
Abstract
Objective
As a follow-up study, we solicited opinions a decade later from fellowship-trained craniofacial surgeons to explore shifting perspectives on their training and assess the impacts on careers and practice patterns.
Design
An anonymous 26-question survey was sent to all surgeons completing craniofacial fellowships in 2013. Additionally, current craniofacial fellowship descriptions were tabulated to assess variations in program experiences.
Results
With a 47% response rate out of 30 original respondents, 14% reported no longer practicing craniofacial surgery. Among those still engaged, 42% described no longer performing intracranial/midfacial osteotomies, with 21% desiring more intracranial/midfacial volumes, 29% more cleft/orthognathic, and 30% less pediatric plastic surgery. Surprisingly, 31% reported in retrospect they would have chosen a different training program. Fifty percent had changed jobs since fellowship, with 50% practicing at centers with an average of 4.5 craniofacial surgeons. A review of current craniofacial fellowship descriptions revealed aside from intracranial/midface and cleft training, an additional 29 different surgical procedure types were advertised.
Conclusions
This follow-up assessment suggests most trainees remain active in craniofacial surgery, but many expressed dissatisfaction with their training. Almost one-third indicated they would have selected a different program, raising questions about the perceived quality of training. Considering the diversity of procedures currently falling under the craniofacial marque, a clearer description of expected case volumes might improve reported levels of fulfillment. An additional consideration is restricting the term craniofacial to programs focused on intracranial/midfacial surgery, while developing more descriptive alternative labels that better reflect the unique surgical experiences provided at each center.
Introduction
How does one measure the quality of craniofacial fellowship training and the subsequent impact on a surgeon's career? From a fellow's perspective, an ideal experience involves exposure to techniques and conditions that culminate in technical ability, confidence, and sound judgment when faced with future complex problems. From the perspective of a training program, quality is often aligned with postgraduate success metered by scholarly contribution, national leadership positions, academic notoriety, and of course, safe and effective patient care.1–3 In either case, the fundamental purpose of surgical training is simply preparation for future independent practice. An optimal assessment of fellowship training ideally benefits from the input from fellowship graduates, especially after having been in independent practice.
In 2013, we queried fellows as they finished their training with the purpose of evaluating the status of craniofacial training and to explore how this educational experience might have changed since this specialty first arose. 4 In that study, considerable heterogeneity was identified with respect to the clinical experience provided by different centers, as well as a shift in training from a mentorship experience toward more of a residency-type educational model. This current study sought to solicit opinions from this same group of surgeons after having been in practice for 10 years, to examine how their perspectives on their own fellowship training might have evolved, determine how this experience impacted their careers, and to gain insights that could add to the conversation as to how to best enrich craniofacial training.
Methods
An internet search was undertaken to identify the current locations for all the surgeons who had completed their craniofacial fellowship training in 2013. An anonymous online survey was then sent (Google Forms, Mountain View, CA) via email, followed by 2 follow-up emails to nonresponders from May through June 2024 (Appendix 1). No financial compensation or incentives were provided for participation. The survey included 26 questions, seeking information concerning: practice location, practice type, case mix, levels of career satisfaction, craniofacial research interests, reassessments of their fellowship training, and suggestions for training improvements.
In addition, we examined craniofacial fellowship descriptions for all programs participating in the 2023 to 2024 SF (San Francisco) Match, to catalog the various types of surgical experiences offered. This study was approved by the Medical City Institutional Review Board.
Results
Of the 30 respondents to our initial fellowship survey, 14 (47%) completed the follow up questionnaire. Eleven (79%) were practicing in the United States and 3 (21%) internationally (Canada, Lebanon, and Sweden). Two of the 14 respondents indicated that they were no longer performing craniofacial procedures. Most respondents from this class (86%) were practicing at academic centers or had an association with one, and over half (57%) reported being engaged in some form of craniofacial research. Over 70% reported being either satisfied, or strongly satisfied, with their current practice. Of those still identifying as craniofacial surgeons, 42% reported no longer performing intracranial/orbital/midfacial osteotomies and 14% of all respondents reported no longer being involved in cleft care. Twenty-one percent indicated they would like to perform more intracranial, orbital, and midfacial operations and 29% wanted to have more cleft/orthognathic volume (Figure 1). The majority (86%) reported that trauma reconstruction comprised only a minor aspect (< 25%) of their practice. When queried about what aspects of their current practice they would like to see reduced, 29% wanted to see less pediatric plastic surgery (Figure 2).
