
Abstract
Objective
To compare the oral hygiene and gingival health of children with and without cleft lip and palate.
Design
Cross-sectional comparative study.
Setting
Institutional tertiary referral hospital.
Patients/Participants
This study was conducted on 108 children aged 6 to 12 years, divided into 3 groups: Group 1 = children with cleft lip and alveolus with or without cleft palate, unilateral or bilateral (n = 36, 22 boys and 14 girls, aged 8, 39 ± 1.61 years), Group 2 = children with isolated cleft palate (n = 36, 8 boys and 28 girls, 8.11 ± 1.88 years); and Group 3 = children without clefts (n = 36, 18 boys and 18 girls, 8.53 ± 1.33 years).
Main Outcome Measures
The clinical parameters evaluated were Gingival Index (GI) and Patient Hygiene Performance (PHP) Index. analysis of variance and Kruskal–Wallis tests were used to evaluate intergroup differences. Correlations between the variables age, PHP Index and GI were assessed by the Spearman correlation (P < .05).
Results
The results demonstrated no statistically significant difference between the three groups for the PHP index (P = .126). There was also no intergroup difference for GI (P = .418).
Conclusions
No difference for the gingival status was observed between children with cleft lip and palate and with isolated cleft palate. Children with oral clefts present adequate gingival status compared to noncleft children.
Introduction
Plaque-induced gingivitis is an inflammation of the gums resulting from the action of bacterial plaque located at the gingival margin and has been considered the most common form of periodontal disease. Epidemiological data have shown that plaque-induced gingivitis is prevalent in all dentitions of populations. The clinical signs and symptoms of gingivitis may vary between patients as well as between sites of the same dentition. Clinical signs include increased gingival contours due to edema or fibrosis, transition to red and/or red-gray, elevated sulcus temperature, bleeding on touch and increased gingival exudate. 1
Prevention of this disease is directly related to adequate control of dental plaque. 1 In daily practice, complete removal of dental plaque by mechanical means remains limited and may be incomplete due to limited dexterity and precision of the patient. In addition, oral hygiene devices allow only limited access when local conditions exist, 2 such as anatomical factors and the use of orthodontic appliances.
In patients with cleft lip and palate, the presence of the cleft itself, the presence of scar frenulum and bridles, dental anomalies, gingival recession, and crowding, which can make hygiene difficult, increasing the risk of plaque accumulation and incidence of plaque-induced gingivitis.1,3–8 Reports on the gingival health of children with cleft lip and palate are currently limited. Most studies refer to the periodontal condition of adult patients3–7,9 or in children and young adults with wide age ranges,10–15 encompassing different types of fissures in the same group, 16 with no control group, 17 or with a reduced sample.11–13
Studies related to gingival health among different types of clefts in children still in mixed dentition, including a control group, are still scarce in the literature. In the early phase of mixed dentition, orthodontic treatment of children with clefts begins, aiming at aligning the maxillary segments for subsequent grafting on the alveolar ridge, and an adequate oral health condition is necessary for successful cleft rehabilitation. 18
In this sense, considering the importance of oral hygiene for maintaining gingival homeostasis, it is imperative to analyze the changes in gingival tissues in patients with cleft lip and palate. This allows planning dental care, providing not only curative dental treatment but also preventive therapies. 1 Therefore, the present study aimed to compare the oral hygiene and gingival status of children with and without cleft lip and palate. The null hypothesis is that children with cleft lip and palate have worse oral hygiene and gingival health when compared to children without cleft.
Patients and Methods
Ethical Aspects
This study was approved by the Research Ethics Committee of institution (CAAE: 55015016.6.0000.5441).
Patients
The sample size of the study was calculated with a power of 80% and an alpha error of 5%, based on the results of the epidemiological evaluation of the periodontal condition (prevalence and severity) in individuals with cleft lip and palate. 6
The sample consisted of 108 children aged between 6 and 12 years of both sexes, divided into 3 groups: Group 1 (n = 36): patients with cleft lip, ridge and palate, Group 2 (n = 36): patients with cleft palate, and Group 3 (n = 36): patients without cleft (control).
