
Abstract
Objective
Augmented reality (AR) has recently emerged as a potential alternative to 3D-printed technology in craniomaxillofacial surgery. The purpose of this study was to evaluate the feasibility and accuracy of AR craniotomy guides for fronto-orbital advancement (FOA) compared to conventional 3D-printed guides.
Design
Retrospective comparative study.
Setting
Cleft and craniofacial center at a tertiary children's hospital.
Patients
3D-printed skull models from 9 patients with metopic or coronal craniosynostosis who underwent FOA between January 2022 and November 2023.
Interventions
A novel application was developed to project AR craniotomy guides onto 3D-printed skull models. AR guides were compared to conventional 3D-printed guides by utilizing both guidance modalities. The discrepancy at 8 pre-determined reference points was measured, including bilateral nasofrontal (NF), zygomaticofrontal (ZF), barrel stave (BS), and tenon extension (TE).
Main Outcomes Measure
Measured discrepancy in millimeters between AR guides and 3D-printed guides at the pre-determined reference points.
Results
The anterior reference points (NF, ZF) had mean discrepancies ranging from 0.31 to 0.61 mm. The posterior points had mean discrepancies ranging from 1.39 to 3.28 mm (BS, TE). There was no statistically significant difference found between the two modalities at any reference point.
Conclusions
AR craniotomy guides had a high level of accuracy, particularly at the anterior reference points. AR guides demonstrated feasibility as an alternative to 3D-printed craniotomy guides, in-vitro. Further research is required to translate this novel application to cadaver models and improve precision at posterior landmarks.
Keywords
Background
Craniosynostosis is the premature fusion of one or more sutures resulting in abnormal head growth, which may result in cosmetic concerns, elevation in intracranial pressure, visual abnormalities, and developmental delay. 1 In patients with metopic or coronal craniosynostosis, fronto-orbital advancement (FOA) is often performed to expand the anterior cranial vault and correct the position of the frontal and orbital bones. In 1967, Tessier first introduced the FOA to formally reconstruct the forehead; since then, many iterations of the procedure have been described. 2 More recently, the advent of computer-aided design and computer-aided manufacturing (CAD/CAM) has allowed surgeons the opportunity to virtually plan FOA procedures and utilize 3-D printed craniotomy guides and intraoperative templates to improve surgical precision.3,4
Augmented reality (AR) has recently emerged as a promising alternative to CAD/CAM technology in craniomaxillofacial surgery. AR is the projection of a virtual environment onto the physical world, enabling users to interact with both digital and real-world elements simultaneously. AR has been used in many surgical subspecialties for both clinical and educational purposes.5–7 In craniofacial surgery, AR has been utilized intra-operatively for visualization of cranial defects, visualization of planned osteotomies, management of fibrous dysplasia, and reduction of zygomaticomaxillary complex (ZMC) fractures.8–15 There is a paucity of data evaluating the use of AR for cranial vault reconstruction.
The purpose of this feasibility study was to develop and evaluate an AR application for craniotomy guides in FOA procedures. We compared novel AR craniotomy guides to conventional 3D-printed guides using 3D-printed anatomic models of patients who had previously undergone FOA for craniosynostosis. The primary outcome measure was the discrepancy between the two guidance modalities at predefined anatomic landmarks. We hypothesized that there would be no significant difference between landmarks derived from the AR and 3D-printed craniotomy guides.
Methods
Institutional review board approval was obtained for this retrospective study. Inclusion criteria were patients less than 10 years old with a diagnosis of metopic or coronal craniosynostosis who had previously undergone FOA between January 1, 2022 and November 10, 2023 at our institution. All subjects had pre-operative craniofacial computed tomography (CT), and their respective Digital Imaging and Communications in Medicine (DICOM) files were obtained from the electronic medical record.
