
Abstract
Partners in African Cleft Training (PACT) is a collaborative education program between cleft team providers from African countries and United States that focuses on interdisciplinary team care for children with orofacial clefting to improve outcomes and expand access to team care in Sub-Saharan Africa. In this paper, we describe the evolution of a partnership, initiated by an African surgeon, to determine how to support sustainable cleft team care in Africa and share the impact of the PACT program on participating teams. This narrative review discusses 3 major steps in the evolution of the PACT program. The initial step was a pilot study to identify requirements for sustainable team care in Africa. This study concluded that the identification of challenges and solutions for cleft team care must come from within the African continent and that training centers focused on team cleft care should be established. This led to a 3-year program to establish regional cleft training centers for surgery, anesthesiology, and speech. The partnership evolved to include in-person workshops focused on interdisciplinary team care with the addition of new teams. The current PACT program includes team workshops, virtual curriculum, and seminars. Since 2011, there have been 15 workshops. All teams have increased in size and composition and 90% of participants reported a positive impact of workshop on patient care and strengthening teams. The impact of the PACT program has included the establishment of regional training programs and team building resulting in improved access to comprehensive cleft team care in sub-Saharan Africa.
Keywords
Introduction
Orofacial clefts are one of the most common congenital anomalies worldwide with a prevalence varying from 1 in 500 to 1 in 1500 births. 1 Care of a child with an orofacial cleft begins at birth and continues until the completion of facial growth in early adulthood. Complex healthcare needs include feeding and nutrition support, hearing and speech assessments and interventions, orthodontic and dental treatment, psychosocial assistance, and surgical management. As an orofacial cleft can occur as part of an underlying genetic condition, assessment for associated health concerns that might impact general health is important for optimal outcomes. Thus, management of children with orofacial clefts is best provided by an interdisciplinary team of dedicated specialists.
Partners in African Cleft Training (PACT) is a collaborative education program between providers from the Seattle Children's Hospital Craniofacial Center and cleft teams in Ghana, Ethiopia, Nigeria, Liberia, Kenya, and Tanzania, focusing on interdisciplinary team care for children with cleft lip and/or palate. Current education activities include annual weeklong team training workshops in Sub-Saharan Africa, quarterly virtual seminars, and access to a virtual cleft team classroom. Since inception of the PACT program, over 190 African providers have participated in workshop training with an associated increase in size and interdisciplinary composition of their local teams over time, resulting in improved access to team care for children with cleft lip and palate in Sub-Saharan Africa.
The purpose of this narrative is to describe the evolution of the PACT partnership (Figure 1) and the impact of its educational program on interdisciplinary team care in Sub-Saharan Africa. Our goal is for these lessons learned to be used to identify the path forward for the continued evolution of team-based cleft care in Africa.
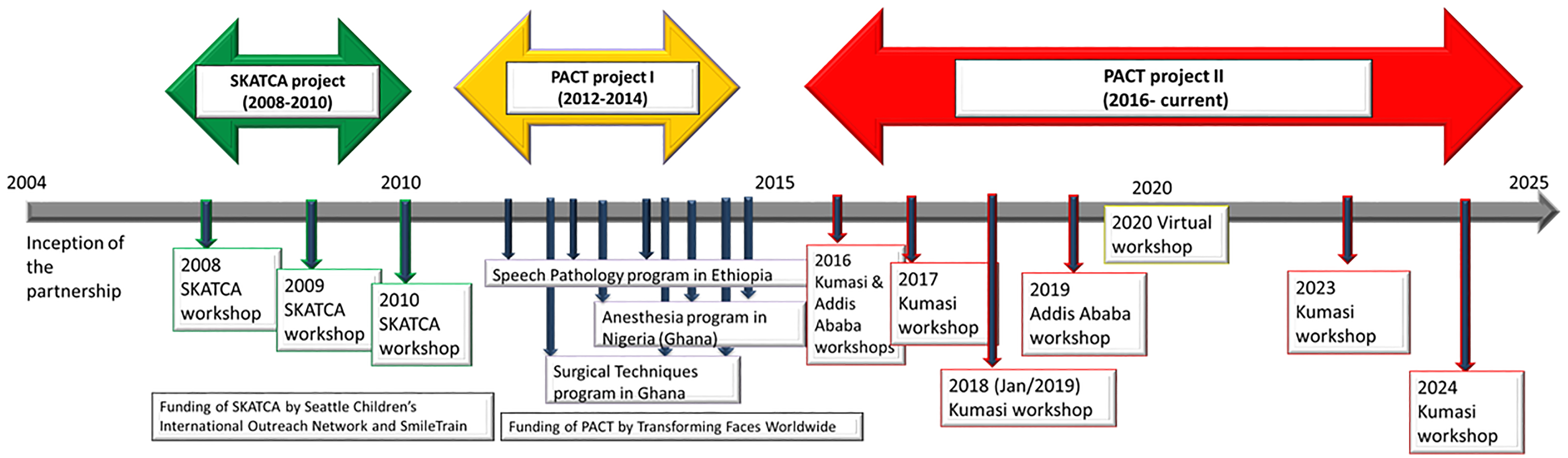
Evolution of Partners in African Cleft Training (PACT) program.
