
Abstract
Objective
To investigate whether the use of buccal fat pad flap during cleft palate repair reduces the risk of post-operative palatal fistula formation.
Design
Retrospective analysis of cleft palate repairs undertaken by a single surgeon over the period 2013–2025.
Setting
Tertiary care institution in London.
Patients
Two hundred and seventy-seven patients (146 female, 131 male) who underwent cleft palate repair between 2013 and 2025 were included in the study. One hundred and seventy-three patients had an isolated cleft palate, 78 patients had a unilateral cleft lip and palate, and 26 patients had a bilateral cleft lip and palate. The range of cleft width treated was 3–22 mm. The standard surgical technique employed a Sommerlad style intravelar veloplasty with von Langenbeck releases where necessary.
Interventions
The utilization of pedicled buccal fat pad flap in primary cleft palate repairs.
Main Outcome Measure(s)
Development of post-operative palatal fistula.
Results
Among 277 patients, 21 (7.6%) patients developed a post-operative fistula, most commonly in Zone IV (52%). The fistula rate was 3.7% with buccal fat pad flap use compared with 8.5% without (P = 0.39). Bayesian logistic regression showed a two-thirds reduction in the odds of fistula formation (odds ratio [OR] = 0.33; 95% credible interval [CrI]: 0.15–0.74), suggesting a high probability of a protective effect.
Conclusions
This study demonstrates that the use of buccal fat pad flaps in primary cleft palate repair is an effective adjunct associated with a reduced incidence of post-operative oronasal fistula.
Introduction
Cleft lip and palate is a global problem, affecting approximately 10 million people worldwide. 1 Isolated cleft palate (ICP) has an incidence varying between 1 and 25 per 10,000 live births depending on geographical location. 2 Palate repairs are performed to facilitate speech development and to prevent nasal regurgitation during feeding. Numerous palatoplasty techniques have been described but 2 of the commonest techniques are the intravelar veloplasty as modified by Sommerlad and the Furlow double-opposing Z-plasty.3,4 The main goals of palatoplasty are separation of the oral and nasal cavities, reorientation of levator veli palatini and achieving a watertight, tension-free closure.
Palatal or oronasal fistula formation is a recognized complication of palatoplasty, typically resulting from impaired healing or wound dehiscence at the site of primary cleft palate repair. The presence of palatal fistula can lead to speech hypernasality, difficulty with articulation and regurgitation of food and liquid. Consequently, post-operative palatal fistula formation provides a useful surgical outcome measure. The reported incidence rates of palatal fistula vary widely in the literature, from 0 to 77.8%. 5 Possible reasons for this wide variation include lack of uniform definition and reporting bias. 6 Buller et al. performed a systematic review in 2023 and cited a few meta-analyses that are most likely to provide the best estimates of the incidence of palatal fistula, between 6.4% and 8.6%. 6
Palatal fistulae have been associated with multiple factors including type and severity of cleft, patient's age at the time of operation, repair technique, tension at the site of closure and surgeon experience.7–9 Over time, various surgical techniques have been developed to reduce the risk of palatal fistula formation following palatoplasty. In particular, the use of pedicled buccal fat pad has gained increasing popularity in recent years.10,11 The buccal fat pad was first identified by Heister in 1732 and later more thoroughly described by Bichat in 1802. Its use in the closure of oronasal fistulae was first reported by Egyedi, and it has continued to remain a valuable adjunct in the surgical repair of palatal defect.12,13 In 2009, Levi described a technique in which a buccal fat pad flap was placed beneath the mucoperiosteal flaps of the Furlow repair to reinforce areas of high tension in 10 patients undergoing primary cleft palate repair. 14 No patients had complications related to the donor site and there was no fistula formation observed at 3 months follow-up. 14
This article aims to report our 13-year experience and outcomes using the pedicled buccal fat pad in cleft palate repair performed by a single surgeon.
Patients and Methods
A retrospective evaluation was performed on all patients who underwent cleft palate repair by a single surgeon at the our Hospital over 13 years from 2013 to 2024 inclusive. Clinical data gathered were gender, type of cleft: ICP, unilateral complete cleft lip and palate (UCLP) and bilateral complete cleft lip and palate (BCLP), severity of cleft (width), use of lateral releases or buccal fat pad, presence of post-operative fistula and fistula location. A total of 277 patients were treated, consisting of 147 female and 130 male children. In this study, the formation of palatal fistula was considered the final outcome data.
Surgical Technique
Cleft palate repair is performed according to our standardized protocol, using the Sommerlad intravelar veloplasty (IVVP) technique.3,15 Lateral releases and pedicled buccal fat pad (Figure 1) are used as adjuncts when indicated, and the decision is made on a case-by-case basis.
