
Abstract
Objective
This study compares mandibular distraction osteogenesis (MDO) and tracheostomy in managing severe airway obstruction in patients with the Pierre Robin sequence (PRS).
Design
A systematic review and meta-analysis following PRISMA guidelines was performed. Literature searches were conducted across PubMed, ScienceDirect, Cochrane Library, Scopus, E.B.S.C.O., and Web of Science, including grey literature, covering studies until May 30, 2024. Study quality was assessed using the Newcastle-Ottawa Scale.
Patients
patients with Pierre Robin Sequence.
Interventions
Mandibular distraction osteogenesis (MDO) and tracheostomy.
Main Outcome Measures
Primary outcomes included airway management (tracheostomy avoidance for MDO, decannulation for tracheostomy) and feeding outcomes (G-tube placement). Secondary outcomes were hospital length of stay and associated costs.
Results
Thirteen studies were included. MDO and the MDO-first approach demonstrated significantly better airway outcomes (OR = 10.72, 95% CI = 1.97–58.44, p = 0.006; OR = 4.51, 95% CI = 2.61–7.79, p < 0.00001). MDO also reduced the need for G-tube placement (OR = 0.09, 95% CI = 0.04–0.18, p < 0.00001) and lowered hospital costs (MD = -47.90 thousand USD, 95% CI = -59.93 to −35.87, p < 0.0001). A shorter hospital stay was observed but was not statistically significant.
Conclusions
MDO offers better airway outcomes, lower G-tube placement rates, and reduced costs, making it a preferred option. Larger studies within the same syndromic status are needed to minimize confounding factors and validate these findings.
Keywords
Introduction
Pierre Robin sequence (PRS) is a congenital condition defined by micrognathia, glossoptosis, and airway obstruction, commonly linked to cleft palate. In more complex cases, PRS may correlate with supplementary congenital anomalies.1–3 Effective management of airway obstruction in these patients is critical, as insufficient intervention may lead to life-threatening complications and increased morbidity. Airway obstruction causes additional feeding difficulties, especially when combined with the existence of a cleft palate, increasing morbidity and death in patients with PRS.2,3
The degree of airway obstruction in PRS varies, with some instances requiring surgical intervention to ensure sufficient respiratory function. However, there are no universally accepted guidelines for managing airway obstruction in PRS, so treatment approaches are primarily determined by the surgeon's experience and the practices of their medical facility.1,3,4 Tracheostomy has historically served as the principal intervention for severe and persistent airway obstruction; however, it is associated with risks such as pneumonia and stomal granulation, which may result in further complications.5,6
Mandibular distraction osteogenesis (MDO) has developed as an alternative treatment, providing a physiological solution by targeting the anatomical basis of mandibular hypoplasia. By moving the mandible forward, MDO improves airway patency, potentially removing the need for a tracheostomy and related problems. Although further study is required to validate its definitive function in clinical practice, this developing method offers a potential option for managing airway congestion linked to PRS. 7
In many healthcare facilities, MDO has become the recommended surgical option for addressing severe airway blockage in patients with PRS. However, tracheostomy remains a viable option, having been used in roughly 10–15% of patients with PRS. 2 Tracheostomy is still the predominant treatment in some facilities due to surgeon training bias or a lack of experience with other surgical methods. 8
There currently needs to be a comprehensive systematic review or meta-analysis that directly compares the effects of these two treatment modalities in the PRS Population. Therefore, this study evaluates the effectiveness of mandibular distraction osteogenesis compared to tracheostomy in managing airway obstruction in patients with PRS.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines conducted this meta-analysis and systematic review. The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the identifier CRD42024574071. An examination of PROSPERO revealed that no additional registered protocols on this particular topic exist.
Search Strategy
A comprehensive search was performed using numerous electronic databases, including PubMed, ScienceDirect, Cochrane Library, Scopus, EBSCO (CINAHL, dentistry, and oral medicine), and Web of Science, as well as grey literature sources, including medRxiv and Scopus preprint databases. The search terms included “Pierre Robin Sequence,” “micrognathia,” “obstructive sleep apnea,” “mandibular distraction,” and “tracheostomy,” as well as any applicable MeSH terms. The investigations were completed by May 30, 2024. A detailed description of the search strategy is available in Supplementary Table 1.
The titles and abstracts of the identified papers were evaluated, and the full texts of possibly relevant articles were reviewed to determine their eligibility for inclusion. Furthermore, all included studies’ reference lists were searched for other relevant publications, which were subsequently catalogued, retrieved, and reviewed for inclusion in this analysis.
Study Selection
All studies included in this review involved children with PRS clinical features characterized by micrognathia, glossoptosis, and airway obstruction, with or without cleft palate. Both syndromic and non-syndromic cases were considered, provided the patients underwent either MDO or tracheostomy within the same study. This study excluded patients with micrognathia or obstructive sleep apnea (OSA) who were not explicitly identified as having PRS.
The primary outcomes measured were airway outcomes and feeding outcomes, specifically the necessity for gastrostomy tube (G-tube) implantation. We defined successful airway outcomes as the patient's ability to breathe independently without assistive devices; thus, airway success in the MDO group was indicated by tracheostomy avoidance, and in the tracheostomy group, by successful decannulation.
Secondary outcomes were hospital length of stay and associated expenses. Costs were categorized as operating room (OR)-related expenses, other hospital-related costs (including hospitalization, diagnostics, and consultation fees), and total costs (combining OR and other hospital expenses).
Eligible studies were limited to prospective or retrospective cohort studies and randomized controlled trials (RCTs). Case series, case reports, meta-analyses, literature reviews, and articles without empirical data or systematic analysis, such as editorials, commentaries, and letters to the editor, were excluded. Non-English language studies were also excluded from the analysis.