All subjects had previously undergone FOA utilizing 3D-printed craniotomy guides from a third-party vendor (KLS Martin Group; Tuttlingen, Germany). Stereolithography (STL) files were obtained from the third-party vendor for all subjects’ craniotomy guides. STL files were uploaded to Formlabs software (Formlabs, Inc.; Somerville, MA) for printing. Utilizing the Form 3B (Formlabs, Inc.; Somerville, MA), each patient-specific craniotomy guide was printed at 100% scale and 0.1 mm thickness with amber surgical guide resin. DICOM files for subjects’ pre-operative Craniofacial CT were segmented in Materialise Mimics (Materialise; Leuven, Belgium) to generate the STL files of the subjects’ skulls. These were uploaded to Ultimaker Cura 5.10 Software (Utrecht, The Netherlands) and skull models were 3D-printed to 100% scale in polylactic acid utilizing the Ultimaker S5 (UltiMaker Cura; Utrecht, The Netherlands) with 0.03-millimeter layer thickness.
The STL file of each skull model was uploaded to Vuforia Engine Model Target Generator (MTG) (Vuforia; Boston, MA) to generate target outlines. This would allow Vuforia engine to track the outline of the 3D printed skull model and align the uploaded STL file target skull model to the 3D-printed model. The target outlines were exported to Unity (Unity Software, Inc.; San Francisco, CA) as a “unity package file” (.unitypackage). Within the Unity application, the skull model was set as the model target. The STL file of the craniotomy marking guide was uploaded and linked as a “child object” of the model target. Because objects in STL files preserve their orientation within the XYZ coordinate system, the skull model and the craniotomy marking guide automatically align to their respective position. Within the Unity application, when the 3D-printed skull model was viewed through a USB-connected digital camera, the virtual craniotomy guide overlaid onto the 3D-printed skull model in AR. The same process was repeated by exporting images to a tablet PC (iPad; Apple, Inc.; Cupertino, CA) and visualizing through the Unity Hub application (Unity Software, Inc.; San Francisco, CA).
