
Abstract
Objective
Examine factors that impact ratings of speech acceptability and parent-reported speech intelligibility using the Intelligibility in Context Scale (ICS).
Design
Prospective, cross-sectional study.
Setting
Public research university.
Patients
Thirty children 4 to 7 years old with a repaired cleft palate.
Variables
Perceptual ratings derived from the Cleft Audit Protocol for Speech-Augmented-Americleft Modification, ICS, percent consonants correct (PCC), age, and sex.
Main Outcome Measure(s)
Factors associated with speech accepatability were assessed using Spearman's rho (ρ) and chi-square tests. Factors that predicted the average score on the ICS were assessed using linear regression.
Results
Hypernasality ratings and PCC were associated with ratings of speech acceptability. There was a moderate, positive correlation between ratings of hypernasality and ratings of speech acceptability [ρ = .51, P < .01]. As hypernasality ratings increased, speech was rated as less acceptable. There was a moderate, negative correlation between PCC and ratings of speech acceptability [ρ = −.67, P < .01]. Children who produced more consonants correct were rated as having more acceptable speech. PCC predicted (P = .010) the average total score on the ICS. As PCC increased, the average score on the ICS also increased. While PCC predicted ICS scores, hypernasality ratings significantly predicted PCC (P = .023) and percent of compensatory misarticulation errors used (P = .001).
Conclusions
Speech-language pathologists need to develop individualized treatment plans that may include (1) recommending speech therapy to increase consonant accuracy that would improve both speech acceptability and intelligibility and (2) identifying children who require surgical intervention to address moderate-to-severe hypernasality, which may be impacting consonant production.
Keywords
Introduction
Speech-language pathologists (SLPs) on cleft teams play a critical role in evaluating speech and making appropriate recommendations for intervention. 1 The team SLP assesses whether individuals would benefit from speech therapy, surgical, or prosthetic management for velopharyngeal insufficiency (VPI), 2 neither, or both. 3 SLPs make these determinations by conducting a comprehensive speech and resonance evaluation. Recommendations for speech therapy are typically based on articulation testing. 4 SLPs may administer standardized assessments, such as the Goldman-Fristoe Test of Articulation–Third Edition (GFTA-3),5,6 to obtain a standard score compared to same age peers or use criterion-referenced measures like percent consonants correct (PCC).7–9 Information from a comprehensive evaluation of speech can be used to develop treatment plans and goals for speech therapy. In addition to articulation assessment, perceptual evaluation is essential for identifying symptoms of VPI, 10 including hypernasality, audible nasal emission, and presence of nonoral compensatory misarticulation errors. 11 Perceptual evaluation results aid SLPs in determining the status of velopharyngeal function. Because SLPs separately evaluate multiple speech characteristics, a composite outcome measure is needed that captures the combined impact of all speech characteristics. 12
The Cleft Audit Protocol for Speech-Augmented-Americleft Modification (CAPS-A-AM) is a commonly used perceptual rating scale used by SLPs in the United States. 13 The CAPS-A-AM scale includes a composite rating of “speech acceptability” to describe the combination of speech sound production characteristics observed. Speech acceptability is rated on a 4-point ordinal scale ranging from “acceptable” to “very unacceptable.” 13 Speech that is rated as “acceptable” is understandable, typical for age, and speech differences do not draw attention away from the message. Factors that make speech “mildly,” “moderately,” or “very unacceptable” include articulation errors that are not appropriate for a person's age, articulatory distortions, the presence of nonoral compensatory misarticulation errors, hypernasality, audible nasal emission, voice concerns, and/or marked hyponasality. 13 Assessing speech acceptability is an important outcome for cleft teams to consider as it can influence how children with cleft palate are perceived by their peers.14,15 Additionally, prior research has shown lower speech acceptability is associated with concerns for anxiety and depression. 16
Another speech outcome that can be used to capture a combination of speech characteristics is speech intelligibility. Speech intelligibility refers to the degree to which a listener accurately understands another person's speech. 17 Several perceptual rating scales include a rating for intelligibility made by the evaluating SLP such as “good, mildly reduced, and moderately to severely reduced.”12,18 However, the evaluating SLP alone does not have insight into how intelligibility varies across different contexts or communication partners, which raises concern for the objectivity of the rating.12,19 Additionally, prior work has found subjective intelligibility estimates made by SLPs differ from transcription-based intelligibility scores by over 12% 20 and SLPs rate speaker intelligibility higher than other medical professionals and naïve listeners. 21
Other areas of research report using Systematic Analysis of Language Transcripts (SALT) software and orthographic transcription to calculate the percentage of intelligible utterances produced.22,23 To perform this type of analysis, the SLP needs to elicit a recorded speech sample and then transcribe the speech sample. This type of analysis for intelligibility is time consuming and is often not feasible in a clinical setting. 24 Use of SALT or transcription of spontaneous speech also does not capture the nuances of how intelligibility may be different across communication partners. Soriano et al found transcription-based intelligibility scores were only weakly correlated with caregiver-reported intelligibility and suggest caregivers consider situational, gestural, and contextual cues. 23 Due to limitations with SALT, transcription-based intelligibility scores, and SLP ratings of intelligibility, the Intelligibility in Context Scale (ICS) is increasingly being used to assess speech intelligibility for children with cleft palate.25,26
The ICS is a measure of functional intelligibility that is completed by parents and/or caregivers. 17 The ICS is a 7-item questionnaire that assesses how well a child is understood across different communication partners using a Likert scale ranging from 1 = never to 5 = always. The ICS is available in a multitude of languages, can quickly be completed in a clinic setting, and aligns with the growing movement to utilize patient (and caregiver) reported outcome measures so individuals are reporting their own functional status. 27 Additionally, growth curves patterns of the ICS have been reported for typically developing English-speaking children ages 2;6 to 9;11 years old that can be used for reference. 28 Prior research using the ICS with 3-year-old children with cleft palate found that speech was most intelligible to the caregiver and least intelligible to strangers. 26 Recent research found that cleft-related speech errors had an effect on intelligibility by immediate and extended family members, acquaintances, friends, and strangers, however speech intelligibility for teachers and caregivers was not impacted by any type of cleft-related speech error. 25 The ICS is an accessible tool that SLPs may consider using to assess speech intelligibility for individuals with cleft conditions.