Data Collection and Quality Assessment
Three independent reviewers (I.L.P, K.I, and R.P) conducted the literature search and assessed the relevance of full-text papers before agreeing on which research to include. In certain cases, the fifth reviewer (C.D.K.W) was brought in to settle disagreements through conversation. The third author (I.F.A) was responsible for writing, editing, and reviewing the article in English, as well as conducting the visualization work and paper resources. Data retrieved into Excel files included baseline study information (author, year of publication, study design, single or multicentre), patient demographics (sample size, age, gender, syndromic status), and study results.
For airway outcomes, dichotomous data were collected, focusing on tracheostomy avoidance in the MDO group and decannulation in the tracheostomy group. Similarly, data on the need for gastrostomy tube (G-tube) placement were extracted for feeding outcomes. Continuous variables, such as length of hospital stay and cost outcomes, were reported as mean and standard deviation. Cost data, including operating room (OR) costs, other hospital-related expenses (hospital stay, diagnostic tests, and consultations), and total costs, were converted to USD and adjusted for inflation using the consumer price index (CPI). As cost analysis parameters varied across studies, hospital stay, diagnostics, and consultation fees were combined under “other hospital-related costs.” The total cost was calculated by summing OR-related and other hospital-related expenses. Qualitative analysis was performed for data that were too heterogeneous for quantitative synthesis.
Two reviewers (K.I and R.P) independently assessed the methodological quality utilizing the Newcastle-Ottawa Scale (NOS). 9 Disagreements were addressed via discussion or by consulting a fifth reviewer (C.D.K.W). Studies rated 7–9 stars were classified as high-quality, 5–6 stars as good quality, 3–4 stars as satisfactory, and 0–2 stars as unsatisfactory.
Statistical Analysis
The statistical analyses were performed with version 5.4 of Review Manager (RevMan). Quantitative data, such as impact sizes for airway and feeding outcomes, were presented as odds ratios (OR) with matching 95% confidence intervals. The length of hospital stays, and cost outcomes were reported as mean differences (MD) accompanied by 95% confidence intervals (CI). A p-value below 0.05 was taken to be statistically significant. The I² statistic was utilized to assess heterogeneity among the studies, with values exceeding 50% signifying substantial heterogeneity. A random-effects model was utilized for data exhibiting substantial heterogeneity to address study variability.
Results
Studies Characteristics
A total of 12.928 articles were identified. After eliminating duplicates, 7819 studies remained for abstract and title screening. Sixty-one studies were subjected to a full-text examination, but only 52 were retrieved. Twelve studies remained after an additional 40 were eliminated after the full-text examination. Reviewing the reference lists revealed one additional article, resulting in 13 studies being considered for the overall evaluation (Figure 1).
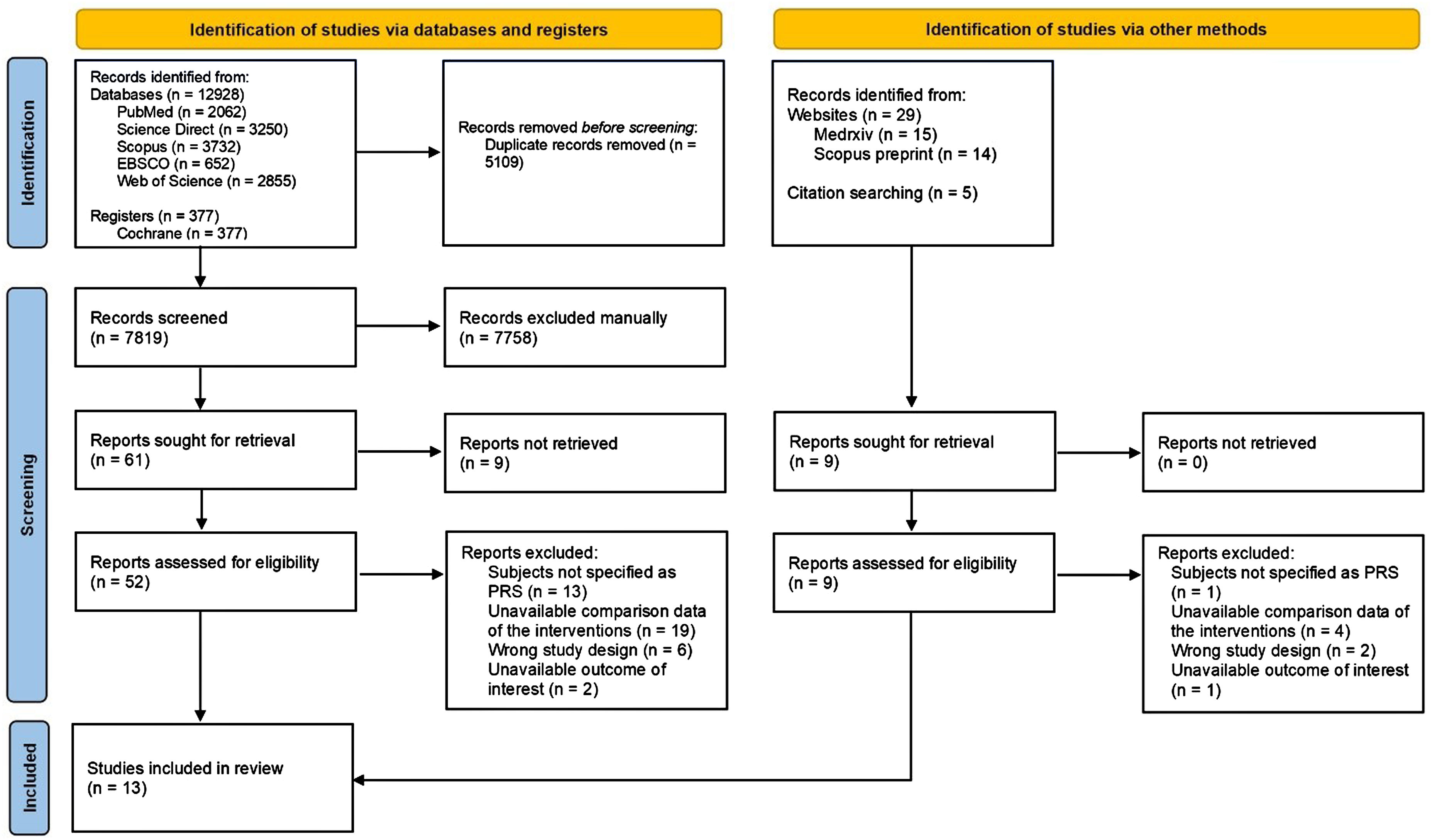
PRISMA flow diagram data added to the PRISMA template (from page mj, mcKenzie je, bossuyt pm, boutron I, Hoffmann tc, mulrow cd, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71) 9 under the terms of the Creative Commons Attribution License. Figure is available in color online only.