Methodology
Partners in African Cleft Training began as an African initiative to establish a partnership to promote sustainable cleft team care in Africa. In 2004, Dr Peter Donkor, oromaxillofacial surgeon and cleft team leader at Komfo Anokye Teaching Hospital in Kumasi, Ghana, reached out to the Seattle Children's Hospital Craniofacial Center Medical Director, Dr Michael Cunningham, to discuss how to enhance cleft team care in Africa. In 2005, Dr Donkor was selected as an American Cleft Palate Craniofacial Association visiting professor and was sponsored by the Seattle Craniofacial Center with the support of Dr Cunningham and Surgical Director, Dr Richard Hopper. Over the next 2 years, the partnership between Drs. Cunningham, Hopper, and Donkor led to the initiation of the Seattle–Kumasi Advocacy for Team Cleft-care in Africa (SKATCA) program through financial support from the Smile Train Foundation and Seattle Children's Hospital Foundation. Distinct from short-term medical or surgical missions at that time, the focus of SKATCA was not on delivery of surgery, but instead on promotion of sustainable interdisciplinary team cleft care in Africa. The program began with an assessment of the requirements necessary for sustainable cleft team care from the perspective of African cleft providers.
Seattle–Kumasi Advocacy for Team Cleft-Care in Africa Program
The mission of the SKATCA program was “to foster, facilitate, and sustain team care for children with cleft and craniofacial disorders in Sub-Saharan Africa through shared educational and clinical activities.” The primary goal of this pilot project was to reach a shared consensus on the needs of each participant group to move forward with sustainable team cleft care. The leadership of SKATCA hypothesized that “advancement of cleft care in Sub-Saharan Africa would be facilitated by access of independent African cleft surgical and nonsurgical practitioners to regional collaborations, continuing education, and training of future providers.”
The SKATCA program was initiated in December 2007 with a memorandum of understanding between the clinical and educational institutions of Dr Peter Donkor (Komfo Anokye Teaching Hospital and Kwame Nkrumah University of Science and Technology), and Drs. Richard Hopper and Michael Cunningham (Seattle Children's Hospital and University of Washington). Acknowledging that the design of cleft team structure may vary within and between African countries, 13 cleft providers from 6 Sub-Saharan African countries (Nigeria, Ethiopia, Senegal, Cote D’Ivoire, Tanzania, South Africa) interested in developing or expanding multidisciplinary cleft teams and 13 team members of the Seattle Craniofacial team from multiple clinical disciplines (surgery, anesthesiology, pediatrics, nursing, and speech-language pathology) participated in the SKATCA program. In total, 3 one-week workshops (2008-2010) were held at the Komfo Anokye Teaching Hospital in Kumasi, Ghana.
The SKATCA program incorporated didactic lectures, group discussions, and shared observational and clinical experiences with a focus on interdisciplinary team care and patient outcomes. Group discussions at the conclusion of each workshop facilitated identification of perceived barriers to cleft care and team building as well as potential solutions. Following workshops in Kumasi in years 1 (2008) and 2 (2009), the African providers had reciprocal visits to the Seattle Craniofacial center for continued interactions.
In year 3 (2010) of SKATCA, cleft team providers from Maidiguri (Nigeria), Addis Ababa (Ethiopia), Kumasi (Ghana), and Seattle (USA) met to discuss consensus from their shared experiences. Providers agreed that hands-on clinical experiences in Africa were considered more valuable by participants than observational experiences in Seattle. Participant feedback was that observations of team care using the clinical resources available in Seattle were not directly applicable to home environments. There was consensus that the identification of challenges and solutions for cleft team care must come from regional providers within the African continent. They also recommended that providers at workshops use host facilities and equipment. Participating African teams identified the need for cleft-speech training, cleft-specific training for nurse anesthetists, and cleft surgery training for nurses and surgeons. This consensus decision led to the establishment of the PACT program.
Partners in African Cleft Training Program Specialized Training Centers
Following the conclusion of the SKATCA program in 2010 its learnings were used to create the PACT program, with partial funding from Transforming Faces Worldwide and the Phil and Helen Smart “Unknown Child” endowment. In 2011, PACT started as a 3-year program as cleft team providers from Seattle, Ghana, Ethiopia, and Nigeria partnered to establish specialized training centers (STC) for surgery, anesthesiology, and speech in Sub-Saharan Africa. Drs. Cunningham and Hopper provided programmatic and clinical leadership for the program. The major goal of the PACT STC program was to establish Centers of Excellence in cleft and craniofacial training and patient care.
The STC in Cleft Surgical Techniques, directed by Dr Peter Donkor (Komfo Anokye Teaching Hospital, Kumasi, Ghana) was designed as an African-based training site for up-to-date cleft surgical techniques. Over the course of 3 years, 8 surgeon–nurse pairs were selected from across Africa to attend a 2-week didactic and practical surgical training program. The PACT STC Cleft Surgical Techniques program was held at the Komfo Anokye Teaching Hospital in Kumasi, Ghana (2012, 2014) and at the Korle-Bu Teaching Hospital in Accra, Ghana (2013).