Speech acceptability and intelligibility are measures that can be easily collected as a part of routine clinical care to inform team treatment planning. The ideal speech outcome for individuals with cleft conditions is for speech to be both acceptable and intelligible. To achieve this goal, it is critical to identify factors—including demographic and speech characteristics—that impact speech acceptability and intelligibility. Understanding the factors that impact ratings of speech acceptability and intelligibility may aid cleft teams with making specific intervention recommendations to improve both outcomes. The purpose of the present study was to assess factors that impact ratings of speech acceptability using the CAPS-A-AM protocol and parent-reported speech intelligibility using the ICS. It was hypothesized that PCC, percent compensatory misarticulation errors, and hypernasality ratings would be correlated with ratings of speech acceptability while PCC and age would be correlated with the average score on the ICS.
Methods
Study Design
A prospective, cross-sectional study was completed to examine factors that impact speech acceptability and caregiver-reported intelligibility in 4- to 7-year-old children with repaired cleft palate. Institutional Review Board approval was obtained from Arizona State University and Barrow Cleft and Craniofacial Center prior to the onset of this study. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): guidelines for reporting cross-sectional studies were followed for this study. 29
Setting
Participants were recruited from a single metropolitan children's hospital in the Southwest United States. All data were collected onsite at the hospital's cleft and craniofacial center by a SLP on the team.
Participants
Thirty consecutive children who met inclusion criteria were recruited from a single metropolitan hospital for this study. Participants were eligible if they had a history of a repaired cleft palate and were between 4 and 7 years old. Participants could be enrolled even if they had a prior history of surgical management to treat VPI. Participants were excluded if (1) they had a diagnosed syndrome per medical record review and/or parent report and (2) if they presented with a sensorineural hearing loss. During recruitment, 2 children were excluded after screening due to having a diagnosed syndrome.
Variables, Data Sources, and Measurement
Demographic and Background Information. Detailed background information was completed by the caregiver that brought the child to the visit and consented for the study. Background information included details about participant demographics and prior medical history.
Speech Evaluation. Participants were seen by a cleft team SLP for completion of a perceptual speech evaluation. The evaluation included an audio- and video-recorded speech sample with (1) 2 to 3 min of elicited conversation using prompts such as, “Tell me about your favorite movie or TV show” and “Tell me about your family”; (2) counting 1 to 10 or 1 to 20 depending on age; (3) a sentence repetition task using the American English Sentence Sample as a part of the CAPS-A-AM. 13 Recordings were collected in an audiology booth with the child, caregiver, and SLP, to mitigate background noise. Video recordings were made with a digital Canon Vixia HF R700 recorder on a tripod with an external lapel Shure BLX14/CVL Microphone. Both video with audio and audio-only recordings were uploaded to a secure site. Audio recordings were saved as .wav files and were used for the perceptual ratings and transcriptions in this study.
Perceptual Ratings. Two SLPs with greater than 10 years of experience assessing resonance rated the speech samples. One SLP was not involved in the clinical care of any of the participants. The other SLP (JLC-W) was involved in the clinical care of approximately half of the participants but rated the samples 4 years after collection. All recordings were indepdendently rated by both raters. The complete audio-recorded speech sample was played that included conversation, counting, and a repetition task. The samples could be listened to as many times as needed to complete perceptual ratings. Both raters had previously attended training on rating using the CAPS-A-AM scale.
The CAPS-A-AM rating scale was used to rate speech acceptability and hypernasality.13,30,31 Speech acceptability was rated on a 4-point ordinal scale: speech is acceptable, speech is mildly unacceptable, speech is moderately unacceptable, and speech is very unacceptable. Hypernasality was rated on a 5-point ordinal scale: none, minimal, mild, moderate, and severe. Reliability for rating perceptual parameters was calculated from the initial ratings. In cases of disagreement, each rater relistened to the sample and independently re-rated the target parameter. The mode across the 4 ratings (2 raters with an initial rating and re-rating) was used for analysis.
Intelligibility in Context Scale. The ICS was given to the participant's caregiver at the time of the perceptual speech evaluations. The ICS is a 7-item questionnaire that a caregiver fills out to rate how their child's speech is understood by different communication partners including parents, immediate family, extended family, friends, acquaintances, teachers, and strangers. 17 For each communication partner, the caregiver rates if the child is always (5), usually (4), sometimes (3), rarely (2), or never (1) understood. The total number is added up across communication partners and then divided by the number of items rated to calculate an average score.
Percent Consonants Correct. The American English Sentence Sample Recording Form used for this study can be found in Supplemental Appendix 1. As a part of the speech evaluation, participants were prompted to imitate the American English Sentence Sample after a model by the SLP. The recorded sentence samples were utilized for phonemic transcription. Accurate productions were denoted with a checkmark and sound errors were transcribed. The speech samples were phonemically transcribed using the International Phonetic Alphabet (IPA 2015) and the extended International Phonetic Alphabet (extIPA 2015) using broad transcription by 2 SLPs (JLC-W and NJS). The samples could be listened to as many times as needed to complete the transcription.
Productions were marked in error if it was denoted to be a substitution, omission, distortion, or addition compared to the target phoneme. Productions that included passive errors such as weak articulation, aspiration, and slight nasalization were not marked as errors. The CAPS-A-AM protocol rates audible nasal emission as a separate perceptual parameter 13 ; therefore, structural audible nasal emission was not marked as an articulation error. During coding, data were marked as missing and excluded from subsequent analyses if a target word or full sentence was not obtained during testing. The PCC was calculated for each participant.8,32 The American English Sentence Sample elicits 24 consonants in initial word position, 20 consonants in medial word position, and 18 consonants in final word position for a total of 62 items. Of the 62 consonants elicited, 8 nasal phonemes are elicited, 18 stops, 19 fricatives, 6 affricates, 4 liquids, 2 glides, 1 glottal, and 3 consonant clusters. PCC was calculated by dividing the number of accurate consonants produced by the total number of consonants produced and then converting the number to a percentage.
