
Abstract
Objective
To explore if observations on nasopharyngoscopy influence the surgical procedure selected for the management of velopharyngeal insufficiency (VPI).
Design
Cross-sectional survey.
Participants
Seventeen surgeons with experience treating VPI.
Interventions
Review of twenty-four nasopharyngoscopy videos with a combination of velopharyngeal closure patterns and gap sizes.
Main Outcome Measures
Surgical procedure was selected after watching a nasopharyngoscopy video. Chi-square tests were used to evaluate if, for each surgeon, procedure selection varied based on closure pattern and gap size combination. Variable importance scores were obtained from a random forest analysis to quantify contribution of nasopharyngoscopy observations on procedure selection.
Results
Four procedures accounted for 86% of all surgeries selected: Furlow double-opposing Z-Plasty (33%), palatal lengthening using buccal myomucosal flaps (20%), pharyngeal flap (19%), and sphincter pharyngoplasty (14%). Four surgeons (23.5%) significantly varied their surgical selection when different closure pattern and gap size combinations were shown on nasopharyngoscopy. Ten surgeons (58%) selected the same procedure in ≥ 50% of the 24 nasopharyngoscopy videos. Individual surgeon preference was the strongest predictor of surgical selection, accounting for 57.9% of surgical selection variance. Velopharyngeal gap size accounted for 36.5% of the variance in surgical selection, yet the specific surgeries selected based on gap size varied widely across surgeons. Closure pattern was a weak predictor, contributing 5.6% to surgical selection variance.
Conclusions
Nasopharyngoscopy findings influence VPI surgical procedure selection in a highly individualized, surgeon-specific manner. Among factors observed on nasopharyngoscopy, velopharyngeal gap size has a much larger influence on procedure selection than closure pattern.
Keywords
Introduction
Nasopharyngoscopy is the most commonly used imaging technique in the preoperative evaluation of velopharyngeal insufficiency (VPI). 1 Nasopharyngoscopy can be quickly completed in clinic, allowing for the surgical recommendation to be reviewed with the patient and their caregivers in the same appointment. 2 While the use of velopharyngeal imaging in VPI management is widely agreed upon by cleft providers to be necessary and a standard of care, 3 there is substantial variation in how cleft teams interpret nasopharyngoscopy findings to guide surgical selection.4–8
It is not clear which factors visualized during nasopharyngoscopy should influence surgical selection and there is substantial variation in the resulting clinical pathways. Abdel-Aziz et al. used closure pattern on nasopharyngoscopy to select a surgical procedure, selecting a pharyngeal flap to treat patients with a sagittal closure pattern and a sphincter pharyngoplasty to treat patients with circular or coronal closure patterns. 9 Sitzman et al. used gap size on nasopharyngoscopy to select a surgical procedure, selecting a secondary Furlow to treat patients with a small to medium gap, and palate lengthening with buccal myomucosal flaps to treat patients with a medium to large gap. 5 Nam reported using both gap size and closure pattern, selecting an overlapping intravelar veloplasty with oral Z-Plasty for small gaps and sagittal or circular closure pattern, a pharyngeal flap for large gaps with circular or coronal closure pattern, and a sphincter pharyngoplasty for small gaps with coronal closure pattern. 10 It is unclear if this variation among single-institution studies reflect broader variations among providers in the field.
Even as surgeons disagree about what factors to use from nasopharyngoscopy to inform surgical decision making, the influence of those factors on surgical selection appears to differ among surgeons. Some surgeons appear to use the same surgical procedure across all patients, regardless of the findings on nasopharyngoscopy. In a 2022 study, all patients (N = 87) presenting for VPI management completed nasopharyngoscopy as part of their standardized evaluation, then, regardless of nasopharyngoscopy findings, all patients who had a prior straight-line palate repair were treated with a Furlow double-opposing Z-Plasty. 11 Another institution reported similar findings: only 76% of nasopharyngoscopy exams were deemed ratable on blinded review, yet nearly all patients with non-syndromic cleft palate underwent a palate-based procedure to treat VPI. 2 These findings suggest that while nasopharyngoscopy is widely used in the evaluation of VPI, its impact on surgical selection may be limited, with some surgeons prioritizing preferred surgical approaches over findings on nasopharyngoscopy.
If nasopharyngoscopy is not being interpreted similarly across providers−or in some cases never changing their surgical selection−the indications for preoperative nasopharyngoscopy should be re-examined. The purpose of the current study was to explore how findings observed on nasopharyngoscopy influence surgical procedure selection while also considering the impact of surgeon preference. The null hypothesis was that surgeons do not alter their surgical selection based on different gap size and closure pattern combinations. The alternative hypothesis was that surgeons do alter their surgical selection based on nasopharyngoscopy feature combinations.
Method
This study was reviewed by Phoenix Children's IRB # IRB-24–068 and was qualified as exempt research under guideline 45 CFR 46.101(b) (3).
Study Design. This was a cross-sectional study of VPI surgeons in which a survey instrument was used to elicit specific surgical procedure recommendations for a series of hypothetical case studies.