The craniotomy guide was projected via AR onto the 3D-printed skull model for each subject (Figure 1). With a blue marker, the skull model was marked at 8 predetermined points based on the AR-projected guide—right and left zygomaticofrontal (ZF), nasofrontal (NF), tenon extension (TE), and barrel stave (BS) points (Figure 2). The AR-projected craniotomy guide was removed, and the 3D-printed craniotomy guide was subsequently affixed to the skull model (Figure 3). With a red marker, the same 8 points were marked. For demonstration, one skull model was fully marked utilizing AR in blue marker, and again with the 3D-printed guide in red marker; these markings are shown in Figure 4.
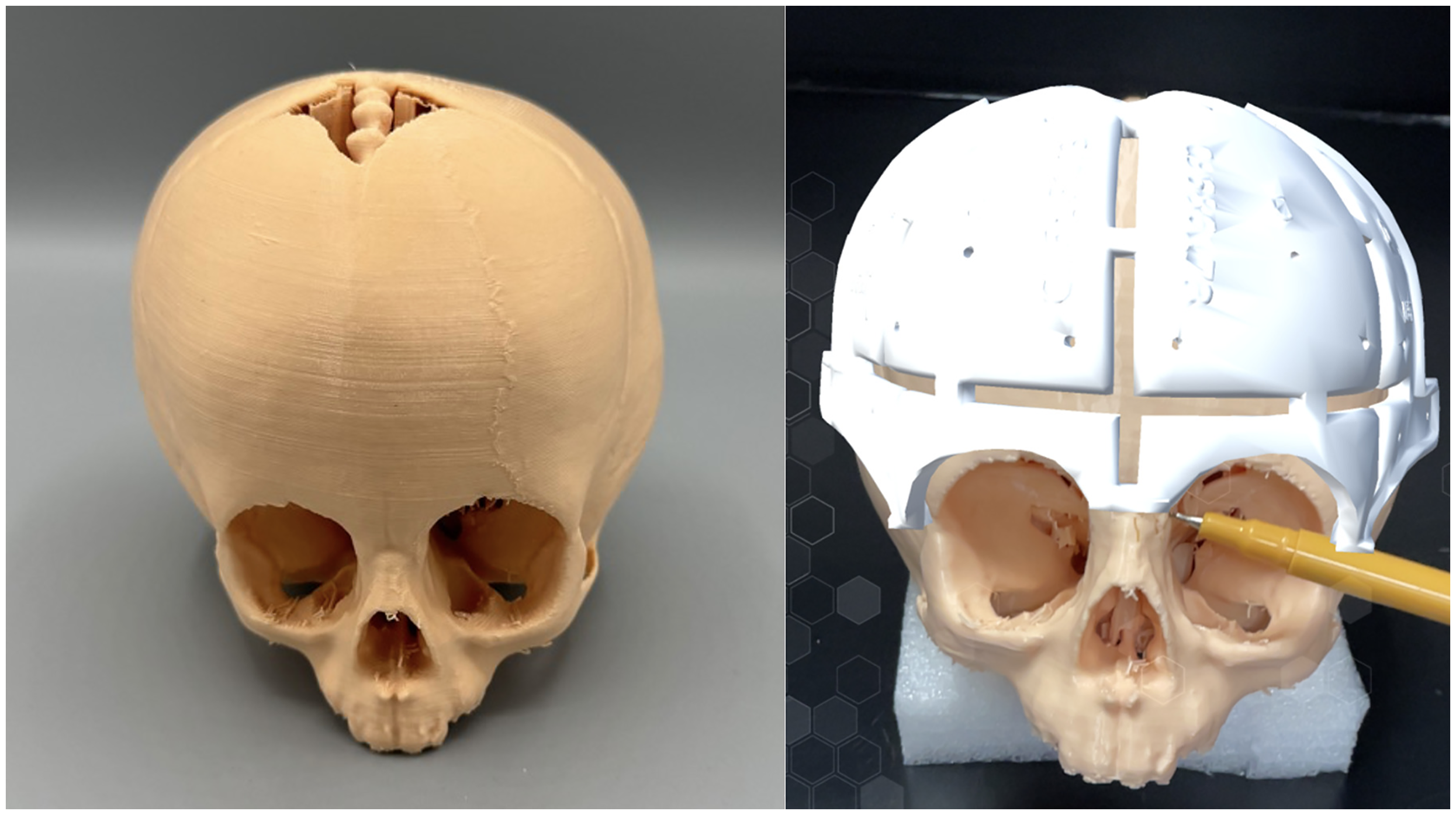
Skull Model (Left) and Skull Model with Augmented Reality-Projected Craniotomy Guide (Right) being Marked at the Left Nasofrontal Reference Point.
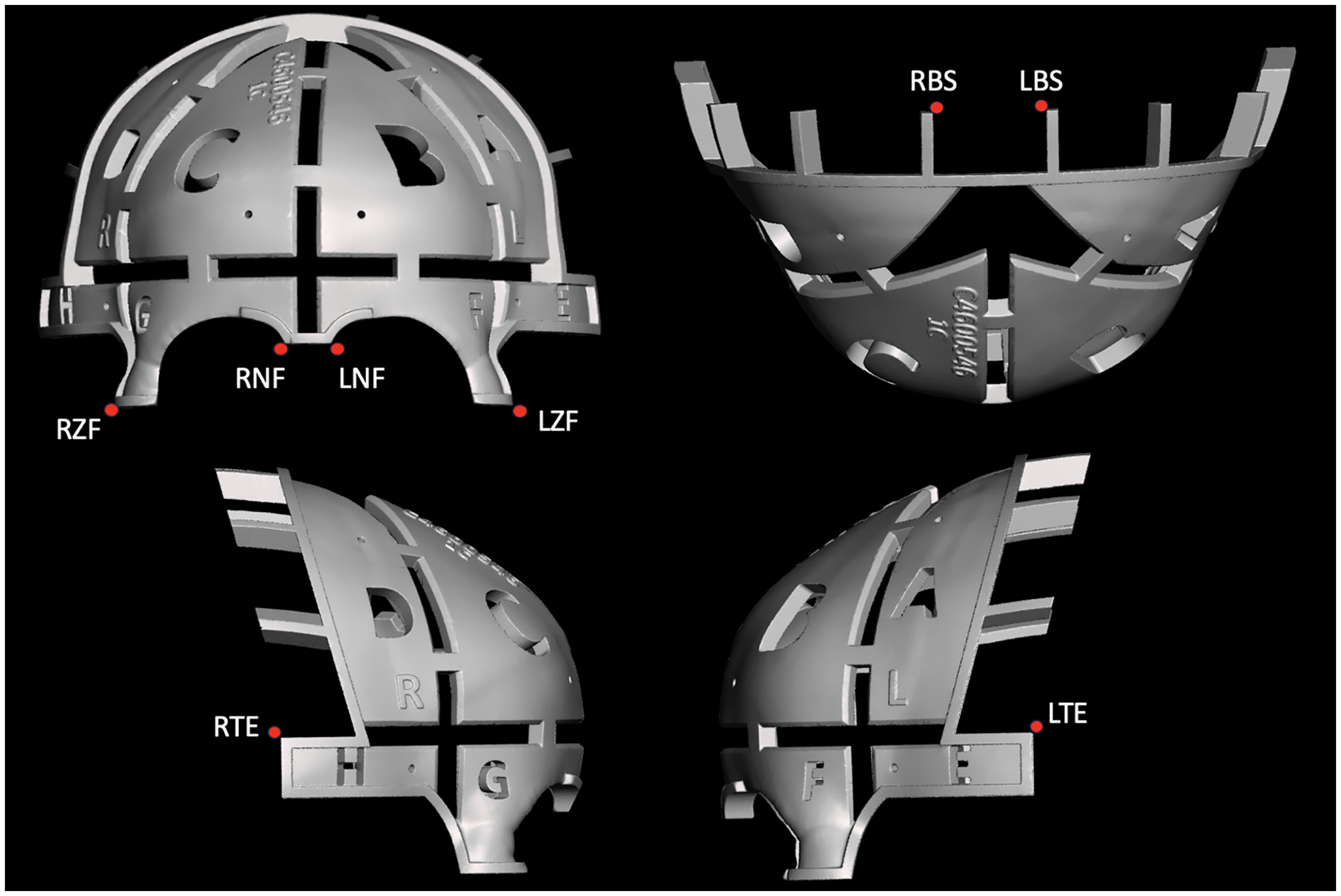
Eight Pre-Determined Anatomic Reference Points.
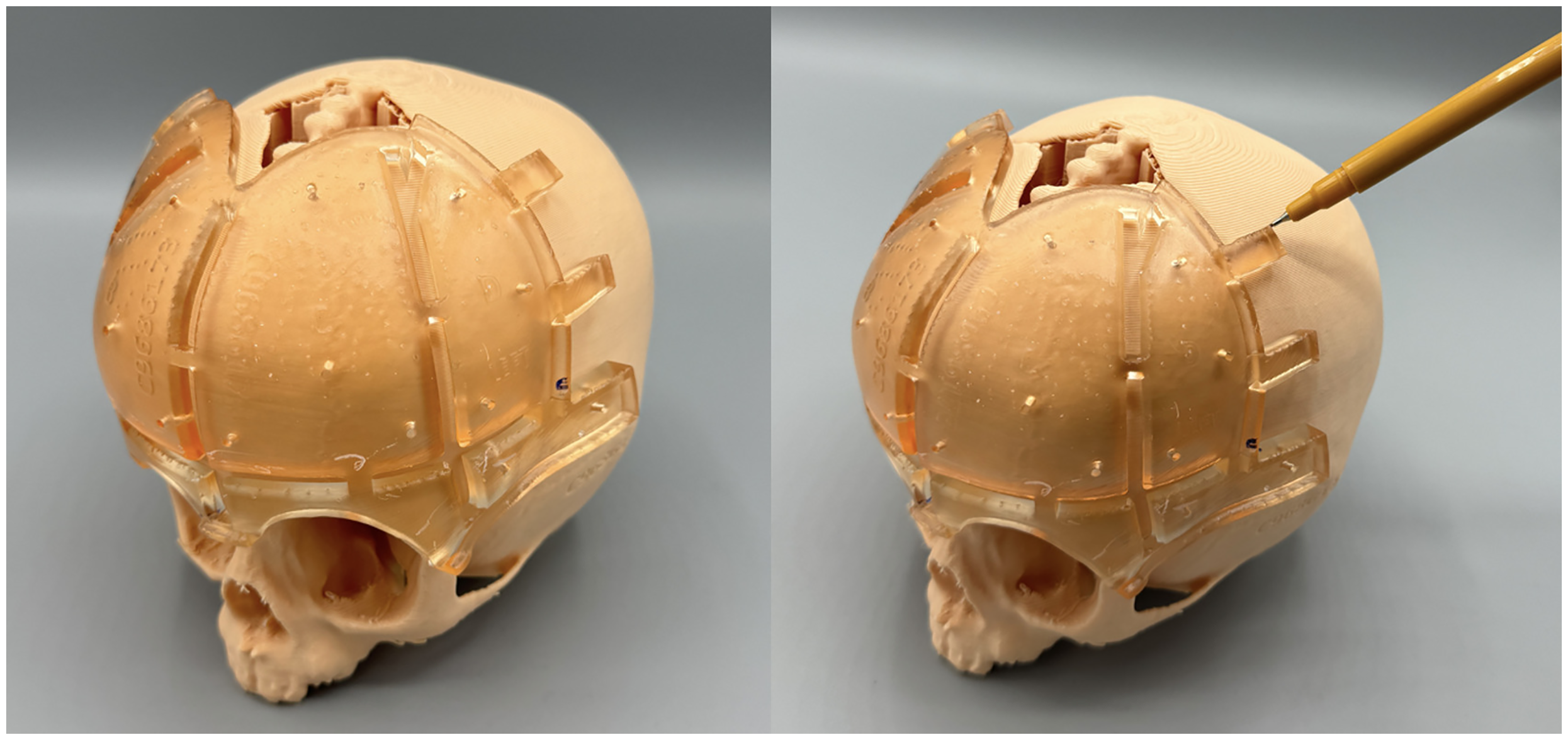
Skull Model with 3D-Printed Craniotomy Guide Affixed (Left). Marking the Left Barrel Stave Reference Point (Right).