The STC in Cleft Anesthesia, directed by Dr H.O. Olasoji (University of Maiduguri Teaching Hospital, Maiduguri, Nigeria) was designed as an expanded nurse anesthetist training program with a cleft-specific anesthesiology training component. Over the course of 3 years, 16 nurse anesthetists were selected to participate in workshops for targeted anesthesiology training by anesthesiologists with experience in cleft surgery, dedicated surgeons, and nurses for children undergoing cleft lip and cleft palate surgery. The PACT STC Cleft Anesthesia program was held at the Obafemi Awolowo University Teaching Hospital in Ile-Ife, Nigeria (2013), and the Komfo Anokye Teaching Hospital in Kumasi, Ghana (2012 and 2014).
The STC in Cleft Speech Pathology, directed by Dr Mekonen Eshete Abebe (Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia) was designed to provide African-specific speech-language therapy and feeding technique training for cleft nurses. Over the course of 3 years, 13 nurses from Ethiopia, Nigeria, and Ghana were recruited to attend 2 months of intensive observational and practical training in Speech-Language therapy to assess and manage patients before and after surgery. The PACT STC Cleft Speech Pathology program was held at Yekatit 12 Hospital Medical College in Addis Ababa, Ethiopia (2011-2014).
Each STC developed a site-specific education program that included didactics, hands-on experience, and mentorship by trainers with expertise in cleft care. Outcome measures included: (1) establishment of regional training programs for cleft care for surgery, speech, and anesthesiology, and (2) growth of participating teams. Over the course of 3 years, 37 cleft providers (surgeons, nurse anesthetists, and nurses) received training at one of the PACT STC sites. At the conclusion of the 3-year PACT STC program in 2014, team leaders from Ghana, Ethiopia, Nigeria, and Seattle elected to continue in-person PACT education workshops with a primary focus on interdisciplinary team care to support growth of existing teams and establishment of new teams.
Partners in African Cleft Training Program Interdisciplinary Team Workshops and Virtual Program
After completion of the 3-year STC project in 2014, the PACT program shifted to weeklong in-person cleft team workshops dedicated to enhancing interdisciplinary team care and included participants with clinical expertise in nursing, surgery, anesthesia, orthodontics, pediatrics, speech, nutrition, genetics, and social work. Although the 2015 workshop was delayed because of the Ebola outbreak, 2 weeklong workshops were pursued in 2016, one in Addis Ababa and one in Kumasi. These workshops included providers from 6 disciplines (surgery, nursing, anesthesiology, speech, pediatrics, and orthodontics) and 4 teams (Addis Ababa, Ethiopia, Kumasi, Ghana, Ile-Ife, Nigeria, and Seattle). In 2017, a new team from Monrovia, Liberia joined the PACT program followed by teams in Nyeri, Kenya (2019), and Mwanza, Tanzania (2024). Since 2019, cleft team providers from 2 teams in Nigeria (Ile-Ife and Maiduguri) have attended PACT workshops. In total, since the PACT STC programs began, there have been 7 in-person workshops with gaps in 2015 (Ebola outbreak) and 2020 to 2022 (COVID pandemic). Partners in African Cleft Training educational workshops held between 2016 and 2024 took place at either the Komfo Anokye Teaching Hospital in Kumasi, Ghana (October 2016, November 2017, January 2019, January 2023, and February 2024) or at the Yekatit 12 Hospital Medical College in Addis Ababa, Ethiopia (March 2016 and September 2019). Figure 2 shows how PACT workshops have grown over time with an increase in number of teams, number of participating trainees, number of disciplines, and size of host team. Many trainees have participated in more than one workshop, and some have become PACT trainers and team leaders. At the 2024 workshop in Kumasi, 35 participants traveled to Kumasi from 5 African countries and Seattle, joined by over 40 host team members. In total, there were 25 trainees representing 8 disciplines.