Participants. This study focused on the surgical decision-making process based on nasopharyngoscopy among surgeons treating VPI. The survey was sent to all 35 surgeons in the United States and Canada participating in the Velopharyngeal Insufficiency Outcomes Prediction Study (VPI-OPS). 12
Survey Instrument and Procedures. Participants were emailed a link to an online survey via REDCap where they were asked to engage with a series of case studies. Twenty-four fictitious case studies were presented with varied clinical features. Each case study included information regarding patient age, gender, and perceptual speech ratings for hypernasality and audible nasal air emission followed by a nasopharyngoscopy video. All cases stated the patient was born with a cleft of the hard and soft palate, had no other medical problems, had undergone cleft palate repair in infancy using a Furlow double-opposing Z-Plasty technique, and was now presenting for VPI management. The only feature that differed substantially between the cases was the nasopharyngoscopy video. After reading the case study and watching the video, surgeons were asked to select their recommended surgery from a list. Nine surgical procedures were presented as options, including an ‘Other’ option. When surgeons selected ‘Other,’ they were asked to describe the surgery they would perform. Only one surgical option could be selected. Table 1 lists the surgical options listed for each video case study. The surgeons could watch the nasopharyngoscopy video as many times as needed prior to making a selection.
Surgical Options Provided on Survey and Frequency of Selection.
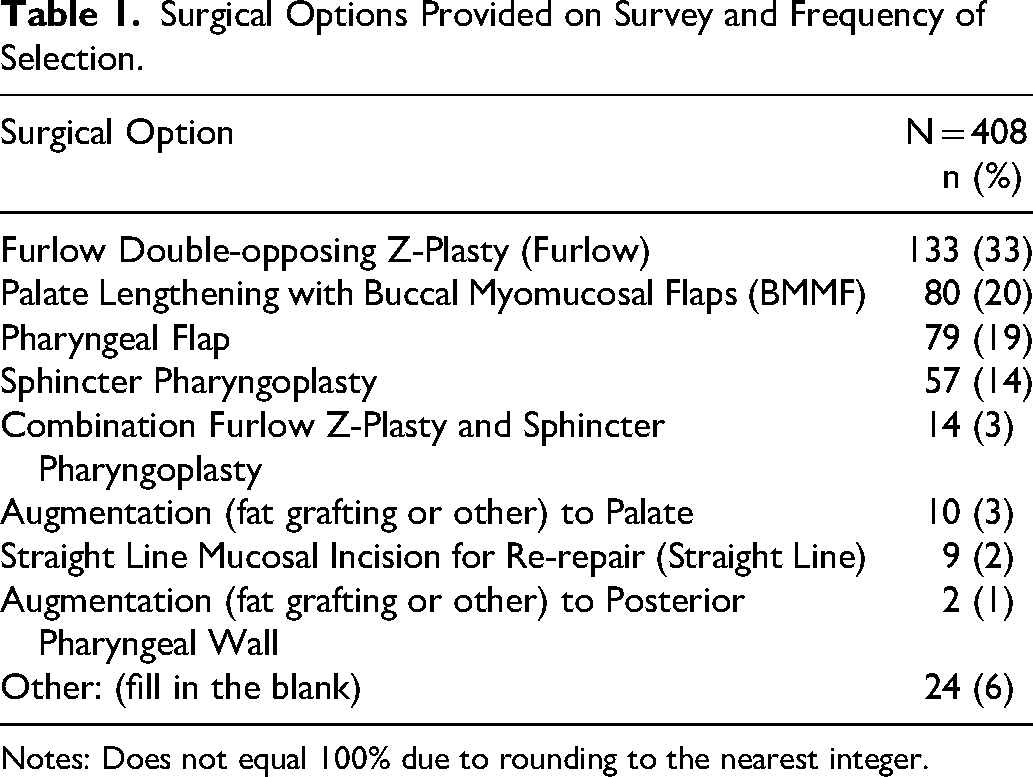
Notes: Does not equal 100% due to rounding to the nearest integer.
Rating of Nasopharyngoscopy Videos. The nasopharyngoscopy videos embedded in the survey had been previously rated by a panel of three trained and calibrated speech language pathologists (J.C.W., J.L.P.). Clinical features rated on nasopharyngoscopy included: closure pattern (mode across raters), and gap size quantified as total percent closure of the velopharyngeal port during speech (mean across raters) following standardized guidelines. 13 The videos were cropped to remove insertion of the scope into the naris, crying, clinicians talking to calm or encourage the child, and speech elicited below the syllable level (eg, sustained phonation). The average video time was 52 seconds. From a pool of 85 previously rated nasopharyngoscopy videos, 14 12 videos with coronal closure pattern were selected along with 12 videos with circular closure pattern. Closure pattern was rated as coronal if the velum was the primary contributor to closure; closure pattern was rated as circular if both the velum and lateral pharyngeal walls contributed to closure. 15 Inter-reliability was assessed for each clinical feature observed on nasopharyngoscopy. Examples of clinical features rated are shown in Figure 1. Lateral wall movement was not included as a separate variable in the analysis and was accounted for through closure pattern (more lateral wall motion with circular closure). No videos with sagittal closure pattern were included as none were available to the authors.