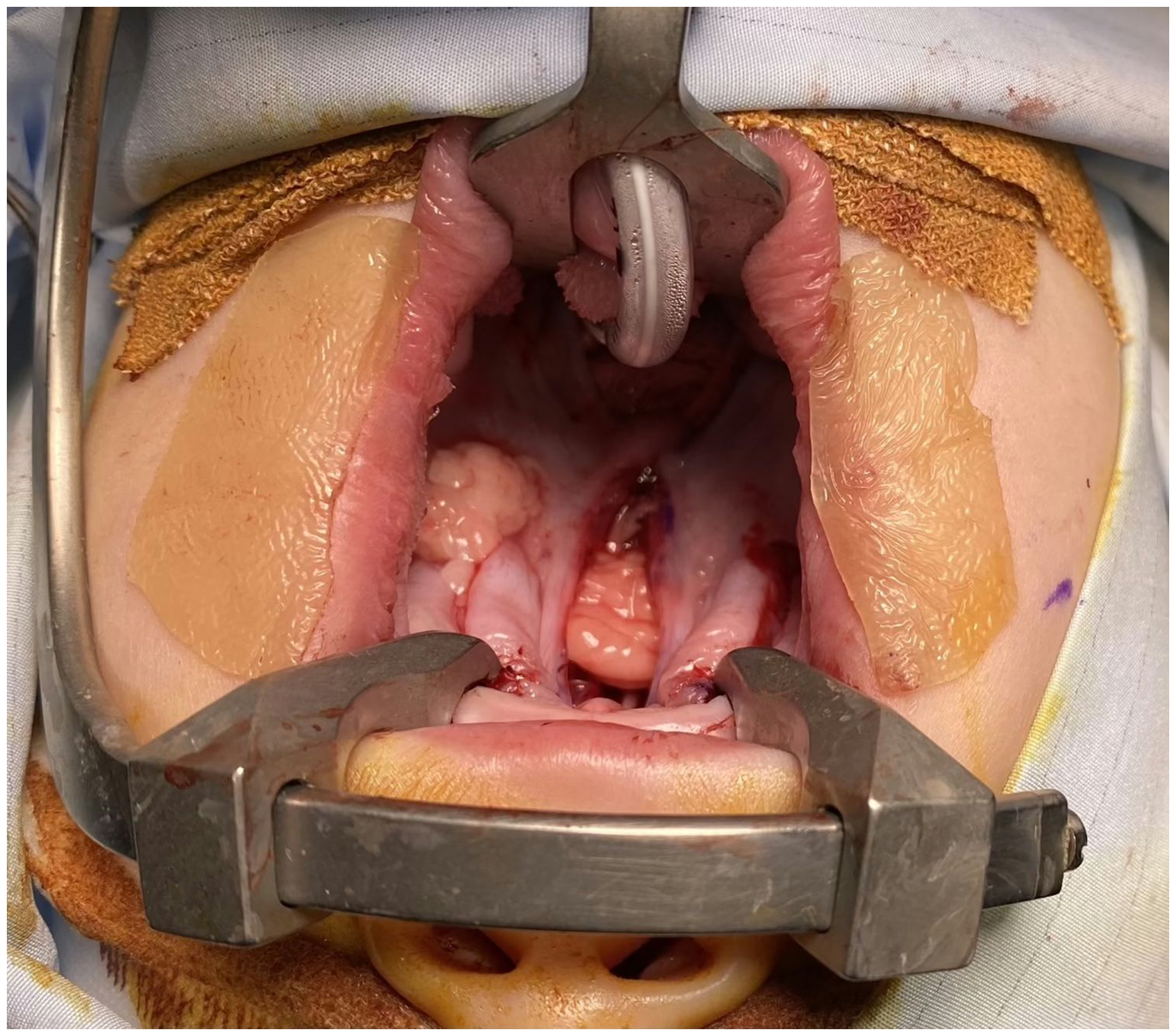
The buccal fat pad flap has been harvested from the left cheek and tunneled beneath the von Langenbeck flap to cross the midline, providing a vascularized interpositional layer between the oral and nasal mucosa while simultaneously obliterating dead space. The oral mucosa will then be sutured together over the top of the flap.
Under general anaesthesia, the patient is prepped and draped in the usual fashion. The patient's neck is extended and the Sommerlad modified mouth gag inserted. The margins of the cleft at the junction of oral and nasal mucosa are marked with ink prior to infiltration with lidocaine and adrenaline. After 10 minutes, allowing for the vasoconstrictive effect of adrenaline, incisions are made at the medial edge of the palate as marked, to the tip of the uvula. Mucoperiosteal flaps are raised with blunt dissection using the Mitchell trimmer. Blunt dissection continues laterally and posteriorly, raising mucous glands to expose the tendon of tensor veli palatini. 3 As described by Sommerlad, the greater palatine vessels are carefully identified and mobilized to facilitate closure of the oral layer and reducing tension. 3 The soft palate is freed from the muscle layer with a combination of sharp and blunt dissection. The nasal mucosa is then mobilized and sutured in the midline. Tensor tenotomy and radical retro-positioning of the velar musculature are performed using the operating microscope for improved visualization of the anatomy and surgeons’ comfort.3,16 The levator palatini muscle layer is sutured in the midline using a monofilament suture, specifically the violet 4-0 PDS*II on a ½ circle round bodied needle. For the nasal and oral layers, the author uses 4-0 Vicryl suture on a conventional cutting needle. A buccal fat pad flap was employed when the surgeon was concerned about a higher risk of fistula formation; either because of width of the cleft, the von Langenbeck flap, or the tightness of the nasal layer closure. A single buccal fat pad flap was generally used, passed posterior to the neurovascular bundle. When there was a very large dead space within the repair, 2 buccal fat pad flaps were employed, with the second flap passed anterior to the neurovascular bundle on the other side. The flaps were secured with one or two 4-0 Vicryl sutures, placed through the distal end of the flap and then in a horizontal mattress fashion through the oral palatal mucosa, as far from the wound edge as practical. Sutures were tied only tight enough to prevent retraction, to reduce the risk of strangulating the fat pad. The vector of suturing was adjusted according to whether the flap needed to be advanced transversely or in a more anterior direction.
Patients with UCLP underwent early hard palate repair using the vomerine flap at the same time as lip repair, as first described by Pichler in 1934 and later popularized by the Oslo cleft team.17,18 Although the approach has its proponents and its detractors, there is evidence to demonstrate that the use of vomerine flap has no adverse effect on maxillary growth in UCLP patients.19,20 Patients with BCLP were treated with either a 1- or 2-stage lip repair, combined with either staged unilateral vomerine flap or a single-stage hard palate repair using less extensive bilateral vomerine flaps.