The selected patients with cleft lip and palate (Groups 1 and 2) were enrolled at the institutional tertiary referral hospital. The control group patients (Group 3) were recruited at the Orthodontics Clinic of the institution.
Exclusion criteria comprised the presence of other congenital anomalies, systemic disorders, use of fixed orthodontic appliances, use of antiinflammatory or anticonvulsant drugs, calcium blockers, or any other drug that might interfere with the study results. Other congenital anomalies could have a systemic and local influence on gingival inflammation and the patient's hygiene performance. Therefore, patients with concomitant disorders were excluded to avoid confounding factors.
Clinical Parameters
All examinations were performed by a single examiner who was calibrated by evaluating 10 children, with an interval of 10 days, in a dental chair with good lighting, using a dental mirror and an exploratory probe. The Kappa coefficient was used to assess the reliability of all data collected, 19 and the agreement was greater than 85%.
The method for evaluating gingival tissue used in this study was the Gingival Index (GI). 20 The evaluation was performed at 6 sites of all teeth: distobuccal, vestibular, mesiobuccal, distolingual, lingual, and mesiolingual. The criteria for evaluating the GI are: 0 = normal gingiva; 1 = incipient inflammation: slight change in color and edema, absence of bleeding on probing; 2 = moderate inflammation: reddish, edematous, and shiny gingiva, bleeding on probing; 3 = severe inflammation: tendency to spontaneous bleeding.
According to the indices obtained, resulting from the arithmetic mean of each tooth, gingivitis was classified as incipient when the degree was 0.1 to 1.0; moderate from 1.1 to 2.0; and severe between 2.1 and 3.0.
The oral hygiene assessment was verified by the Patient Hygiene Performance (PHP) Index. 21 To demonstrate the biofilm, a 0.6% malachite green solution was used. The following teeth were evaluated: upper right first molar, upper right central incisor, upper left first molar, lower left central incisor, lower left first molar, and lower right first molar. The clinical crown is subdivided longitudinally into mesial, middle, and distal thirds. The middle third is subdivided horizontally into gingival, middle, and occlusal thirds. The final result is the arithmetic mean of the teeth evaluated.
Patients received professional prophylaxis after the examinations and oral hygiene instructions for the children individually, as well as guidance for those responsible after plaque was detected.
Statistical Analysis
To verify normality, each group was individually subjected to the Kolmogorov–Smirnov test. In the comparison between groups and within groups, analysis of variance (ANOVA) was used for the PHP Index, the only index that passed the normality test, and the Kruskal–Wallis test was used for the GI.
The pairwise comparison test was also applied to the three groups. For correlations between the variables age, PHP Index and GI, the Spearman correlation test was used. A 5% significance level was adopted.
Results
One hundred and eight children aged 6 to 12 years, divided into 3 groups, were evaluated. Group 1 consisted of 36 children with cleft lip and alveolus with or without cleft palate, unilateral or bilateral, being 22 boys and 14 girls, with a mean age of 8.39 ± 1.61 years. Group 2 consisted of 36 children with isolated cleft palate, being 8 boys and 28 girls, with a mean age of 8.11 ± 1.88 years. Group 3 consisted of 36 children without clefts (18 boys and 18 girls) with a mean age of 8.53 ± 1.33 years (Table 1).
Sample Characterization.

In the PHP Index evaluation, Group 3 presented the highest value (4.30 ± 0.52), followed by Group 2 (4.15 ± 0.63) and Group 1 (4.0 ± 0.65), with no statistically significant difference between them (P = .126, ANOVA, P < .05).