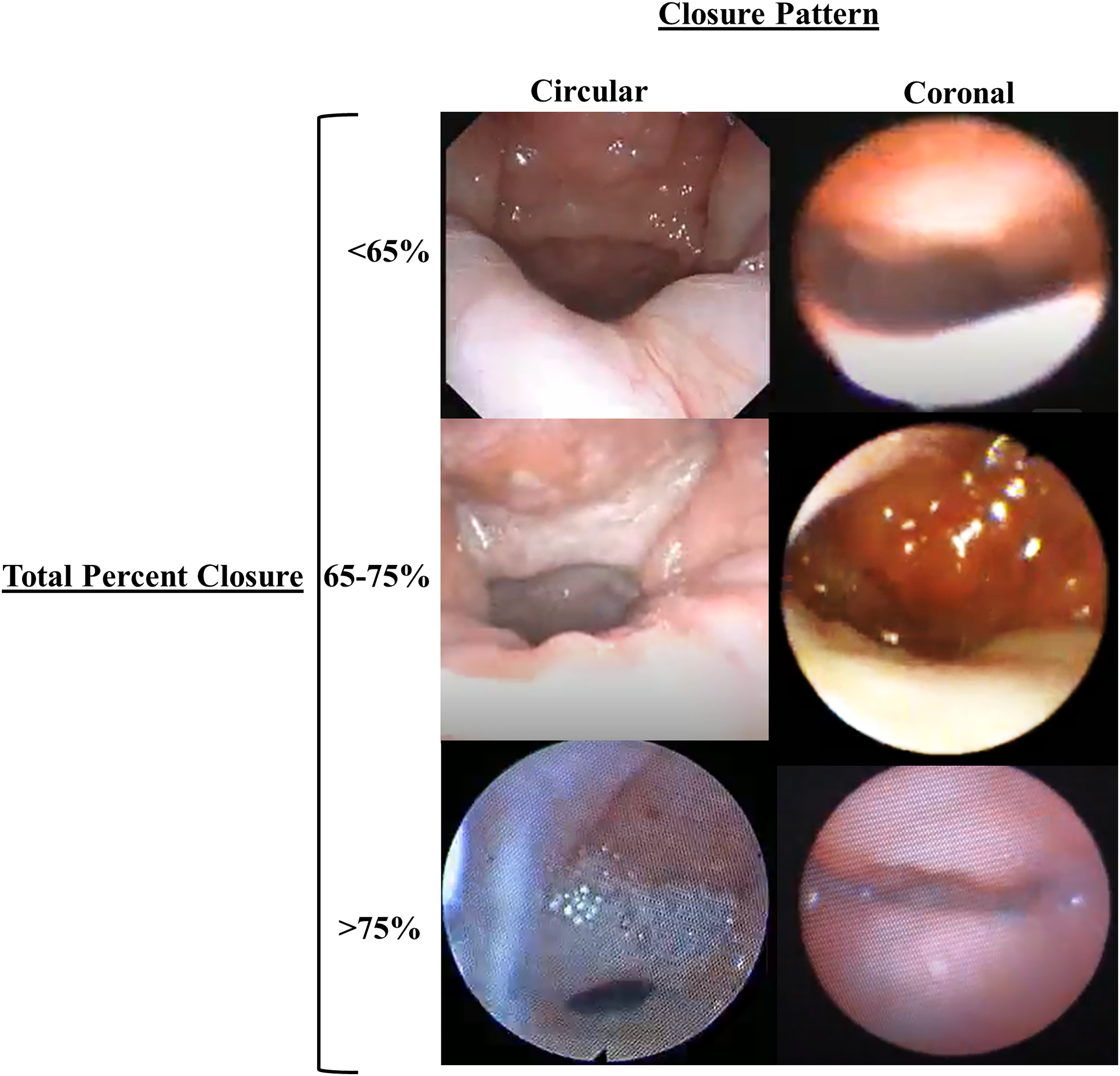
Examples of circular closure patterns are shown in the left column and coronal closure patterns are shown on the right. Gaps with <65% closure are shown in the top row, gaps with 65–75% closure in the middle row and gaps with >75% closure in the bottom row.
Statistical Analyses. Study data were collected and managed using REDCap electronic data capture tools hosted at Phoenix Children's Hospital.16,17 Statistical analyses were performed using the statistical software package STATA 17.0. Data were summarized using frequency and proportions. Fleiss's kappa was used to evaluate inter-rater reliability for closure pattern (k = 0.71). To assess reliability for total percent closure, the intraclass correlation coefficient (ICC) was used (ICC = 0.78).
To assess if surgeons change their surgical selection based on closure pattern, 12 videos with a circular closure pattern and 12 videos with a coronal closure pattern were shown. To assess if surgeons change their surgical selection based on percent of total closure, eight videos were shown with a total percent closure of <65%, eight videos with a total closure of 65–75%, and eight videos with a total closure of >75%. This provided a total of six different closure pattern/closure ratio video configurations for review, with four videos per configuration presented. The videos were randomized to avoid showing the same gap sizes or closure patterns in succession. After randomization, the videos were embedded in REDCap and all surgeons viewed the videos in the same order.