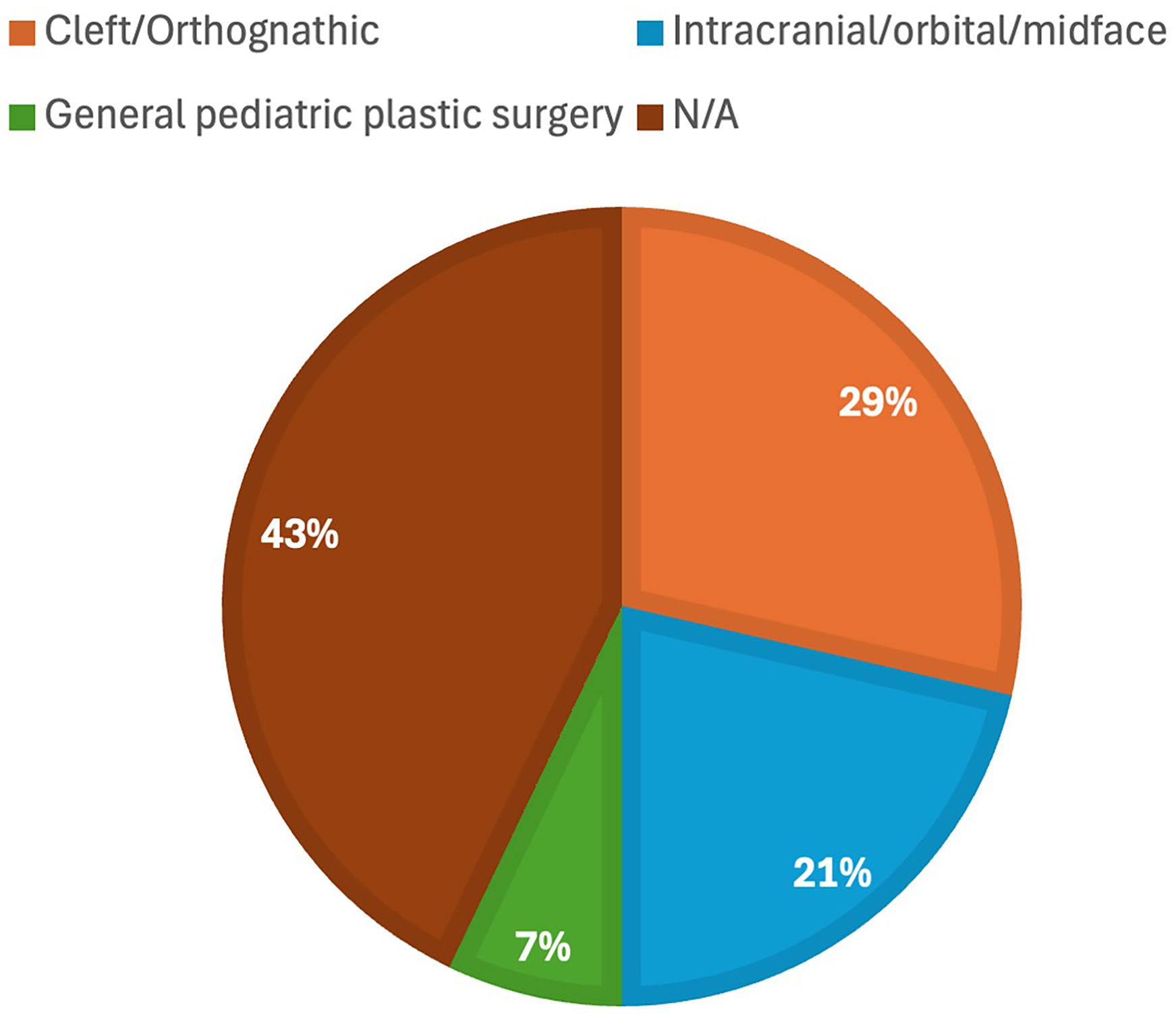
Types of procedures surgeons would like to see increased in their practices; 21% indicated they would like to perform more intracranial, orbital, and midfacial operations and 29% wanted to have more cleft/orthognathic volume.