In the GI, the means obtained were 0.09 ± 0.08 for Group 1, 0.08 ± 0.08 for Group 2 and 0.07 ± 0.09 for Group 3. According to the GI values, 88.8% of the children in Group 1 had incipient gingivitis (GI = 0.1-1) and 11.02% had normal gingiva (GI = 0). In Group 2, 88.8% of the children had incipient gingivitis and 11.02% had normal gingiva. Among the children in Group 3, 83.3% had incipient gingivitis and 16.7% had normal gingiva. In the comparison between the groups, there was no statistically significant difference (P = .418).
In the correlation between groups and age, the results demonstrated that the higher the age, the higher the GI value, with a statistically significant difference (P = .019). In the intragroup evaluation, there was a correlation between age and GI only in Group 3 (P = .006) (Tables 2 and 3).
Overall Correlation Between the Variables PHP, GI, and Age (Spearman Correlation, P < .05).
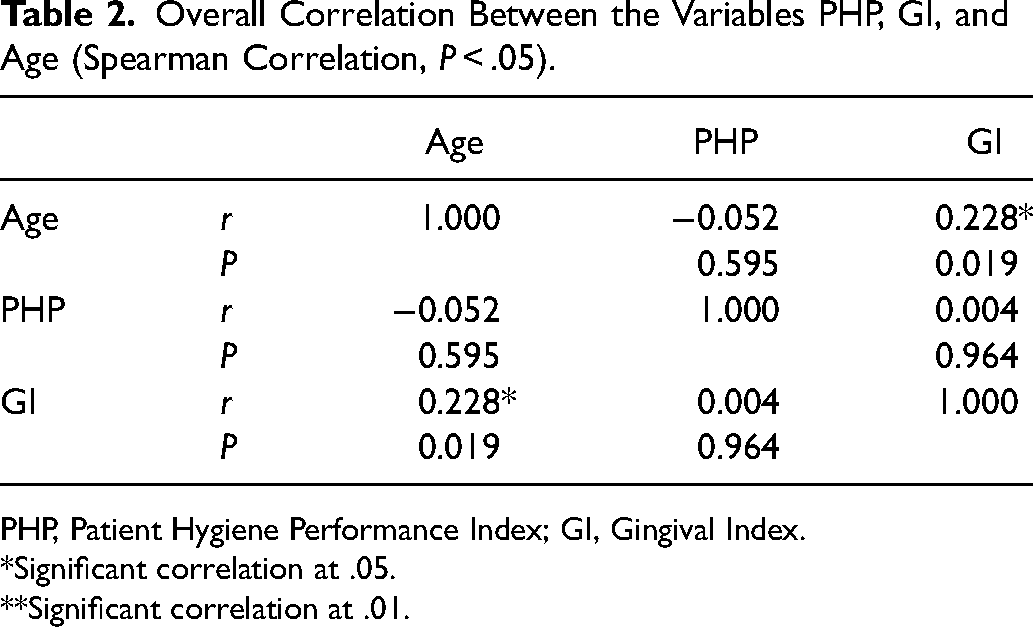
PHP, Patient Hygiene Performance Index; GI, Gingival Index.
Significant correlation at .05.
Significant correlation at .01.
Each Group Correlation Between the Variables PHP, GI, and age (Spearman Correlation, P < .05).
