
Abstract
Background
Maxillary hypoplasia is a common sequela of cleft lip and palate (CLP), often requiring surgical correction through maxillary advancement osteotomy. However, the resulting aesthetic outcome can be unpredictable. Frequently, these cases involve maxillary lateral incisor agenesis, managed either by preserving the space for dental rehabilitation or through orthodontic space closure.
Purpose
To investigate the correlation between aesthetic and occlusal outcomes and the management of the missing maxillary lateral incisor space. Secondary objectives included assessing the relationship between aesthetic and occlusal scores and space management, nasolabial angle, the extent of maxillary advancement, and the maxillary incisor axis.
Study design
Retrospective cohort study.
Patients/participants
This retrospective study analyzed 47 patients with CLP sequelae who underwent maxillary advancement surgery between 2008 and 2022 at our center.
Intervention
Aesthetic evaluation and occlusal evaluation.
Main outcome variables
Aesthetic evaluation and occlusal evaluation were independently conducted by 5 examiners. Aesthetic and occlusal scores were deemed satisfactory if they exceeded ≥30 of 40 and 15 of 20, respectively. These outcomes were correlated with the preservation of the maxillary lateral incisor space, extent of maxillary advancement, nasolabial angle, and maxillary incisor axis.
Results
No significant improvement in aesthetic or occlusal outcomes was observed, regardless of whether the maxillary lateral incisor space was preserved. However, space closure was associated with greater maxillary advancement (P = .025).
Conclusions and relevance
Orthodontic space closure may lead to better outcomes. Further research involving larger sample sizes and consideration of additional factors is needed to determine the optimal approach for each patient.
Keywords
Introduction
Cleft lip and palate (CLP) is the most prevalent craniofacial malformation, affecting up to 1 in 700 births worldwide. 1 The reparative journey is complex, involving multiple interventions from infancy into adulthood. 2 Maxillary retrusion is a common consequence of CLP, resulting from a deficiency in maxillary growth across all dimensions, primarily attributed to multiple surgeries, particularly those performed in early childhood. Its prevalence ranges from 6% to 48% across various studies, depending on the timing and protocols of primary treatment.3,4 Addressing maxillary hypoplasia typically involves a combination of orthognathic surgery and orthodontic intervention. Surgical approaches include maxillary advancement through conventional orthognathic procedures or external distraction devices.5,6 The primary goals of maxillary advancement are to correct occlusion toward an angle class I relationship and to enhance the aesthetic profile. 7 However, morphological outcomes remain unpredictable, as skeletal adjustments can yield variable responses across different cleft types. Aesthetic consequences may include a flattened midface appearance, a straight or retrusive upper lip, a closed nasolabial angle—often resulting from a drooping nasal tip and reduced maxillary projection—, and the appearance of lower lip eversion.
In addition, patients with CLP frequently exhibit the absence of the maxillary lateral incisor on the side of the cleft, either due to agenesis or subsequent extraction necessitated by undersized or malformed teeth. Collaboration between orthodontists and surgeons is essential in formulating optimal strategies to manage the resulting space. In orthodontic–surgical management, the approach depends on whether the space for the absent or unusable lateral incisor is preserved or closed. Orthodontic space closure (OSC) involves mesial movement of adjacent teeth, with the adjacent canine substituting for the missing incisor. Conversely, space preservation involves maintaining the gap throughout treatment, allowing for potential subsequent prosthetic dental rehabilitation (PDR).
The primary objective of this study was to evaluate whether space preservation influences aesthetic and occlusal outcomes following maxillary advancement surgery. Secondary objectives included assessing the impact of space preservation on the magnitude of maxillary advancement and examining other factors influencing final aesthetic results, such as the extent of maxillary advancement, the axis of central incisors, and the nasolabial angle.
Materials and Methods
Study Design, Patient Selection, and Surgery
We conducted a single-center, analytical, retrospective cohort study involving patients with CLP sequelae who underwent orthognathic surgery between 2008 and 2022. Inclusion criteria included individuals with unilateral or bilateral CLP accompanied by maxillary retrusion, who underwent orthognathic surgery and exhibited the absence of the maxillary lateral incisor on the cleft side. Exclusion criteria included missing data, refusal by patients or caregivers to participate, syndromic presentations, or concurrent surgeries such as septorhinoplasty or other soft-tissue procedures altering midface morphology.