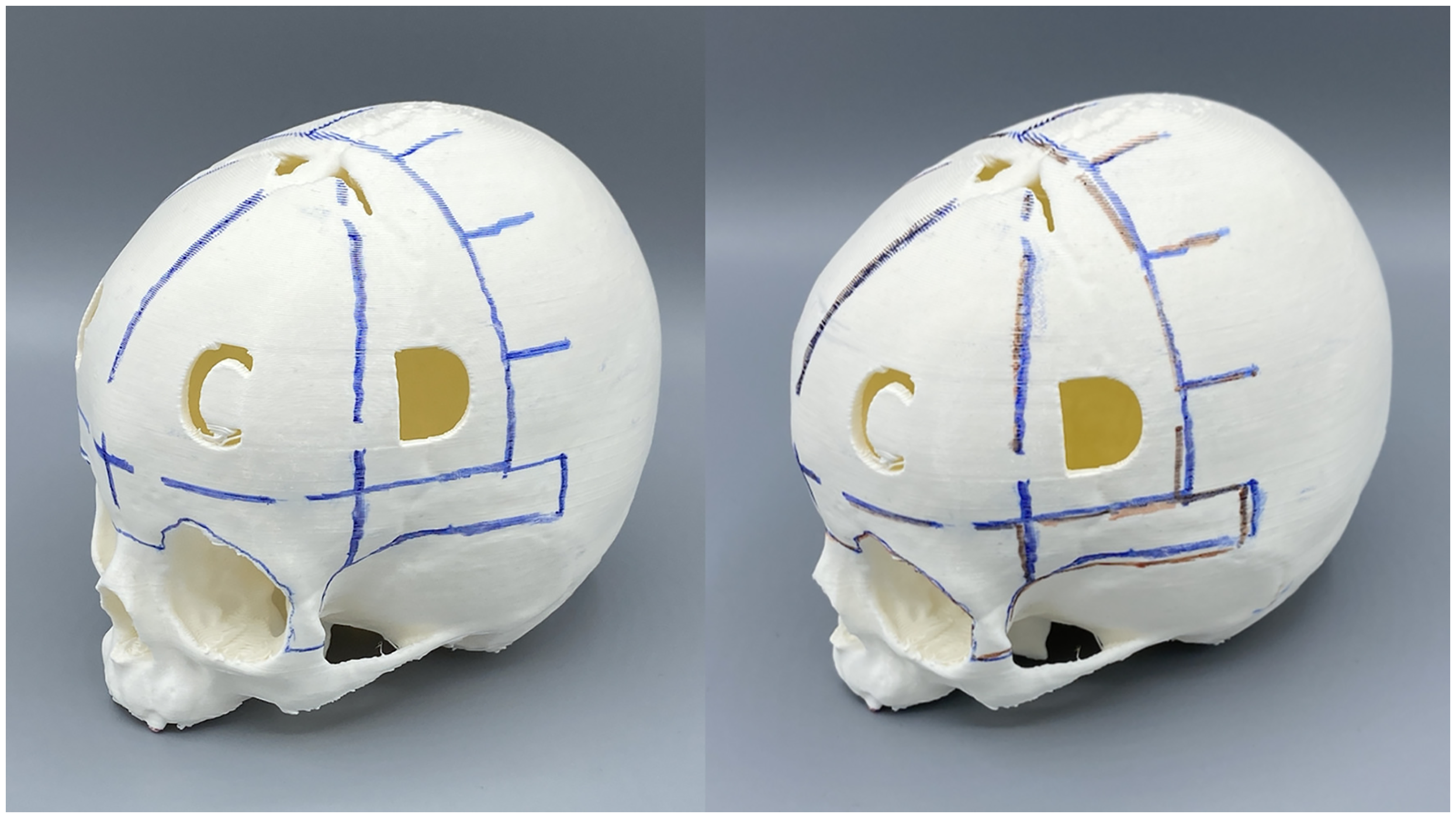
Skull Model Marked to Completion with Augmented Reality Guide in Blue Marker (Left). The Skull Model was Subsequently Marked in Red with the 3D-Printed Craniotomy Guide (Right).
Discrepancy between the red and blue points was then measured with a caliper to the nearest 0.25 mm by the first author (DLB). The entire procedure was repeated by a second author (VY). The primary outcome variable was the mean distance between blue marking (AR guide) and red marking (3D guide) at each of the 8 reference points. Inter-rater reliability was performed to determine the variance between investigators. Descriptive statistics were performed. Because the data consisted of paired and non-normally distributed with a small sample size (n = 9), the Wilcoxon signed-rank test was used to evaluate whether the median discrepancy at each anatomical point differed significantly. To correct for multiple comparisons, the Bonferroni correction was applied, adjusting the significance level to alpha = 0.00625.
Results
Nine subjects met inclusion criteria. All subjects had a 3D-printed skull model, 3D-printed craniotomy guide, and AR craniotomy guide fabricated per the aforementioned protocol. All 8 reference points (bilateral ZF, NF, TE, and BS) were marked in all subjects. The mean discrepancy at each point was as follows—right ZF: 0.61 mm (SD: 0.55), left ZF: 0.47 mm (SD: 0.54 mm), right NF: 0.47 mm (SD: 0.54), left NF: 0.47 mm (SD: 0.40); right TE: 1.39 mm (SD: 1.31); left TE: 2.44 mm (SD: 1.85); right BS: 2.97 mm (SD: 1.88); left BS: 3.28 mm (SD: 3.43). Measured discrepancies at each point are shown in Table 1. The smallest discrepancy between the AR craniotomy guide and 3D-printed craniotomy was observed at the left ZF point; whereas the greatest discrepancy was at the left BS point. No statistically significance difference was observed between the AR guide and the 3D-printed guide at any of the reference points (alpha = 0.00625 after Bonferroni correction). Two-rater inter-rater reliability was fair with an agreement of 70.8% and kappa of 0.246.