Percent of Compensatory Misarticulation Errors Produced. Ananalysis was completed to assess production of compensatory misarticulation errors. Phonemes were classified as a compensatory misarticulation errors if the transcription fell under any of the following categories: pharyngeal articulation, glottal articulation, nasal fricatives, glottal coarticulation, or ingressive errors. 33 The percent of compensatory misarticulation errors used was calculated by dividing the total number (count) of compensatory misarticulation errors produced on the American English Sentence Sample divided by the number of total consonants produced by the participant.34,35
Bias. To reduce bias, the speech samples in this study were gathered prospectively and no secondary data from an electronic health record was used. Additionally, perceptual ratings—speech acceptability, hypernasality—were rated to calculate reliability. Interrater reliability was assessed using a quadratic weighted kappa. Interrater reliability was κ = 0.81 speech acceptability, and κ = .80 for hypernasality. There was substantial agreement across all parameters. For PCC, interrater reliability was calculated using the intraclass correlation coefficient (ICC). Interrater reliability was ICC = .86, indicating excellent agreement. Raters in this study had extensive experience rating and transcribing speech of children with cleft palate. Results may have been different if parameters were rated and/or transcribed by different listeners. Additionally, the raters knew all children in this study had a history of cleft palate, which could have influenced ratings and been different if children without a cleft had also been included.
Bias may still have been present and impacted findings given the measures selected. Some caregiver-reported measures have been shown to have bias in reporting across demographic variables such as the sex of the caregiver responding, child's age, and socioecomonic status. 36 Bias was addressed by using a validated caregiver-reported outcome measure (ICS) that has strong psychometric properties and is widely used in clinical care and research.17,37
Statistical Analysis
Statistical analyses were performed using the statistical software package STATA 17.0 (StataCorp, 2023). Data were summarized using frequency and percentage for categorical variables and mean and standard deviation for continuous measures.
Assessment of Factors Related to Speech Acceptability. The variables examined in this study were selected based on factors previously reported in the literature to be associated with speech sound disorders and speech outcomes. Spearman's rho was used to assess the relationship between the ordinal variable of speech acceptability with other ordinal (hypernasality 38 ) and continuous variables (PCC, 39 percent compensatory misarticulation errors, 25 age 40 ). Spearman's rho values (ρ) were interpreted as a very strong association (ρ ≥ 0.7), moderate association (ρ = .5−.6), fair association (ρ = .3−.4), and a poor association (ρ < .3). 41 A chi-squared test was used to assess the relationship between speech acceptability with the nonordered categorical variable 41 of sex. 42 A Bonferroni correction was applied to control for type I error, resulting in an adjusted alpha level of P = .01.
Assessment of Factors Related to Speech Intelligibility. Linear regression was used to access factors that impacted the total average score on the ICS. The average score on the ICS was the dependent variable and scores ranged from 1.0 to 5.0. Demographic variables assessed included age 43 and sex 42 Speech related variables included ratings of hypernasality, 44 PCC, 43 and percent of compensatory misarticulation errors. 25 Univariate analyses were conducted for all independent variables (age, sex, hypernasality, PCC, and percent compensatory misarticulation errors) with average ICS scores as the dependent variable. The significance level was set at 0.05. Because only one variable had a P-value ≤ 0.05, a multivariate model was not constructed.
Interplay between Hypernasality, PCC, and Compensatory Misarticulation Errors. A secondary analysis was conducted to explore the impact of hypernasality on PCC and the percent of compensatory misarticulation errors used. Univariate linear regression analyses were conducted to examine the associations between hypernasality ratings (independent variable) and PCC (dependent variable), and between hypernasality ratings (independent variable) and the percentage of compensatory misarticulation errors (dependent variable). The significance level was set at .05.
Results
Participants
Most children in this study were female (n = 20; 67%), non-Hispanic (n = 23; 77%), and white (n = 22; 73%). The mean age at the time of evaluation was 5.4 years old (SD = .8) with a range of 4 to 6.7 years. Most children had been referred at some point to speech therapy (n = 23; 77%) and had attended speech therapy (n = 21; 70%). All evaluations were conducted in English. Five children (17%) were exposed to another language at home including Navajo (n = 1; 3%), Spanish (n = 3; 10%), and Tamil (n = 1; 3%). Eleven participants (37%) had previously undergone secondary surgery to treat VPI which included a pharyngeal flap (n = 9), secondary Furlow (n = 1), and one parent reported the child had “revision” of the original cleft palate repair. One participant was adopted at 2 years of age. Most participants (n = 28; 93%) had a history of ear tube placement. Full participant demographic information is provided in Table 1.
Participant Demographics (N = 30).