All studies were retrospective cohorts (n = 13), with the majority done in the United States (n = 10), and the rest were from Canada (n = 2) and the Netherlands (n = 1). Most of the studies were conducted in a single-centre setting (n = 12), with the remaining in a multicentre setting (n = 1). The number of studies in which the outcomes were able to be analysed is as follows: Airway outcomes in MDO vs tracheostomy and MDO-first vs tracheostomy-first, n = 2 and 8, respectively; feeding outcomes, n = 3; hospital length of stay, n = 3; cost outcomes, n = 2. Most of the studies were very good quality (n = 12), and the remaining was good quality (n = 1) (Supplementary Table 2).
Cohort Characteristics
A total of 591 patients were included in the analysis: 305 patients in mandibular distraction osteogenesis (MDO) group, 143 patients in tracheostomy group, and 177 patients in tracheostomy followed by MDO group. The sex distribution was reported in ten studies, indicating that 54.02% (262 out of 485) of the patients were male. Patients in the tracheostomy group were younger, with a mean age of 1.07 months (ranging from 0.45 to 1.71 months). In contrast, MDO group had an older mean age of 6.53 months, with a broader age range of 1.55 to 34 months. Notably, patients who underwent MDO following tracheostomy had an even older mean age of 25.35 months (ranging from 3.59 to 46 months). The syndromic distribution between groups was quite comparable, with a slightly lower proportion of syndromic patients in the MDO group. In the MDO group, 11 studies reported data, with 103 patients (42.39%) identified as syndromic. In the tracheostomy group, seven studies indicated that 75 patients (52.45%) were syndromic. In the tracheostomy followed by MDO group, five studies reported that 55 patients (59.78%) were classified as syndromic. A summary of the cohort characteristics is provided in Table 1.
Baseline Data and Demographics.
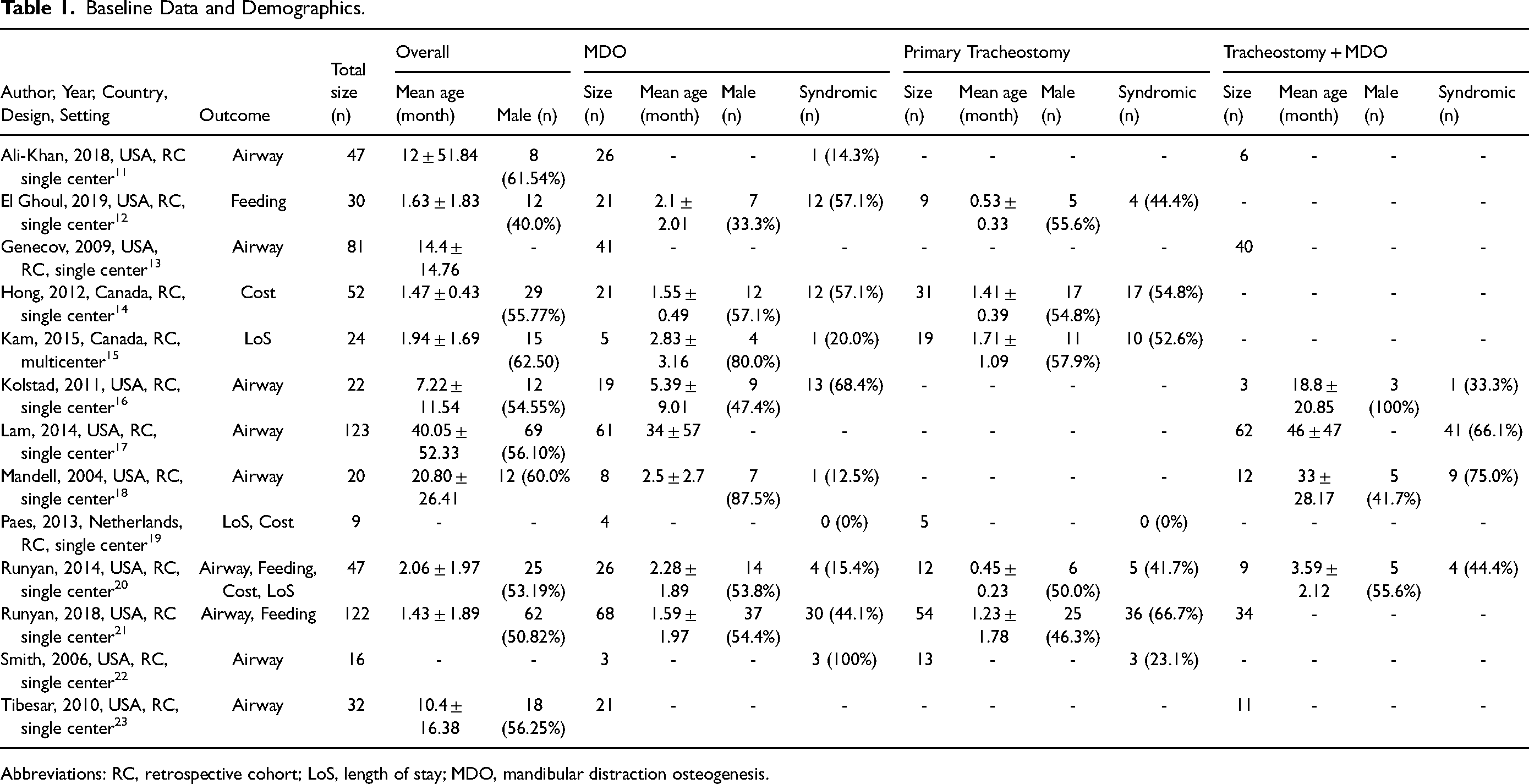
Abbreviations: RC, retrospective cohort; LoS, length of stay; MDO, mandibular distraction osteogenesis.