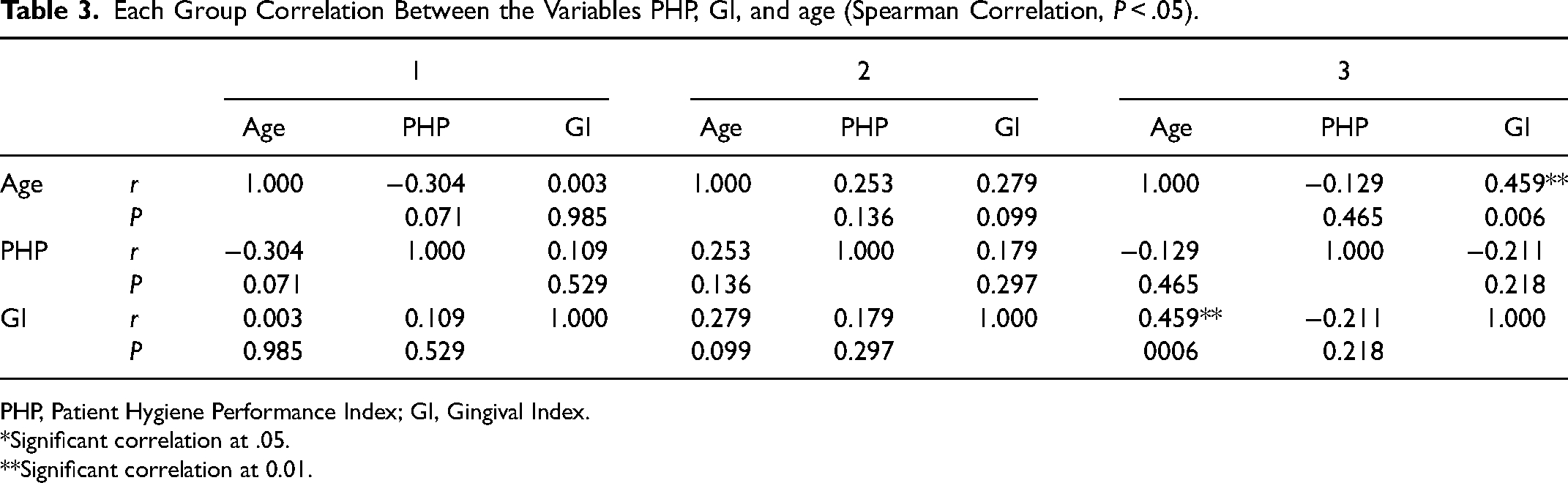
PHP, Patient Hygiene Performance Index; GI, Gingival Index.
Significant correlation at .05.
Significant correlation at 0.01.
Discussion
The main etiological agent of gingivitis is biofilm, which may be related to inadequate oral hygiene.2,22–24 In this study, there was a correlation between the presence of dental plaque and gingival inflammation only in Group 3 and there was no statistically significant difference in the parameters evaluated between the groups.
It is well established in the literature that gingivitis is initiated and maintained by the presence of mature plaque deposits around the teeth25–28 and there is substantial evidence that several mechanical and chemical methods of plaque control can prevent gingivitis. 29
Provided that control is sufficiently thorough and performed at appropriate time intervals, tooth brushing and mechanical interdental cleaning procedures can reliably control plaque.
Nevertheless, considering the three groups studied, a prevalence of gingivitis was observed in more than 87% of children. Corroborating our results, other studies have reported a high prevalence of gingivitis ranging from 91% to 97.93%.30,31 It is suggested that children over 7 years have a high prevalence and severity of gingivitis, particularly due to puberty or the presence of mixed dentition.32–34
Regarding oral hygiene and prevalence of gingivitis, there was no significance between the 3 groups when evaluated by the PHP Index and GI. The results suggest that children with cleft lip and palate do not have worse oral hygiene compared to children without clefts. These data differ from other studies where children with cleft lip and palate had worse plaque and gingival inflammation scores.35–40 However, a similar result to the present study was found by Lucas et al. (2000) 10 who reported no significance in plaque and GI scores between children with and without cleft lip and palate.