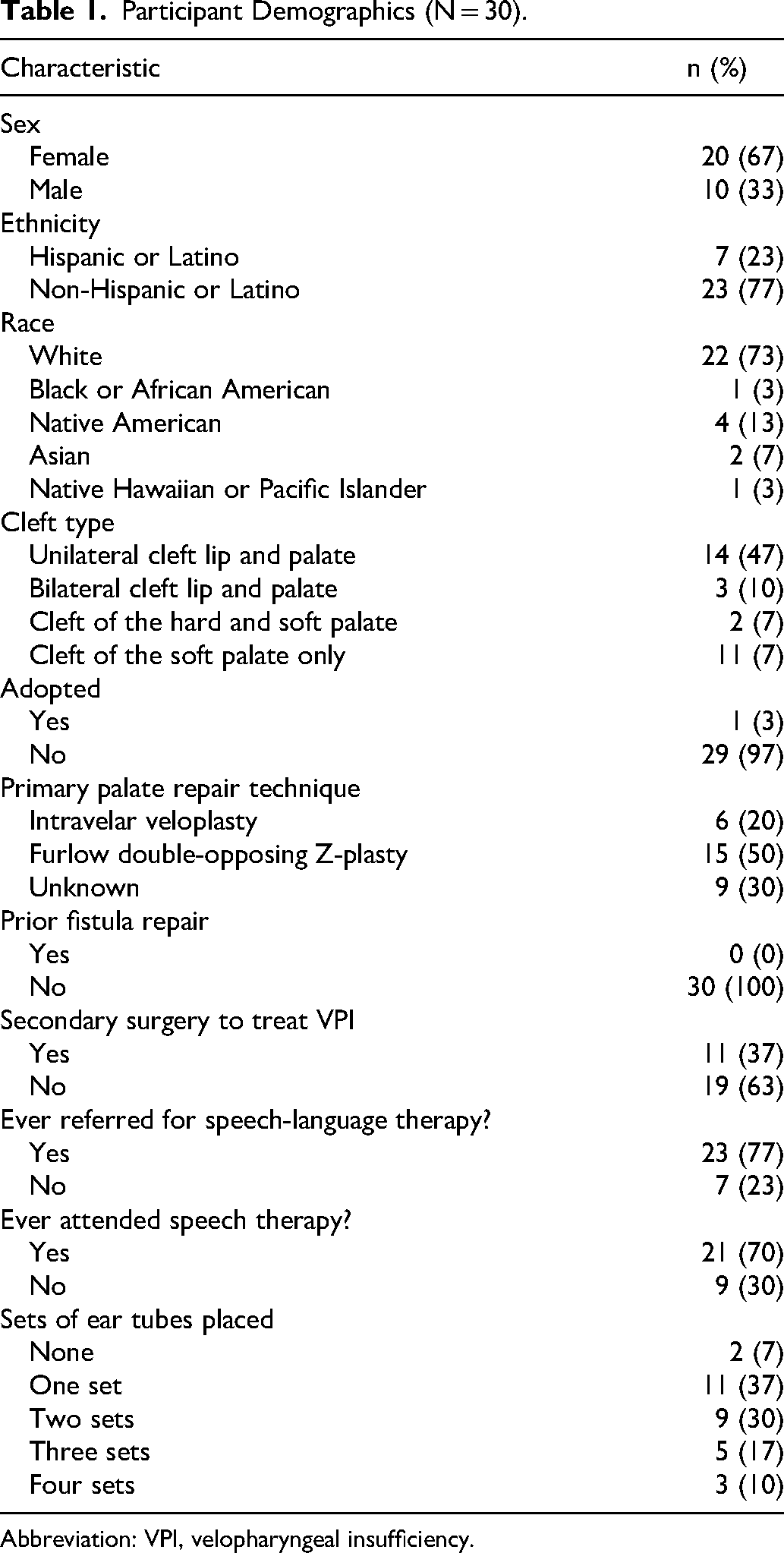
Abbreviation: VPI, velopharyngeal insufficiency.
Descriptive Data
Speech Acceptability. Twelve children (40%) were rated as having acceptable speech, 9 (30%) with mildly unacceptable speech, 6 (20%) as moderately unacceptable and 3 (10%) with very unacceptable speech.
Hypernasality and Audible Nasal Emission. Nine children (30%) had a hypernasality rating of none, 12 (40%) were rated as minimal, 3 (10%) as mild, 4 (13%) as moderate, and 2 (7%) as severe. Most children did not have audible nasal emission (n = 18; 60%). Eight children (27%) were rated as having occasional/seldom audible nasal emission and 4 (13%) with frequent nasal emission.
Percent Consonants Correct (PCC) and Compensatory Misarticulation Errors (CMAs). The mean PCC across the group was 79% (SD = 21) with a range from 22% to 100%. Most children (n = 18; 60%) did not produce any CMAs. Four children (14%) produced 1 CMA; 3 children produced 1 glottal fricative, and 1 child produced 1 glottal stop. One child (3%) produced 2 CMAs including 1 glottal fricative and 1 glottal stop; 1 child (3%) produced 3 glottal fricatives; 1 child (3%) produced 4 CMAs including 3 nasal fricatives and 1 glottal stop. Four children (14%) produced CMAs on ≥10% of consonants produced on the American English Sentence Sample that are described in Table 2.
Description of Children That Produced ≥10% Compensatory Misarticulation Errors.
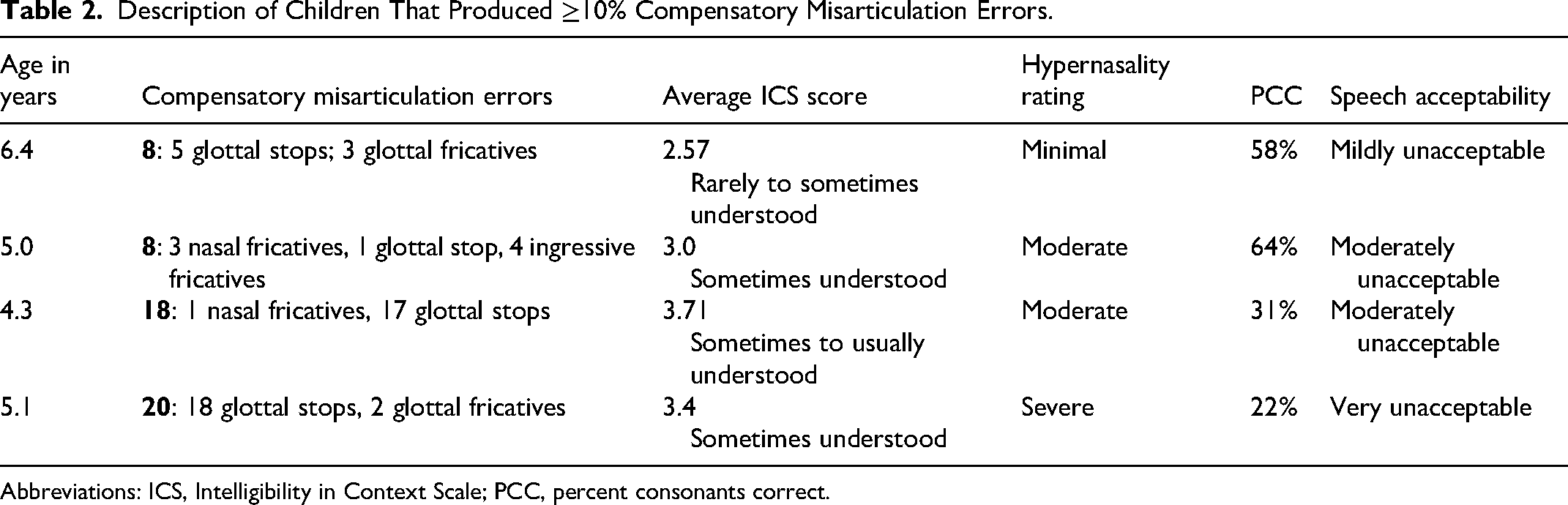
Abbreviations: ICS, Intelligibility in Context Scale; PCC, percent consonants correct.
