
Abstract
Objective
Beyond aesthetic implications, craniosynostosis can profoundly impact neurocognitive development. There is a notable gap in standardized methodologies for identifying which of these patients are at-risk for developing adverse neuropsychosocial outcomes through screening techniques. This research aims to identify and recommend a standardized, routine approach inclusive of free or low-cost screening instruments for patients with craniosynostosis that are easily administered in clinic with or without a trained examiner.
Design
A systematic review was conducted. Data related to various developmental assessments were extracted and subsequently reviewed by two trained neuropsychologists for analysis, categorization, and recommendation.
Main Outcomes Measures
Neurocognitive screening assessments for patients with craniosynostosis.
Results
In total, 114 different tests regarding neurocognitive examination of patients with craniosynostosis were cited. We identified six areas of neuropsychosocial development that are relevant for routine screening: Development, Social-Emotional/Behavioral, Adaptive Functioning, Academic Achievement, Autism, and ADHD/Attention. Within each category, screening recommendations are made, including instruments that are free or low-cost and can be easily administered in clinic with or without a trained examiner.
Conclusions
Literature supports the impact of craniosynostosis on neuropsychosocial development, so we urge teams to screen patients from an early age using these suggestions as they are free or relatively low-cost, can be administered to a wide range of patient ages, and can be administered in clinic with or without a trained examiner. This study serves as a starting point towards a more standardized approach to effectively evaluate and address the neurocognitive implications of craniosynostosis, ultimately enhancing patient care and treatment outcomes.
Keywords
Introduction
Craniosynostosis, a congenital malformation of the skull, arises from the premature fusion of one or more of the cranial sutures. These critical fibrocellular structures act as expansion joints between the bones of the skull, accommodating the brain's rapid growth during infancy. Under normal circumstances, the calvarial sutures adapt to changes in intracranial pressure and mechanotransduction signals emanating from the dura mater, thereby facilitating proportional skull expansion. 1 However, when this intricate cell signaling pathway is disrupted, craniosynostosis ensues, causing an abnormal cranial shape.
This condition is broadly categorized into two main types: syndromic and nonsyndromic craniosynostosis. Syndromic craniosynostosis is associated with known genetic syndromes, such as Crouzon, Apert, Muenke, Pfeiffer, and Saethre-Chotzen syndromes—each of which involve craniosynostosis along with their own characteristic set of congenital anomalies. 2 In contrast, nonsyndromic craniosynostosis, characterized by the premature fusion of skull sutures, occurs without the presence of additional symptoms or anomalies typically linked to genetic syndromes. 3 Both variants can affect single or multiple sutures, with syndromic cases more frequently involving multiple sutures and presenting with greater deformity severity.
Beyond the aesthetic implications, craniosynostosis can profoundly impact neurocognitive development. The interplay between anatomical structure and physiological function is particularly evident in the context of cranial development. A normocephalic skull, considered the optimal shape for accommodating brain volume, exemplifies this relationship. Alterations in skull shape can lead to increased intracranial pressure, changes in cerebral blood flow, and potential developmental irregularities.
Children with craniosynostosis frequently encounter challenges in areas such as academic performance, 4 motor skill development, 5 language acquisition, 6 and social interactions. 7 For example, previous studies have found that children with surgically corrected single-suture craniosynostosis consistently scored lower on language and memory measures when compared to their non-affected peers.6,8 Both noted that this difference was most stark amongst individuals with unilateral coronal craniosynostosis, with Chieffo et al. positing that this finding may be explained by early persisting effects on the frontal lobe. This correlation underscores the intricate connection between the physical structure of the skull and the functional areas of the brain. The importance of addressing these neurocognitive aspects in craniosynostosis management cannot be overstated. As surgeons, we must encompass a comprehensive understanding of the functional outcomes of craniosynostosis.