Classification of Fistulae
The definition of palatal fistulae varies widely in the literature, ranging from small, asymptomatic fistulae to large symptomatic fistulae necessitating surgical repair. 21 To address this inconsistency, Smith et al. introduced the Pittsburgh fistula classification system to standardize the terminology and reduce ambiguity in the reporting of palatal fistulae. 22 In this study, a fistula in the secondary palate following palatoplasty is considered to be an unintended defect as a result of impaired healing.
Statistical Analysis
Variables were statistically analyzed using R (R Core Team, Vienna, Austria) and a specific R package, ROSE: Random Over-Sampling Examples for performing over-sampling. 23 Categorical comparisons were made with Fisher's exact test, and the Wilcoxon signed-rank test was used to assess the association between cleft width and the formation of post-operative fistula. Bayesian logistic regression (brms package, R) was employed to evaluate the associations of lateral releasing incisions and buccal fat pad flaps with the risk of fistula formation. Additionally, Bayesian multivariate model was performed to assess the effects of multiple covariates on fistula risk including sex, diagnosis, year and cleft width. The outcome was modelled with a Bernoulli distribution and a logit link. Weakly informative priors were specified for most coefficients (Normal (0, 1)) and the intercept (Normal (0, 2.5)), while a more informative prior was used for the buccal fat pad flap coefficient (Normal (−1, 0.5)) based on clinical expectations of a protective effect. Four Markov Chain Monte Carlo (MCMC) chains were run with 2000 iterations each, and model convergence was confirmed by a potential scale reduction statistic close to 1 and adequate effective sample sizes. Results are reported as odds ratio (OR) with 95% credible intervals (CrI). To address class imbalance and improve model performance, over-sampling was also performed. A P-value of 0.05 or less was considered significant.
Results
Patients
A total of 277 patients (146 female, 131 male) who underwent cleft palate repair between 2013 and 2025 were included in the study. The majority of the patients had an ICP, accounting for 173 (62%) patients. Seventy-eight (28%) patients had a UCLP, and 26 (9.8%) patients had a BCLP. The range of cleft width treated was 3‒22 mm with a median of 9 mm.
Surgical Technique
