
Abstract
Objective
To evaluate learners’ acceptance of multiuser virtual reality (VR) simulation platform while practicing the Furlow repair technique for cleft palate reconstruction.
Design
Nonrandomized with pre- and postsurveys.
Setting
Tertiary care institution's Department of Surgery September 2023 through August 2024.
Participants
Twenty plastic surgery residents from level PGY1 to PGY6 from a single institution.
Interventions
Multiuser Meta Quest 2 VR simulation-based workshop with an expert surgeon demonstrating a Furlow cleft palate repair. Feedback included audio and visual.
Main outcome measures
Learner confidence in using VR as a tool for surgical education, understanding of the Furlow technique, and opinion regarding the incorporation of VR into surgical and medical education. Satisfaction as measured by the Student Evaluation of Educational Quality questionnaire survey with a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree).
Results
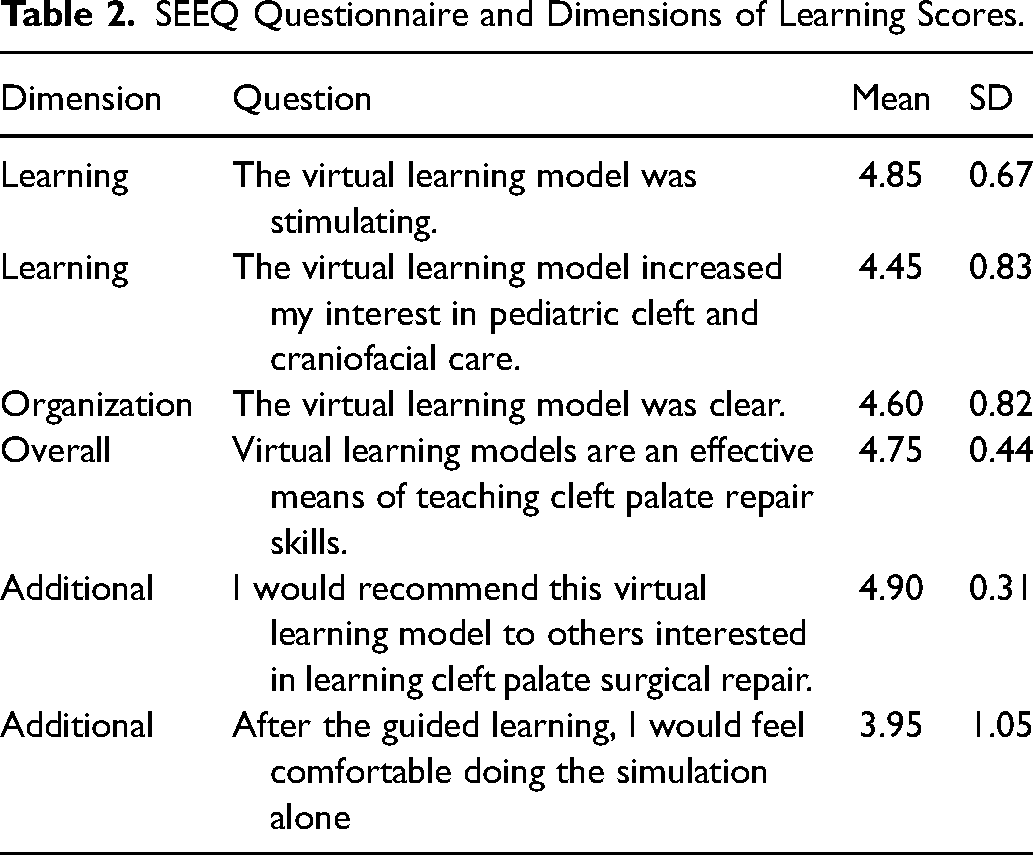
20 residents participated in this study, of which 65% had previously participated in a cleft palate repair and 40% had used VR. After the simulation, trainees’ confidence in using VR as a tool for surgical education, understanding of the Furlow technique, and opinion regarding the incorporation of VR into surgical and medical education significantly increased (P < .05). Trainees found the simulation stimulating (4.85 ± 0.67), interesting (4.45 ± 0.83), clear (4.60 ± 0.82), an effective teaching tool (4.75 ± 0.44) and would recommend it to others (4.90 ± 0.31). Participants reported that they would feel somewhat comfortable repeating the simulation alone (3.95 ± 1.05).