Chi-square tests of independence were used to test whether, for each surgeon, surgical selection varied based on the closure pattern and gap size combinations. Contingency tables were generated for each surgeon to compare the distribution of surgery selections across different closure pattern and gap size combinations. The alpha level was set at 0.05.
Nominal logistic regression was used to determine which features on nasopharyngoscopy change a surgeon's surgical selection from the most frequently selected procedure. The dependent variable was non-ordered procedures including Furlow double-opposing Z-Plasty, palatal lengthening using buccal myomucosal flaps, pharyngeal flap, and sphincter pharyngoplasty. Furlow double-opposing Z-Plasty was set as the reference procedure as it was the most selected procedure across all videos. Independent predictor variables included closure pattern (nominal variable) and total percent closure (continuous variable). Individual surgeons were not added as a variable to the model due to collinearity with surgical selection. The alpha level was set to 0.05.
A random forest analysis was used to assess the influence of nasopharyngoscopy findings and individual surgeon preference on the choice of procedure. A random forest analysis was selected as it can handle nonlinear relationships and complex interactions between predictors. 18 The outcome variable was the surgical procedure selected. Surgical procedures were grouped into 5 categories: Furlow double-opposing Z-Plasty, palatal lengthening using buccal myomucosal flaps, pharyngeal flap, sphincter pharyngoplasty, and all other procedures. The following procedures were consolidated into the category ‘all other procedures’ due to the low frequency of selection: Combination Furlow Z-plasty and sphincter pharyngoplasty, augmentation to palate, straight line mucosal incision for re-repair, augmentation to posterior pharyngeal wall, and other (fill in the blank). Predictor variables included total percent closure, closure pattern, and individual surgeons. Variable importance scores were obtained to quantify the contribution of each predictor variable on the outcome.
Results
Descriptive Data. A total of 17 surgeons from 11 different cleft centers completed the survey, for a response rate of 49%. The average total completion time was 20.7 minutes. All 17 surgeons selected a procedure for all 24 nasopharyngoscopy videos yielding a total of 408 surgical selections. Four procedures accounted for 86% of all surgeries selected: Furlow double-opposing Z-Plasty (33%), palatal lengthening using buccal myomucosal flaps (20%), pharyngeal flap (19%), and sphincter pharyngoplasty (14%). Table 1 shows the frequency of surgical selection for each procedure. Figure 2 shows the distribution of surgeries selected for each video.
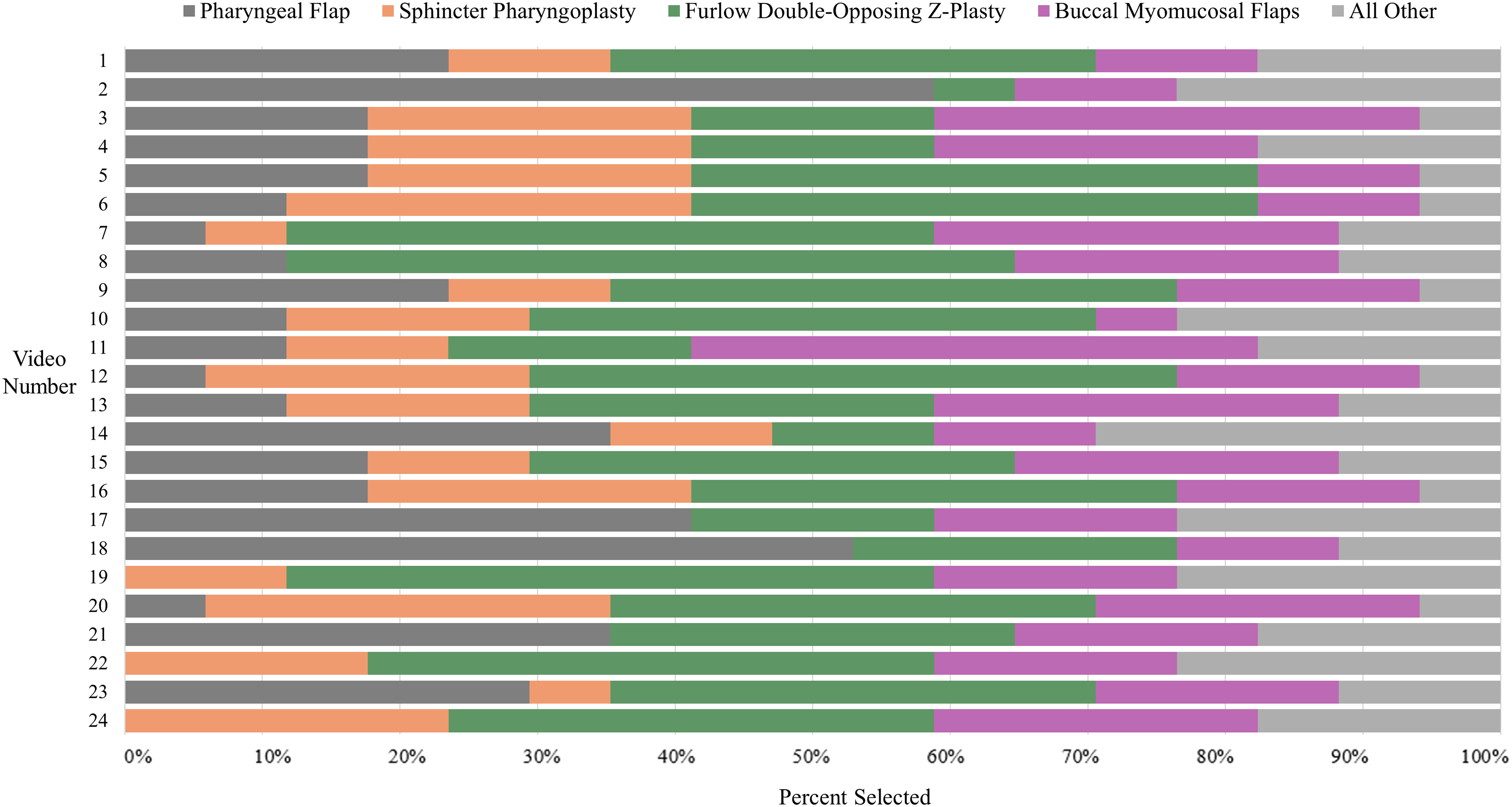
Distribution of surgeries selected by video.