Intelligibility in Context Scale. The ICS was completed for 86% (n = 26) of participants by their mother and for 13% (n = 4) of participants by their father. The mean average score on the ICS was 3.9 (SD = .7), indicative of speech being “sometimes to usually understood.” Scores ranged from 2.3 (rarely understood) to 5.0 (always understood).
Main Results
Factors Associated with Speech Acceptability. Two variables assessed using Spearman's rho were significantly associated with speech acceptability: hypernasality ratings and PCC. There was a moderate, statistically significant positive correlation between ratings of hypernasality and ratings of speech acceptability [ρ = .51, P < .01]. As hypernasality ratings increased, speech was rated as less acceptable. There was a moderate, statistically significant negative correlation between PCC and ratings of speech acceptability [ρ = −.67, P < .01]. Children who produced more consonants correct were rated as having more acceptable speech. Figure 1 shows the proportion of children with each speech acceptability rating and the mean PCC by group.
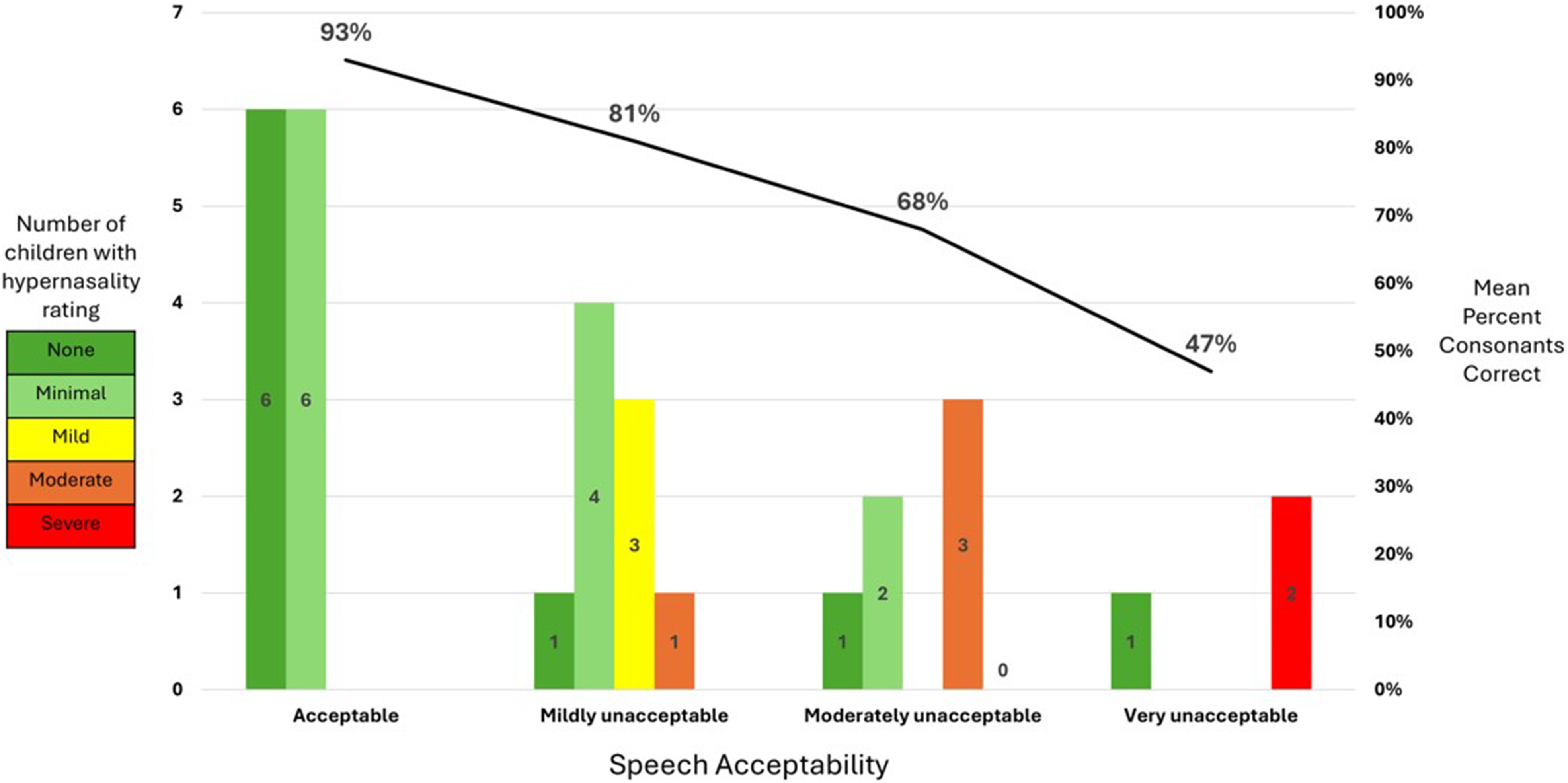
There was a moderate, positive correlation between ratings of hypernasality and ratings of speech acceptability [ρ = 0.51, P < .01]. As hypernasality ratings increased, speech was rated as less acceptable. There was a moderate, negative correlation between percent consonants correct and ratings of speech acceptability [ρ = −0.67, P < .01]. Children who produced more consonants correct were rated as having more acceptable speech.
No other variables assessed were significantly associated with ratings of speech acceptability including: percent CMAs (ρ = .27, P = .16), age (ρ = −.29, P = .12), or sex (P = .18).
Factors That Impacted Speech Intelligibility. One variable predicted the average score on the ICS using linear regression: PCC. As PCC increased, the average score on the ICS also increased (P = .010) as shown in Figure 2. A medium to large effect size was observed (β = .47). Unlike speech acceptability, hypernasality ratings did not predict (P = .721) the average score on the ICS as shown in Figure 3. Age (P = .588), sex (P = .406), and percent of CMAs (P = .094) did not predict the average score on the ICS.