Conclusion
Multiuser VR-based simulation workshops can significantly increase learners’ confidence and skills in the Furlow technique and promote positive opinions regarding VR as an educational tool. Learners considered this platform effective and stimulating and would recommend it as an educational tool.
Introduction
Congenital cleft lip and palate are the most common causes of craniofacial defects affecting infants. Incidences of clefting have been long studied and differ based on geographical, racial-ethnic, and socioeconomic factors.1 According to the World Health Organization (2024), the global cleft lip and palate incidence average is 1 in 700 live births.2 Similarly, the long-term consequences of this uncorrected or poorly reconstructed patients can affect speech feeding and impact an individual's self-consciousness and social interaction.3–5
Given the nuances of cleft care, medical trainees in high- and low-resource settings alike encounter significant hurdles as traditional teaching methods and textbooks fall short in providing adequate surgical conceptualization of the complexity of orofacial clefting, including the multitude of surgical techniques employed in clefting reconstruction.6–8 In appreciation of these deficiencies, new training resources have been incorporated into medical education to make learning more efficient, safe, and effective.9 Ranging from actors playing patients in objective structure clinical examinations to simulators of surgical procedures, teaching has incorporated technology to model real-life clinical scenarios to prepare future providers.10,11 Furthermore, internet-based applications have been proven successful in delivering interactive multimedia content through intraoperative videos and surgical skill quizzes, enhancing surgical education efforts.12–14 Of these, virtual reality (VR) has emerged as a novel educational modality that allows for an immersive and interactive virtual environment in which visual, auditory, haptic, and tactile perspectives can be incorporated.15 Furthermore, virtual reality technology offers a cost-effective, sustainable solution to train surgical techniques in low-resource areas where trainers, equipment, and facilities are not present.
Previous research has demonstrated the benefit of VR in improving surgical competency and technique while improving patient care.15 As quality and surgical knowledge are often dependent upon the total number of clinical hours trainees undergo, VR supports the motto of “see one, do one, teach one,” providing students a realistic surgical environment and technique before even encountering an operating room.16 This is especially important when the surgical anatomy is complex and the surgical exposure for trainees is limited.17 As such, through the creation of immersive online interactive classrooms, virtual reality has the power to connect educators and students globally and even supplement local training programs with deficiencies in certain surgical subspecialties.15
Studies in other surgical specialties involving VR technology have shown that immersive virtual reality improves surgical skills acquisition, movement efficiency, and procedural knowledge.18,19 Despite the known potential benefits of VR to surgical training, the technology has yet to be applied to cleft lip and palate reconstruction. Considering the importance of providing cleft education to trainees in both local, national, and international scales, the current study aims to present a novel virtual reality module which demonstrates the Furlow cleft palate repair and report the potential benefits of an immersive VR classroom for teaching cleft surgery.
Methods
Overview of the Simulator
In partnership with the nongovernmental organization Smile Train, Inc. (New York) and the immersive-reality technology company BioDigital, Inc. (New York) a multiuser cleft surgery VR platform was created that simulates a metaverse operating room. Utilizing the multiuser simulation system Autodesk Maya® (Autodesk, San Rafael, CA) for content creation, the simulation demonstrates a Furlow cleft palate repair where trainees are immersed in the virtual operating room with an experienced surgeon teaching the individual steps of the procedure on a virtual patient with a cleft that responds to users’ control-based commands. While in the immersive environment, users are guided by visual and audio feedback. The duration of the VR module was approximately 8 min. The headset model used for the simulation was Meta Quest 2 (Meta, Menlo Park, CA).
Study Design
Plastic surgery trainees from a single institution were invited to complete the VR-based cleft simulation class. As this constituted an education quality improvement study, IRB was exempt. Following general instructions on VR operability including remote control use and how to navigate the virtual environment, participants entered a virtual operating room in which the senior surgeon would perform the Furlow palatoplasty including the surgical markings. All participants would have an unobstructed view of the surgical field and the operative (senior) surgeon would explain all procedural steps in a similar manner as performed in an operating room setting (Supplementary Video A). A stable Wi-Fi connection was needed to complete the simulation class. The VR devices were connected to a portable hotspot at each class. No more than 3 devices at a time were connected to the hotspot to ensure a stable internet connection.