As described earlier, all cleft palate repairs were performed using the Sommerlad IVVP technique. 3 Lateral release incisions were performed on 157 (57%) patients and buccal fat pads were utilized in 55 (20%) patients. Fifty-four (19%) patients had both lateral release incisions and buccal fat pad flap. In one case, a buccal fat pad flap was raised without a lateral releasing incision; this is technically more challenging and carries a higher risk of tearing the fascial sheath of the flap. In most cases, cleft palates requiring a buccal fat pad flap have also been of sufficient size or shape to benefit from lateral releasing incisions, which facilitates passage of the flap into the center of the repair.
Outcome
In our study, overall, 21 patients (7.6%) developed post-operative fistula. This group consisted of 13 male and 8 female patients. Four fistulae were located around the incisive foramen (Zone V); 11 were in the main area of the hard palate (Zone IV); 2 were at the junction of the hard and soft palate (Zone III) and 4 cases were in the soft palate. The median cleft width was 9.25 mm (IQR 7.88–12.62) in patients who developed a post-operative fistula and 9.0 mm (IQR 7.5–11.5) in patients who did not. Seventy-one patients did not have cleft width recorded and were excluded from this analysis. There was no significant difference in cleft width between the 2 groups (P = .47; Supplementary figure 1). When stratified by the presence or absence of lateral releasing incisions, this finding remained consistent, with no significant difference in cleft width between cases that developed a fistula and those that did not (Supplementary figure 2).
The fistula rate was 3.7% (2 cases) in patients who had pedicled buccal fat pad flap compared to 8.5% in the group which did not. Although this point estimate suggested a lower fistula rate with the use of buccal fat pad, this difference was not statistically significant (P = 0.39; Figure 2).
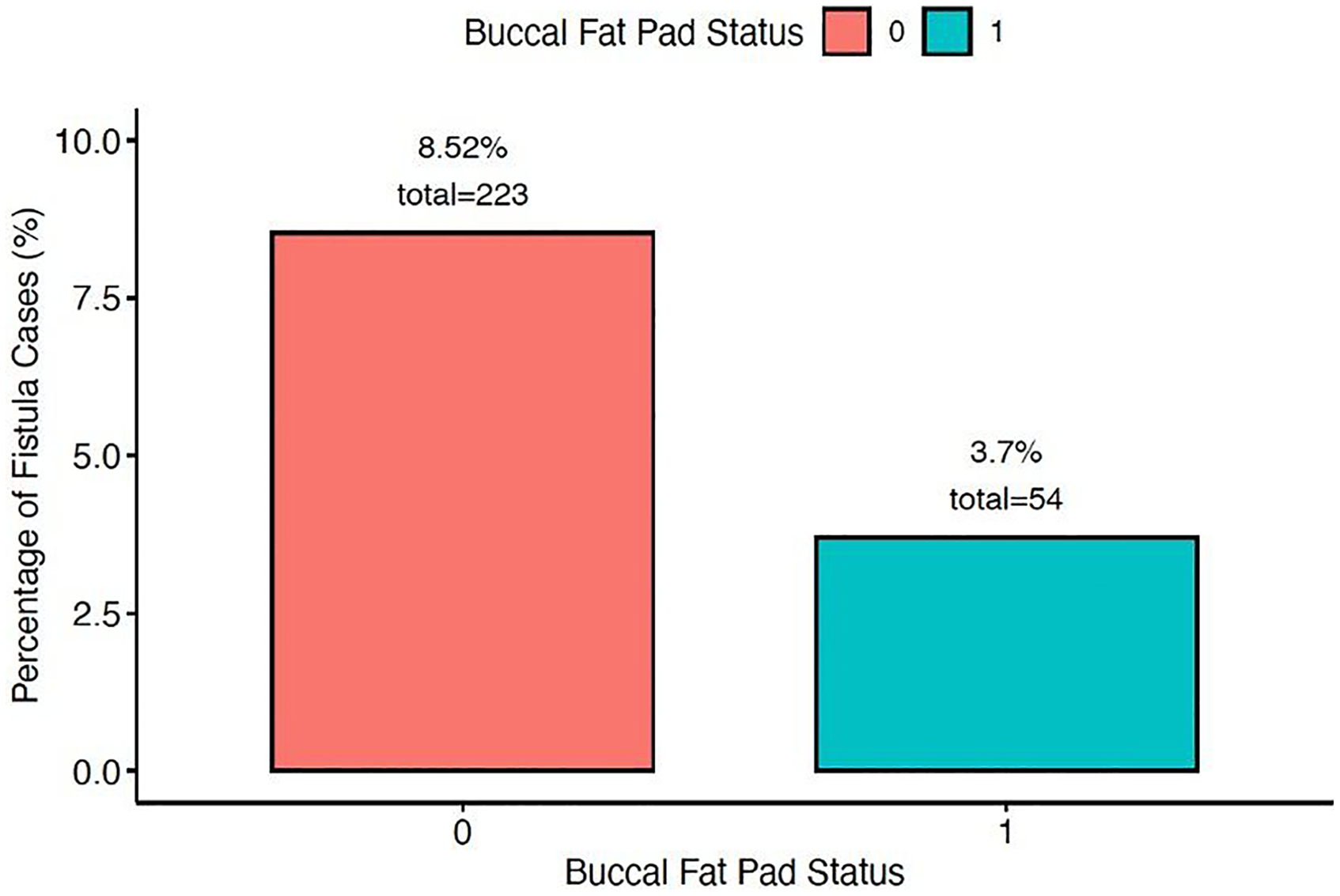
Bar chart showing the impact of buccal fat pad flap on post-operative fistula rates. “0” indicates no buccal fat pad used; “1” indicates utilization of buccal fat pad flap.
A total of 157 patients required lateral releasing incisions and 119 patients did not. This information was missing from one patient's record. Out of these, 10.3% and 4.1% of patients developed a fistula respectively, and no statistical significance was observed (P = 0.07, Figure 3). The trend observed here was a reverse association where patients who subsequently developed a fistula were more likely to require adjunctive lateral releasing incisions during cleft palate repair.
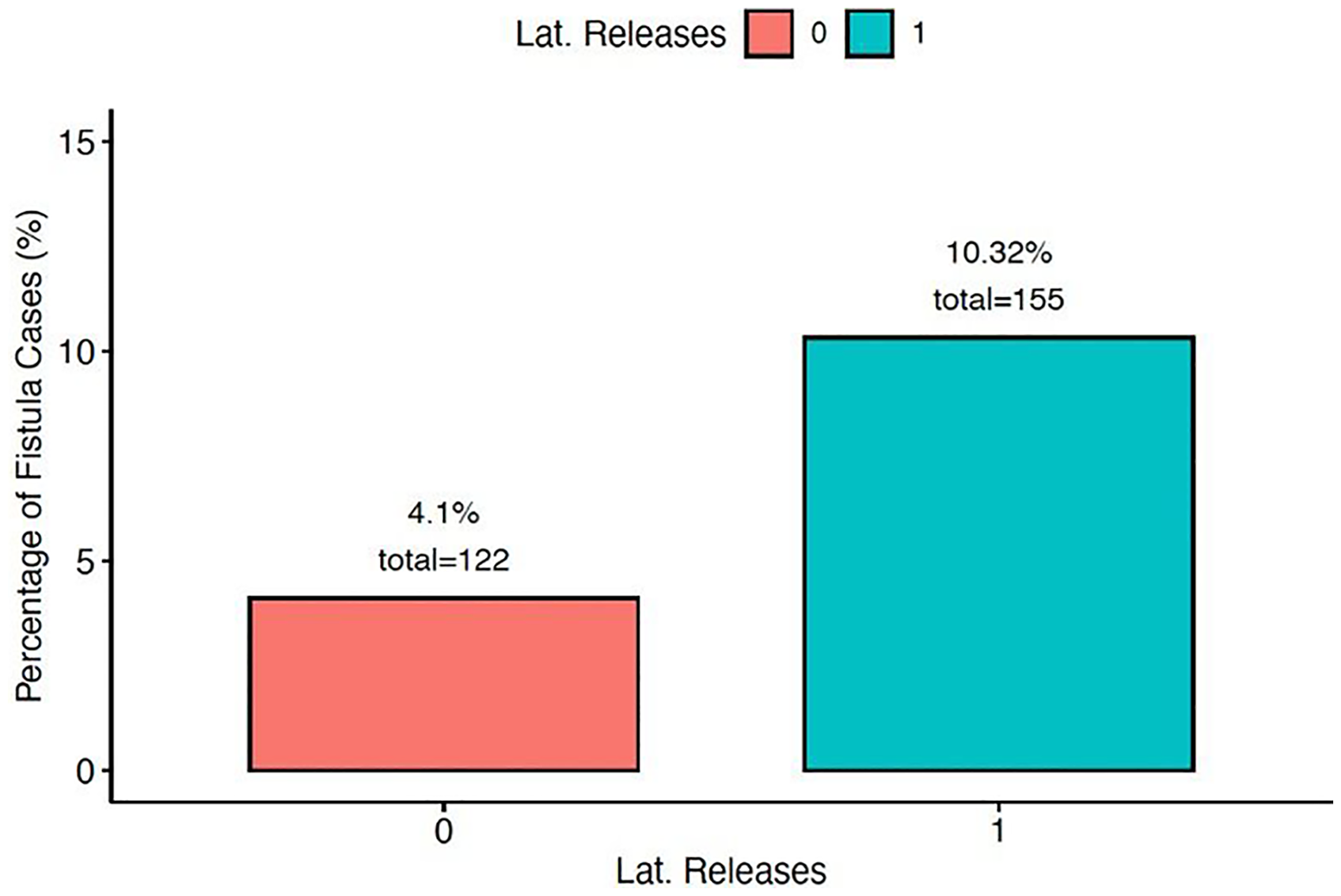
Bar chart showing the association of lateral releasing incisions and post-operative fistula rates. “0” indicates no lateral releasing incisions used; “1” indicates utilization of lateral releasing incisions.