However, the field faces a notable gap in standardized methodologies for neurocognitive screening in this patient population. Andrews et al. underscore the absence of consistent assessment tools, covering areas such as verbal, motor, cognitive, and psychosocial development, within the conventional treatment framework for patients with craniosynostosis. 9 The selection of appropriate neurocognitive screening tools is pivotal, as it significantly influences the evaluation of patient progress, timely patient referral if necessary, and the efficacy of interventions. This research aims to delve into the array of neurocognitive scales utilized in craniosynostosis studies and seeks to identify, compare, and consolidate these tools. Through this investigation, we aim to contribute to the establishment of a more standardized and effective approach to identifying patients who are at-risk of developing adverse neurocognitive implications of craniosynostosis through screening techniques, ultimately enhancing patient care and treatment outcomes.
Methods
Systematic Review Protocol
This systematic review was deemed exempt from institutional review board registration. It was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search Approach
A comprehensive search was conducted in PubMed up to October 2023, focusing on studies evaluating the neurodevelopmental status of patients with craniosynostosis. The search strategy and terms, formulated by the authors and refined with the assistance of a medical librarian, were: “craniosynostosis AND (neurodevelopment* OR delay OR cogniti*).” No specific filters or limits were applied to the search, which resulted in 821 unique entries. Duplicate studies were identified and extracted manually.
Criteria for Inclusion and Exclusion
The primary objective of our study was to analyze the specific assessments used to evaluate psychosocial and neurocognitive development in patients with craniosynostosis. For initial inclusion, abstracts needed to describe one or more patients with craniosynostosis undergoing neurocognitive assessment or diagnosed with developmental delay. Eligible cases included any age group and any form—syndromic or nonsyndromic—or location—sagittal, coronal, lambdoid, metopic, single, multi-suture—of craniosynostosis. Exclusion criteria encompassed non-English language articles, studies on non-human subjects, basic science research, cases without craniosynostosis, reports omitting neurodevelopmental discussion, videos, and secondary literature such as reviews and editorials.
The review of full-text articles was next. Inclusion required (1) patients with craniosynostosis and (2) explicit mention of a specific, named neurocognitive or psychosocial development assessment. Articles were excluded if they either described or diagnosed developmental delays without disclosing the assessment method used.
Study Selection and Data Compilation
Two authors independently and manually reviewed titles and abstracts from the initial search results. Full-text articles meeting the initial criteria were further analyzed by the same authors. In cases of uncertainty regarding inclusion or exclusion, the principal investigator made the final decision. Data related to various neuropsychosocial development measurements were extracted using a standardized form and independently reviewed by two trained neuropsychologists at different institutions for categorization and analysis of best-use screening practices. Upon initial disagreement, discussion occurred between the two neuropsychologists until a consensus was reached. Screening assessments were deemed as best practice if they were characterized by all of the following attributes: 1) empirically validated for use in the appropriate age range; 2) easy to perform without the presence of trained examiners; and 3) free or low-cost.
Results
Literature Search and Study Selection
Eight hundred ninety-six articles were identified from the database searched—75 of which were found to be duplicates. The titles and abstracts of the remaining 821 studies were analyzed, and 319 were relevant to neurocognitive screening tools for craniosynostosis and underwent full-text review. Results of the study selection process are reflected in Figure 1. One-hundred-ninety-three were excluded for the following reasons: studies did not mention a specific neuropsychological test (n = 166), studies described irrelevant or inappropriate cognitive outcomes in patients with craniosynostosis (n = 8), studies included non-clinical assessments of the patients’ cognitive delay (n = 7), studies were published in a non-English language (n = 6), and studies only described patients with positional plagiocephaly rather than craniosynostosis (n = 6).

A photo of the screening process in accordance with PRISMA guidelines.
Study Characteristics
A total of 126 studies met all screening criteria and were included in our review. A full reference list of the included articles is provided in Table, Supplementary Digital Content 1. Of these papers, 16 were case reports, 15 were case series, 21 were cross-sectional studies, 19 were retrospective reviews, and 55 were prospective cohort studies. The oldest included paper was published in 1981, and the most recent study that met inclusion criteria was published in the fall of 2023. The youngest patient assessed was one month old, and the oldest patient was 50 years of age at the time of testing. 42 studies (31.3%) examined individuals with known syndromic craniosynostosis. Analyzed outcomes included specific named tests of mental or motor development and were grouped into one of the following categories based on the test's utility: Development, Social-Emotional/Behavioral, Adaptive Functioning, Academic Achievement, Autism Spectrum Disorder (ASD), Attention Deficit Hyperactive Disorder (ADHD)/Attention, Executive Functioning, IQ/Cognition, Language, Memory, Motor: Gross/Fine, Visual-Motor, and Imaging.