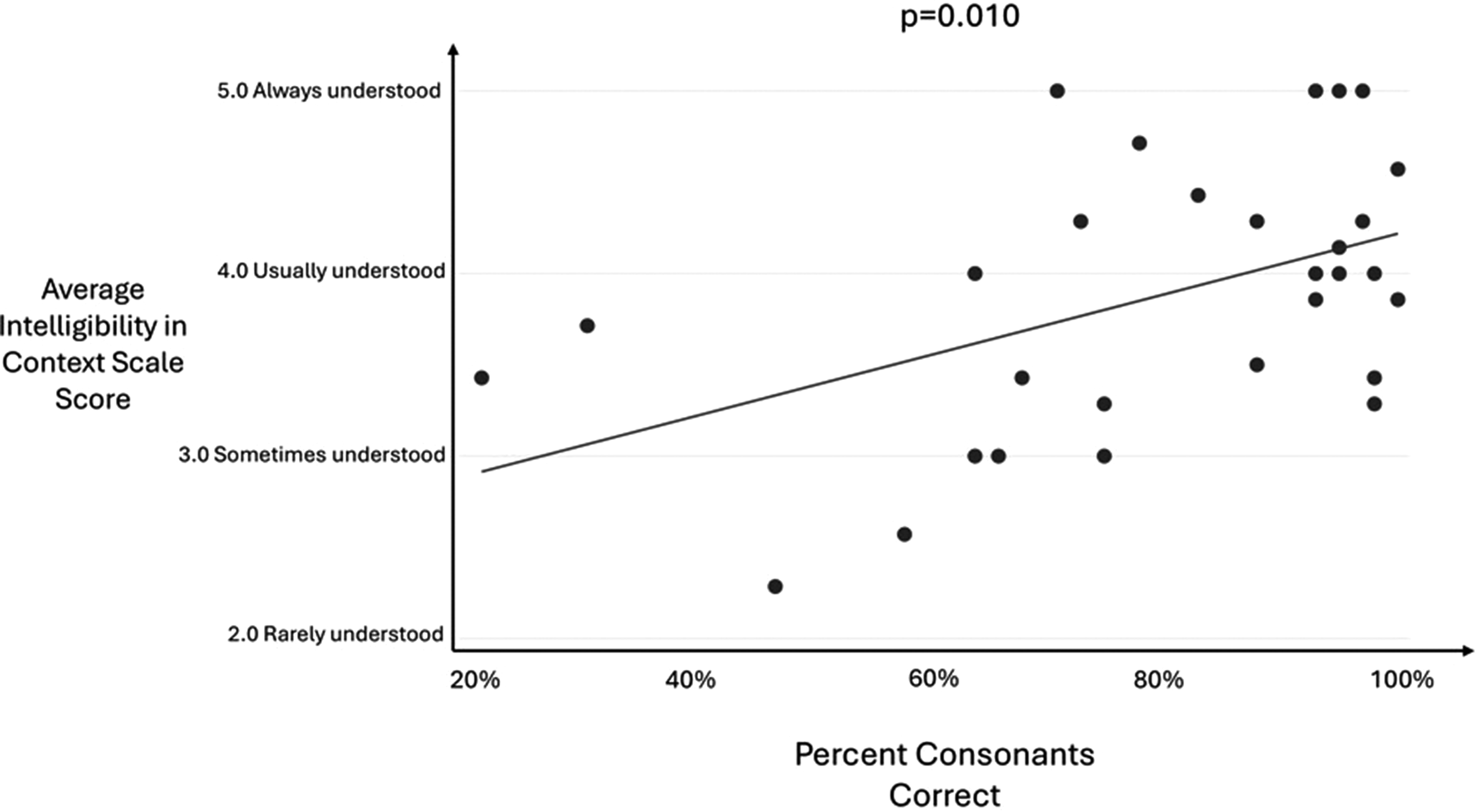
As percent consonants correct increased, the average score on the Intelligibility in Context Scale also increased (P = .010). A medium to large effect size was observed (β = 0.47).
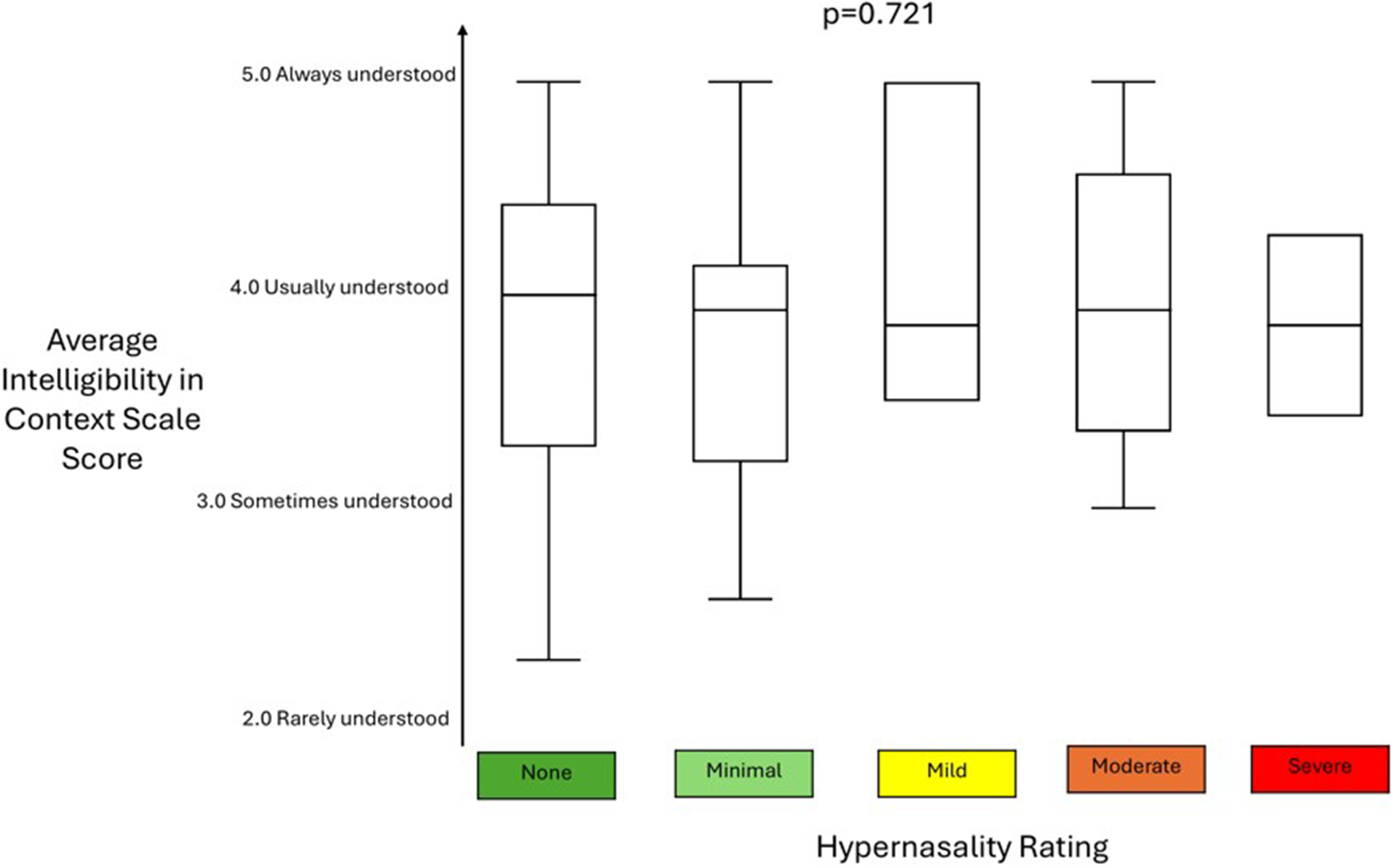
Hypernasality ratings did not predict (P = .721) the average score on the ICS score. The only predictor of speech intelligibility as measured using the ICS was percent consonants correct. Abbreviation: ICS, Intelligibility in Context Scale.