Data Collection
To assess the participants’ experience with the virtual reality simulator, validated deidentified pre- and postsimulator surveys were completed electronically through Qualtrics. The purpose of the presurvey was to assess each participant's prior experience with virtual reality, interest in the technology as an educational tool, and experience level with formal cleft surgery training (see document, Supplemental Digital Content 1). The survey scores were based on a 5-point Likert scale, with 1 being “strongly disagree” and 5 being “strongly agree.” The postsurvey consisted of similar presurvey questions, assessing postintervention confidence in simulation tasks, trainees’ opinions of the fidelity of the simulation model as well as a modified version of the Student Evaluation of Educational Quality (SEEQ) survey (see document, Supplemental Digital Content 2).
The SEEQ Survey
The SEEQ survey is a validated instrument to assess tools of higher education by learners. The SEEQ survey asked residents whether the VR simulation workshop was stimulating, increased interest, provided a better learning experience, was clear, was effective in teaching, and whether they would recommend it to others.18,19 This portion of the postsimulation survey was also scored on the same 5-point Likert scale.
Results
Prior Experience of Participants with VR and Cleft Surgery
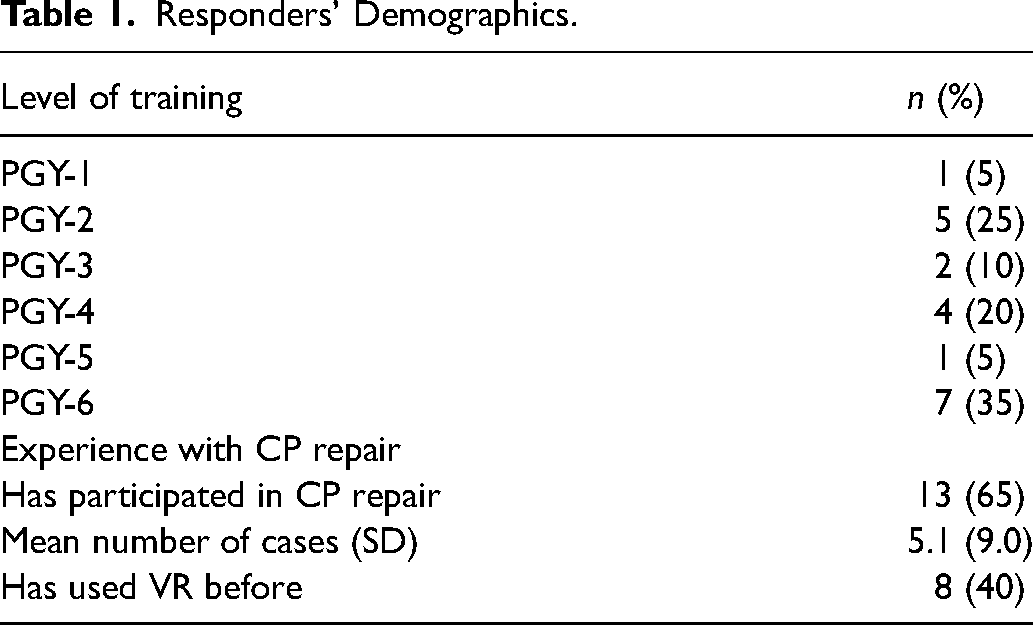
A total of 20 residents participated in the simulation experience. Eight participants (40%) confirmed prior experience with VR, here defined as any prior educational or leisure exposure to technology. Furthermore, thirteen participants (65%) reported previous active participation in cleft surgery (20% in medical school, 100% in residency) with an average of 5.1 cases in those with previous experience (Table 1).
Responders’ Demographics.