In the standard multivariate logistic regression model, the effect of buccal fat pad flap use on post-operative fistula formation was inconclusive (Figure 4). Lateral releasing incisions were significantly associated with increased risk of fistula, as discussed above. Male sex was also associated with higher fistula risk. All other associations were insignificant, and the results were unchanged after adjusting for cleft width.
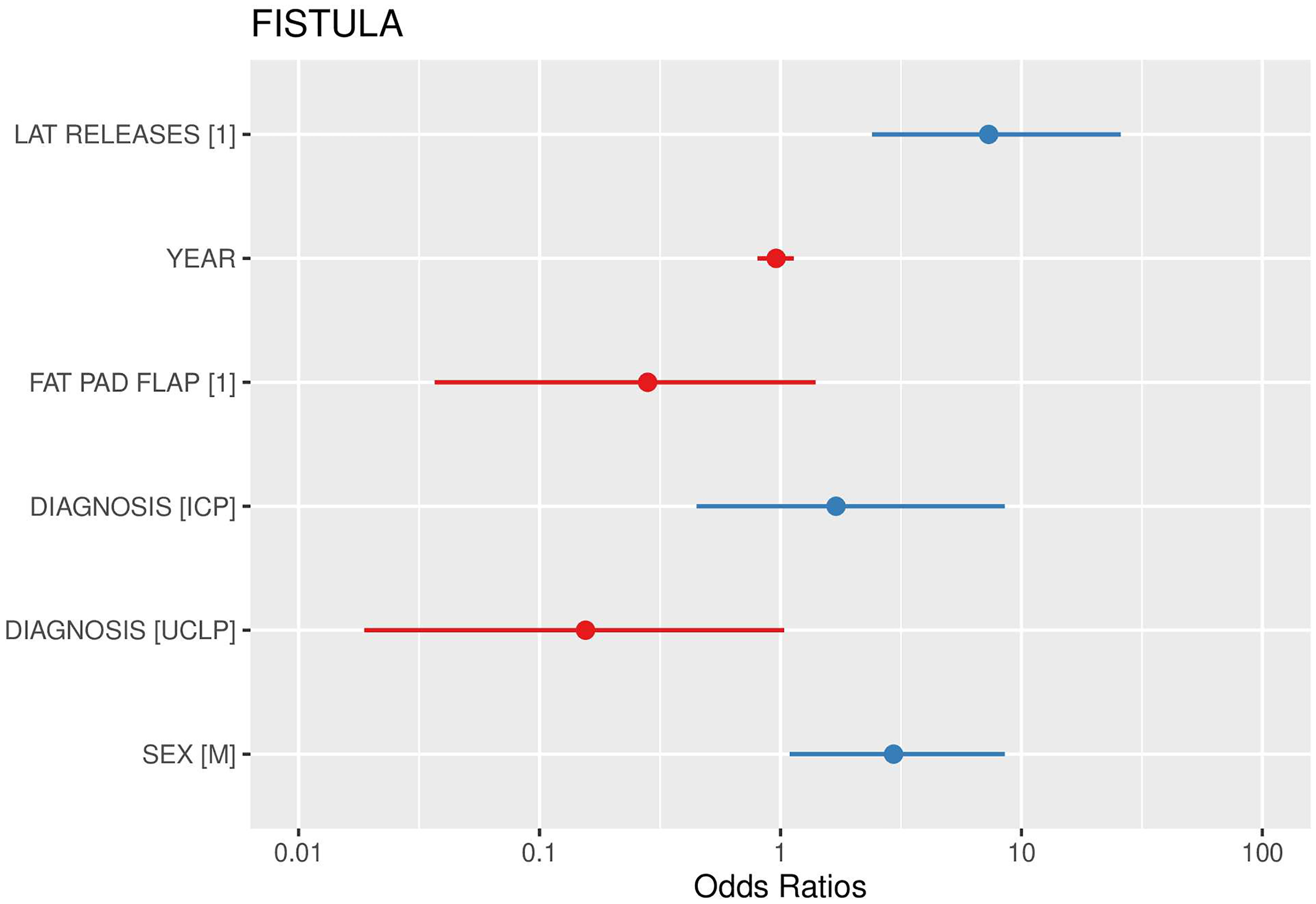
Forest plot from a multivariate logistic regression model assessing risk factors for post-operative fistula formation. The use of buccal fat pad flaps showed an inconclusive association with fistula rate, with wide confidence intervals. Lateral releasing incisions and male sex were associated with increased risk, while all other associations were not significant.