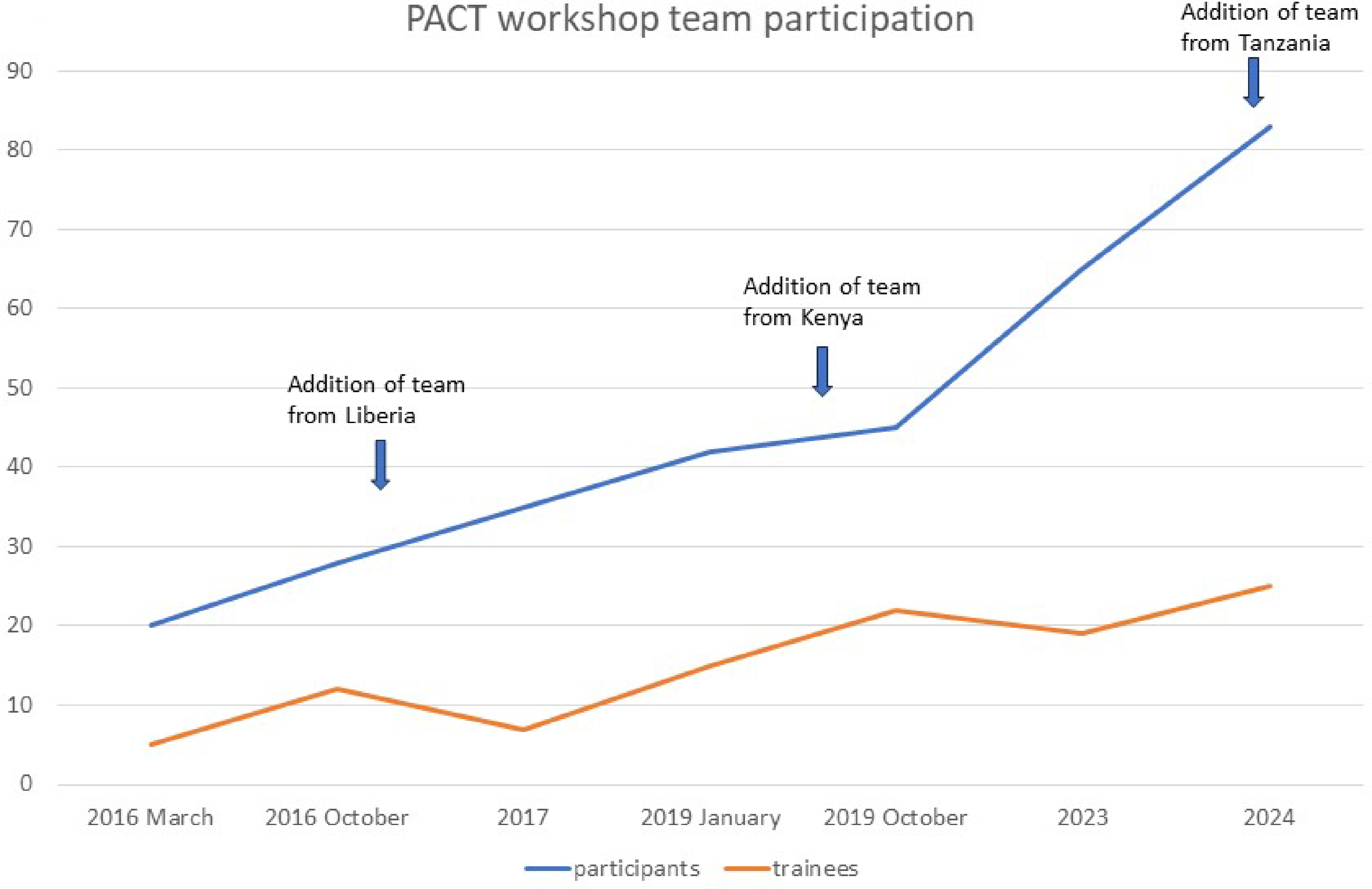
Partners in African Cleft Training (PACT) workshop participation 2016 to 2024. In 2016, cleft team providers from 6 disciplines (surgery, anesthesia, pediatrics, nursing, orthodontics, and speech) participated in the PACT workshop. In 2017, members from social work joined the workshop. Since 2019 with the addition of nutrition, providers from 8 disciplines have attended PACT workshops.
In-person PACT training workshops have included didactics, group discussions, and in-person patient care experiences including interdisciplinary team clinics and surgery. All workshop trainees have been selected by their respective team leaders and matched, by discipline, with mentors from African and Seattle teams. Oversight of clinic assessments and surgical care for patients during each workshop has been provided by the Host Cleft Team. Select Seattle providers have been able to provide direct patient care using temporary clinical privileges from host medical centers during workshops.
The general format of the in-person PACT team workshop has included 2 interdisciplinary team clinics, 2 days of surgery, and lectures (Figure 3). Although workshop lecture content, discussion sessions, and organization of clinical experiences have been modified in response to post-workshop survey comments, the overall format of the workshop has remained constant since 2016. Programmatic improvements have included the utilization of a WiFi borescope to assist with teaching palatoplasty in the operating theater starting in 2016 (Figure 4) and design of a surgical readiness checklist in 2019 (Supplement 1) to model interdisciplinary team care focused on patient safety. This worksheet has been used in workshops to stimulate discussion between disciplines after the presurgical team clinic to safely select patients for surgery the following day. With the addition of nonsurgical participants, didactics and clinical activities have been designed for speech, nutrition, pediatrics, orthodontics, and social work on surgical days to enhance learning. Surgical and anesthesiology trainees have been paired with mentors in the operating theater to optimize education of regional African providers. The environment and resources of the operating room are intentionally not modified from their usual baseline to ensure shared learning is translatable after the workshop. Each workshop has included group discussions focused on barriers and challenges to cleft team care with breakout sessions to troubleshoot solutions with established regional teams.

Template of Partners in African Cleft Training (PACT) 1-week workshop with lecture topics.