Pre- and Postintervention Confidence with VR Simulation
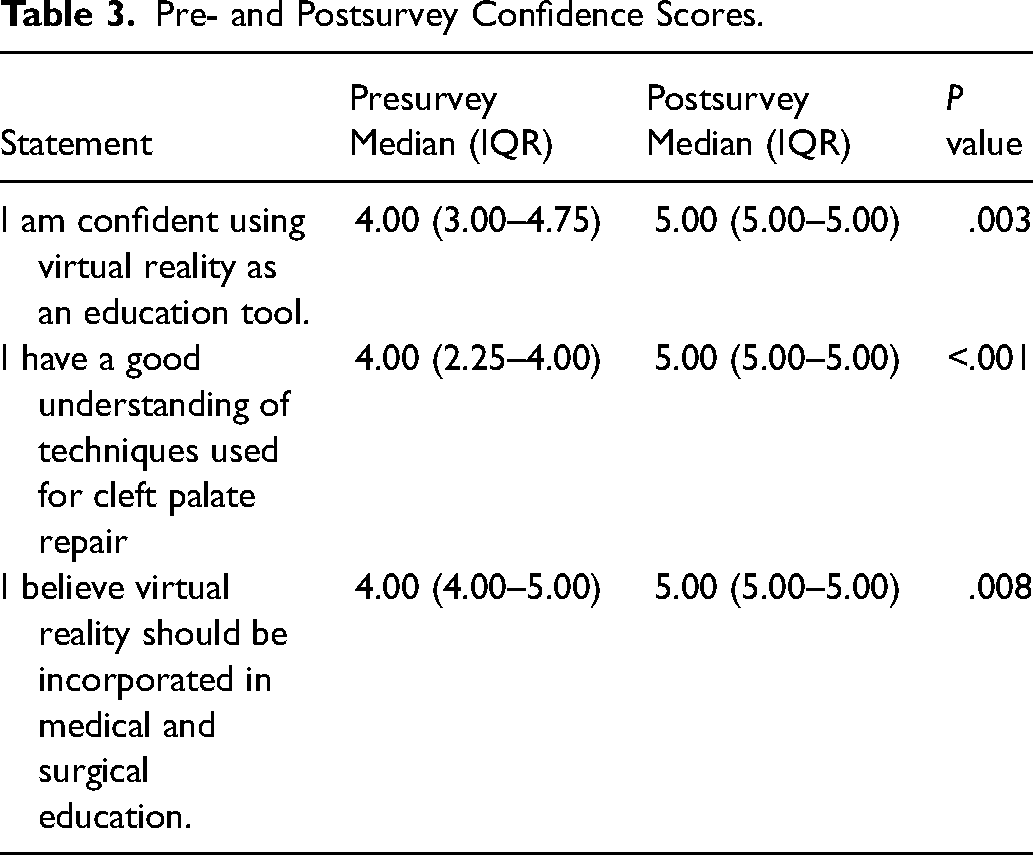
In assessing participants’ confidence with cleft palate repair, the preintervention median confidence score was 4.00 (IQR, 3.00-4.75). After the simulation, there was a statistically significant increase (P = .003) in the median confidence score to 5.00 (5.00-5.00). Participant understanding of the Furlow technique for cleft palate repair started at a median of 4.00 (2.25-4.00) and significantly increased to 5.00 (5.00-5.00) postsimulation. Prior to the simulation, trainees were somewhat favorable to the incorporation of VR in residency training on incorporating VR with a median response of 4.00 (4.00-5.00). Their opinion positively increased following the workshop 5.00 (5.00-5.00), P = .008 (Table 2, Figure 1).
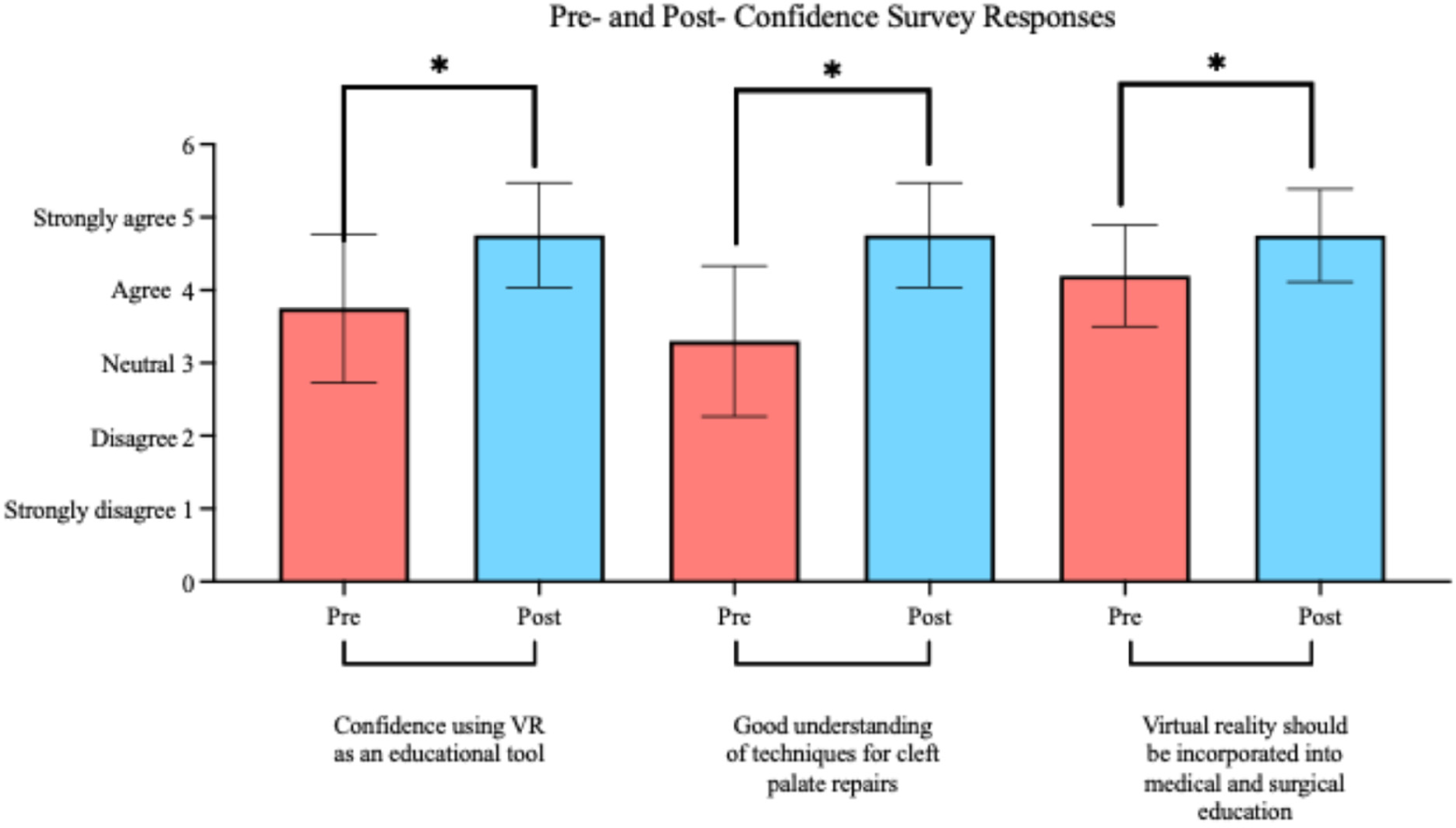
Pre- and postconfidence survey responses.
SEEQ Questionnaire and Dimensions of Learning Scores.
Evaluation of VR Educational Experience
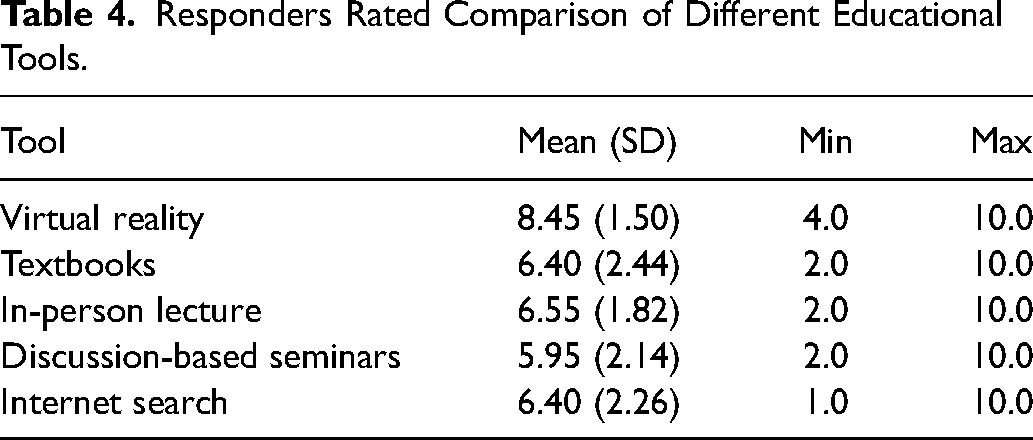
In the SEEQ survey, trainees reported a high degree of satisfaction with the virtual reality class as a tool for learning cleft palate reconstruction. The majority strongly agreed that the simulation was stimulating (95%), increased their interest in pediatric plastic surgery (65%), believed that the VR instructions were clear (75%) and that VR is an effective tool for teaching cleft lip and palate reconstructive techniques (75%), and would recommend the VR workshop to others interested in learning more about cleft lip and palate (90%) (Table 3, Figure 2). Finally, on a scale from 0 to 10 with 10 being the most useful, when compared to other traditional surgical technique learning modalities, trainees rated the workshop higher (8.45) as compared to textbooks (6.40), in-person lectures (6.55), discussion-based seminars (5.95), and internet searching (6.40), Table 4. Furthermore, trainees stated that they felt somewhat (50%) or extremely comfortable (30%) performing the simulation alone after the initial experience. (Table 3).