Discrepancy Between Augmented Reality Craniotomy Guide and 3D-Printed Craniotomy Guide at Each Anatomic Reference Point.
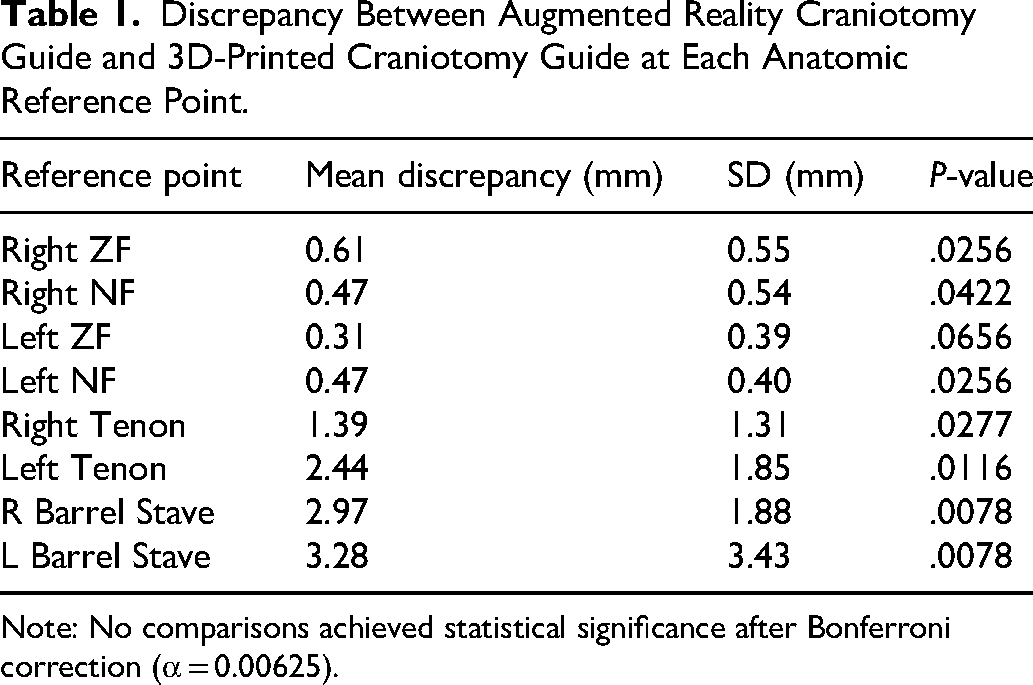
Note: No comparisons achieved statistical significance after Bonferroni correction (α = 0.00625).
Discussion
In recent years, the use of AR technology has become increasingly commonplace in personal and workplace environments; however, its use in medicine and surgery remains limited. This study developed a novel application for the use of AR in craniofacial surgery by creating an application for AR-projected craniotomy guides. The accuracy of the AR craniotomy guides was evaluated in comparison to the current gold-standard of CAD/CAM, 3D-printed craniotomy guides.
Our results demonstrated that the AR guides were accurate at the anterior reference points (bilateral ZF and NF), with mean discrepancies of 0.61 mm or less. However, there was decreased precision at the posterior reference points with discrepancies ranging from 1.39 to 3.28 mm. This finding is likely due to the paucity of distinct anatomic landmarks in the posterior cranium, as compared to the facial bones, which contain several well-defined anatomic landmarks (orbits, piriform rim, and zygomatic prominences). Despite the posterior variance, the overall accuracy demonstrated in this pilot study suggests that AR technology may be a potential alternative to 3D-printed craniotomy guides.