Interplay Between Hypernasality, PCC, and CMAs. Univariate linear regression analyses found hypernasality ratings significantly predicted PCC (P = .023). Hypernasality ratings also predicted percent of CMAs used (P = .001). Total PCC decreased when hypernasality ratings worsened to moderate and severe; an increased use of CMAs was also observed for hypernasality ratings of moderate and severe. Figure 4 shows the mean total PCC and the percent CMAs by hypernasality rating.
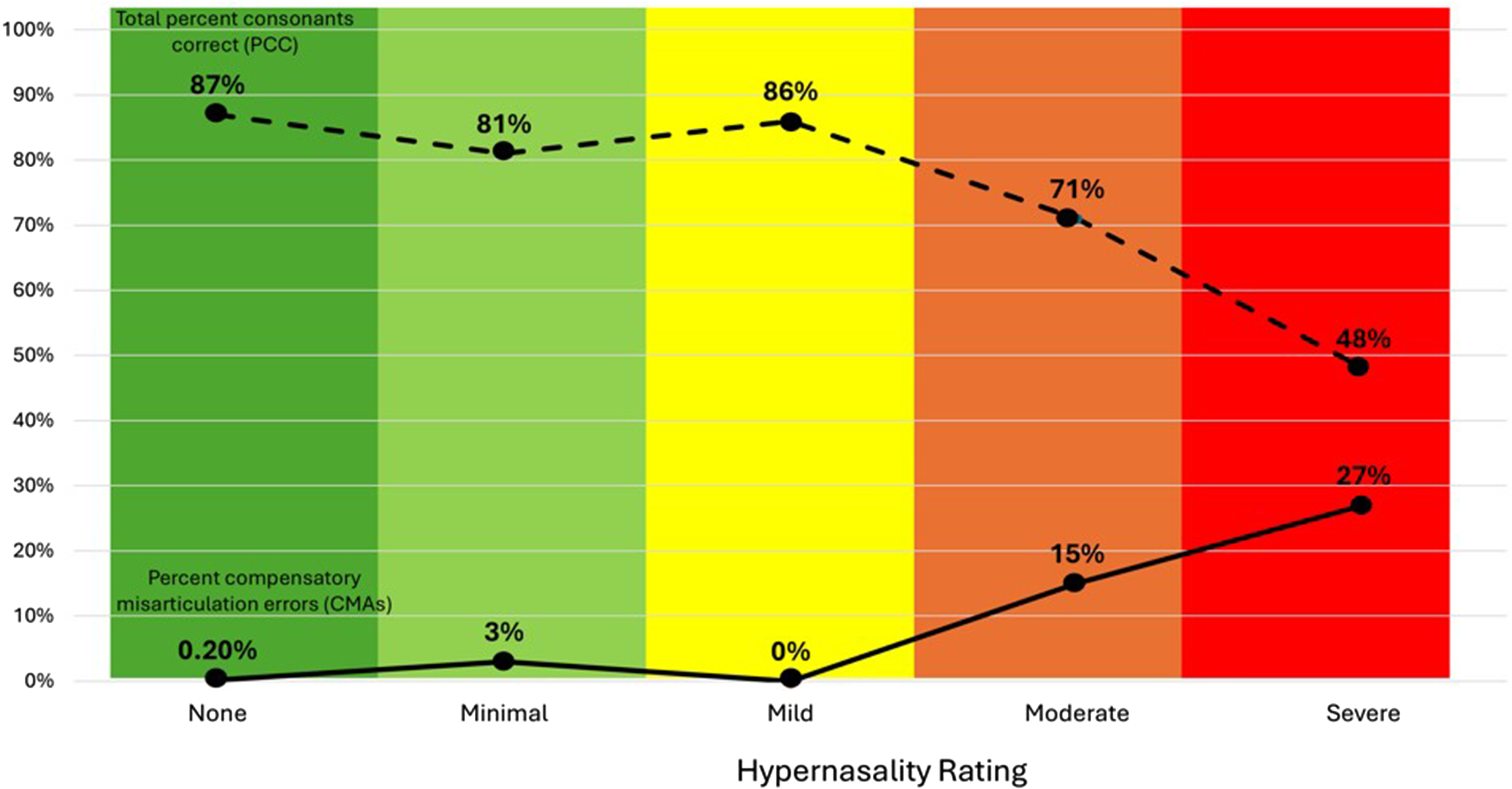
Hypernasality ratings significantly predicted total PCC (P = .023) as shown by the dashed line. Hypernasality ratings also predicted percent of CMAs used (P = .001) as shown by the solid line. Total PCC notably decreased when hypernasality severity worsened to moderate and severe and an increased use of CMAs was observed. Abbreviation: CMAs, compensatory misarticulation errors; PCC, percent consonants correct.