The surgical procedure primarily involved conventional orthognathic techniques, typically a Le Fort I osteotomy for maxillary advancement, optionally combined with a bilateral sagittal split osteotomy. The Le Fort I osteotomy included complete mobilization of the maxilla, down-fracture, and pterygomaxillary disjunction. All orthognathic procedures were performed by the same surgeon.
Orthodontic treatment for all patients focused on aligning the dental arches, with or without preserving the space left by the absent maxillary lateral incisor. Patients were treated by orthodontists specializing in cleft care, with whom we routinely collaborate, though not all patients were treated by the same orthodontist.
This was a single-center, retrospective cohort study. Because of its retrospective nature, the study was formally granted an exemption from requiring approval by the ethics committee of Our University Hospital, in accordance with French legislation Article L 1121-1 paragraph 1 and R1121-2 of the Public Health Code.
Evaluation Methods
Demographic, orthodontic, and surgical data were collected from patient medical records, including gender, cleft type, age at surgery, type of surgical procedure, and the approach to managing the orthodontic space resulting from the absence of the maxillary lateral incisor.
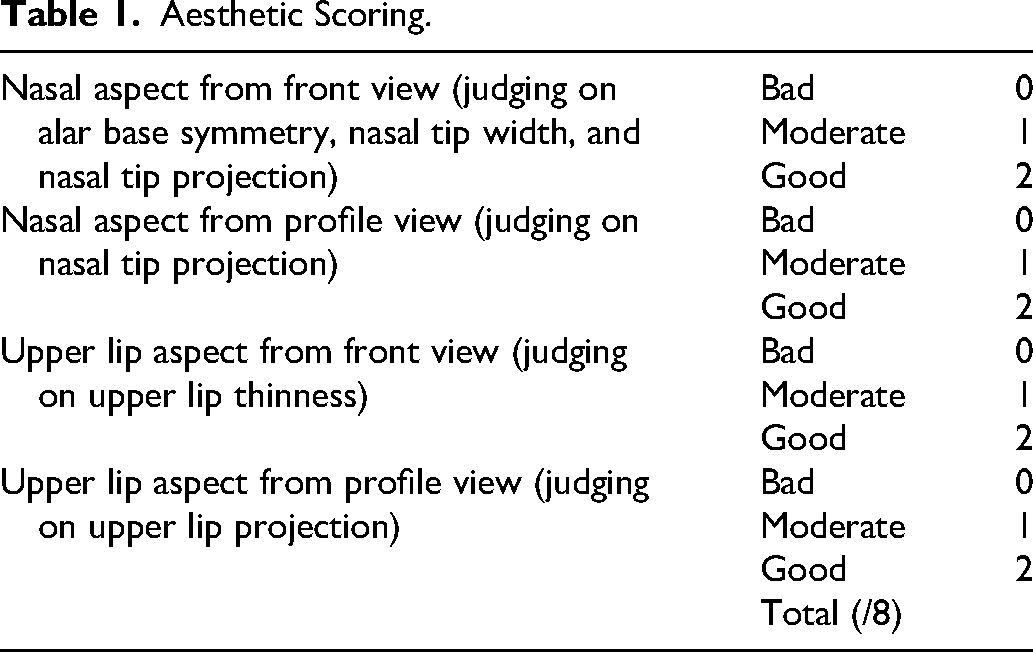
Aesthetic assessment was performed using a scoring system outlined in Table 1. The evaluation was carried out by 3 surgeons specializing in CLP and 2 maxillofacial surgery residents who have already completed a rotation in pediatric maxillofacial surgery. Standardized photographs were utilized, including static images taken from frontal, right and left profile views, and a lower view, as well as dynamic images capturing the patient smiling. Each examiner graded aesthetic features on an 8-point scale, resulting in a total score out of 40. A good aesthetic outcome was defined as a score of ≥30 of 40.
Aesthetic Scoring.