Primary Outcomes
Airway Outcomes
Two studies (n = 53) compared MDO vs. tracheostomy airway outcomes. MDO showed significantly higher success than tracheostomy (OR = 10.72, 95% CI = 1.97–58.44, p = 0.006, I2 = 49%) (Figure 2a). When comparing success in population with MDO and tracheostomy followed by MDO, we obtained eight studies (n = 415). Similarly, the MDO-first group showed significantly better outcomes than the tracheostomy-first (OR = 4.51, 95% CI = 2.61–7.79, p < 0.00001, I2 = 4%) (Figure 2b). Funnel plot analysis revealed no risk of publication bias (Figure 3).
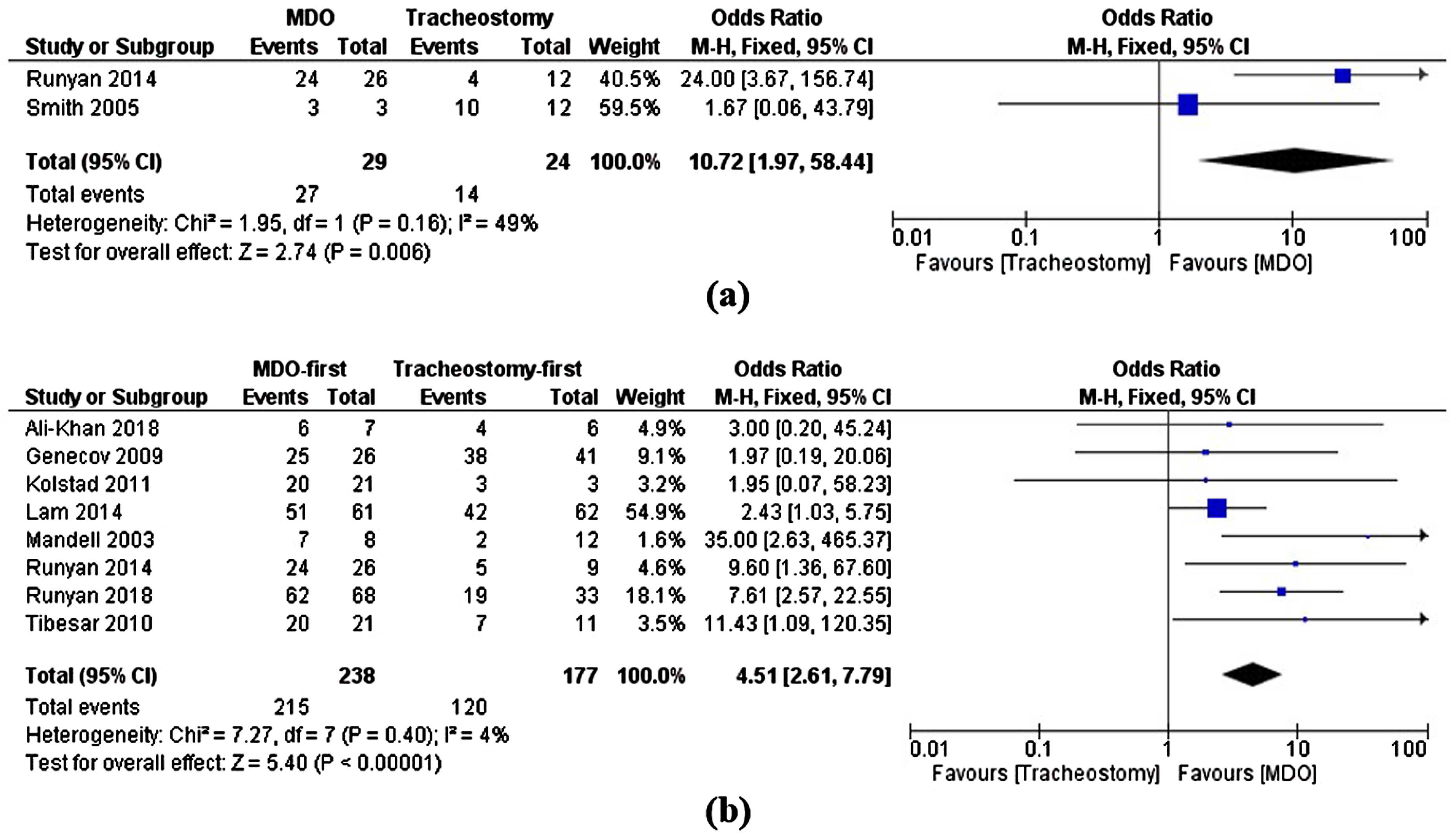
(a) Airway outcomes in MDO vs tracheostomy, measured by avoidance of tracheostomy in MDO and natural decannulation rate in tracheostomy; (b) airway outcomes in MDO-first vs tracheostomy-first, measured by avoidance of tracheostomy in MDO and decannulation rate in tracheostomy.
Feeding Outcomes
Three studies (n = 190) reported the rate of G-tube placements. MDO was shown to have significantly lower rates of G-tube placements compared to tracheostomy (OR = 0.09, 95% CI = 0.04–0.18, p < 0.00001, I2 = 0%) (Figure 4).