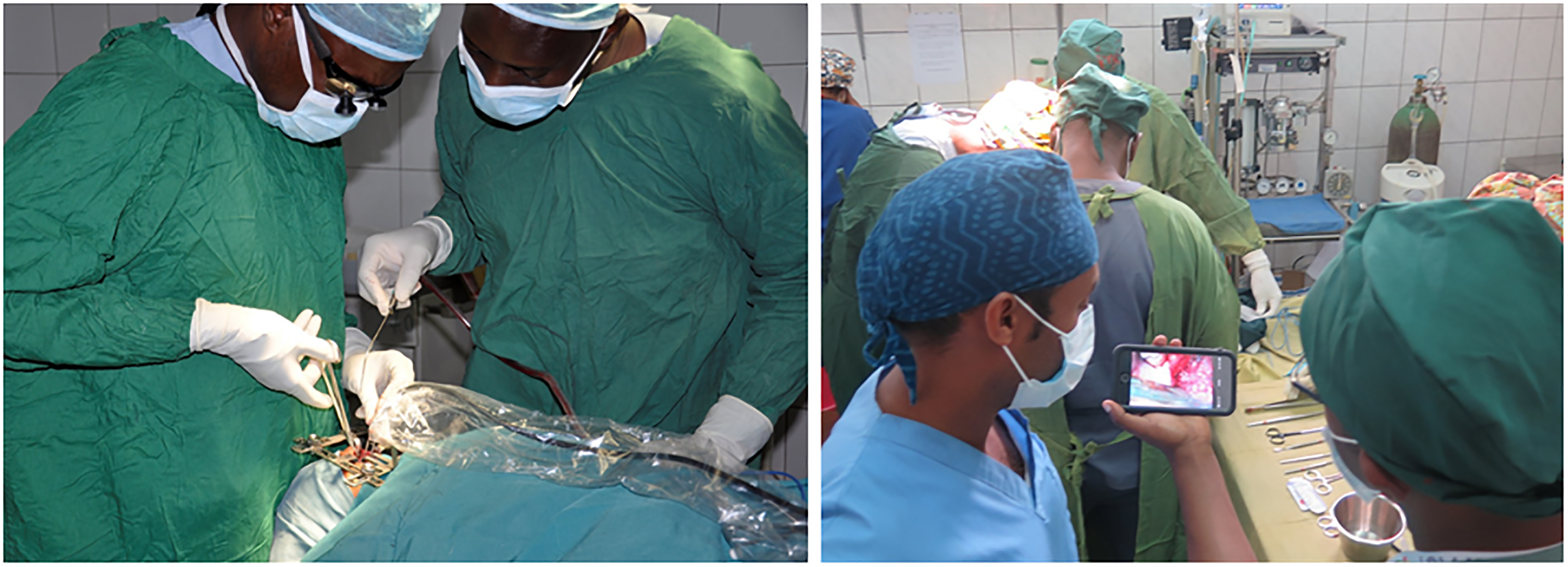
Surgeons using a WiFi borescope and smart phone for teaching cleft palate repair.
Since 2019, participants (trainees) have been contacted by mentors to discuss involvement in workshop teaching events one month prior to each workshop and since 2023, trainees have received access to the virtual PACT Canvas classroom (described below) to take PACT classroom learner modules in advance of the workshop. In 2024, the PACT workshop trainee curriculum (Supplement 2) was updated to include preworkshop learner assignments and workshop presentations with 100% compliance by trainees. Outcome assessments of the in-person PACT workshops have included in-person review of each workshop on day 5 with focus on recommendations for future workshop discussion topics and programmatic changes including program expansion. Beginning in 2017 participants were requested to complete annual post-workshop surveys with response rates ranging from 38% to 51%.
The virtual component of the PACT program was developed in 2020 in response to the COVID pandemic. This week-long virtual PACT workshop included twice daily videoconferences and learner modules supported by the Canvas platform, a web-based learning management system. The Canvas digital learning environment facilitated links to live Zoom videoconference meetings, access to prerecorded lectures, and learner modules with embedded tests. Canvas could be accessed via a smartphone application and engagement could be tracked to monitor participation.2,3 In preparation for the virtual workshop, 8 learner modules (Nutrition, Surgery part 1 and 2, Pediatrics, Speech, Anesthesia, Social Work, and Orthodontics) were developed by African team leaders and Seattle team providers. Each learner module included prerecorded educational videos, learner assessments, and reading resources. During the workshop, participants attended 5 group lectures and 8 Zoom sessions entitled “meet the experts” to discuss discipline-specific healthcare needs of a child with cleft lip/palate. Zoom sessions were recorded and added to the Canvas platform. In 2021, quarterly 90-min virtual seminars were established to provide year-round PACT participant engagement and education. In 2022, access to PACT discipline-specific learner modules, video recordings from the 2020 virtual workshop, and quarterly seminars were made available to all participants in the PACT Canvas classroom. The virtual component of the PACT program has been used to create year-round engagement and to supplement in-person workshop education resources.
Results
In 2024, the Komfo Anokye Teaching Hospital was recognized as a center of excellence in cleft care with a Smile Train–funded post-fellowship cleft surgery training program and the construction of a dedicated cleft treatment center. Additionally, the University of Addis Ababa, in collaboration with Yekatit 12 Hospital Medical College Cleft team, has established a successful speech pathology program including a master's program. 4 Civil unrest resulted in the Nigeria-based anesthesia STC program relocating from Maiduguri to Ile-Ife where the anesthesiology and difficult airway program provided training for nurse anesthetists during cleft surgery regionally and through the PACT program. Since 2008, Anesthesiologists and Nurse Anesthetists have been active members and leaders of regional cleft teams participating in the SKATCA and PACT programs. It is important to recognize that the progress made following the initial PACT STC program was due to continued efforts of regional cleft team leaders and attainment of local and international resources.