A total of 114 different tests regarding neurocognitive examination of patients with craniosynostosis were cited. A full list of tests along with references for included articles can be found in Table, Supplemental Digital Content 1. Seventy unique assessments were cited in only one publication. The most commonly administered test was the Wechsler Intelligence Scale for Children (WISC), which was utilized in 38 (30.2%) included studies. Minimum age of WISC administration was six years, and maximum patient age was sixteen years. The second most commonly used test was the Bayley Scales of Infant and Toddler Development (BSID), which was utilized on a younger patient cohort. At least one edition of the BSID was administered to patients between the ages of 1.5 and 43 months old and was cited by 35 (27.8%) included papers. Both of these tests require a trained assessor—such as a trained neuropsychologist, developmental pediatrician, pediatric psychologist, etc.—for proper implementation.
Assessment Analysis
This systematic review included 126 studies that cited specific, clinically-conducted neurocognitive assessments for patients with craniosynostosis.
In alignment with our aim to focus on screening assessments, further emphasis was placed on recognizing low-cost, easy-to-administer screening instruments for routine use by anyone on the healthcare team—such as nurses or medical assistants—to identify patients at risk in each area. We have identified six areas of neuropsychosocial development that are most relevant for routine screening for patients with craniosynostosis: Development, Social-Emotional/Behavioral, Adaptive Functioning, Academic Achievement, Autism Spectrum Disorder, and ADHD/Attention.