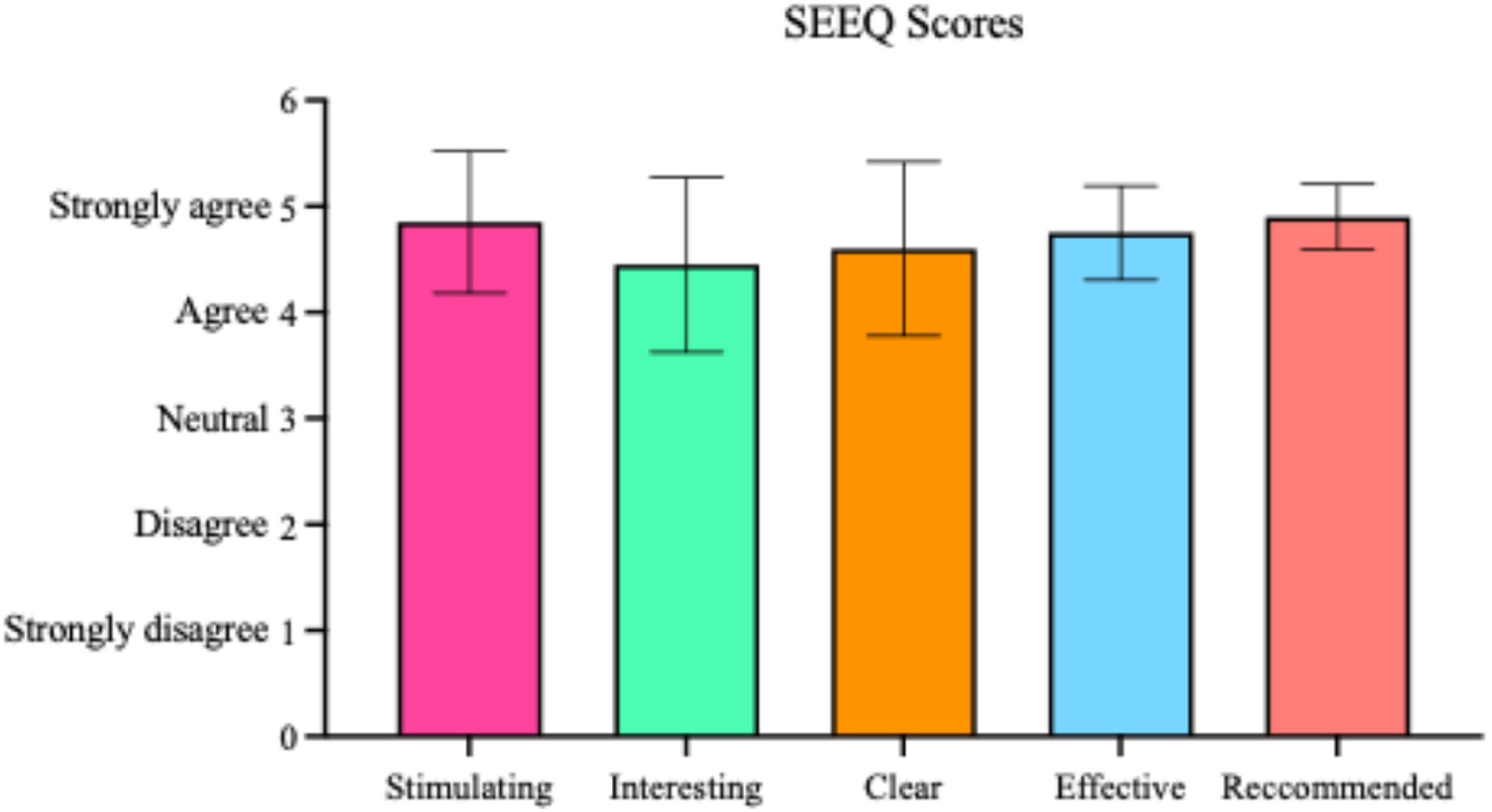
SEEQ scores.
Pre- and Postsurvey Confidence Scores.
Responders Rated Comparison of Different Educational Tools.