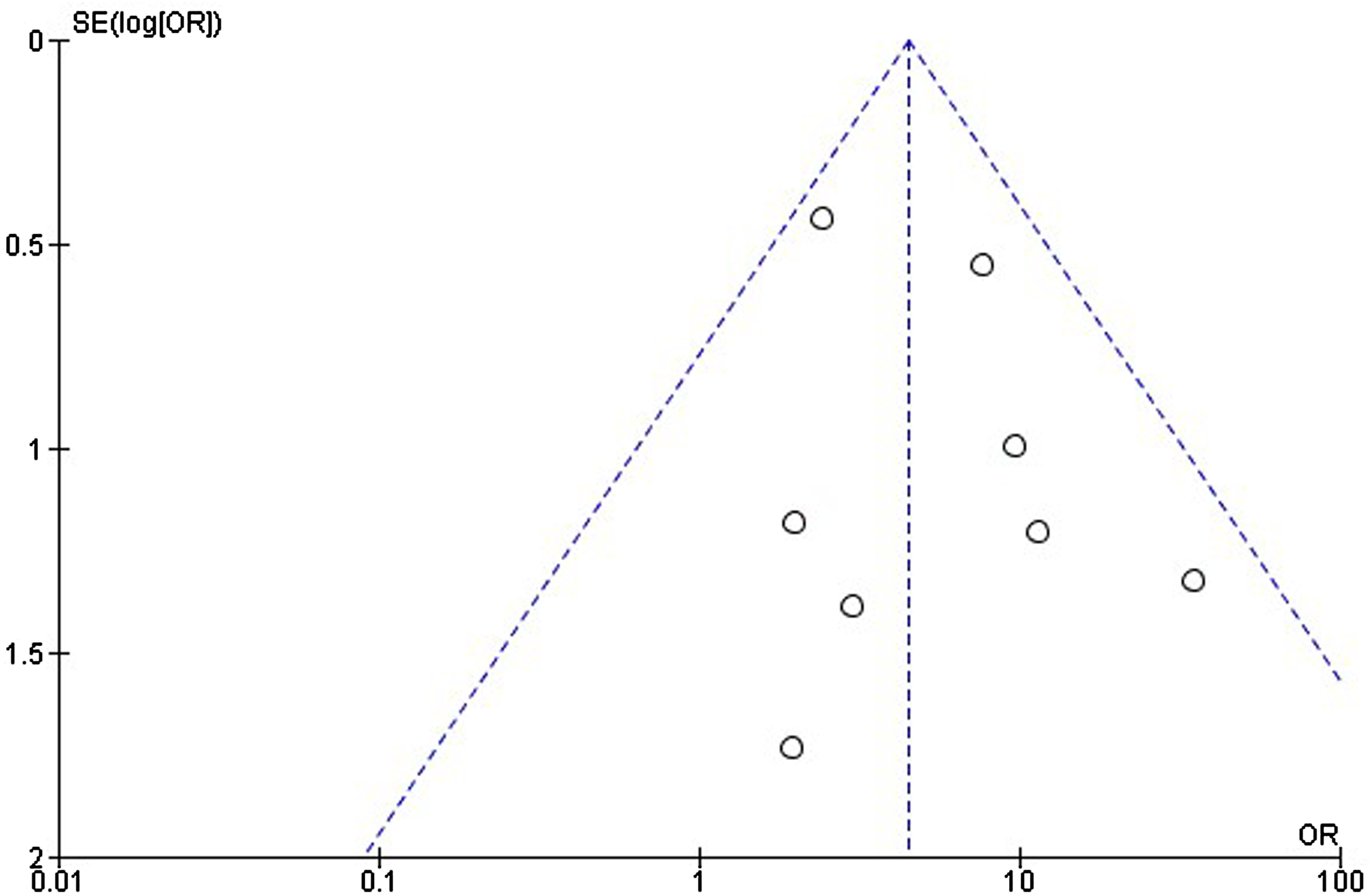
Funnel plot comparison of airway outcome in MDO-first vs tracheostomy-first group.
Secondary Outcomes
Hospital Length of Stay
Three studies (n = 71) reported hospital length of stay in days. Compared to tracheostomy, MDO has shown a shorter hospital length of stay but is not significant (MD = -44.88, 95% CI = -95.94 to −6.17, p = 0.08, I2 = 94%) (Figure 5a). The analysis detected high heterogeneity.
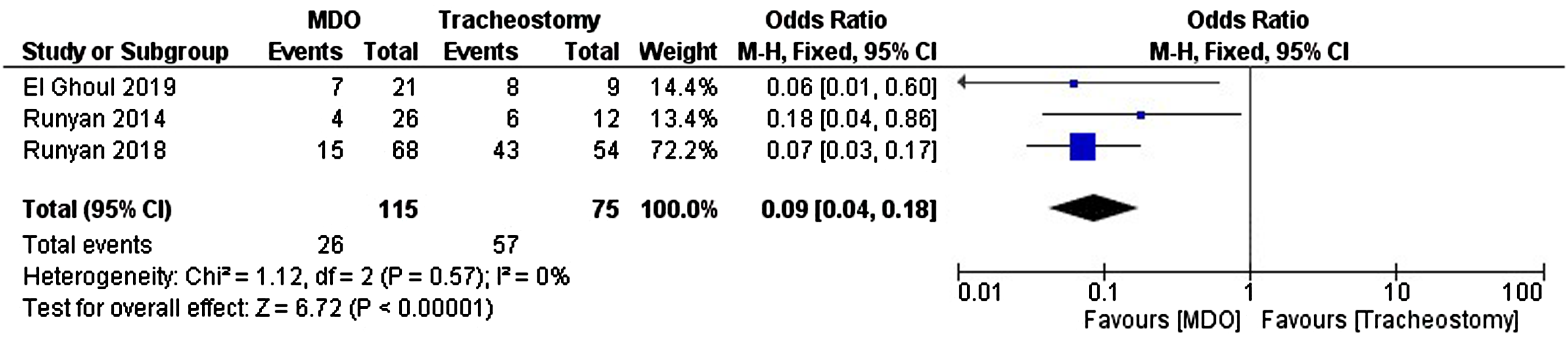
Feeding outcomes in MDO-first vs tracheostomy-first, measured by rate of gastrotomy-tube placements.