Dennler et al. utilized AR to visualize 3D models of patient-specific anatomy in the operating room setting. They used a commercially available holographic headset (HoloLens I; Microsoft; Redmond, WA), which was worn by the surgeons during the procedure. Of note, the authors did not overlay the anatomy onto the patient; rather, they visualized AR-projected anatomic models in their field of view in the operating room. There were some limitations to the HoloLens in their study—namely, technical issues and ergonomic shortcomings. 16
Sakamoto et al. similarly used the HoloLens 2 (Microsoft; Redmond, WA) to visualize dural venous sinuses for posterior cranial vault distraction. They manually aligned the hologram of the patient's CT to the patient's sagittal and lambdoid suture, intraoperatively. The authors did not evaluate the accuracy of the HoloLens in their study. They also reported difficulty with visualizing the hologram and difficulty with hologram movement. Despite their difficulties, they reported theoretical improvements in safety and improved surgeon confidence when utilizing AR. 14
Other studies report the use of fiducial markers to align the AR projected model onto the patient or 3D-printed model. Lin et al. reported a randomized control trial protocol for reduction of ZMC fractures with AR technology. They utilized Quick Response (QR) codes as fiducial markers. 13 Thabit et al. developed an AR electromagnetic navigation system and assessed its accuracy on phantom skulls, utilizing conical fiducial markers. The authors found a mean delineation error of 2.4 mm and concluded that the AR technology helped to accurately identify cranial sutures. 15 Recently, Kaiser et al. reported the use of intraoperative AR for craniofacial fibrous dysplasia debulking; they also used QR-tracking. 10 The primary issue with utilizing fiducial markers or QR-tracking is that the accuracy of the registration is largely dependent on the accuracy of the placement of the markers. In the present study, we utilized the patient's own anatomy for registration, and we did not use additional fiducial markers. For the anterior reference points, we found greater accuracy than reported by Thabit et al.; however, we found less accuracy for the posterior reference points where there are less unique anatomic landmarks. 15
The use of AR craniotomy guides presents several potential advantages over conventional 3D-printed guides. First, AR guides would eliminate the need for 3D-printed models, reducing costs from production and shipping. Additionally, physical models require sterilization, which further increases time and expense, as well as introduces potential risks. Secondly, by circumventing the manufacturing and shipping process, AR guides could significantly decrease lead time from surgical planning to the operation. In urgent or emergent cases, such as increased intracranial pressure, AR craniotomy guides could be ready immediately after surgical planning. In rare situations or unforeseen circumstances requiring change to original surgical plan, a digitally altered AR guide can potentially be deployed quickly at the point-of-care, in comparison to the lengthy turnover of a reprinted guide.
Despite the encouraging findings in this pilot, there were several study limitations. The first is inherent to current AR technology, which is the registration process—this describes the way that the virtual environment aligns with the physical environment. For AR to have improved accuracy, there must be improvement in the registration process, whether that's QR-tracking, fiducial markers, anatomic references, or other modalities. A second limitation was the currently available technology for visualizing the AR craniotomy guide onto the skull models. We utilized a USB-connected digital camera, which lacks feasibility in the operating room setting. We also trialed a tablet PC (iPad; Apple, Inc.; Cupertino, CA) and the HoloLens 2 (Microsoft; Redmond, WA). The HoloLens lacked consistency and field-of-view, the hologram was difficult to visualize, and its use was abandoned. The tablet PC was effective, and its accuracy will be evaluated in future studies. Supplemental 1 demonstrates a video, taken via tablet PC, of the skull model with AR craniotomy guide overlaid.
In conclusion, although AR applications in craniomaxillofacial surgery have made significant strides, the technology remains in its early stages of clinical implementation. Our findings demonstrate that AR has considerable potential to be an accurate alternative to traditional 3D-printed craniotomy guides for craniosynostosis management. The next phase of this research will involve translating our methods to cadaveric models and incorporating AR-specific headsets. Additionally, future investigations must focus on refining registration techniques to improve accuracy, particularly in the posterior cranium where less anatomic landmarks naturally exist.
Supplemental Material
Footnotes
Ethical Statement
University at Buffalo IRB approval was obtained for this study. The study was completed in an ethical manner in accordance with the Declaration of Helsinki and ICMJE recommendations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Meeting Presentations
This abstract was presented at the American Academy of Oral and Maxillofacial Surgery Annual Meeting 2024, Halifax, Nova Scotia, April 6, 2024.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.