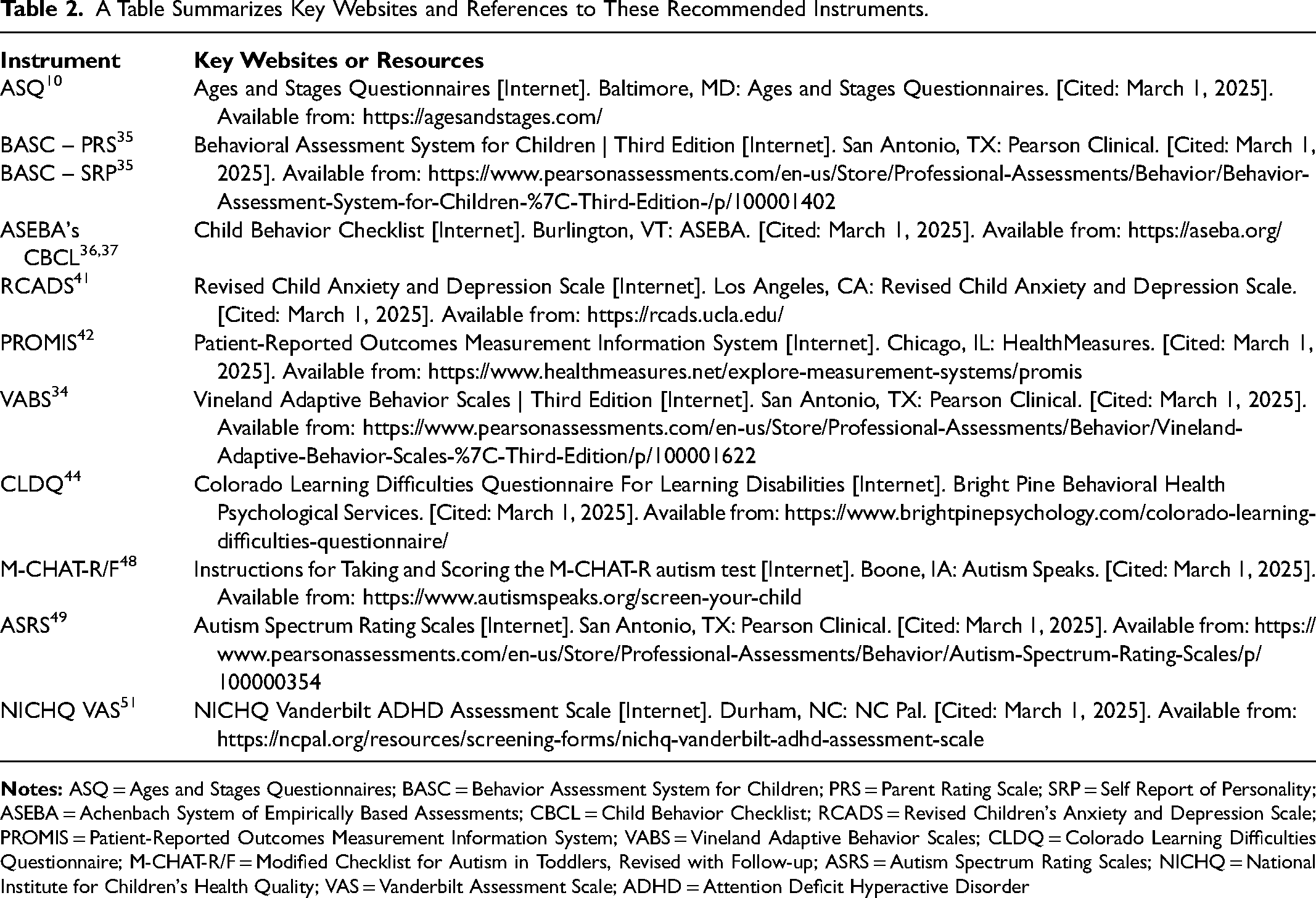
Within each category, we propose best-use screening practices for use across resource-limited and resource-extensive settings. Table 1 summarizes these recommendations and includes information about each instrument's utility, length, cost, available languages, and personnel requirements. Table 2 summarizes key websites and references to these recommended instruments.
A Table Summarizing Screening Recommendations, Including Information About Each Instrument's Utility, Length, Cost, Available Languages, and Personnel Requirements.
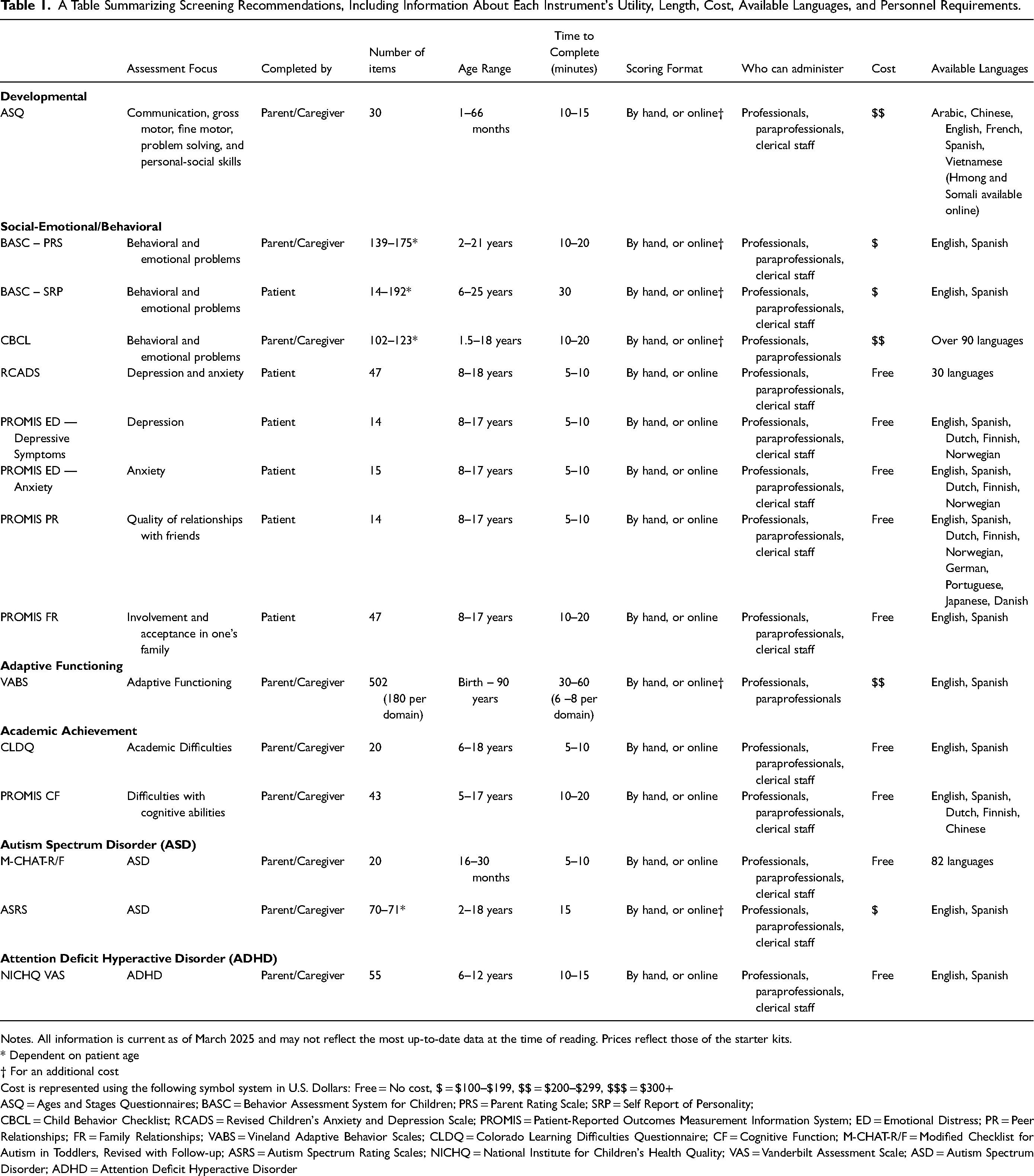
Notes. All information is current as of March 2025 and may not reflect the most up-to-date data at the time of reading. Prices reflect those of the starter kits.
* Dependent on patient age
† For an additional cost
Cost is represented using the following symbol system in U.S. Dollars: Free = No cost, $ = $100–$199, $$ = $200–$299, $$$ = $300+
ASQ = Ages and Stages Questionnaires; BASC = Behavior Assessment System for Children; PRS = Parent Rating Scale; SRP = Self Report of Personality;
CBCL = Child Behavior Checklist; RCADS = Revised Children's Anxiety and Depression Scale; PROMIS = Patient-Reported Outcomes Measurement Information System; ED = Emotional Distress; PR = Peer Relationships; FR = Family Relationships; VABS = Vineland Adaptive Behavior Scales; CLDQ = Colorado Learning Difficulties Questionnaire; CF = Cognitive Function; M-CHAT-R/F = Modified Checklist for Autism in Toddlers, Revised with Follow-up; ASRS = Autism Spectrum Rating Scales; NICHQ = National Institute for Children's Health Quality; VAS = Vanderbilt Assessment Scale; ASD = Autism Spectrum Disorder; ADHD = Attention Deficit Hyperactive Disorder
A Table Summarizes Key Websites and References to These Recommended Instruments.
Discussion
Currently, there is a lack of standardized guidelines concerning neurocognitive screening for patients with craniosynostosis, despite an abundance of evidence demonstrating worse cognitive, behavioral, and psychosocial outcomes for children with craniosynostosis when compared to their healthy peers.10–13 The number of different tests that were encompassed in this systematic review underscores the incongruity of best clinical practices utilized for developmental screening of patients with craniosynostosis amongst the craniofacial community.
As Kapp-Simon et al. point out in a review paper focused on neurodevelopment in children with single-suture craniosynostosis, there are two predominant theories explaining the causal relationship between craniosynostosis and developmental abnormalities in these patients. First, restricted cranial growth secondary to premature suture ossification leads to increased intracranial pressure that, in turn, may adversely impact brain growth and neurocognitive development—a hypothesis that has been debated since first presented in 1982.14–16 Second, the abnormally shaped skull caused by craniosynostosis may cause secondary cerebral deformation that impacts cortical connectivity and functioning.15,17 The exact causational relationship between craniosynostosis and developmental delay remains unknown, but it is reasonable to believe that this relationship is complex and multifactorial.