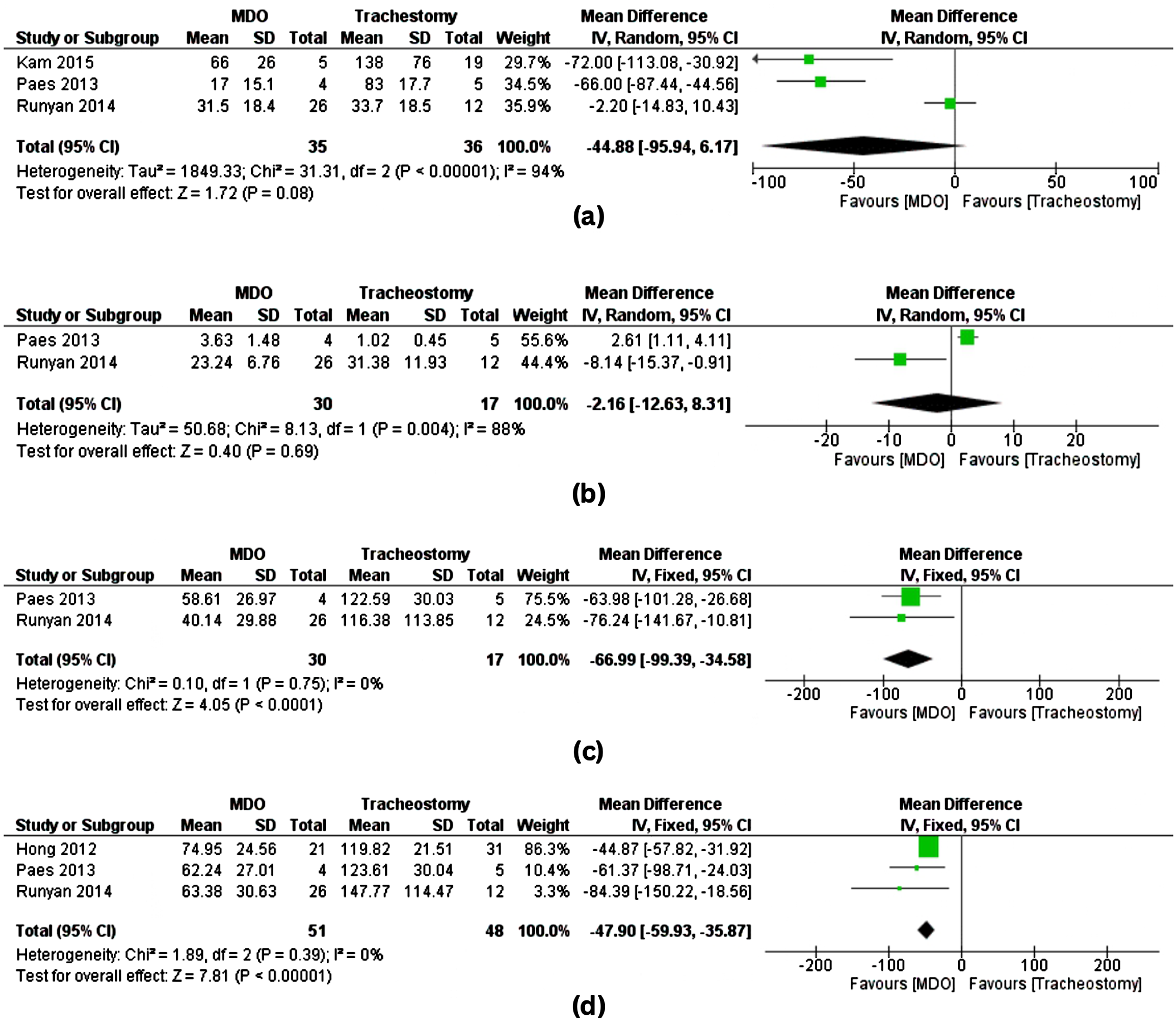
(a) Hospital length of stay in MDO vs Tracheostomy; (b) OR-related cost in MDO vs tracheostomy (in thousand USD); (c) Other hospital-related cost in MDO vs tracheostomy (including hospital stay cost, diagnostics, consultation fees) (in thousand USD); (d) Total cost in MDO vs Tracheostomy (total of OR-related cost and other hospital related cost) (in thousand USD).
Cost Outcomes
Two studies (n = 30) reported OR-related and other hospital-related costs, while three (n = 51) reported total costs in MDO and tracheostomy. All data were converted to USD (adjusted with CPI inflation) and presented as thousand USD. Our analysis found no significant difference in OR-related costs between the two interventions, with high heterogeneity observed (MD = -2.16, 95% CI = -12.63 to −8.31, p = 0.69, I2 = 88%) (Figure 5b). However, in other hospital-related costs, which include hospital stay cost, diagnostics, and consultation costs, MDO has significantly lower charges than tracheostomy (MD = -66.99, 95% CI = -99.39 to −34.58, p < 0.0001, I2 = 0%) (Figure 5c). The total cost is also significantly lower in MDO (MD = -47.90, 95% CI = -59.93 to −35.87, p < 0.0001, I2 = 0%) (Figure 5d).