Variation in Surgical selection by Feature Combination. The most common procedure selected (41.2%) for gaps with <65% closure with circular movement was a pharyngeal flap. Furlow double-opposing Z-Plasty was the most common procedure selected for all other gap size and closure movement combinations. Figure 3 shows the surgeries selected for closure pattern and gap size combinations by surgeon. Five surgeons (29%) selected the same procedure in ≥ 75% of the 24 nasopharyngoscopy videos; Five (29%) selected the same procedure in 50–74% of the videos. Only four surgeons (23.5%) significantly varied their surgical selection when different features combinations were shown on nasopharyngoscopy.
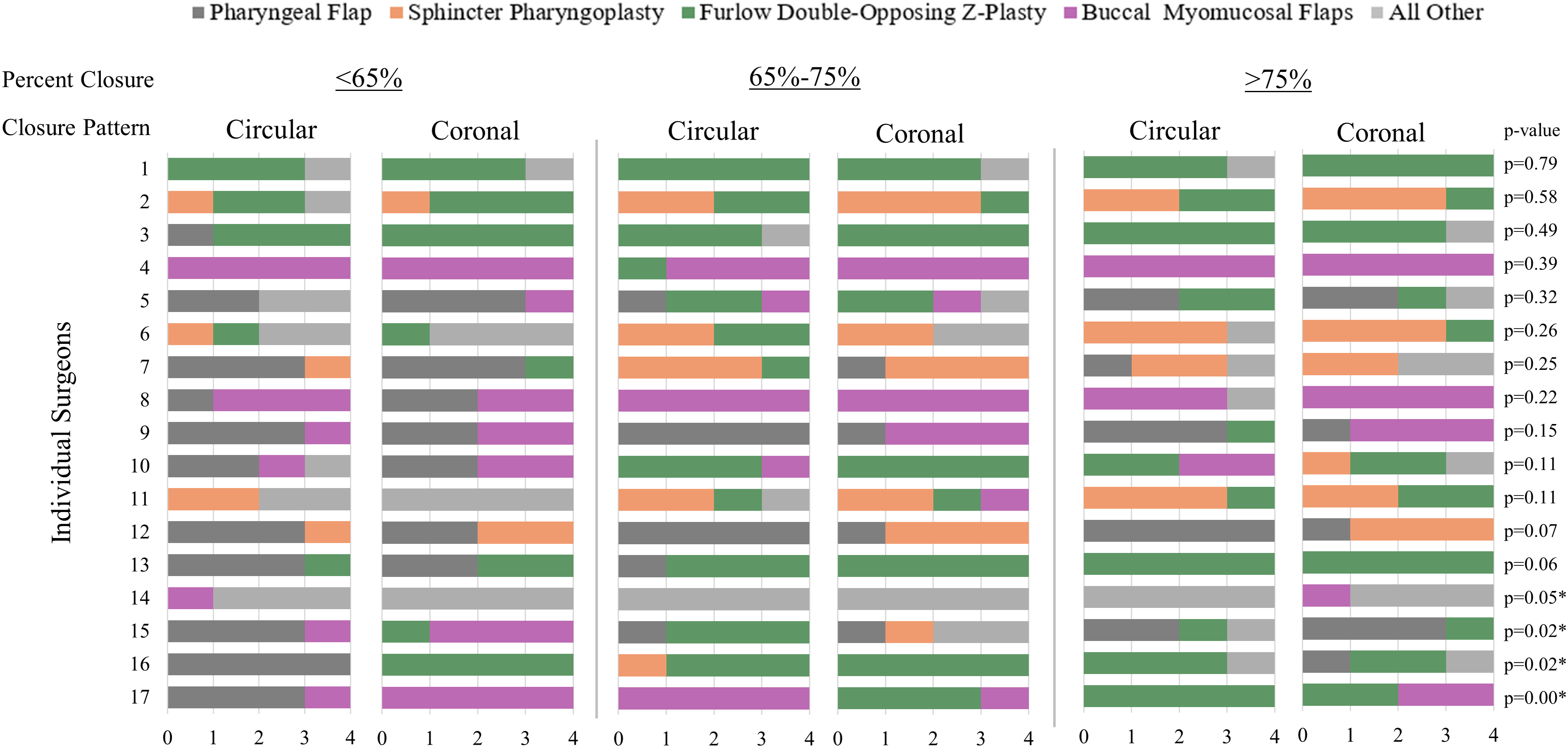
Surgical selection by individual surgeon. Four surgeons (14, 15, 16, 17) significantly varied their surgical selection when different features combinations were shown on nasopharyngoscopy (note: surgeon 14 demonstrated varied surgical selection across ‘all other’ category options). Five surgeons (29%) selected the same procedure in ≥ 75% of the 24 nasopharyngoscopy videos; five (29%) selected the same procedure in 50–74% of the videos.