The association between craniosynostosis—in its many forms—and abnormal neuropsychosocial outcomes is a known area of interest in previous literature. In a systematic review by Speltz et al., authors noted that 35–40% of reviewed cases described an “adverse neurocognitive outcome”—defined by the authors as “learning disability, language impairment, test scores below a defined threshold, or ‘behavioral or cognitive abnormality’”—with no one particular suture being linked with higher risk of problems.18–20 In a separate work that assessed 125 infants with single-suture craniosynostosis who had not yet undergone surgical repair, Speltz et al. compared them to a matched control population and found that affected infants scored significantly lower on tests of mental and psychomotor development, though language development showed no difference. 21 Similarly, Da Costa et al. found that infants with untreated nonsyndromic single-suture craniosynostosis scored significantly lower than the normative population for mental and motor assessments, with this population being 2.2 times more likely to display both gross and fine motor delay than the comparison group. 22 When considering the role of age, Sidoti et al. found that only 17.6% of patients with isolated metopic craniosynostosis below the age of five had neurocognitive or behavioral issues, while 47.4% of similar patients over the age of five had such difficulties. 23 In a series of broader longitudinal studies, authors noted that, depending on the assessment, between 22% to 28% of the studied children with surgically-treated single-suture craniosynostosis scored in the delayed range (compared to the 10–20% of controls) at age three, which rose to over 42% of the same cohort at school-age.24,25
Further, syndromic craniosynostosis has been found to manifest with a wide range of neurocognitive and psychosocial outcomes.26–28 Studies have shown that individuals with syndromic craniosynostosis are at a higher risk for intellectual disabilities than the general population, with risk of Apert syndrome being the highest.3,28,29 Maliepaard et al. also noted that those with syndromic craniosynostosis were more at risk for social, behavioral, and attention difficulties. 3 However, the research team discovered that the mean Full Scale IQ (FSIQ) scores of patients with syndromic craniosynostosis were within the normal range. Da Costa et al. similarly found that, despite being of significantly lower intelligence than the normative population, individuals with syndromic craniosynostosis often displayed FSIQ scores within the normal range. 26 Yet, patients with syndromic craniosynostosis scored significantly lower in both verbal and nonverbal (visual-spatial) intelligence than their counterparts with nonsyndromic craniosynostosis. 26 The authors, therefore, emphasize the importance of recognizing the diversity of possible outcomes associated with such syndromes.
Existing literature underscores the necessity of timely and accurate assessment and management of neuropsychosocial outcomes for patients with both syndromic and nonsyndromic craniosynostosis. While much effort has been put forth in examining the neurocognitive and developmental repercussions of craniosynostosis, we were unable to identify a contribution to the literature that has analyzed the screening tests being utilized as part of a multidisciplinary craniofacial clinic.
Recommendations
In an ideal situation, patients with craniosynostosis will receive care in a multidisciplinary clinic that includes a specialist (eg, developmental pediatrician, neuropsychologist, pediatric psychologist or psychiatrist) who is trained to administer and interpret various neurodevelopmental assessments directly with the patient as well as provide recommendations for intervention in the clinic setting. In fact, the American Cleft Palate Craniofacial Association (ACPA) requires that craniofacial teams have access to a psychologist capable of administering such tests. 30 Unfortunately, the extent of involvement and access vary across settings, due to a range of issues including a lack of funding or a limited clinical capacity of available providers in these subspecialities.
Given this reality, we offer the following suggestions based on this systematic review and urge teams to screen patients from an early age. In addition to providing suggested age-ranges for administration, each measure suggested is a screening questionnaire that is free or relatively low-cost and can be administered in the clinic setting with or without a trained examiner as an initial assessment, which may then necessitate follow-up with more specific and time-intensive instruments. For those who may not have a trained neuropsychologist or similar professional as part of their team, we recommend creating a list of providers in their system or region to whom the clinic can refer if, and when, elevations are noted on any screenings. Due to time and accessibility constraints, an additional, more specific screening assessment in concerning areas may, in some cases, be appropriate prior to referral for full neurodevelopmental workup. Finally, we emphasize that these suggestions need not necessarily be deemed the comprehensive solution but, instead, as a first guiding step for those seeking direction. We encourage each clinic to consider their unique patient population and select the combination of initial screening instruments that most effectively address clinical concerns while lowering the burden on both patients and practitioners.