Discussion
The Pierre Robin Sequence is now appropriately classified as a sequence of developmental abnormalities, where an initial defect initiates a chain of subsequent events leading to additional abnormalities. The primary defect, micrognathia, results in glossoptosis and airway obstruction. 10 The posterior positioning of the tongue acts like a ball valve, obstructing the airway during inspiration. 11 This small mandible may arise from a congenital growth abnormality, either as an isolated condition or as part of a craniofacial syndrome. Factors such as oligohydramnios and multiple births can further restrict mandibular growth and impede normal head extension.11,12
Various surgical interventions are available for severe airway obstruction that does not improve with prone positioning or non-invasive ventilation. Mandibular distraction osteogenesis (MDO) involves surgically creating a gap in the mandible, gradually widening over several weeks. This process allows for new bone formation in the gap, effectively lengthening the mandible and advancing the tongue. 7 MDO offers significant advantages, including the definitive correction of micrognathia and alleviation of airway obstruction and feeding difficulties.13,14 However, it is a complex procedure requiring specialized skills and experience, which limits the number of trained surgeons available to perform it.13,15 Complications associated with MDO can include device failure, surgical site infections, dental injury, and temporomandibular joint (TMJ) ankylosis.16,17 Moreover, while MDO effectively addresses upper airway obstruction, it is less beneficial in cases with concurrent lower airway abnormalities or central apnea. 18
On the other hand, tracheostomy bypasses the obstruction by creating a permanent opening in the trachea to stabilize the airway. In some patients, it may provide a temporary solution while awaiting natural mandibular growth. Tracheostomy can also be a lifesaving intervention for complex patients who are ineligible for MDO, such as those with central apnea, multilevel airway obstruction, neurological abnormalities, or as a permanent solution for individuals unresponsive to other surgical treatments.3,4,7,19,20 Tracheostomy is a well-established procedure that is widely accessible and familiar to many surgeons. 15 However, prolonged use of tracheostomy is associated with significant morbidity and mortality. Complications may include pneumonia, tracheitis, and tracheomalacia, as well as long-term consequences such as speech difficulties, increased incidence of gastroesophageal reflux disease, swallowing difficulties, granulation tissue formation, and subglottic and tracheal stenosis. These complications can impose a substantial burden on caregivers.2,4,21–23
To define success in airway outcomes, prior studies have used varying criteria. A review by Zaballa 24 suggested polysomnography as an objective measure, while other study assessed airway outcomes based on the need for supplemental oxygen, CPAP, or tracheostomy dependence. 25 Additionally, some studies defined success as the avoidance of tracheostomy or achieving decannulation.26–29 We chose the latter definition, as it reflects sustained relief from airway obstruction. For tracheostomy-dependent infants, the objectives include early decannulation to minimize the risks of morbidity and mortality associated with prolonged dependence.4,5,30,31 While polysomnography objectively measures obstruction severity, our goal extends beyond immediate relief; we aim to help patients achieve freedom from airway obstruction without reliance on assistive devices. This approach is particularly relevant given the substantial morbidity and burden associated with tracheostomy, despite its effectiveness in relieving obstruction.
This study compared the two interventions by evaluating airway outcomes based on tracheostomy avoidance in patients with MDO and the natural decannulation rate in those with tracheostomy. Although data are limited, this analysis indicates that MDO is associated with improved airway outcomes compared to primary tracheostomy.28,32 The natural decannulation rate observed in this study was 58.3%, aligning with findings from previous studies.4,21 Many patients may struggle to achieve decannulation because infants with inherent mandibular growth defects often lack the ability for spontaneous catch-up growth. If no additional interventions are implemented to address the underlying anatomical issues, this may lead to long-term dependence on tracheostomy.4,11
When expanding the analysis to compare outcomes between the MDO-first approach and the tracheostomy-first approach followed by MDO, the MDO-first group demonstrated significantly better outcomes than the tracheostomy-first group.25–27,29,32–35 Overall, tracheostomy was avoided in 90.4% of cases, with a decannulation rate of 67.8%. Previous studies have consistently supported the advantages of MDO in terms of preventing tracheostomy and improving decannulation in tracheostomized patients.14,18,36
Aside from the superior outcome of MDO, the poorer outcomes observed in the tracheostomy group may also be influenced by the increased complexity of patients within this group, suggesting that patient complexity could be a confounding factor. Factors contributing to this complexity include syndromic status and additional comorbidities such as multi-level airway obstruction, neuromuscular disorders, swallowing difficulties, undiagnosed central apnea, and degenerative encephalopathy.25–27,29,34 Additional airway procedures may be necessary in these complex cases to achieve successful decannulation. Our data suggest that even when tracheostomy is performed first, subsequent MDO can yield beneficial outcomes. However, limited data made it challenging to directly compare primary tracheostomy with tracheostomy followed by MDO. One study did find a higher decannulation rate in tracheostomized patients who subsequently underwent MDO than those who received primary tracheostomy (55.6% vs. 33.3%, respectively). 32
Airway difficulties in patients with PRS can also lead to feeding impairments. Gastrostomy tube (G-tube) placement is often necessary for prolonged oral feeding difficulties. 37 Pooled data indicate that mandibular distraction osteogenesis (MDO) is associated with significantly lower G-tube placement rates than tracheostomy in patients with PRS.25,32,37 This finding suggests that MDO may lead to better feeding outcomes, as it effectively corrects micrognathia and glossoptosis, thereby improving pharyngeal swallowing. However, this difference could also be influenced by more severe impairments in the tracheostomy group, such as neurological abnormalities affecting swallowing function.25,37 Previous studies have reported improved feeding outcomes and a reduced need for G-tube placement following MDO.38–40 Additionally, syndromic conditions may contribute to a higher rate of G-tube requirement, regardless of the surgical intervention.28,41