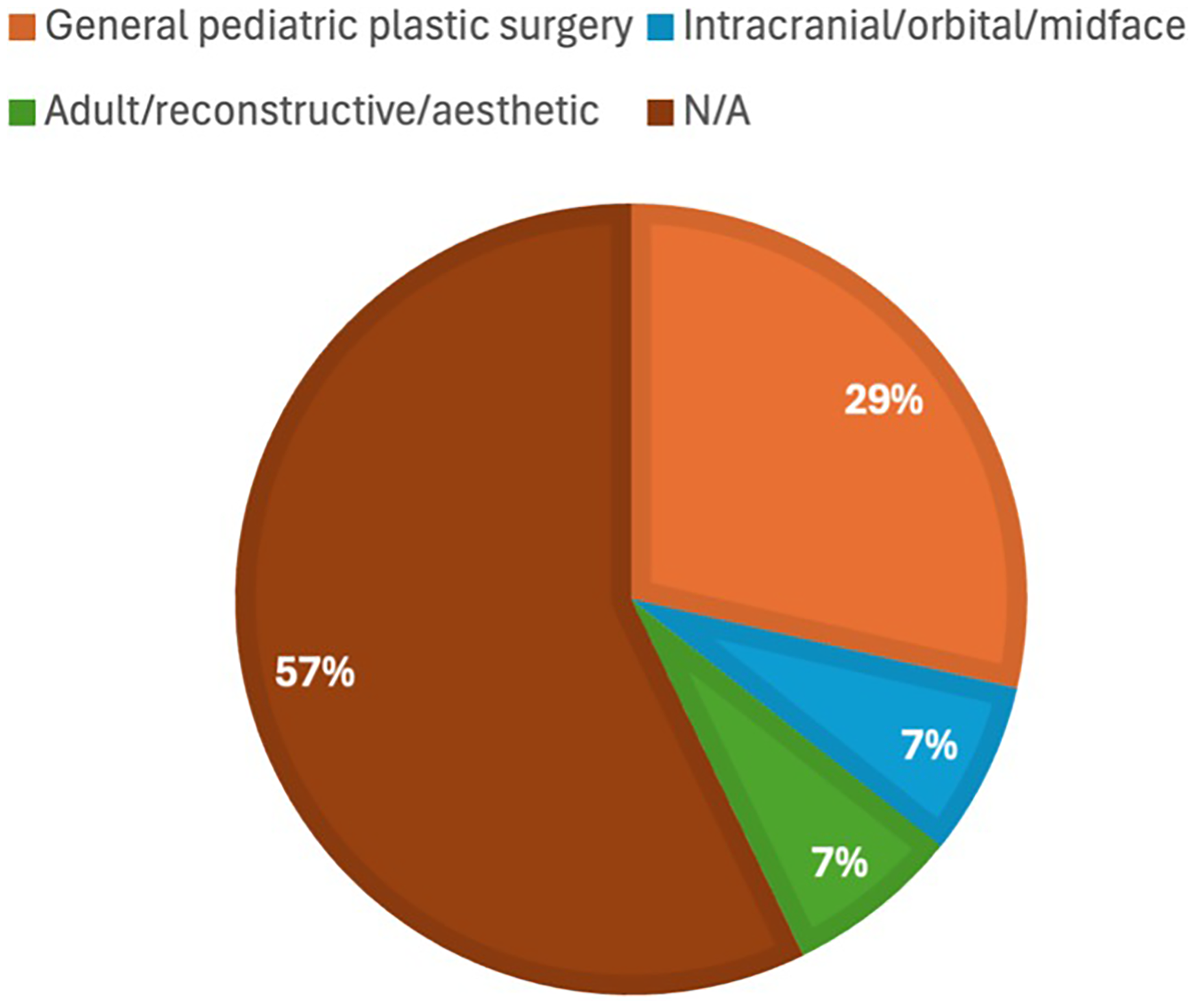
Types of procedures surgeons would like to see decreased in their practices; 29% wanted to see less pediatric plastic surgery.
With respect to current perceptions of their former craniofacial training, 86% indicated being satisfied overall. However, when asked about their decision to pursue craniofacial surgery training, 4 (29%) indicated that in retrospect they would not have pursued craniofacial training, with 2 indicating that they would have instead chosen esthetic surgery. Although the specific rationale behind these responses, including an examination of the exact reasons for any dissatisfaction, was not further explored, some information may be gleaned from the free-text responses. This included complaints related to burdensome administrative work, the amount of required case presentations, and the impact of multiple learners (residents and other fellows) while assisting in the operating room.