The following suggestions are organized by the specific neuropsychosocial domains they asses, rather than in chronological order. It is of note that these categories represent important areas of concern regarding patients with craniosynostosis and that there is considerable overlap between them within individual tools.
Developmental Screening
Developmental screening typically involves comprehensive direct or indirect assessments of cognition, language, social-emotional behavior, adaptive functioning, and fine and gross motor development, depending on the specific test and the age of the individual undergoing screening. The American Academy of Pediatrics currently recommends general developmental screening for all children at their nine-, eighteen-, and thirty-month routine health visits. 31 However, because individuals with craniosynostosis are considered high-risk for developmental delay, earlier and more frequent screening is warranted.
For patients with craniosynostosis, we recommend developmental screening at every clinic visit from one month to five years of age using the Ages and Stages Questionnaire (ASQ). 32 The ASQ screens for development regarding communication, gross and fine motor skills, problem solving abilities, and personal-social behaviors and is completed by the parent. 33 Further, it is relatively low cost, quick to both administer and score, and able to be conducted by clerical staff. If there is a cause for concern at any time during or between screenings, a more comprehensive evaluation or referral to a specialist may be indicated.
Social-Emotional/Behavioral
Given the emotional vulnerability of this particular population, clinics may also wish to consider an annual parent-report of emotional functioning beginning around the age of two or three years, using the Behavior Assessment System for Children (BASC) or the Achenbach System of Empirically Based Assessments’ (ASEBA) Child Behavior Checklist (CBCL).34–36 Beyond this study, both were identified in a systematic review that examined known psychosocial screening instruments for children with long-term physical conditions. 37 Both instruments assess similar constructs relating to behavioral functioning, with both including measures of internalizing (ie, anxiety, depression) and externalizing (ie, hyperactivity, aggression, conduct) behaviors. 38 Additionally, both include subscales that evaluate social skills like cooperation, the ability to establish and maintain friendships, and communication.
At present, the two are comparable in administration time and starter kit pricing, with the BASC being slightly more affordable than the CBCL. The BASC, however, is only available in English and Spanish, and, for this reason, some prefer the CBCL, which is available in over 90 languages. Both can be administered and scored by hand, or online for an additional cost. The online scoring system for the BASC requires a yearly subscription, while the ASEBA's scoring program, which includes that for the CBCL and is a one-time cost, necessitates clinical computer compatibility with a Compact Disc Read-Only Memory (CD-ROM). Here, we again emphasize each clinic's consideration of their resources and the needs of their particular patient population.
Further, it is essential to begin screening for social-emotional issues by eight years of age with self-report instruments, with the recommended tool being the Revised Child Anxiety and Depression Scale (RCADS) or the Patient-Reported Outcome Measurement Information System (PROMIS) Emotional Distress—Depressive Symptoms and Emotional Distress—Anxiety pediatric measures.39–41 Additionally, assessment of social functioning—including feelings of acceptance among family and peers or experiences with bullying—is important at this age as well. Therefore, the PROMIS social health measures which include the Peer Relationships and Family Relationships forms are recommended at eight years of age as well. The short forms of these PROMIS measures are appropriate in the clinic setting as well to reduce time burden. Please be aware that emotional screening measures will include “critical” items pertaining to suicide and self-harm. These items must be checked immediately during the clinic appointment and addressed if endorsed.
Adaptive Functioning
Adaptive functioning refers to age-appropriate skills that are necessary for children to complete activities of daily living and to communicate their needs. This is crucial for overall patient well-being, development of independence, and optimal quality of life. When patients turn five-years-old, providers should consider screening for adaptive functioning using the Vineland Adaptive Behavior Scales (VABS), with reassessment once every two or three years. 42 Clinical judgment should guide the decision to administer either the comprehensive assessment or only the relevant subscales.