The analysis of hospital length of stay (LoS) indicated that this difference was not statistically significant, while MDO was associated with a shorter hospital stay compared to tracheostomy.32,42,43 The observed high heterogeneity suggests variability in the data, which may stem from differing protocols among institutions. In some facilities, the prolonged hospital stay for the tracheostomy group was attributed to caregiver preparation and the availability of home care services.42,43 Other studies have also reported longer hospital stays for patients undergoing tracheostomy.22,44 In contrast, one study noted a longer hospital stay for MDO, as this procedure was typically performed only after a nasopharyngeal airway (NPA) placement and when patients reached at least three weeks of age and weighed 8 lb. In comparison, tracheostomy was performed in patients who were not stabilized by NPA. 45
The cost analysis comparing MDO and tracheostomy offers essential insights into the financial implications of these interventions for managing PRS. While operating room (OR)-related costs did not significantly differ between the two procedures, MDO demonstrated a notable cost advantage in other hospital-related expenses, which include hospital stays, diagnostics, and consultations. OR-related costs tend to be higher for MDO when considering a single procedure, as the distraction device alone can cost nearly 30 times more than a tracheostomy tube, as highlighted in a Canadian study. 44 However, tracheostomy may incurs greater OR-related expenses over time due to the need for additional interventions, such as serial gastrostomy tube placements and ongoing airway maintenance procedures. 32 The elevated costs of tracheostomy are primarily driven by extended hospital or ICU stays.25,43,44 Moreover, the total cost analysis consistently favoured MDO, showing significantly lower overall expenses compared to tracheostomy. These findings suggest that while the initial surgical costs may be similar, MDO offers substantial overall cost savings, primarily due to reduced hospital stays. Other studies in the literature further support this conclusion.13,22
Due to limited data, we only focused on analyzing hospital-related costs. However, studies also suggest that the tracheostomy group incurs significant expenses from the extensive care required, leading to notably higher homecare and indirect costs, such as work absences, compared to MDO.43,46
While this study provides valuable insights into the comparative effectiveness of MDO and tracheostomy in managing PRS, several limitations must be acknowledged. First, the number of studies directly comparing MDO and tracheostomy is relatively small, and the sample sizes within these studies are limited, which may impact the generalizability of the findings. Additionally, the included studies vary in patient demographics, syndromic status, and follow-up duration, contributing to heterogeneity in some outcomes. Notably, high heterogeneity was observed in specific analyses, particularly concerning hospital length of stay and operating room (OR)-related costs, indicating variability in the data that could influence the results. Furthermore, the retrospective nature of many included studies may introduce bias, and the absence of randomized controlled trials limits the strength of the evidence. The financial analyses primarily relied on cost data from the U.S. and Canada, which may not adequately reflect economic differences across diverse healthcare systems. Future research should focus on larger, multicenter randomized controlled trials with standardized protocols. Additionally, future studies should aim to compare the two interventions within groups of similar syndromic status to minimize potential confounding factors and provide a more definitive comparison.
Despite the overall advantages of MDO in managing severe airway obstruction in patients with PRS, the decision to proceed with this intervention requires careful consideration due to the potential for significant complications. Major complications associated with MDO include dental injury (6–22.5%) and TMJ ankylosis (0.7–16%). Moderate complications, including device failure (3.4–13.2%) and surgical site infections (9.5–10%), have also been reported, alongside minor complications.17,21,26,27,47 Additionally, there is a notable risk of relapse, with incidence rates reaching up to 64.8%. This relapse is primarily attributed to a growth mismatch between the maxilla and the slower-growing mandible, resulting in an increased sagittal overbite. 47
Given those risks, MDO should only be considered when there is a solid clinical indication, such as severe airway obstruction or the failure of less invasive treatments. Meticulous preoperative preparation is essential, including detailed diagnostics to assess the level of airway obstruction, the type of OSA, and any associated comorbidities. Decision-making models, such as the decision tree proposed in previous studies, can assist in identifying appropriate candidates for MDO.21,22 By carefully selecting candidates for this procedure, clinicians can ensure that the benefits—namely, improved airway function and a reduced need for tracheostomy—outweigh the associated risks, ultimately leading to better overall patient outcomes.
Conclusion
MDO is associated with significantly higher success in airway outcomes, demonstrating its ability to prevent tracheostomy. It may also serve as a strategy to assist tracheostomized patients in achieving decannulation. Additionally, MDO is associated with lower rates of gastrostomy tube (G-tube) placements, and substantial reductions in hospital costs. Although MDO also tends to reduce the length of hospital stay, this finding did not reach statistical significance.
Overall, MDO demonstrates superior outcomes compared to tracheostomy. Given these findings, MDO should be considered the preferred initial treatment strategy for severe airway obstruction in PRS patients, as well as for those dependent on tracheostomy to facilitate decannulation. However, the poorer outcomes observed in the tracheostomy group may also be influenced by patient complexities, such as syndromic status and other comorbidities, suggesting that tracheostomy is often selected for more complex cases. Therefore, the decision to pursue MDO must be made carefully, as it also has its own risks and not all patients are viable candidates. Tracheostomy may still be required in certain cases or as a secondary intervention. Meticulous pre-operative planning, including assessment of syndromic status, level of airway obstruction, and other abnormalities, is essential to ensure the best outcomes for each patient.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241311549 - Supplemental material for Mandibular Distraction Osteogenesis vs. Tracheostomy in the Management of Pierre Robin Sequence: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cpc-10.1177_10556656241311549 for Mandibular Distraction Osteogenesis vs. Tracheostomy in the Management of Pierre Robin Sequence: A Systematic Review and Meta-Analysis by Indri Lakhsmi Putri, Kusuma Islami, Imaniar Fitri Aisyah, Rachmaniar Pramanasari and Citrawati Dyah Kencono Wungu in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
We would like to thank all authors whose studies are included in our systematic review and meta-analysis.
Author Contributions
-
- - - -
Data Availability Statements
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statements
This article does not contain any studies with human or animal participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.