Nominal Logistic Regression. Nominal logistic regression identifies predictors for non-ordered categorical outcomes, such as how features on nasopharyngoscopy influence surgical selection. Fourteen surgeons (82%) selected both palate-based and pharynx-based procedures. 19 As total percent closure decreased (larger gap sizes) surgeons were more likely to select a pharyngeal flap (p = 0.004) or a sphincter pharyngoplasty (p < 0.001) instead of a Furlow double-opposing Z-Plasty. Closure pattern did not impact selection of a pharyngeal flap (p = 0.183) or sphincter pharyngoplasty (p = 0.195). Neither total percent closure (p = 0.826) or closure pattern (p = 0.673) were associated with selection of buccal myomucosal flaps over a Furlow double-opposing Z-Plasty.
Predictors of Surgical selection. The random forest analysis built decision trees from the data and combined the decision trees to identify relationships between predictors−gap size, closure pattern, individual surgeons−and surgical selection. The random forest analysis identified individual surgeons as the strongest predictor of surgical selection, accounting for 57.9% of surgical selection variance. This was followed by total percent closure, which accounted for 36.5% of the variance in the outcome. Closure pattern was a weak predictor, contributing 5.6% to surgical selection variance. Figure 4 outlines the percentage of importance each variable contributed to the model.
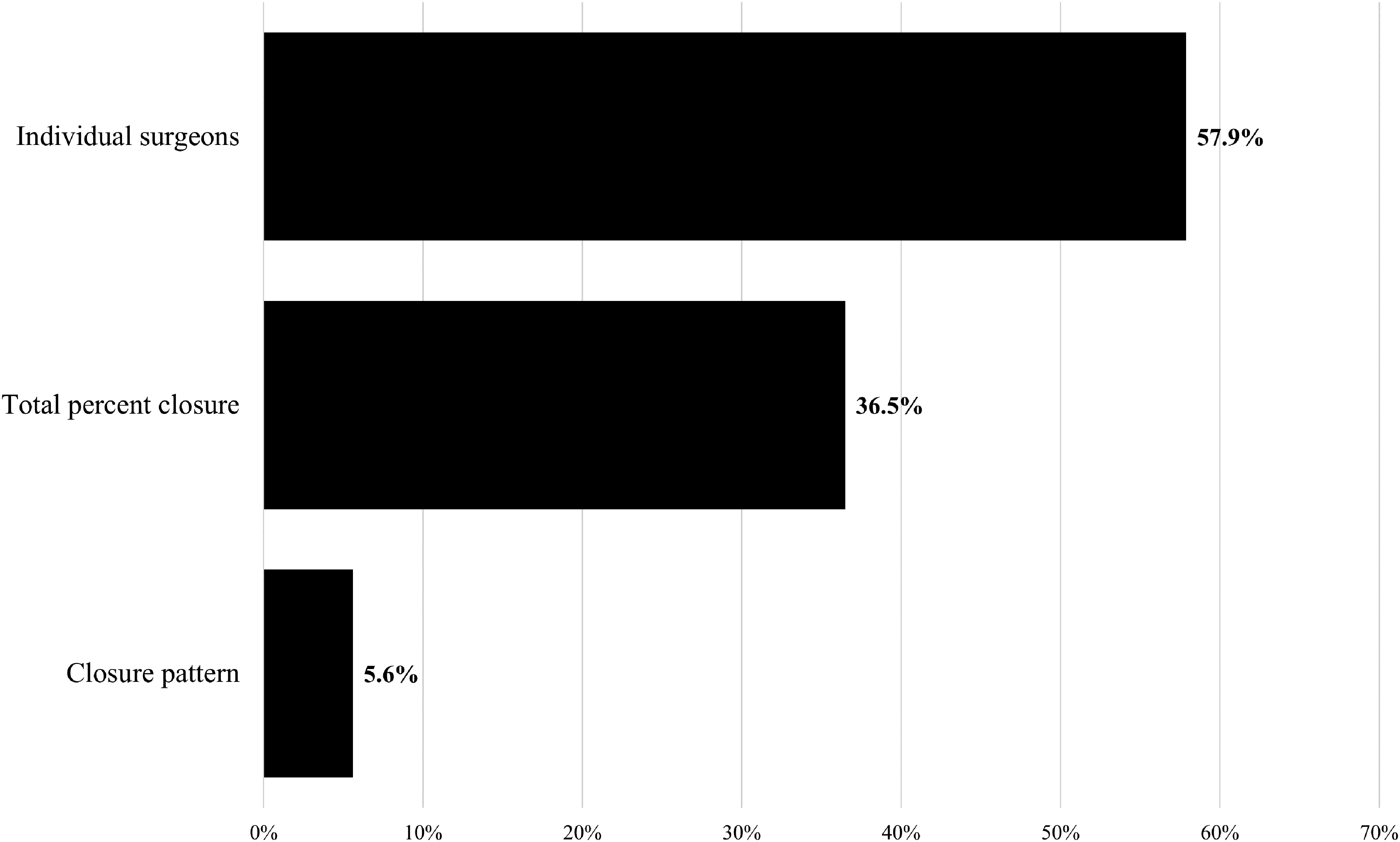
Feature importance for predicting surgical selection. Individual surgeons were the strongest predictor of surgical selection, accounting for 57.9% of selection variance, followed by total percent closure at 36.5%.
