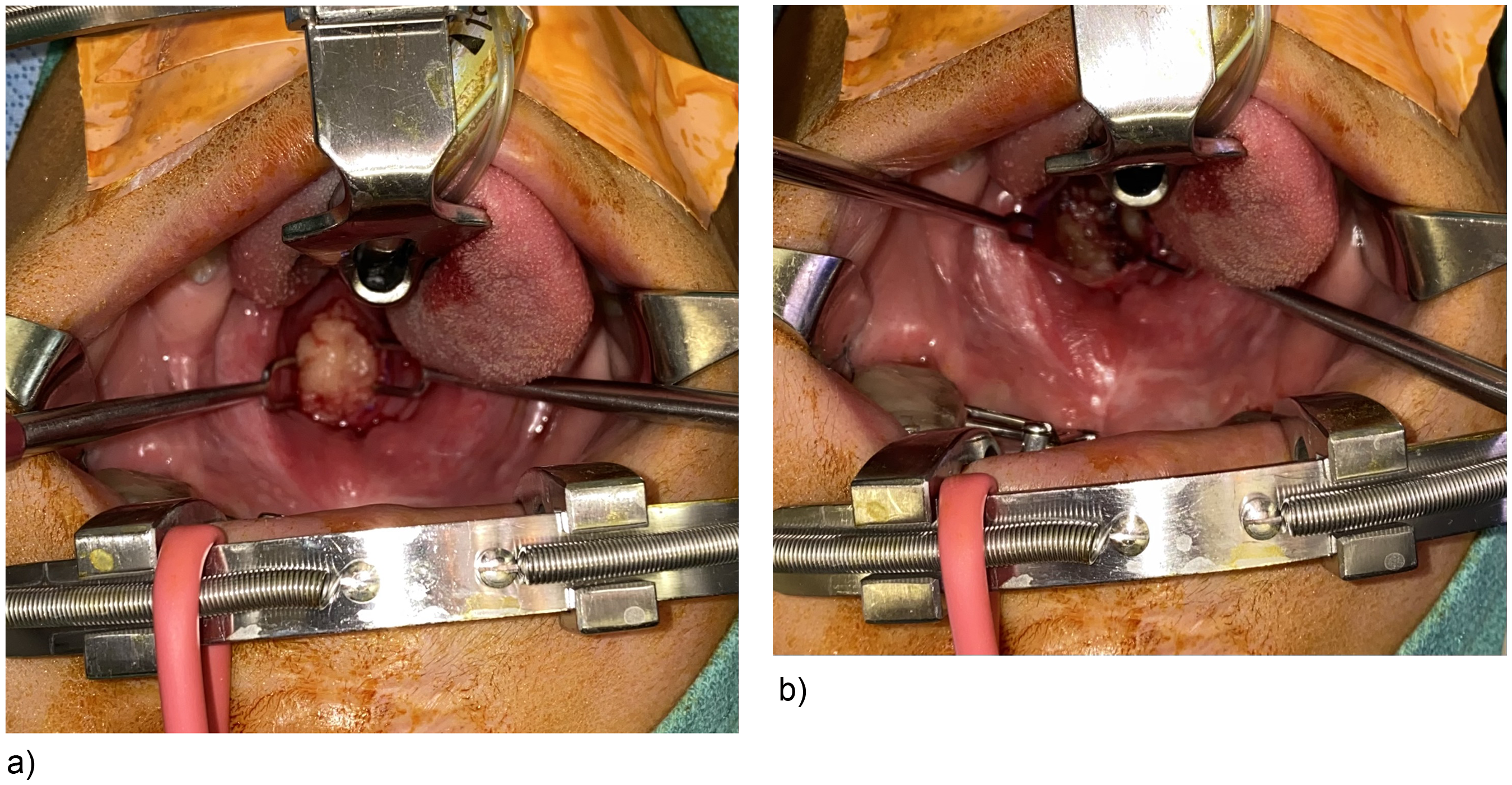
(a) A vertical incision was made on the posterior pharyngeal wall revealing a large, protrusive mass that exceeded the volume of fat injected. (b) The fat was excised to open the velopharyngeal sphincter.