Participation in the SKATCA and PACT programs resulted in several unanticipated outcomes for both Seattle and African teams. After the SKATCA program, participating surgeons identified a redundancy of instruments delivered for cleft surgery in the African workshops, but with deficiency of key tools required for successful performance of the techniques taught. In response, 4 critical surgical instruments for cleft palate repair (Double Ended Hourigan Modified Woodson Periosteal Elevator, Gerald straight-toothed forceps, long narrow needle driver, fine-tipped Metzenbaum scissors), and 5 for cleft lip repair (Fine-toothed Addison forceps, fine single skin hook, Iris scissors, Webster needle driver, Tenotomy Scissors) were identified. The Seattle team has provided teams with these essential surgical instruments. Due to concerns for stable airway and adequate visualization of the surgical field during cleft palate repair, in 2016, Dr Hopper initiated efforts to design an inexpensive oral retractor for cleft palate repair to optimize visualization and prevent kinking of the endotracheal tube. At the conclusion of SKATCA, nonsurgeon providers in Kumasi and Seattle combined efforts to design a specialized feeding cup for infants with cleft palate that would circumvent need for specialized cleft bottle. This partnership led to the design and testing of an infant feeding cup called the NIFTY (

NIFTY (
In addition to the evolution of the African teams’ treatment pathways, there was reciprocal learning that led to changes in care pathways in Seattle. Seattle providers observed a reduced need for opioids and decreased infant distress through the African teams immediately reuniting the baby with the mother in the recovery room after cleft repair. In addition, they observed no complications and multiple benefits from avoiding arm restraints and allowing immediate feeding with modified nipples or breastfeeding after all cleft repairs. In 2016, the Seattle Children's Hospital implemented these African-based practices into their Clinical Standard Work pathways with documented decreased need for pain medication and improved family and patient satisfaction. The Seattle team also reduced the number of instruments in surgery kits for each cleft surgery resulting in savings of both time and cost.
Outcome assessments of the in-person PACT workshops since 2017 have included annual post-workshop surveys. A review of survey responses from the last 5 workshops (2017-2024) showed that over 92% of respondents had prior experience caring for an individual with cleft lip/palate and more than 83% were members of a cleft team at the time of the workshop. The majority (>95%) responded that participation in the workshop had a positive impact on patient care at their center, and all respondents indicated that they would attend another workshop. Over 95% would recommend the workshop to their colleagues.
In 2023, team leaders completed a survey to provide information about the size and composition of their team since joining PACT program. As noted in Figure 6, all participating teams have grown in size and composition (number of disciplines). Additionally, team leaders reported that team conferences to discuss patient care occurred on a regular basis, and 50% of PACT teams held interdisciplinary team clinics. In response to the PACT leadership survey question, “What has been the impact of the PACT program on your team's growth and patient care?,” participating team leaders reported the following:
Establishment of interdisciplinary team clinics
Improved surgical skills and knowledge
Improved support of speech and nutrition
Improved quality and scope of care
Improved communication and synergy of care
Improved safety (surgical and nonsurgical)
Collaboration between African teams
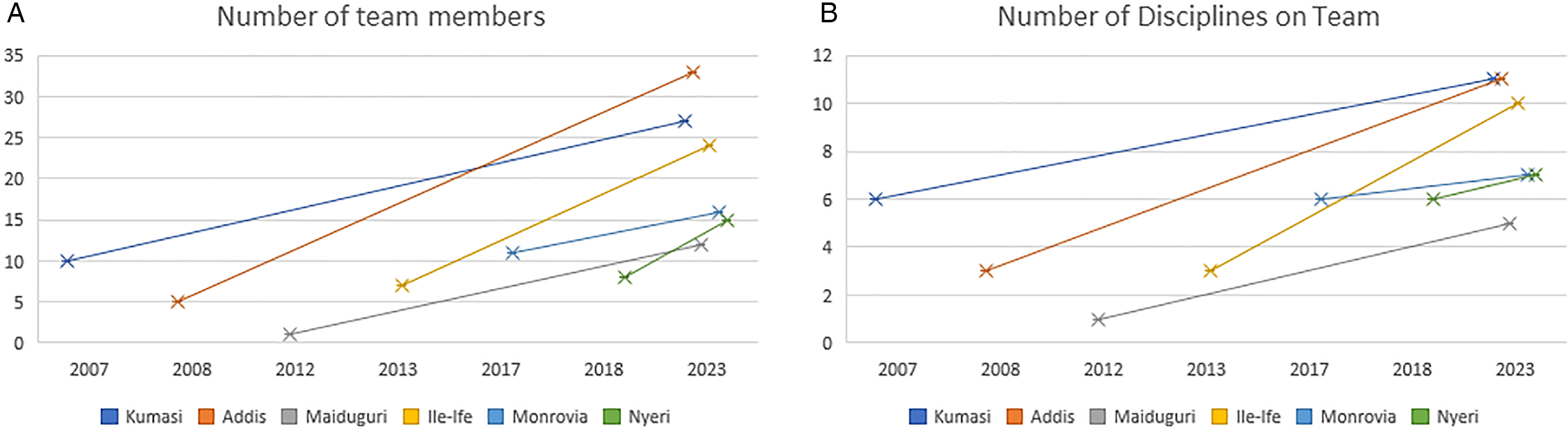
Growth of Partners in African Cleft Training (PACT) teams. (A) Team composition: average 6-fold increase in number of team providers (range of 1.4-12 fold), (B) average 2.67-fold increase in number of disciplines (range of 1.16-5 fold).