Among those still content with their decision to become a craniofacial surgeon, 31% offered in retrospect they would have chosen a different program. Less than half (43%) felt that their training provided them with a preferential edge on referrals. With respect to current employment, 50% of the respondents did not secure their current positions directly out of their fellowship, with this half having changed jobs since fellowship training, with just one going from academic to private practice. Twenty-one percent of respondents pursued an additional fellowship (hand and/or microsurgery) following their craniofacial training—whether this represents a reflection of genuine interest, the desire for enhanced marketability, or other reasons was not specifically assessed and requires further study. When asked about suggestions for improving fellowship training, responses included: standardized instruction, elective rotations and global health experiences, increased mentoring, and simulation training for lesser encountered procedures.
Half of those still practicing craniofacial surgery were either the only craniofacial surgeon, or were 1 of 2 at their center, whereas of the other half were working at institutions that had a mean of 4.5 total craniofacially trained plastic surgeons on staff. Just under half (42%) described a clear division of case types at their institution.
A review of posted craniofacial fellowship descriptions for the 2023 to 2024 Match cycle reveals considerable variability with respect to the offered training experiences. Aside from the core procedures involving intracranial, orbital, midfacial osteotomies, and cleft care, 29 different surgical procedure types were advertised (Table 1).
Types of Noncore Experiences Offered by Craniofacial Fellowship Programs Participating in the 2023 to 2024 Match Cycle.
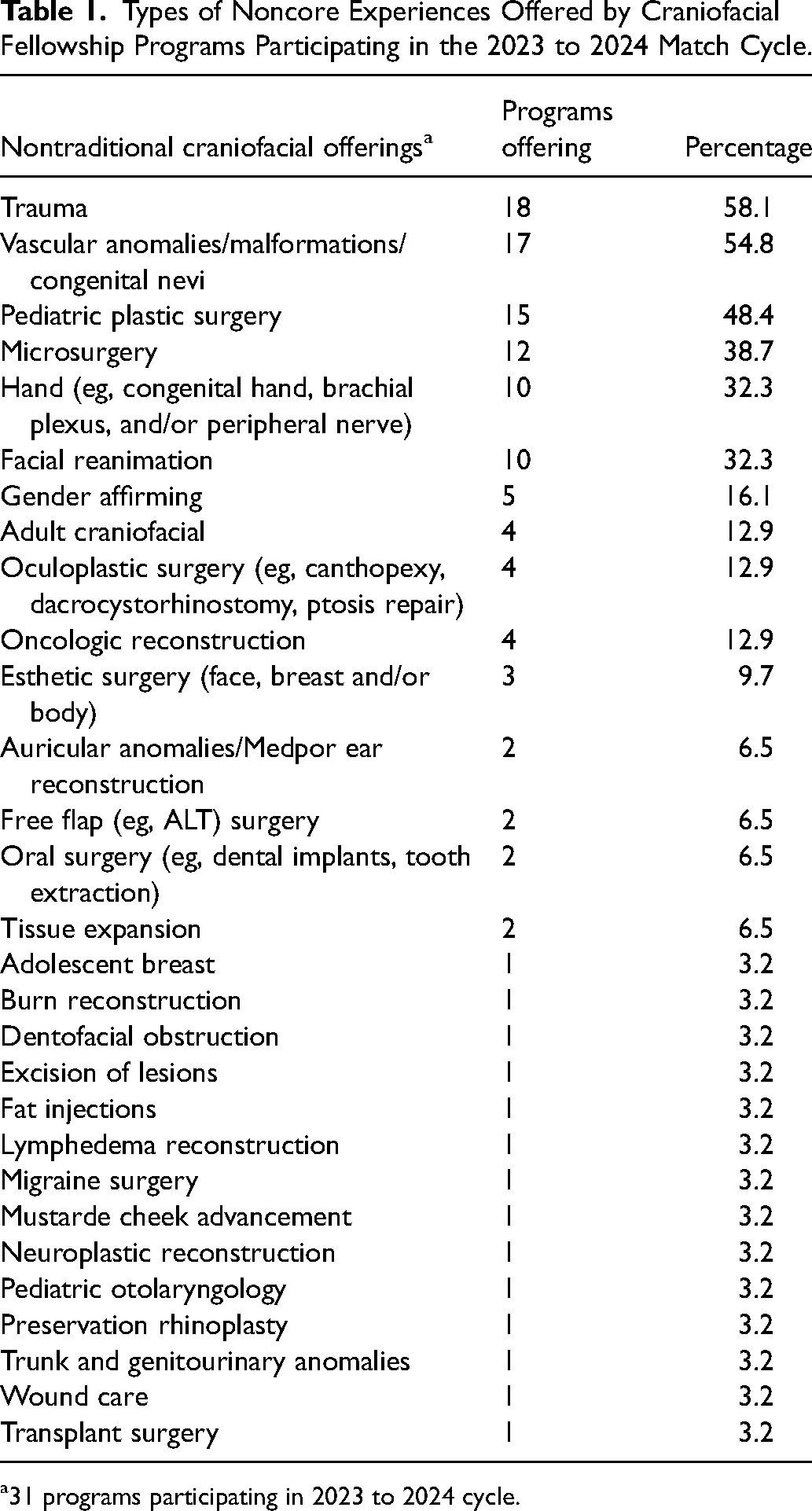
31 programs participating in 2023 to 2024 cycle.