Simulation Feedback
Informal feedback on the virtual reality technology was very positive, other than 1 participant (5%) who completed the exercise but reported discomfort in the form of nausea. Concerning positive feedback, respondents mentioned the improved visualization of the surgical field when compared to in-person visualization as a first or second surgical assist. In addition, trainees were excited about the possibility of other surgical techniques also migrating to the virtual environment as it gives them “a foundation stone before stepping in the operating room and participating in a ‘real’ surgery.” Constructive feedback from participants included an improved easiness of situating themselves in the virtual operating room to allow for optimal visualization as well as improvements in the quality of the VR headset as 1 individual felt it to be “blurry,” which can be corrected by adjusting the headset lenses for interpupillary distance, i.e., to align the lenses with the width of the eyes. All respondents nonetheless agreed that if given the opportunity, they would want to re-utilize the simulation before a future surgery performing a Furlow reconstruction.
Discussion
This study indicates that plastic surgery residents positively embraced the VR simulation workshop as an effective educational resource for surgical skill acquisition. Not only did trainees feel more comfortable with the technique, but they found the simulation and technology effective, stimulating, and a practical tool in preparation for in-person procedures. These findings are consistent with prior studies and indicate the potential application of this surgical educational technology in cleft care.14,20
As surgical procedures become increasingly complex and training hours have become limited, there is a growing concern for trainee unpreparedness during residency, particularly for cases that are uncommon and anatomically complex.21 Previous studies has confirmed that surgical skill is acquired through continued practice and is significantly improved with an increase in caseload.16,22 Although the authors do not believe that virtual reality will substitute real in-person surgical experience and training, we believe that this training resource, like other digital simulators, can help trainees understand the anatomic concepts and steps of a surgical procedure more effectively than a textbook or video while affording a realistic, immersive learning experience. This can result in a more efficient understanding of the 3-dimensional aspects of surgery prior to entering the operating room. Although we believe that full user immersion offered by virtual reality can provide distinct benefits to real-time clinical decision-making and surgical understanding in cleft care, to an extent not offered by synthetic models, animal models, and cadavers, these types of analysis are pending.23
Participants in this study felt more comfortable with cleft palate reconstruction after the simulation and would enjoy revisiting it before a real-life surgery. They also subjectively ranked the tool higher than other forms of currently available training resources, including print and websites. This early study suggests that VR simulations may have benefit to cleft surgery training and could permit remote self-directed learning and gradual proficiency acquisition in preparation for operating room training.
Apart from its potential benefits on local and global education, the virtual operating room setting allows surgeons to learn and practice complex procedures before encountering a real case. This early exposure and practice can increase patient safety.24,25 As seen in other specialties, VR has been demonstrated to reduce error rates in trainees and improve operating room performance when compared to controls exposed to traditional learning methods.26–29 Furthermore, surgical planning has also undergone initial testing into the VR space.30,31 By uploading preoperative computed tomography and/or magnetic resonance imaging into VR software, surgeons may visualize an individual patient's anatomy, and anatomical borders, creating a personalized preoperative planning approach.15,31,32 This allows for surgeons to practice performing intended surgeries in the virtual environment. While to the authors’ best knowledge the application of this technology to pediatric plastic and cleft surgery has yet to occur, other plastic surgery subspecialties as well as other surgical fields have seen improvements in surgical access and effectiveness with its use, translating to improved patient outcomes.27,33–35
From a global health perspective, while reduced trainee hours have been a reality in high-income nations, low and middle-income countries also face an added problem when it comes to surgical education: the lack of in situ professional educators. For example, of the 17 West African nations, only 4 have subspecialty training.36 This lack of access to subspecialty education impacts the desire of African medical students to remain and practice in their native countries: for instance, 68% of Ghanaian-trained medical graduates emigrated between 1993 and 2000; this is also seen in the case of Nigerian-trained students whose majority plans to practice abroad upon graduation.37,38 While in-person training and educators are necessary, providing additional resources such as VR to areas of need could alleviate these educational disparities.15 The lack of trained local surgeons and expense of surgical care also pose major obstacles to cleft-affected infants and children receiving corrective surgery. Globally, 5 billion people have no access to surgical facilities.39 The morbidity and mortality incidence rates in untreated cleft patients exceed 100 000 in low-resource regions highlighting the need to expand cleft care training opportunities.40 Previous work with an online cleft simulation available on both smartphones and computers has demonstrated the potential of technology in supporting local trainees in low and middle-income nations.14 Thus, virtual reality would go even beyond a simulation-only instrument as it allows educators in high-resource institutions to provide simultaneous education without the need for travel or geo-socio-political barriers.15
Finally, concerning user-friendliness, the participants in the reported limited physical discomfort during or following the simulation. Previously reported simulation workshops using similar technology to practice upper airway management in pediatric patients, reported episodes of nausea, lightheadedness, and dizziness. Known as “cybersickness,” this constellation of symptoms stems from a “discrepancy between the sensory signals, which provide information about the body's orientation and motion” and is not rare in those using virtual reality.41 As severity of symptoms has been associated with duration of VR exposure, the teaching of full surgical cases may be precluded in those susceptible to vertigo-like symptoms. Unfortunately, these symptoms do not improve upon immediate VR discontinuation but can linger for several hours following exposure.42 Even if there are current developments aimed at preventing cybersickness such as designing VR environments with stable visual references, user attention and advising is needed prior to subjecting any trainee to the technology.