Discussion
Obstructive sleep apnea is a known risk factor of surgery performed for the treatment of VPI. Overcorrection of the velopharyngeal sphincter size can lead to a critical narrowing and subsequent compression of the upper airway leading to restrictive breathing and obstructive apnea events. This complication is well documented following pharyngeal flaps and DSP surgery leading many to abandon these pharyngeal techniques in favor of palatal lengthening procedures. Guided by direct visualization on nasoendoscopy, targeted autologous fat grafting to the posterior pharyngeal wall has long been considered a less invasive and safe alternative for closing small to moderately sized velopharyngeal gaps. 24 A recent systematic review of 20 studies concluded that a mean injection volume of 6.3cc of fat can result in significant improvement in perceptual speech assessment and reduction in velopharyngeal gap size with a 2.7% summative complication rate among 594 patients. Development of OSA specifically was reported in only 3 patients. 13 In our own series of 76 patients treated over the last 15 years with a mean fat injection volume of 10.4cc (range 2.0-31.5 cc), we found a 4% incidence of OSA.
However, some published studies report mixed results and raise concerns regarding the safety and efficacy of fat grafting. In a retrospective study of 28 patients who underwent autologous fat grafting for VPI, Phua et al reported that 3 patients (11%) developed severe OSA requiring the surgical removal of the engrafted fat. 25 All patients were found to have diffuse overgrowth of the fat in the area injected. The authors further highlight that while improvement in hypernasality was found in 63% of patients, only 25% had complete resolution of hypernasality. Factors associated with success were a preoperative velopharyngeal gap size of less than 0.5 cm2, and the authors advocate for stringent criteria in determining patient candidacy for fat grafting. A more direct corollary to our own case series, Teixeira et al published a case report of a patient who developed severe OSA after 2 rounds of fat grafting for a total volume of 12cc. 26 The patient had a significant increase in BMI over this time period. The patient required 2 debulking procedures to achieve resolution of his OSA, and the authors posited that the fat hypertrophy observed intraoperatively was related to his generalized weight gain. Interestingly, all 4 cases previously described involved patients who had syndromes associated with hypotonia. This was not the case for any of our patients.
The association between weight gain and development of fat hypertrophy, however, is consistent with our series. In the first case, the patient's BMI increased from the 28th to the 96th percentile over 2 years following the second fat grafting procedure, which coincided with symptom onset and an increase in AHI from 4.5 to 59.5 on polysomnography. In the remaining cases, fat grafting was chosen as a less invasive intervention precisely because the patients’ elevated preoperative BMI (>95th percentile) placed them at a higher risk for developing OSA. Both patients continued to gain significant weight postoperatively resulting in obstructive symptoms. While weight gain alone in pediatric patients can lead to OSA, 27 our intraoperative findings suggest that interval hypertrophy of our engrafted fat contributed significantly to sleep-disordered breathing. In all 3 patients, the volume of fat excised during debulking procedures greatly exceeded the total volume initially injected.
These findings were also seen on MRI and CT scan images, which showed significant overgrowth of the adipose tissue. Adipocyte hypertrophy is the primary physiologic response to obesity to accommodate the increased storage demand induced by higher circulating lipids seen in high-fat feeding conditions.28,29 This process is orchestrated by a complex interaction of cell signaling adipokines, peroxisome proliferator-activated receptor gamma, and other signaling molecules. 30 Adipocytes remain responsive to these signaling pathways even after transplantation. Previous studies have shown that adipocytes retain the behavior of the donor site and fat grafts fluctuate in size with associated weight changes.31–33 In our case series, the superficial fat of the abdomen, which is particularly susceptible to hypertrophy with systemic weight changes, was used as the donor site for all patients. It is unclear if similar results would be expected in cases where the buttocks or flanks are used as donor sites.