Discussion
The journey to become a board-certified plastic surgeon is a lengthy one, with the decision to pursue additional fellowship training further delaying the start of one's career by an additional year. Our original survey of newly trained craniofacial surgeons, published in 2015, highlighted the variability of the craniofacial training experience across different programs, as well as the gradual metamorphosis away from a mentorship-type educational experience to more of a residency-type model. 4 This second inquiry sought to provide updated insights, by examining the changing perspectives offered by this same group of surgeons. One of the first things we looked to ascertain was the percentage of craniofacially trained surgeons still utilizing the skills acquired in their fellowship. Among the respondents, 86% still identified as practicing craniofacial surgeons; yet of these, 42% reported no longer performing intracranial/orbital/midfacial osteotomies, a finding that appears to corroborate prior surveys.5,6 Although speculative, perhaps individuals no longer practicing craniofacial surgery would be less inclined to answer a survey concerning craniofacial training; thus, our survey response rate might suggest that a larger proportion of surgeons are no longer utilizing the skills acquired during their year-long craniofacial fellowship than previously thought.
How have surgeons’ perceptions of their fellowship training changed? It seems that with the evolving perspectives that come from having been in practice for 10 years, for most this experience remains a favorable one, although the degree of dissatisfaction with fellowship training increased for many. Although only one respondent reported being completely unsatisfied with their craniofacial training program, nearly one-third reported that given the opportunity, they would have chosen a different fellowship. Does this level of dissatisfaction speak to a possible mismatch in training expectations? It is challenging for applicants to get a clear picture of the types of surgical procedures they might be exposed to during a year-long fellowship, with much of this depiction being based on more nebulous sources such as a program's reputation, or input from faculty members at the applicant's residency program. Fellows emerging from training report some degree of confidence in performing a new procedure after having experienced approximately 12 cases. 4 How many centers offer exposure to 12 individual metopic, unicoronal, or sagittal synostosis cases? Less likely would it be to experience 12 syndromic synostosis cranioplasties, or 12 midfacial advancements. Completing a 1-year fellowship without gaining the desired experience with the types of procedures of particular interest to any trainee is bound to engender some regret. Another possible source of training dissatisfaction might arise from a misguided criteria in selecting a particular fellowship, such as the belief a specific training program will improve subsequent job opportunities beyond their personal credentials. This survey found half of the respondents’ current practices were different from where they first started out, raising questions about the true impact of a training program on future employment. Might this represent success at an initial position that leads to a more desirable job elsewhere, or do specific training programs have a lesser impact on posttraining job placement? This survey also found that most respondents were still in an academic practice, in contradistinction to an earlier report that found only a minority of craniofacial fellowship graduates opted for academic practices. 5 Lastly, dissatisfaction with fellowship training could reflect suboptimal mentorship. Any program comprised of multiple craniofacial surgeons necessarily equates to a reduction in any one individual faculty's shared caseload, which in turn impacts experience levels that hamper teaching ability. 7 One possible counterpoint to this observation is the notion that training with multiple faculty members introduces different approaches and techniques which may resonate positively with the trainee.