In contrast, Bayesian multivariate logistic regression indicated that buccal fat pad flaps were associated with lower odds of fistula formation by approximately two-thirds (odds ratio [OR] = 0.36; 95% credible interval [CrI]: 0.15–0.82), suggesting a high probability of a protective effect (Figure 5). Lateral releasing incisions were associated with increased odds of fistula formation (OR = 4.1; 95% CrI: 1.1–10.6), although, as noted previously, this likely reflects reverse causation. Male sex tended towards higher odds of fistula (OR = 2.1; 95% CrI: 0.9–5.3). Compared with bilateral cleft lip and palate (BCLP), unilateral cleft lip and palate (UCLP) showed lower odds of fistula (OR = 0.33; 95% CrI: 0.09–1.18), while isolated cleft palate (ICP) showed little difference. When stratified by year of surgery, no meaningful temporal trend was detected (OR = 0.9, 95% CrI includes 1). In a subset analysis, cleft width demonstrated minimal effect on fistula risk (OR 1.05; 95% CrI: 0.88–1.25) (Supplementary figure 3). The model's intercept corresponded to baseline odds of 0.05 (95% CrI: 0.02–0.10), equivalent to a predicted fistula probability of approximately 4.8% in the absence of both surgical interventions. Convergence diagnostics supported the stability and reliability of all parameter estimates.
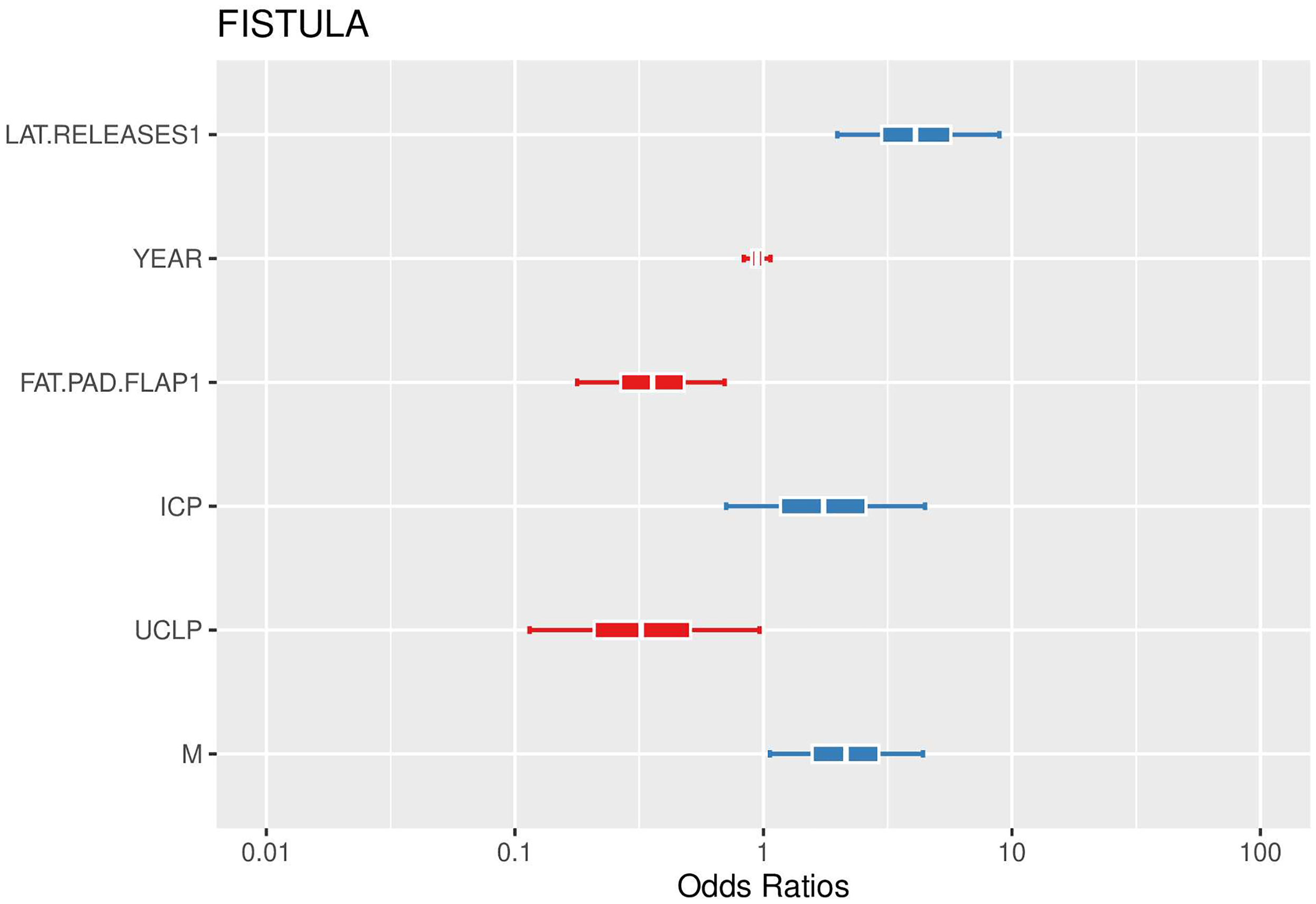
Bayesian multivariate logistic regression model evaluating factors associated with post-operative fistula formation. Buccal fat pad flap use was associated with reduced odds, while lateral releasing incisions and male sex were associated with increased odds of fistula formation. Unilateral cleft lip and palate (UCLP) showed lower odds compared with bilateral cleft lip and palate (BCLP) as the reference, whereas isolated cleft palate (ICP) showed little difference.
The Bayesian logistic regression approach is preferable in this setting as it permits formal incorporation of prior clinical knowledge – specifically, the expectation that buccal fat pad flaps confer a protective effect. This prior information helps stabilize estimates in a relatively small dataset and in situations where the outcome is uncommon (only ∼8% fistula incidence), thereby reducing the risk of unstable or exaggerated effects. Bayesian modelling also produces direct probability statements about parameters (e.g., “there is a high probability that the buccal fat pad flap reduces risk”) rather than relying solely on p-values, which makes the results more intuitive to interpret in a clinical context.