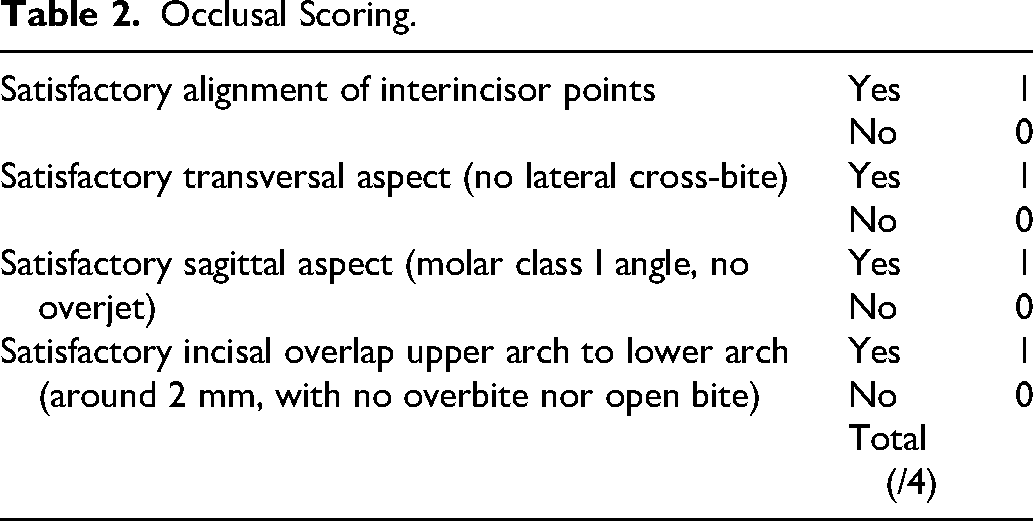
Occlusal evaluation followed a scoring method described in Table 2 and was conducted by the same 5 examiners using standardized photographs of dental occlusion. Scores were assigned for specific aspects, with each examiner grading up to 4 points, leading to a total score out of 20. A good and satisfactory occlusal outcome was defined as a score of ≥15 of 20. Figures 1 and 2 illustrate examples of good and poor occlusal and aesthetic scores.

Example of a Good Aesthetic and Occlusal Result, with Satisfactory Projection of the Middle Third and A Good Occlusion: (A) Frontal View, (B) Left Profile, (C) Right Profile, and (D) Occlusal View.

Example of a Poor Result, with an Inadequate Occlusal Result and an Unsightly Profile with Persistent Maxillary Retrusion: (A) Frontal View, (B) Left Profile, (C) Right Profile, and (D) Occlusal View.
Occlusal Scoring.
Radiographic measurements were taken from postoperative profile teleradiographs obtained 1 year after surgery and included the following parameters:
Maxillary advancement (in mm): Measured by superimposing preoperative and postoperative radiographs on the cranial base and measuring the displacement of subspinal point A in a sagittal direction exclusively. Maxillary incisor axis (in °): Determined by drawing a line along the long axis of the most prominent maxillary incisor and measuring its inclination relative to the palatal plane (defined as the line connecting the anterior nasal spine and posterior nasal spine). Nasolabial angle (in °): Measured as the angle formed by 2 intersecting lines, one extending from the nose and the other from the upper lip.
Statistical Analyses
Normality was assessed, and data were treated as a sample with a normal distribution. All continuous measures are presented as mean ± standard error of the mean (SEM), while categorical data are expressed as N (%). Statistical analyses were conducted using Jamovi® software (Jamovi, Sydney). Binomial logistic regression was employed to evaluate the impact of space retention on aesthetic and occlusal outcomes. Linear regression was used to examine the relationship between space retention and the extent of maxillary advancement, the axis of the maxillary central incisors, and the nasolabial angle. The reliability and interrater reproducibility of the measurements and scoring were analyzed with a calculation of an intraclass correlation coefficient (ICC). Based on the 95% confident interval of the ICC estimate, values less than 0.50, between 0.50 and 0.75, between 0.75 and 0.90, and greater than 0.90 were indicative of poor, moderate, good, and excellent reliability, respectively as defined by Koo et al. 8 Statistical significance was defined as P ≤ .05 and was denoted by *.
Results
General Results
Samples were equally distributed in each group. 88 patients were initially included in the study, 11 were excluded because of missing data. Finally, 47 patients were included and analyzed.