Discussion
The present study explored whether surgeons altered their surgical procedure selection based on gap size and closure pattern configurations as viewed on nasopharyngoscopy. No surgeon used the same surgical procedure for all cases, suggesting nasopharyngoscopy had at least some influence on surgical procedure selection. Still, 58% of surgeons used a single procedure in ≥50% of cases, and only 23.5% of surgeons demonstrated significant variation in their surgical procedure selection across gap size and closure pattern configurations. These findings suggest most surgeons have an individual preferred surgical procedure for VPI management in children with repaired cleft palate, moving away from their preferred procedure only in select cases.
Velopharyngeal Gap Size as the Most Influential Factor Evaluated on Nasopharyngoscopy
The study results are consistent with and extend prior research on the nasopharyngoscopy factors used in VPI surgical decision making for children with repaired cleft palate. The results indicate that movement away from a surgeon's preferred surgical procedure is driven primarily by velopharyngeal gap size: closure pattern accounted for 5.6% of variation in procedure selection, while gap size accounted for 36.5% of variation in procedure selection. This finding is consistent with a prior systematic review of VPI treating algorithms, in which gap size was the predominate feature of published surgical decision making pathways. 6 That systematic review identified velopharyngeal closure pattern as an important factor only when selecting between pharyngeal flap and sphincter pharyngoplasty,6,20 an approach which has been recommended by multiple surgeons.21,22 The present study identified only one surgeon (1 of 17, 5.9%) for whom use of pharyngeal flap and sphincter pharyngoplasty differed based on closure pattern. Taken together, these results suggest that visualization of gap size is currently the predominant decision-making factor obtained from nasopharyngoscopy outside of individual surgeon preference.
At the start of the survey, participants were informed that all children had undergone a Furlow double-opposing Z-plasty as their primary palatoplasty technique in infancy. Despite this, the Furlow procedure remained the most frequently selected option (33%) to treat VPI. Although some respondents may not have retained this detail throughout the survey, findings may be reflective of preference among some surgeons to initiate VPI management with a palate-based procedure for smaller gap sizes − including, reperforming a Furlow double-opposing Z-plasty. Gosain et al. demonstrated the feasibility of performing a secondary Furlow following a primary Furlow repair in 15 children with VPI, reporting successful restoration of levator muscle function and improved speech outcomes. 23 Similarly, Hsu et al. described favorable results in 13 patients with marginal VPI who underwent a redo double-opposing Z-plasty, with all patients achieving adequate velopharyngeal function postoperatively. 24 In the present study, surgeons more frequently selected a palate-based procedure, including Furlow palatoplasty, to treat smaller velopharyngeal gaps. This pattern is consistent with prior outcomes research that indicates palate re-repair is most effective to surgically manage smaller gap size.24,25
If surgeons have a preferred procedure for small and medium size gap sizes versus larger gaps, they could perform their preferred procedure based on the severity of perceptual hypernasality ratings and consider omitting nasopharyngoscopy. Prior research has shown velopharyngeal gap size is strongly associated with hypernasality severity as rated on perceptual speech evaluation. Smaller gap sizes are associated with lower hypernasality ratings, and larger gaps are associated with higher hypernasality ratings.26,27 One study rated gap size on nasopharyngoscopy as “small, medium, and large” and found that perceptual speech evaluation accurately predicted gap size in 70% of cases. 28 A more recent study assessed gap size using magnetic resonance imaging and found a moderate-to-strong positive correlation (r = 0.61) between hypernasality ratings and gap size. 26 The correlation between gap size and hypernasality ratings is consistent with interrater reliability for rating gap size on nasopharyngoscopy (R = 0.63). 29 These findings suggest that, for surgeons in whom gap size is the principal factor in surgical decision making, perceptual evaluation alone could be sufficient. Given the discomfort, 30 cost, and delays in treatment 11 associated with nasopharyngoscopy, along with the lack of evidence showing improved speech outcomes with the addition of nasopharyngoscopy,2,11,31 patients and families may welcome the opportunity to avoid nasopharyngoscopy.