A power calculation was performed to estimate the sample size required to detect a statistically significant difference (P < 0.05) in fistula rates with moderate confidence level of 70% (discriminative ability). Assuming a fistula rate of 8%, a sample size of 456 patients with at least 18 fistula events per intervention group would be needed to achieve adequate power. As mentioned earlier, there were only 2 fistulae in the buccal fat pad group in our study. Considering our observed fistula rate of 3.6% and an average of 10 buccal fat pad flaps performed per year, an additional 31 years of operating would be required to achieve the target number of fistula events.
Adverse Events
No adverse events were observed in patients treated with adjunctive buccal fat pad flaps. Specifically, there were no cases of post-operative bleeding, infection, or return to theatre. One advantage of using a single buccal fat pad flap is that, in the event of future complications such as fistula formation, the contralateral side remains available. In our series, we did not observe any long-term post-operative issues with soft tissue over the tuberosity, which we attribute to careful inset of the flap at the level of the lateral releasing incision. We also did not observe any adverse effect on maxillary growth as a result of using the buccal fat pad flap. Post-operative discomfort was not formally recorded but did not result in prolonged inpatient stay or extended use of post-operative opiates, which were routinely discontinued at 06:00 on the first post-operative morning.
Discussion
The buccal fat pad flap is a versatile flap that has been utilized in a wide variety of oral and maxillary reconstruction including the closure of oroantral communications, closure of defects in the oral cavity and malar augmentation.24–26 This versatility is of particular interest in cleft surgery, given the potential of buccal fat pad flaps in reducing the risk of and treating palatal fistulae.
A palatal fistula is an epithelialized tract that creates an abnormal connection between the oral and nasal cavities. Fistula formation following primary cleft palate repair is a significant complication due to its detrimental impact on speech development and feeding. Air escape through the fistula, or adjacent scarring can result in hypernasality and articulation difficulties, leading to reduced intelligibility. 27 During eating and drinking, the primary concern is nasal regurgitation of food and liquids. Among the risk factors for the development of post-operative fistula formation, increased cleft width has been found to be significantly associated with the incidence of oronasal fistula.28,29 Li et al. reported that cleft widths exceeding 7.5 mm were associated with increased fistula rates, either because of width, quality or curvature of the von Langenbeck flaps. Statistical analysis in our cohort demonstrated no increase in post-operative fistula risk after accounting for cleft width. In 2011, Grobe et al. reported on the use of buccal fat pad flaps in 5 patients with wide clefts, confirming excellent and predictable healing with minimal donor site morbidity. 10 In our case series, the buccal fat pad flap was employed as an adjunct in patients where the senior surgeon was concerned about the potential increased risk of fistulae formation.
Anatomically, the buccal fat pad is located in the buccal space within the cheek, between the superficial musculoaponeurotic system and the buccinator muscle.30,31 It consists of anterior, intermediate and posterior lobes, and 4 projections. 31 The buccal fat pad has excellent vascularity and is supplied by the maxillary, temporal, and transverse facial arteries. 32 A cadaveric study involving 30 buccal fat pad dissections demonstrated a mean surface area of 10.2 cm2 and confirmed the flap's ability to reach routinely across the midline without tension. 31 In practical terms, it is easy to harvest and has minimal morbidity. 33
This study is among the few in the literature to examine the role of the buccal fat pad in preventing palatal fistulae following primary palatoplasty, specifically using the IVVP technique as described by Sommerlad.3,16 Our results demonstrated a numerical reduction of approximately 50% in palatal fistula rates with the adjunctive use of buccal fat pad flaps, although this result was not statistically significant. This observed benefit is consistent with the findings of a series by Horswell and Chou, although their study employed the Furlow double opposing z-plasty technique instead. 34 In their CHOP modified Furlow technique, interpositional buccal fat pad flaps were used during 49 primary palatoplasties. Their results showed, with statistical significance, that standard Furlow palatoplasty was 7.3 times more likely to result in post-operative fistula formation compared to the CHOP modified approach. 34 In a prospective study by Kim et al. which enrolled 65 patients, no oronasal fistulae were observed in patients who underwent closure with an adjunctive buccal fat pad flap, compared to a 6.15% fistula rate (4 patients) in those who did not. 35 In the latter study, a range of surgical techniques was utilized, including V-Y pushback palatoplasty in 78% of cases, as well as Dorrance flap and Furlow's palatoplasty. However, no statistically significant association was observed between the type of surgical technique and the incidence of fistula formation. 35
The potential influence of a learning curve during the study period also warrants consideration. Our dataset encompasses every cleft palate repaired since the senior author began his independent practice in the UK. The temporal distribution of post-operative fistulae over this period is shown in Figure 6. The highest number of fistulae occurred in year 4 of practice (2016), which corresponded to a particularly high volume of cleft repairs performed due to increased birth numbers. An even higher operative volume in 2018 was not associated with a further increase in fistula rate, although case numbers remain too small to glean any statistically significant data. Many studies have attempted to describe the learning curves of various surgical procedures. In cleft surgery, Sakamoto et al. demonstrated that operative efficiency and outcomes stabilize only after a certain case volume, with approximately 40 alveolar bone grafts required to achieve consistency in graft survival and operative time, 36 while in breast cancer surgery, performing 30 to 60 sentinel lymph node biopsies have been recommended for accreditation. 37 They also noted that the number of procedures required to overcome the learning curve is not uniform across surgeons. In contrast to the studies mentioned, Smarius and Bregeum performed a retrospective study in 200 patients and found no statistically significant evidence of a learning curve during the initial years of cleft palate repair. 38 In our study, however, it remains important to acknowledge the possibility that a learning curve may have influenced the data as the timeline overlapped with the introduction of the buccal fat pad flap.