In 2024, a 15-question survey was sent by email to past trainees (since 2011) to determine their current involvement in cleft team care and potential impact of the PACT program on patient care. Contact information was available for 90 (67%), and responses were received from 40 trainees (44%). Eighty percent of survey respondents had attended a workshop between 2019 and 2024, and 19% had attended multiple workshops. All respondents had continued to provide cleft care and 97% were members of a cleft team. Although 25% were no longer involved with PACT program, most wanted to reconnect. All respondents reported positive impact of PACT on clinical practice.
Discussion
The PACT program is a longitudinal education program and partnership of over 16 years between cleft team providers in Sub-Saharan Africa and Seattle Children's Hospital. In 2003, Dr Peter Donkor initiated an interdisciplinary team in Kumasi, and in 2007, he published a study that demonstrated a sharp upward trajectory of cleft lip surgeries at the hospital between 2001 and 2005 even though surgery had been available since 1991. In this article, Dr Donkor implored that “visiting teams could expand their role by offering training to cleft teams and developing countries as well as providing longer-term assistance to strengthen the capacity of the local teams to deliver more comprehensive interdisciplinary cleft services to their patients.” 8 Similarly, in a survey of 225 cleft providers attending the second Pan-African Congress on Cleft Lip and Palate in 2007, providers noted limited access to comprehensive teams and reported the need to focus on funding, team building, infrastructural support, and patient education. The authors recognized the role of mission-oriented cleft care but concluded the following, “By focusing on patient education, providing infrastructural support, and addressing the socioeconomic hardship both at the institutional (physician) and individual (patient) levels, cleft care providers can partner with African cleft practitioners in a more dynamic, effectual, and valuable manner to promote cleft care in the region.” 9 In 2008, the Seattle–Kumasi Advocacy for Team Cleft-care in Africa Program was established with a goal to address this focus.
The SKATCA program shared learnings and had far-reaching implications for the development of PACT and other educational-based cleft initiatives: (1) African workshops with shared clinical activities using African-based resources were considered more valuable than reciprocal visits to Seattle observing cleft care in a more technology-based environment, (2) “Africans for Africa”—identifications of challenges and solutions must come from the expertise present in the African continent, and (3) For non-African providers to participate in brainstorming solutions, a prolonged period of communal activities in a relevant environment is required for shared understanding. The SKATCA participants identified the need for regional STC for cleft surgery, cleft speech, and cleft-specific training for nurse anesthetists. The need of cleft specific anesthesia training was well-recognized by regional providers as the risk for anesthetic complications (hypoxia, laryngospasm, kinking of the endotracheal tube, inadvertent extubation, and pulmonary aspiration) in children with cleft lip and cleft palate was reported to be as high as 15% in centers in Nigeria at that time. 10 Currently, anesthesiology providers (nurse anesthetists or anesthesiologists) are active members of PACT-affiliated African cleft teams. Anesthesiology trainees have participated in every PACT workshop focusing on patient safety and airway management. In 2024, a SmileTrain-Lifebox dual parameter capnograph, monitoring CO2 and oxygen saturatiion, was provided by the PACT program to centers that identified a need for improved perioperative monitoring capability. Lastly, it is important to note that group discussions of barriers and challenges to cleft team care in Africa, a focus of the SKATCA program, take place at every PACT workshop. Each discussion includes time and a supportive environment for all team members and disciplines to share potential solutions for the future through facilitated mediation.
At the time that PACT was established in 2011 to support the establishment of regional training centers and interdisciplinary cleft team care in Sub-Saharan Africa, the model of short-term care delivery through medical missions was under intense scrutiny. In 2012, Martiniuk reviewed literature related to health-focused medical missions from 1985 to 2009, of which 23% related to cleft care, with concerns that this short-term and transitory care delivery model included a lack of sustainability and insufficient contact with local healthcare system. 11 Similarly, Patel noted that global cleft surgical missions at that time represented a vertical model of healthcare delivery that was parallel to but not part of the local health system and as such, did not promote improvements in local infrastructure and workforce. 12 He suggested that global cleft missions should pursue a diagonal care delivery model to include integration with local care systems to improve infrastructure and manpower. Two years later, Sykes pursued a systematic literature review noting that over 95% of medical missions did not collect data to look at impact or outcomes and that missions were largely unregulated. 13 In 2018, Lasker reviewed 27 best practice guidelines for short-term medical missions. As the authors reviewed core principles, common themes included collaboration with local health providers and longitudinal evaluation and sustainability. 14 Interestingly, in 2013, international partnerships to transfer expertise, skills, and knowledge from high-income countries to LMIC countries were started in the treatment of childhood cancer. This model of institutional partnering between countries was called “international twinning partnership” (ITP). As noted in the publication by Hopkins, 15 for the ITP model to be successful, the partnership must be led by the local LMIC team, solutions must come from the local team, and the process must be affordable. In 2018, the WHO shared a 6-step protocol for the establishment of ITPs to improve health service delivery. In brief, the 6 steps include: (1) partnership development, (2) needs assessment, (3) gap analysis to identify priority areas for action, (4) establish action plan, (5) implementation, and (6) evaluation and improvement. Once improvements have been achieved, the partners are tasked to scale up and share regionally and beyond. 16 Although not intentional, the similarities of the PACT program and with the ITP process are remarkable.