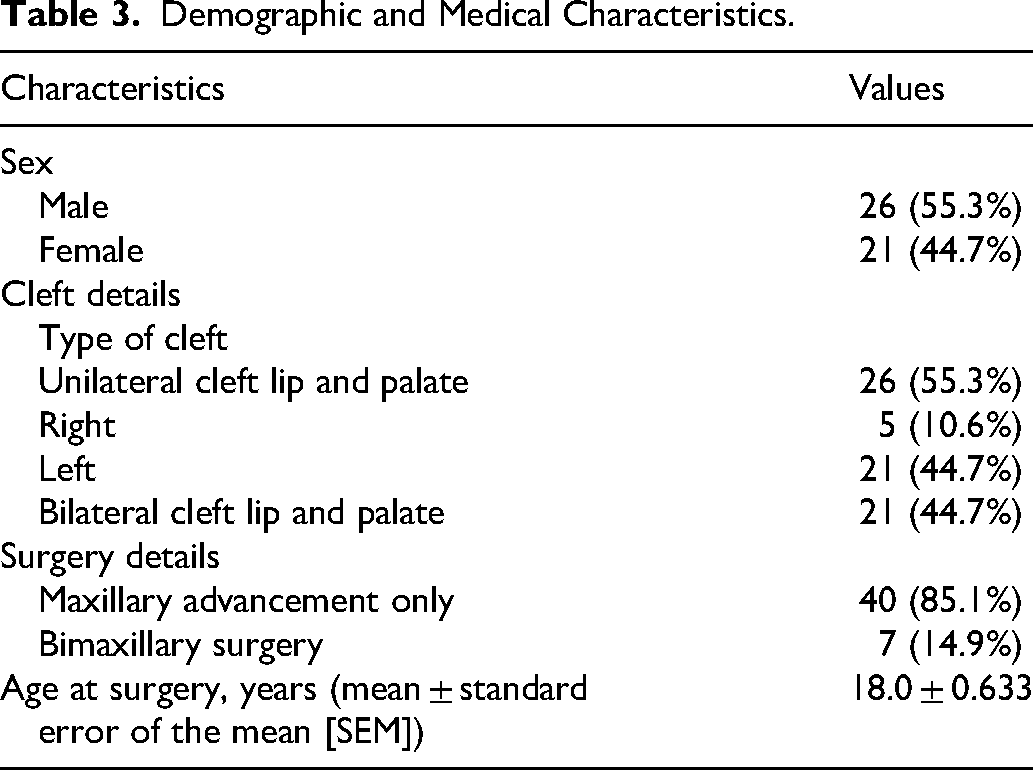
There were 44.7% of female patients and 55.3% of male. In total, 44.7% of the clefts were bilateral CLP and 55.3% of them were unilateral CLP. A total of 40.4% patients had OSC and 59.6% had PDR. Demographic and medical characteristics are presented in Table 3.
Demographic and Medical Characteristics.
Primary Outcome
Statistical descriptions are presented in Tables 4 and 5.
Statistical Descriptive Analyses of Patients with UCLP and BCLP.
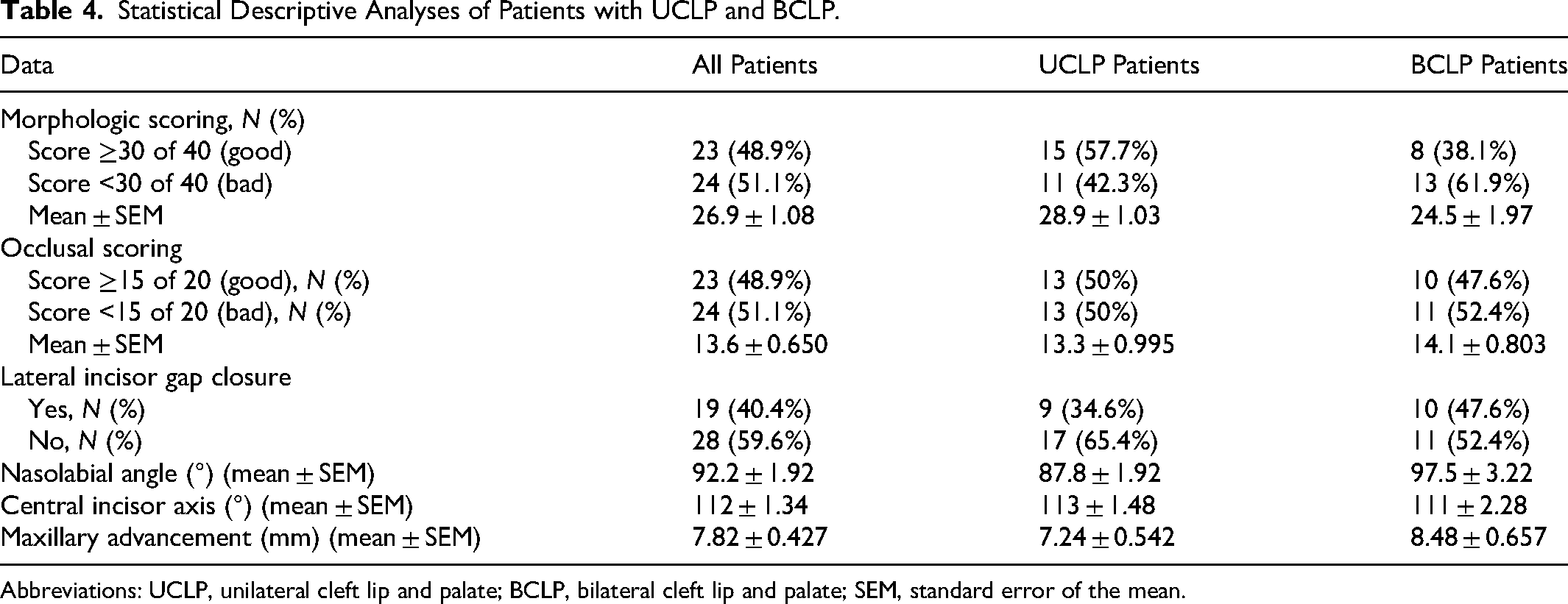
Abbreviations: UCLP, unilateral cleft lip and palate; BCLP, bilateral cleft lip and palate; SEM, standard error of the mean.
Statistical Descriptive Analyses of Patients According to the Management Strategy.
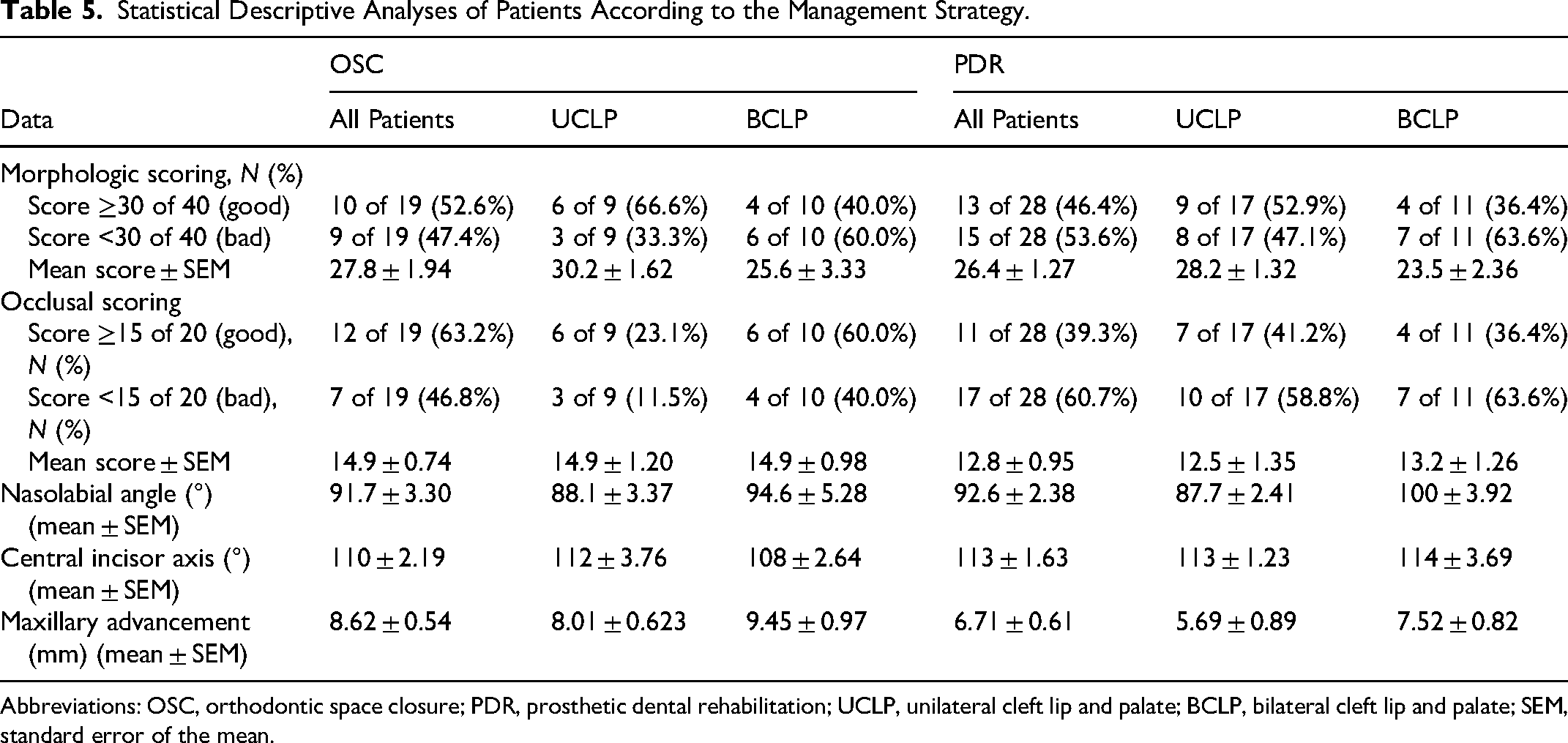
Abbreviations: OSC, orthodontic space closure; PDR, prosthetic dental rehabilitation; UCLP, unilateral cleft lip and palate; BCLP, bilateral cleft lip and palate; SEM, standard error of the mean.
Statistical results of aesthetic and occlusal scoring association with lateral space conservation are presented in Table 5. OSC increased the chances of a good esthetic score by 22% and a good occlusal score by 20%, but not significantly, suggesting that closing the space provided a better aesthetic and occlusal result.