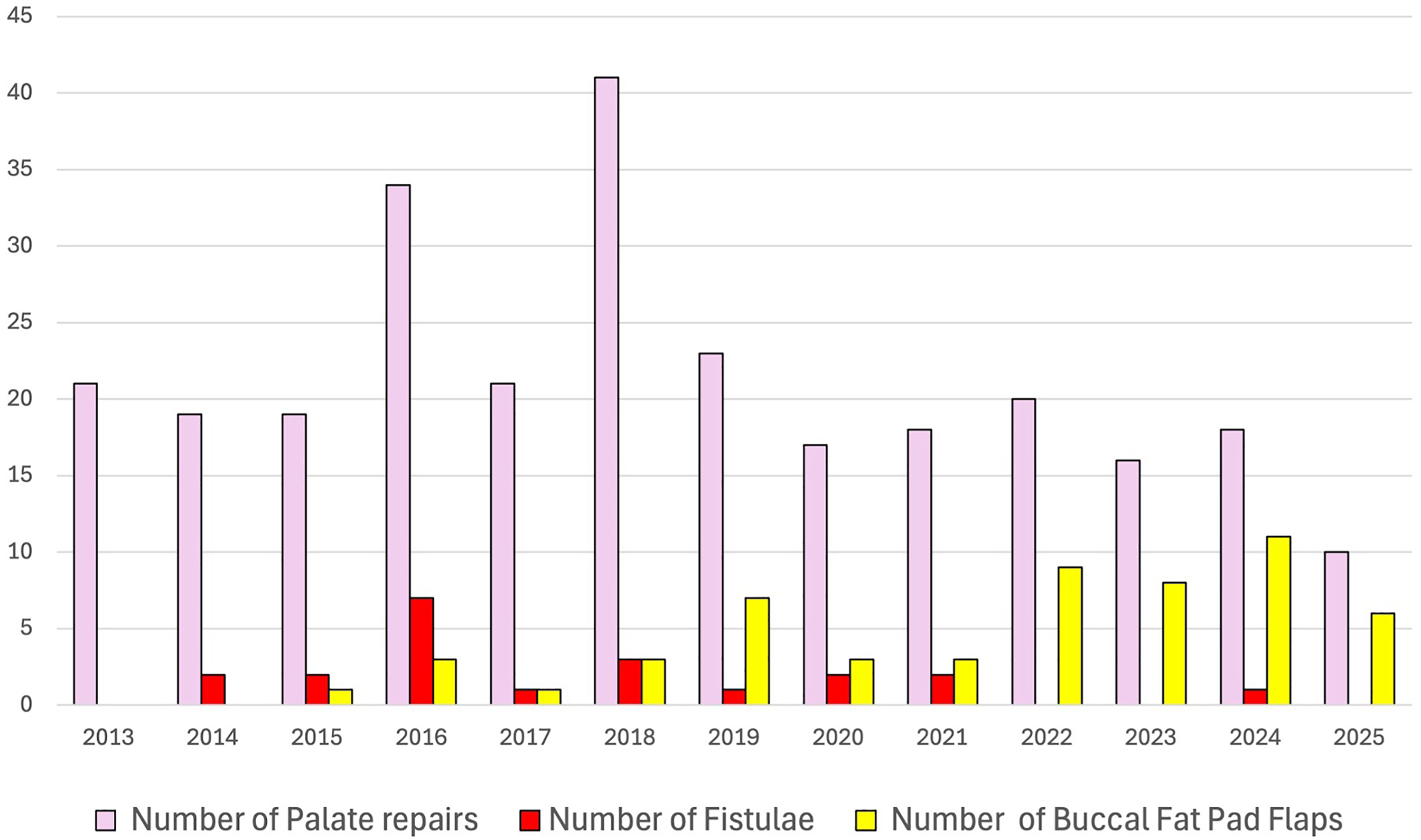
Annual numbers of primary palate repairs and buccal fat pad flaps performed by the senior author from 2013 to 2025 demonstrating trends in surgical volume and post-operative fistulae.
In the current literature, our study represents a high-volume single-surgeon series evaluating the use of pedicled buccal fat pad flaps in primary palatoplasty, comprising 277 consecutive cases performed with the Sommerlad IVVP technique. 3 While Sheppard et al. recently reported a single-surgeon experience involving 212 cleft palate repairs over a 20-year period, the primary outcome was velopharyngeal insufficiency rather oronasal fistula formation. 39 Other published cohorts are smaller in scale; while larger series include multiple surgeons, thereby introducing variability in surgical technique and potentially confounding outcomes. 40 One of the strengths of our study is that it reflects the experience of single surgeon, thereby minimizing variations in either the technique of palate repair or the decision of when to use of buccal fat pad flaps. The size and consistency of our series offers a valuable dataset that contributes to the growing body of evidence supporting the use of pedicled buccal fat pad flaps in reducing the risk of post-operative palatal fistulae.
Conclusion
This study demonstrates that the use of buccal fat pad flaps in primary cleft palate repair is a safe and effective adjunct associated with a reduced incidence of post-operative oronasal fistula. Our results support the selective use of the buccal fat pad flap in patients the surgeon deems are at higher risk of wound breakdown, although we do not suggest it needs to be used in every palate repair.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251399789 - Supplemental material for Does the Buccal Fat Pad Flap Reduce Fistula Rates in Cleft Palate Repair?
Supplemental material, sj-docx-1-cpc-10.1177_10556656251399789 for Does the Buccal Fat Pad Flap Reduce Fistula Rates in Cleft Palate Repair? by Marie S.H. Song and Duncan Atherton in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Approval and Informed Consent Statements
All patient information was de-identified and patient consent was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.