Individualized Approaches to Surgical Decision Making
The present study highlights the individualized approach of applying nasopharyngoscopy imaging in the management of VPI. Individual surgeons accounted for 57.9% of variation in surgical procedure selection. This is consistent with prior research on VPI management, where surgeons at the same hospital frequently used different approaches. 32 Collectively, surgeons in this study utilized over eight different procedures for VPI management. There was no clear agreement or pathway for surgical selection across surgeons when viewing the same nasopharyngoscopy video. As Figure 2 shows, for every case study presented, at least four different surgical procedures were recommended.
Most surgeons (82%) selected both palate-based and pharynx-based procedures. 19 Among palate-based procedures, Furlow double-opposing Z-Plasty was selected slightly more frequently than palate lengthening with buccal myomucosal flaps (33% vs 20%). However, there were no clear criteria distinguishing when a surgeon would select between these two procedures. This surgeon-dependent decision making is supported by research which shows similar lengthening of the palate and similar improvement in degree of hypernasality with both operations. 5 Pharynx-based procedures, in particular pharyngeal flaps, tended to be chosen most frequently for larger gap sizes, when total velopharyngeal closure was <65%, but even in this setting many surgeons chose to perform palate-based operations. In sum, the results demonstrate that individual surgeon preferences are the predominant factor in determining how nasopharyngoscopy observations influence surgical procedure selection and surgeons do not apply findings from nasopharyngoscopy evaluations in the same way.
When Might Nasopharyngoscopy Not Be Useful for Surgical Decision Making?
There are at least three situations in which nasopharyngoscopy may not be useful for VPI surgical decision making. First, a surgeon may choose a procedure based on the underlying etiology of VPI such as recommending palate re-repair for all patients with non-syndromic cleft palate.2,11,32,33 Second, as noted earlier, when the surgical procedure selection is based entirely on gap size, ratings of hypernasality severity may be used as an accurate measure of gap size. Third, when teams have established surgical pathways based on prior surgical history, such as conversion Furlow palatoplasty following a straight-line repair in infancy. Moreover, each of these examples illustrates an opportunity to forego all advanced imaging, including nasopharyngoscopy, videofluoroscopy, and MRI. Such an imaging-free approach to VPI decision making does contradict established norms in the field and would need careful monitoring to confirm that speech outcomes are meeting published benchmarks. 32
Future Directions
All nasopharyngoscopy videos shown in this study included visualization of the entire velopharyngeal port at least one time in the video and a speech sample elicited in words and phrases. In a recent multisite study, Snodgrass et al. found 40% of nasopharyngoscopy videos failed to meet these quality criteria. 14 Future research should examine surgical selection when visualization of the velopharyngeal port is poor, to understand how surgeons proceed with managing VPI in real-word clinical practice. Future research should also assess if surgical selection changes for the same patient when the velopharyngeal mechanism is assessed using different imaging modalities, including nasopharyngoscopy, magnetic resonance imaging, and videofluoroscopy, as each of these modalities provided different views and measures of velopharyngeal anatomy.
Limitations
Results of this study must be interpreted within the context of study design.
The sample size in the present study was small. Evaluation of more case studies by each surgeon may have revealed small but statistically significant differences in surgery selection. A larger sample of surgeons would be unlikely to have substantially changed the principal findings, however, given the broad variation in surgical selection approaches identified in the present sample it is possible that surgeons rely on additional criteria not measured in this study to guide their surgical decision, which could have impacted the findings of this study. For example, some surgeons have reported using notching or grooving on the nasal surface, as an indicator of levator veli palatini muscle continuity, 34 though prior research has shown this finding has poor rater reliability, 29 and that it is not an accurate predictor of muscle continuity. 35 Additionally, some surgeons may not use nasopharyngoscopy for surgical selection, but rather to tailor specific aspects of their preferred procedure − such as the width of a pharyngeal flap 36 − which was not captured in this study. Nasopharyngoscopy videos in this study were limited to coronal and circular closure pattern, therefore decision making in instances of sagittal closure pattern could not be assessed. Additionally, the presence of Passavant's ridge during speech sound production was not analyzed and considered as a variable. Finally, surgical selection may have differed if the surgeon had collaborated with their team speech language pathologist to discuss findings.
Conclusion
Individual surgeons may prefer certain surgical procedures to treat VPI and their recommendation alters based on gap size; however, there was no clear agreement or pathway for surgical selection across surgeons when viewing the same nasopharyngoscopy video. These findings highlight the lack of consensus in VPI surgical selection, including disagreement on which factors on nasopharyngoscopy are important for surgical decision making and for which operation should be performed for any specific set of nasopharyngoscopy findings.
Footnotes
Acknowledgements
The authors would like to thank the surgeons who participated in this survey for their time and contribution.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Dental & Craniofacial Research (NIDCR) and the Office of the Director, National Institutes of Health (OD) under award U01DE029750. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
We have no additional conflicts of interest to disclose and have adhered to all ethical guidelines.