Most studies report some degree of improvement in speech outcomes following autologous fat grafting for VPI, but there is significant variability with some reporting persistent hypernasality, nasal turbulence, and poor perceptual speech assessments.19,21,24,34 This can be not only attributed in part to patient selection and technique but also highlighted the unpredictability of fat grafting itself with respect to retained graft volume and precision of placement. Some degree of fat resorption can be expected though the exact amount is variable and depends on several factors including the harvesting and injection techniques as well as the environment of the recipient site. It is therefore challenging to determine precisely how much fat must be injected to adequately address the degree of VPI. Likewise, the precision of the fat placement can be challenging as the fat injected can easily migrate under pressure in the cranial and caudal direction within the retropharyngeal space. Imaging studies obtained in our patient series demonstrated that fat had migrated as it advanced into areas beyond the initial target region. In one patient, the lipomatous mass extended down to the level of the epiglottis where the upper airway is narrower, which exacerbated the obstructive symptoms. Small volume injection can help mitigate this risk.
Preoperative nasoendoscopy provides a visual guide for identifying the anatomic location of the velopharyngeal gaps but this itself lacks precision. Multiple studies have shown that despite these efforts, persistent gaps remain in postoperative nasoendoscopy leading to repeat fat injections.19,21 This is reflected in the most recent systematic review by Mirsky et al 13 who cite an average of 1.3 fat grafting sessions per patient to achieve the desired functional improvement. As a result, we have felt that overcorrection was prudent to ensure adequate graft survival and to optimize speech outcomes postoperatively. This is evident in the volume of fat injected in the cases presented, which is significantly higher than the reported norm. In spite of this, 19% of patients in our series (15/76) had persistent velopharyngeal gaps and hypernasality postoperatively, and additional grafting was performed. For the majority of these patients (87%), this resulted in additional speech improvements without development of OSA, suggesting there is no direct correlative effect between the number of fat injections and OSA complications. However, when combined with significant weight gain, complications can arise in a subset of patients.
As our case series have demonstrated, there is a meaningful risk associated with overcorrection to be taken into consideration, as the autologous graft will continue to grow and change over time. Several years separated the fat grafting procedures from the onset of obstructive symptoms, emphasizing the importance of long-term monitoring of these patients for OSA. All patients showed improvement in symptoms following the excision of the fat graft. In removing the hypertrophied fat, we excised only enough graft to restore the appropriate size of the velopharyngeal port rather than leaving a depression that could lead to relapse of VPI symptoms. None of the patients developed hypernasality or worsened speech outcomes as a result of fat graft excision.
There are nonautologous injectable materials available that are not affected by weight changes and present a potential alternative solution to avoid this complication. Hyaluronic acid, calcium hydroxyapatite, Gortex, alloderm, and silicone have all been described for use in posterior pharyneal wall augmentation for VPI. 7 In a recent systematic review, complete velopharyngeal gap closure was achieved at a higher frequency with injection of synthetic materials compared with autologous fat, 35 likely due to reduced material resorption. However, synthetic materials have a higher risk of foreign-body reaction, infection, and extrusion and have limited long-term outcomes data. 36 Given the young age of these patients, we prefer to use autologous tissues whenever feasible. Nonetheless, there may be a limited role for these materials in patients at high risk for OSA where the potential of graft hypertrophy is a consideration.
The 3 cases in this series reinforce the sentiment raised by Phua et al that care must be taken in adjudicating the maximum injection volume in patients who are at higher risk for developing OSA. 25 Overcorrection should be avoided and multiple injections may exacerbate the risk of complications, especially in obese patients. Patients and their families should be counseled that posterior pharyngeal wall augmentation with fat grafting can be expected to improve but not necessarily resolve speech resonance in select patients and that any weight gain following surgery may affect the engrafted fat and increase the risk of developing OSA. Buccal myomuosal flaps have become our preferred treatment of VPI in most patients for its greater reliability and predictability in outcomes and lower risk profile. We reserve low-volume fat grafting as a secondary procedure for persistent velopharyngeal gaps and hypernasality following buccal myomucosal flaps in patients who are at low risk for developing OSA. We have rarely found this necessary since adopting the buccal myomucosal flap for treatment of velopharyngeal dysfunction.
Conclusion
Autologous fat grafting to the posterior pharyngeal wall for treatment of VPI can be an effective treatment option. However, weight changes over time can lead to hypertrophy of engrafted fat, which can result in clinically significant OSA requiring graft excision. Risk factors for increased weight gain in specific patient populations may help guide treatment and influence grafting volume.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Approval was obtained for this study from the Internal Review Board (IRB) in accordance with ethical guidelines for conducting clinical research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.