The field of craniofacial surgery was conceived following descriptions of novel intracranial hypertelorism corrections and midfacial advancements for treating syndromic craniosynostosis. 8 Early on, Tessier warned of the need for specialized training before performing any type of orbitocranial surgery. 9 A review of all current craniofacial fellowship descriptions, as listed by the SF Match, provides insights into the degree at which the term craniofacial surgery has morphed beyond the traditional definition. Beginning with a focus on cranial/orbital/midfacial osteotomies and the care of congenital anomalies affecting the face and skull, this term has been further adapted, currently embracing a far broader diversity of conditions and procedure types.
The 2013 fellowship survey, which included a review of submitted cases logs, determined that only about a third of all the advertised craniofacial fellowships offered any significant exposure to intracranial and midfacial osteotomies. A subsequent editorial appearing in the inaugural issue of the journal FACE highlighted a long-held consensus opinion that the supply of future craniofacial surgeons has outpaced demands, citing the differential between total reported case volumes and the numbers of craniofacial fellowship training programs. 10 However, instead of arguing for fewer fellowships, in support of the opposite view is that expanded training opportunities deliver a more inclusive approach, which increases the opportunity and potential for future stars to shine. Today's fellowship offerings highlight a significant diversity in offered educational experiences, with descriptions going beyond adult and pediatric trauma reconstruction to include general pediatric plastic surgery, gender-affirming surgery and facial feminization, microsurgical reconstruction, facial reanimation, tissue expansion, and esthetic surgery, among others. These descriptions suggest that many programs offer more of a focused recapitulation of certain areas of general plastic surgery training. Some have even speculated that the increasing diversity in case types offered by craniofacial fellowship programs is purposely designed to mitigate future employment concerns. 11
The reported levels of dissatisfaction with fellowship training make the designation of exactly what constitutes craniofacial surgery seemingly more relevant. Is fellowship regret a function of the fellowship experience, factors related to practice development after training, or a mixture of both? Future directions include a follow-up survey to better distill reasons for dissatisfaction, whether job changes were promotional or due to other factors, and reasons for no longer performing or offering certain procedure types. An additional consideration is exploring how our data compares to subspecialties in other fields, including neurosurgery, otolaryngology, and oral and maxillofacial surgery.
To help applicants ensure they are applying to those programs that best match their interests, it is critically important to ensure the type of expected surgical experiences a fellow is likely to encounter is clearly described. 12 Some suggestions to enhance a prospective fellow's understanding of the available programs include publishing and consistently updating the proportion of cases performed each year, providing a roster of prior fellows and their current contact information on the program's website, as well as the first position secured by each graduate. Recent initiatives by the American Society of Craniofacial Surgeons and International Society of Craniofacial Surgery—including categorization of cases and enhanced fellowship directories—provide an important step in this direction.
Most applicants choose to pursue craniofacial fellowship training after discovering a passion for this field following exposure to some type of fascinating case in residency training. To maximize the fellowship training experience, the offered surgical caseloads should ideally match the areas of desired knowledge acquisition. We submit that it would serve future trainee's better were our specialty to narrow the designation of the term craniofacial surgery, while developing more descriptive alternative labels that better reflect the surgical experiences offered, such as: trauma, cleft care, microsurgical reconstruction of facial neoplasm resections, microtia, facial feminization, etc.
Conclusion
In conclusion, this follow-up assessment of craniofacially trained surgeons revealed that after a decade of practice, more than half still identify as being a craniofacial surgeon. However, many expressed dissatisfactions with their training experience, with almost a third questioning whether they might have received better training at a different program. Concomitant with a shift in the educational experience from a focused mentorship to more of a residency-type model, has come a significant broadening of the types of surgical procedures offered in fellowship training. Considering the diversity of procedures now falling under the craniofacial marque, likely the result of reduced core case numbers, a clearer description of expected case volumes might improve reported levels of satisfaction. A supplementary consideration is narrowing the term craniofacial to those programs focused more on intracranial/midfacial surgery, while developing more descriptive alternative labels that better reflect the unique surgical experiences provided at each center.
Supplemental Material
sj-pdf-1-cpc-10.1177_10556656251340787 - Supplemental material for Craniofacial Fellowship Training: How Are We Doing?
Supplemental material, sj-pdf-1-cpc-10.1177_10556656251340787 for Craniofacial Fellowship Training: How Are We Doing? by Demetrius M. Coombs, Niyant Patel, Kanlaya Ditthakasem and Jeffrey A. Fearon in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.