It is suggested that there is a correlation between the most aggressive type of cleft and worse oral hygiene.41–44 This fact would be due to the difficulty encountered due to the anatomy of the cleft area, scars from cheiloplasty and bone graft surgeries, limited mobility of the lip, gingival hyperplasia, in addition to the fear of manipulating these tissues on the part of children and guardians.37,41,44–46 In this study, Group 1 consisted of children with the most complex types of cleft, which cause greater esthetic and functional impairment, including those with cleft lip and ridge and/or palate. Comparing this group with Group 2, which included only children with cleft palate, there was no significant difference in any index used in the evaluation of oral hygiene and gingivitis. These data agree with those found by Al-Wahadni et al. (2005) 40 and Pisek et al. (2014). 47
Given the existence of a relationship between periodontal disease and oral hygiene, from an epidemiological point of view, there has been a growing interest in experimental research and clinical investigations. Knowledge of the problem, its extent, severity, as well as the causal hypotheses is of great value for establishing prevention, control and treatment measures. Thus, the use of plaque indices has become increasingly frequent, and determining their discriminatory power is of great value. Given the scarcity of robust data evaluating the periodontal condition of children with cleft lip and palate with the inclusion of a control group, we used a large and representative sample with very close age ranges in order to standardize the sample.
The PHP is a qualitative index that can be quickly assessed, as it involves the assessment of only 6 teeth, unlike the other 2 indices that assess all teeth present. The plaque index requires more time, as it involves the use of an exploratory probe in the mesiobuccal, buccal, distobuccal, mesiolingual, lingual, and distolingual sites of all teeth, and therefore its application in children may be more complicated. The O’Leary Index 48 appeared to overestimate the presence of plaque, as it detects and considers any amount of stained plaque on the surface as present, thus grouping different oral hygiene conditions into a single score. A statistically significant difference was observed between Groups 1 and 3 in the assessment using the O’Leary Index (P = .026). The control group had the worst oral hygiene.
With the PHP Index, all groups presented an average score greater than 4.0, which is considered poor oral hygiene. In Group 1, 77.77% presented poor oral hygiene. Stec et al. (2007) 12 also found a score for dental plaque of over 70% in children with cleft lip, ridge and/or palate. In this sense, it should be considered that it is rare to observe an absolute absence of dental plaque in individuals, especially in children who already brush their teeth by themselves but do not have the manual dexterity to do so. A certain level of dental plaque is probably found in all individuals, and in many, it is clinically compatible with gingival health. 48
Despite the fact that the prevalence of gingivitis was high in both the cleft lip and palate group (88.8%) and the noncleft group (83.3%), both PHP and GI were within reasonable ranges. Thus, we can say that the oral health status in terms of gingival aspect is still good, but it can be improved by implementing comprehensive preventive programs as well as increasing awareness about gingival health and oral health in general, since the presence of gum disease is a major indicator for the later development of periodontal diseases and many other oral health-related diseases. 49
Comparing the three groups in terms of the presence of dental plaque, the control group had the worst average score in the PHP Index. It is worth noting that the institution referral hospital is a reference center for the treatment of individuals with cleft lip and palate, and although patients and their families are concerned about other aspects of the treatment (surgical, speech therapy, social, psychological, and nutritional), they do not neglect preventive dental care. This hospital focuses on dental care, with preventive and educational work being carried out from the first visits when the patient is still a baby.
In view of this, we can emphasize that the anatomical variation due to the presence of the cleft should not be considered a decisive factor in the gingivitis of children with cleft lip and palate. 50 Patients with cleft lip and palate present some anatomical and morphological conditions that facilitate the accumulation of plaque. These patients potentially present a tendency to worse oral hygiene and thus an increased risk of gingivitis. However, with regular oral hygiene guidelines, reinforced by a daily oral health maintenance program, it is possible to prevent gingivitis.
Conclusion
Based on these results, it is concluded that children with cleft lip and palate have similar oral hygiene and gingival condition when compared to children without cleft lip and palate. We reinforce the importance of an oral hygiene awareness and motivation program aimed at maintaining oral health.
Footnotes
Acknowledgments
The authors wish to acknowledge the Hospital for Rehabilitation of Craniofacial Anomalies and Bauru School of dentistry (University of São Paulo) for the support provided.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Research Ethics Committee of the Hospital for Rehabilitation of Craniofacial Anomalies of the University of São Paulo-HRAC-USP (CAAE: 55015016.6.0000.5441).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.