Secondary Outcomes
No significant relation was found between nasolabial angle, incisor axis, or maxillary advancement with neither the aesthetic nor occlusal scoring. Regarding the aesthetic score, the odds ratio (OR) for the nasolabial angle was 1.01, with a 95% confidence interval (CI) ranging from 0.948 to 1.08, and a P value of .754, indicating no statistically significant association. Similarly, the incisor axis had an OR of 1.08 (95% CI: 0.981-1.18), with a P value of .119, also not statistically significant. Maxillary advancement showed an OR of 0.94 (95% CI: 0.705-1.24) with a P value of .642, again suggesting no significant relationship with the aesthetic score. For the occlusion score, the same 3 variables were assessed. The nasolabial angle had an OR of 1.04 (95% CI: 0.974-1.12) with a P value of .223, indicating a lack of statistical significance. The incisor axis demonstrated an OR of 1.06 (95% CI: 0.956-1.18), with a P value of .264, and maxillary advancement showed a lower OR of 0.793 (95% CI: 0.578-1.09), with a P value of .151. None of these associations reached statistical significance, suggesting that within this analysis, these anatomical and positional factors were not strongly correlated with variations in either aesthetic or occlusion scores (Table 6).
Factors Associated with a Risk of Having a Good Aesthetic and Occlusal Score.

Regarding dental space management, the nasolabial angle did not appear to be influenced by whether lateral spaces were conserved or not. However, maxillary advancement was significantly affected. The model coefficient for maxillary advancement indicated that OSC was associated with a significant increase of 1.91 ± 0.82 mm in maxillary advancement amplitude (95% CI: 0.252-3.58; P = .025).
Model coefficient of maxillary advancement showed that OSC significantly increased of 1.91 ± 0.82 mm (95% CI: 0.252-3.58) the amplitude of maxillary advancement (P = .025).
Interrater Reliability Rate
Using ICC coefficients, interexaminer reliability was found to be excellent for both aesthetic and occlusal scoring with narrow 95% CIs (0.92 [0.87-0.95] and 0.91 [0.86-0.95] respectively).