Criticisms of this technology include the equitability as it relates to cost and access to reliable internet connectivity for use. Currently the VR headset used in this study is marketed at 430 dollars—notably lower than most smartphones.43 This is further highlighted by how cost-prohibitive traditional methods of learning such as textbooks can be.15 Finally, concerning internet connectivity, a recent United Nations report indicated a continuous rise in access to the internet among low and middle-income nations, especially in areas such as Latin America and Sub-Saharan Africa where the burden of uncorrected cleft lips and palates is the highest.44,45 Even with these shortcomings, the present and past studies on VR application in the setting of cleft palate care indicate that even without prior VR experience, trainees found the simulation to be easily learned and valuable, demonstrating that the technology can be applied to low- and middle-resource centers alike.
Limitations
The present study is limited by its small sample size and single-institution nature. Additionally, as this is a single-institution study conducted within a single residency program, biases exist which may skew participant responses to be overall more favorable of the VR simulation. However, given the demanding clinical schedule of trainees and surgeon faculty, close coordination between the study team and the residents allowed us to obtain a sample size of 20 residents across different levels of training. Furthermore, trainees from high-resource settings may have their own biases regarding the positiveness and traction of technology on their education which may not be generalizable to trainees in other specialties, levels of training, or geographical areas. Nonetheless, the authors believe the present simulation to be the first of its kind and additional modifications will be made with improve user experience and incorporate additional cleft training modules. This is an early report regarding the potential benefit of this technology. Future studies will aim to validate these findings by conducting similar studies utilizing this technology in both high- and low-resource settings and increase the generalizability of this work.
Conclusion
Virtual reality-based simulation workshops for teaching unilateral Furlow repair can significantly increase trainee confidence with cleft palate repairs and interest in pediatric plastic surgery. Broader implications for global surgery in both high- and low-resource settings include collaborating with remote trainees lacking access to surgical facilities and equipment, enhancing patient safety through deliberate virtual practice, and improving the standards by which formal surgical education is trained. Participants found this simulation an effective teaching tool and would recommend the workshop to others.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251328789 - Supplemental material for Novel Virtual Reality Simulator for Cleft Palate Surgery Training: An Assessment of Educational Feasibility and Traction Among Plastic Surgery Residents
Supplemental material, sj-docx-1-cpc-10.1177_10556656251328789 for Novel Virtual Reality Simulator for Cleft Palate Surgery Training: An Assessment of Educational Feasibility and Traction Among Plastic Surgery Residents by Leya Groysman, Matteo Laspro, Allison L. Diaz, Gregory Dorsainville, Aaron Oliker, Anne Arnold, Liliana Camison and Roberto L. Flores in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656251328789 - Supplemental material for Novel Virtual Reality Simulator for Cleft Palate Surgery Training: An Assessment of Educational Feasibility and Traction Among Plastic Surgery Residents
Supplemental material, sj-docx-2-cpc-10.1177_10556656251328789 for Novel Virtual Reality Simulator for Cleft Palate Surgery Training: An Assessment of Educational Feasibility and Traction Among Plastic Surgery Residents by Leya Groysman, Matteo Laspro, Allison L. Diaz, Gregory Dorsainville, Aaron Oliker, Anne Arnold, Liliana Camison and Roberto L. Flores in The Cleft Palate Craniofacial Journal
Footnotes
Contribution
L.G., M.L., and A.L.D., helped to organize and run each VR session. L.G. and M.L. were responsible for drafting and revising the manuscript with the support of R.LF., L.C., and A.A. A.L.D. created the tables and figures. G.D. consulted on all technical difficulties. A.O. created the software for the simulator. R.L.F. conceived the idea and supervised the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
As this constituted an education quality improvement study, IRB was exempt.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.