While it is encouraging that participating PACT teams have grown in number and composition, it is important to note that participation in the PACT program was an indirect cause of team growth. The growth of participating teams reflects the efforts, determination, and resourcefulness of team leaders using resources made available from a number of nongovernmental and governmental sources. Participants in the PACT program felt the experience increased the awareness of the importance of interdisciplinary cleft team care for patient outcomes, helped to define the roles of each team provider, and demonstrated the importance of communication between team providers. This included improvement in communication across disciplines that traditionally had hierarchical barriers. At the conclusion of the 2024 PACT workshop, the 25 trainees were asked to respond to the question: “what was the impact of the PACT workshop?.” Their top 10 comments included: networking opportunity, raised awareness regarding the dynamics of patient care, mentorship, learned skills, learning about different cultures, the importance of comprehensive (interdisciplinary) care for a patient with a cleft, leadership training, post-op pain management, communication between disciplines, and challenges at different centers to deliver team care.
The PACT program provides a model for team building and training, with the long-term goal of team care for all children with cleft lip and palate in Sub-Saharan Africa. PACT team leaders and participants have valued the education experience with team leaders reporting improvement in quality and scope of care, safety, and synergy of care through communication between disciplines and increased collaboration between PACT teams. PACT team leaders endorse the expansion of the program to include the addition of new teams from more countries with continued support of participating teams during and in between workshops through the PACT virtual platform, establishment of standards of care, initiation of outcome studies, and support of regional centers of excellence for training. The next step toward expansion to other regions in Africa will include the development of a program to train regional PACT trainers to support workshops in Addis Ababa, Kumasi, and other cleft centers in Sub-Saharan Africa. Funding support for this program continues to come from donations to the Seattle Children's Craniofacial Center, Smile Train, and Transforming Faces.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251319898 - Supplemental material for Partners in African Cleft Training (PACT): Evolution of a Partnership Supporting Sustainable Interdisciplinary Cleft Team Care in Sub-Saharan Africa
Supplemental material, sj-docx-1-cpc-10.1177_10556656251319898 for Partners in African Cleft Training (PACT): Evolution of a Partnership Supporting Sustainable Interdisciplinary Cleft Team Care in Sub-Saharan Africa by Anne Hing, Craig Birgfeld, Richard Hopper and Mekonen Eshete Abebe, Shiferaw Degu Berbirssa, Oladapo Olasoji, Gyikua Plange-Rhule, Albert Paintsil, Solomon Obiri-Yeboah, Hitesh Kapadia, Kaylee Paulsgrove, Olawunmi Fatusi, Jerry Fahnloe Brown, Ama A.A. Taplah, Cassandra Aspinall, Sean Flack, Emily Gallagher, Mariah Mazzaferri, Emily Nyamu, Mohammed Abullahi, Olurotimi Aaron, Lauren Beckett, Francis Tegete, , Michael Cunningham, Peter Donkor in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656251319898 - Supplemental material for Partners in African Cleft Training (PACT): Evolution of a Partnership Supporting Sustainable Interdisciplinary Cleft Team Care in Sub-Saharan Africa
Supplemental material, sj-docx-2-cpc-10.1177_10556656251319898 for Partners in African Cleft Training (PACT): Evolution of a Partnership Supporting Sustainable Interdisciplinary Cleft Team Care in Sub-Saharan Africa by Anne Hing, Craig Birgfeld, Richard Hopper and Mekonen Eshete Abebe, Shiferaw Degu Berbirssa, Oladapo Olasoji, Gyikua Plange-Rhule, Albert Paintsil, Solomon Obiri-Yeboah, Hitesh Kapadia, Kaylee Paulsgrove, Olawunmi Fatusi, Jerry Fahnloe Brown, Ama A.A. Taplah, Cassandra Aspinall, Sean Flack, Emily Gallagher, Mariah Mazzaferri, Emily Nyamu, Mohammed Abullahi, Olurotimi Aaron, Lauren Beckett, Francis Tegete, , Michael Cunningham, Peter Donkor in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors would like to acknowledge the administrative support from Seattle Children's Hospital Craniofacial Center [Marti Davis, Jerrie Bishop, Sydney Kaser, Karina Martinez-Lopez, Shalynn Howard, and Joyce Doll], Komfo Anokye Teaching Hospital [Naomi Appiah and Bernard Nkrumah], and Yekatit 12 Hospital Medical College [Dilargachew Assefa] without whom this work would not have been possible. The authors would also like to thank the many individuals and families who have provided financial support for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Primary funding for Seattle-Kumasi Advocacy for Team Cleft-care in Africa (SKATCA) and Partners in African Cleft Training Program (PACT) was provided by the Phil and Helen Smart “Unknown Child” endowment, and the Seattle Children's Hospital foundation. Smile Train (2008-2010) and Transforming Faces Worldwide (2011-2013) provided support for SKATCA and PACT, respectively.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.