Discussion
Individuals with CLP often present with a skeletal class III relationship and varying degrees of maxillary hypoplasia. 9 Le Fort I maxillary advancement is a widely used surgical technique to address maxillary skeletal deficiencies. 10 The primary goal of this procedure is to improve occlusion, ideally achieving an angle class I relationship, while enhancing the aesthetic profile. However, predicting morphological outcomes remains challenging, particularly in soft-tissue responses such as upper lip projection. 11 Residual deformities, including insufficient projection of the upper lip and nasal tip, are common postoperatively, especially in CLP patients where extensive scarring makes tissue detachment more complex compared to noncleft individuals. 12
This study aimed to investigate whether the strategy for managing the space of the missing maxillary lateral incisor influences surgical outcomes. Maxillary lateral incisor agenesis or hypoplasia is the most frequent dental anomaly in patients with CLP.13,14 Effective collaboration between surgeons and orthodontists is essential to plan the best approach for managing the gap left by the missing tooth.
The first option is OSC, which consists in mesially bringing the homolateral canine adjacent to the central incisor and shaping its form to make it look like the missing lateral incisor. This strategy offers the advantage of reestablishing dental arch continuity and avoiding a prosthetic replacement, which entails notable costs and requires lifetime maintenance. 15 OSC thus results in a less costly treatment that does not have to be postponed until the end of growth, and in which adjacent healthy teeth do not have to be prepared. 16 This strategy offers several advantages, including cost reduction, the possibility of completing treatment more quickly, improved periodontal health, and superior aesthetic outcomes compared to prosthetic options. Additionally, OSC promotes a more favorable periodontal prognosis. 17 OSC may also be indicated when there is insufficient space (<6 mm) to restore the missing lateral incisor with another treatment option. 18 However, some authors criticize this technique, declaring that it may lead to maxillary hypoplasia in both transversal and anteroposterior dimensions, necessitating further orthognathic surgery. 19 It may also lead to ventilatory disorders by reducing the intercanine distance and thus the size of the nasal aperture. 20
The second option involves maintaining the space between the central incisor and the canine orthodontically to facilitate PDR. Some authors suggest that this approach yields better functional and aesthetic outcomes, including improved projection of the upper lip and a symmetrical dental arch. 6 Other reasons for choosing this approach include maintaining symmetry in cases of unilaterally missing incisors and ensuring adequate space for the tongue. 21 This strategy entails a longer orthodontic treatment duration and necessitates a prosthetic replacement solution, which can be achieved through options such as dental implants or fixed prostheses like resin-bonded or fixed partial dentures. Dental implants are considered the most conservative option, offering a good survival rate and satisfactory quality of life. 22
Good stability has been reported following both OSC and PDR.23-25 The choice of management strategy may consider various factors, such as the practitioner's preferences, the patient's socioeconomic status and dental insurance coverage, or the patient's oral hygiene practices. 26
The literature on space management for missing lateral incisors is relatively limited. Our cohort was representative, with demographic data and cleft characteristics similar to those observed in previous studies.
In total, 40.4% of our patients benefited of OSC and 59.6% of PDR. These are close rates to previously reported in other studies for different populations: Lee et al found 58.5% of PDR for both unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP), 19 Cassolato et al found 17.2% of PDR in UCLP patients, 15 Oosterkamp et al found 37% of PDR in BCLP, 16 Quenel et al found 77.3% in UCLP patients and 52.6% in BCLP patients. 26
Regarding our primary outcome, we observed no significant difference. Our findings indicate that closing the space prior to maxillary advancement may yield improved aesthetic and occlusal outcomes, although not reaching statistical significance.
Oosterkamp et al conducted a study comparing subjective smile perception following OSC and PDR in patients with BCLP sequelae. Their findings revealed no significant differences in smile perception between the 2 groups. However, in terms of function, PDR was associated with greater impairment in specific masticatory functions, potentially due to concerns about damaging the prosthetic work. 16 Robertsson and Mohlin evaluated patient opinions on aesthetic outcomes between PDR and OSC in a noncleft population missing a maxillary lateral incisor. Their study found no significant differences in patient preference for either method. They concluded that OSC provides outcomes well-accepted by patients, preserves temporomandibular joint function, and promotes better periodontal health compared to PDR. 21
In contrast, Quenel et al investigated the effects of space management for missing maxillary lateral incisors on dental arch relationships and symmetry in UCLP and BCLP populations. Their study showed that PDR resulted in better dental arch relationships and positively influenced the position of the upper interincisal point on the facial midline, particularly in unilateral cases. For bilateral cases, the management approach had no significant impact. 26 It is important to note, however, that Quenel et al included all cleft types, including partial clefts, which differ from the focus of our study.