Academic Achievement
Additionally, this patient population is particularly vulnerable to learning difficulties.23,43 Screening is difficult for this particular concern. Although not seen in our review of the literature, we recommend use of the Colorado Learning Difficulties Questionnaire (CLDQ) beginning at age 6 years, with reassessment as needed for the child. 44 This test is free and open-source. Alternatively, the PROMIS Parent-Proxy Item Bank – Cognitive Function or the School Competence Scale of ASEBA's CBCL are appropriate beginning at the age of five or six years, respectively. 45
Autism Spectrum Disorder
Screening for Autism Spectrum Disorder (ASD) is also highly recommended in this patient population. While the American Academy of Pediatrics recommends routine screening for ASD at 18 and 24 months of age for the general population, earlier screening is warranted for individuals with craniosynostosis. Although not seen in our review of the literature, we suggest the use of the Modified Checklist for Autism in Toddlers-Revised with Follow-up (M-CHAT-R/F), which is a 20-item questionnaire filled out by the child's parent or caregiver, from ages 16 months to 30 months. 26 The M-CHAT-R/F is truly free and open-source and encompasses one of the youngest age ranges to whom it can be administered. Additionally, this screening tool can take between five to ten minutes to complete, is currently available in 82 languages, and can be scored by any clerical staff in as little as two minutes. A systematic review of ASD screening tools identified the M-CHAT-R/F as an appropriate instrument for this age range given its strong sensitivity and specificity performance.46,47 Subsequently, the Autism Spectrum Rating Scale (ASRS) can be administered to patients from age 30 months onwards.48,49 Screening for Autism is only necessary at the first appointment, unless caregivers express new concerns later on.
It is important to note that comprehensive tools like the BASC or ASEBA broadly assess atypicality and could reasonably replace the M-CHAT-R/F and ASRS. However, if those broader tools are not used or if a more accessible, low-cost assessment for ASD is needed, the M-CHAT-R/F and ASRS remain valuable resources.
ADHD/Attention
Further, attention disorders are of particular concern for patients with craniosynostosis, so screening for ADHD is recommended, using the NICHQ Vanderbilt Assessment Scale (VAS), at the first visit that occurs between ages 6 and 12 years.50,51 Repeat assessment is not necessary unless new concerns from the child's pediatricians, educators, or caregivers arise.
Similar to the considerations surrounding ASD testing, the BASC and ASEBA include measures for assessing hyperactivity and inattention, offering a broader alternative to the NICHQ Vanderbilt Assessment Scale. However, for those not using these comprehensive tools or seeking a more accessible, low-cost option that is also more specifically designed for assessing ADHD, the NICHQ Vanderbilt remains a useful resource.
Limitations and Future Directions
Our study is not without limitations. The most impactful limitations may be the potential disconnect between the diagnostic tests and methodologies cited in the literature and those commonly employed in real-world clinical settings. The wide range of tests identified in the present study may be due to their use in research contexts—where hyper-specific outcomes are being targeted or research funding is available—or simply because investigators utilized the available tests at their disposal. As a result, the tests referenced in this literature review may not fully capture the practical realities faced by clinicians in their day-to-day practice. Future directions can be aimed at better understanding the current landscape of neurocognitive and psychosocial testing for patients with craniosynostosis in clinical practice.
Conclusions
Current literature supports the impact of craniosynostosis on patients’ neurocognitive development, yet there is no standardized approach to assessing developmental outcomes in these patients. In the present study, the authors provide recommendations for screening questionnaires that are: 1. free or low-cost; 2. can be efficiently and easily administered in clinic; and 3. do not necessitate the presence of a trained examiner. We hope these recommendations contribute to a standardized framework for comprehensive care that optimizes treatment outcomes for this patient population.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251335475 - Supplemental material for Routine Screening for Neurocognitive Impairment in Patients with Craniosynostosis: Towards a Standardized Approach
Supplemental material, sj-docx-1-cpc-10.1177_10556656251335475 for Routine Screening for Neurocognitive Impairment in Patients with Craniosynostosis: Towards a Standardized Approach by Payton K Grande, Christen M Holder, Billy D Holcombe, Devra B Becker and Robin J Evans in The Cleft Palate Craniofacial Journal
Footnotes
Data Availability
Data files are available as Tables, Supplementary Digital Content 1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.