An intriguing aspect of our study lies in the secondary objectives. Specifically, when patients undergo OSC, there is a notable increase in the extent of maxillary advancement (P = .025), with an estimated value of 1.91 mm. These findings align with those of Hoang et al, who observed that Le Fort I maxillary advancement is greater in cleft patients with dental agenesis. When dental agenesis was managed with canine substitution, Le Fort I advancement increased. 27
This discovery is noteworthy considering that a primary concern in CLP patients’ profiles is the lack of upper lip projection and a drooping nasal tip. Closing the lateral incisor space appears to have artificially exacerbated the sagittal shift, thereby enhancing the potential for maxillary advancement. This, in turn, contributes to better forward projection of the upper lip and overall improvement in profile aesthetics. Chew et al., highlighted the importance of profile aesthetics in subjective perception, making it a crucial criterion. 28
Without space closure, some patients might have experienced only minimal advancement, resulting in limited aesthetic improvement. While this criterion is exploratory and does not allow for definitive conclusions, it opens an interesting avenue for further investigation.
Our study stands out as the first to evaluate both aesthetic and occlusal outcomes based on the planned management of the space resulting from the missing maxillary lateral incisor.
However, there are several limitations to our study, primarily due to its retrospective design and the relatively small sample size. As a result, some differences may not have reached statistical significance, and further prospective studies are needed to confirm our findings. It would have been valuable to explore the influence of initial dental arch relationships on the decision-making process regarding the management of the maxillary lateral incisor space. Unfortunately, such data were not available in our cohort.
Additionally, evaluators could not be blinded to the treatment undergone by the patient, as this information was apparent from the photographs. Another limitation is that the occlusal evaluation was not performed by dental experts. Occlusion and dental aesthetics may be more accurately assessed by orthodontists or dentists/prosthodontists. Another limitation of our study is the use of nonvalidated aesthetic and occlusal scoring systems; although, these were developed based on existing literature and the expertise of surgeons experienced in CLP treatment. Aspects such as gingival shape and height, tooth size, and shade might be overlooked by other healthcare professionals. Finally, aesthetic scoring can be subjective, potentially introducing bias. To mitigate this, scoring was conducted by 5 different examiners, and interrater reliability was calculated, yielding excellent results.
Conclusion
Space management of the missing lateral incisor is a topic that has received limited attention in the scientific literature. Our study represents the first attempt to investigate the impact of space management strategies on both final aesthetic and occlusal outcomes. Assessing these criteria objectively, even with photographs, presents significant challenges in practice. In our study, OSC appeared to be associated with improved aesthetic and occlusal outcomes, although not significantly. The aesthetic outcome in cases of canine substitution depends on several factors, including the shape and shade of the canine, the gingival margin, and the size of the canine—all of which are important to consider. OSC seems to increase maxillary advancement, benefiting both upper lip projection and nasal tip projection.
The goal of our work is not to claim any absolute conclusions but rather to offer an additional point of reflection in the preparation for these complex procedures, particularly maxillary osteotomies for CLP sequelae. Further studies with larger sample sizes are needed to substantiate these preliminary findings. Additionally, the inconclusive results of our study emphasize the need for individualized space management strategies for the missing lateral incisor in patients with CLP, with multidisciplinary collaboration among surgeons, dentists, and orthodontists. Factors such as treatment duration, oral hygiene, and rehabilitation costs must be considered to propose the most suitable option tailored to each patient.
Footnotes
Abbreviations
Acknowledgments
We thank Mrs Caroline Charles and the orthodontists who gave their help in the study.
Ethical Considerations
This was a single-center, retrospective cohort study. Because of its retrospective nature, the study was formally granted an exemption from requiring approval by the ethics committee of Grenoble University Hospital, in accordance with French legislation Article L 1121-1 paragraph 1 and R1121-2 of the Public Health Code.
Patient Consent
Written informed consent was obtained for the use of photographs.
Author Contributions
Alexandra Delay: methodology, data curation, and conceptualization.
Virginie Lafontaine: Data curation.
Clément Dutheil: Data curation.
Aurélie Vigneron: Data curation.
Béatrice Morand: project administration, methodology, and conceptualization.
Georges Bettega: methodology, project administration, methodology, and conceptualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.