Discussion
The present study examined factors that impact ratings of speech acceptability as rated by SLPs and speech intelligibility as reported by caregivers using the ICS. Demographic variables including age and sex were not associated with ratings of speech acceptability or intelligibility. Speech acceptability was impacted by 2 factors: hypernasality and PCC. Children with hypernasality ratings of mild, moderate, and severe were all rated as having unacceptable speech while children with ratings of no or minimal hypernasality and a higher PCC were rated as having acceptable speech. Factors that contributed to ratings of speech intelligibility were more complex. Hypernasality ratings significantly predicted PCC and percent of compensatory misarticulation errors produced; however, only PCC significantly predicted the average total score on the ICS. As PCC increased, the average score on the ICS also increased. These findings suggest that SLPs need to consistently assess both consonant accuracy and hypernasality in clinical care and outcomes research due to the impact on both speech acceptability and intelligibility.
Speech Acceptability
Speech acceptability is rated by the SLP and reflects if speech is typical for a child's age, the presence of any resonance deviations, and if speech differences draw attention away from the message of the speaker. 13 In the present study, speech acceptability was impacted by both hypernasality and PCC, supporting the validity of the rating. Age was not associated with ratings of speech acceptability, as the rater is taking the child's age into consideration when assigning the rating by definition of the scale. Interestingly, all children with mild hypernasality were rated as having mildly unacceptable speech and 75% of children with moderate hypernasality were rated as moderately unacceptable. All children with severe hypernasality were rated as having very unacceptable speech. This finding suggests that raters using the CAPS-A-AM rating scales may be internally aligning hypernasality severity with speech acceptability categories—either consciously or unconsciously.
If SLPs are aligning speech acceptability and hypernasality ratings, not all children with a cleft may obtain a rating of “acceptable speech.” For example, many children with hypernasality who undergo surgical management of VPI see an improvement of 2 rating points, for example improving from severe (hypernasality = 4) to mild hypernasality (hypernasality = 2). 45 In these cases, a child could be rated as having “mildly unacceptable” speech due to the residual hypernasality; however, the family may not desire further surgical intervention, or the team does not feel they can offer a procedure that would provide further improvement. It may be difficult for patients and families to repeatedly hear during speech and team visits that “unacceptable speech” has been noted for several years without any recommendations for improvement. Children may have minor speech differences that impact ratings of speech acceptability, however, they might still be intelligible to many communication partners. Cleft teams and researchers may consider using speech acceptability as an outcome measure in research studies or as a part of quality improvement initiatives to assess the impact of surgical management on speech outcomes, such as timing of primary palate repair46,47 or outcomes after VPI surgery.
Speech Intelligibility
Prior work has found that a child's age is the main factor for interpreting ICS scores for typically developing children 28 ; however, age was not a significant predictor of speech intelligibility in the present study. In the present study, PCC predicted scores on the ICS, suggesting that intelligibility is more impacted by speech sound production than age for children with cleft palate. This finding suggests that successful speech therapy to improve consonant accuracy 48 may increase both speech intelligibility and speech acceptability and most children with a cleft palate may benefit from speech therapy services during preschool and early school years.49–53
Prior work has found that up to 70% of children with a repaired cleft palate attend speech therapy to address consonant production. 54 Findings from the present study align with prior research, with 77% of children having been referred to speech therapy and 70% having attended speech therapy. While multiple studies have identified that many children with cleft palate attend speech therapy, assessment of articulation and speech sound production is only completed by some evaluating cleft team SLPs. 10 It is concerning that some cleft team SLPs are not assessing articulation given recent work that has shown that speech therapy was effective at increasing PCC and eliminating compensatory misarticulation errors which subsequently increased both speech intelligibility using the ICS and speech acceptability. 48
SLPs on cleft teams who do not assess articulation should consider updating clinical protocols to include assessment of articulation to make appropriate recommendations for speech therapy. Assessing both perceptual parameters and articulation aligns with the American Cleft Palate Craniofacial Association Parameters of Care. 1 The ICS may easilty be integrated into clinical protocols so SLPs can compare ICS scores to established normative data for comparison, to support recommendations for intervention, and track progress in speech therapy. 28
Although PCC was the only predictor of the average ICS score in this study, the relationship between hypernasality, PCC and compensatory misarticulation errors suggest there may be a “downstream” effect of hypernasality on speech intelligibility. Hosseinabad et al 55 examined factors impacting speech intelligibility for 100 school-aged children with cleft palate using the CAPS-A-AM protocol. In their study, they dichotomized speech sound production errors as “present” or “absent” for use of anterior oral cleft speech characteristics and posterior oral cleft speech characteristics. Neither of these variables predicted speech intelligibility ratings, however, they did find that increased hypernasality and need for speech therapy were related to speech intelligibility. Hosseinabad et al 39 concluded that there is a complex interplay of factors that contribute to speech difficulties for children with cleft palate. The present study also found the relationship between speech intelligibility, hypernasality, PCC, and use of compensatory misarticulation errors to be complex.
In the present study, ratings of hypernasality predicted both PCC and percent of compensatory misarticulation errors used. Children with moderate and severe hypernasality in particular produced a lower PCC and more compensatory misarticulation errors. This finding aligns with prior research that hypernasality can impact production of high-pressure consonants and is related with a higher use of compensatory misarticulation errors.7,33,56 The presence of moderte to severe hypernasality and higher use of compensatory misarticulation errors appears to impact the total number of consonants accurately produced, thereby reducing total PCC. Chee-Williams et al 35 found that use of compensatory misarticulation errors significantly decreased in patients who had resolved hypernasality following VPI surgery but did not decrease in patients with persistent hypernasality postoperatively. With successful treatment of VPI, children may more readily remediate compensatory misarticulation errors 35 which may increase consonant accuracy and subsequently increase speech intelligibility and speech acceptability.
Clinical Implications and Future Directions
Findings from the present study support recommendations made by the American Cleft Palate Craniofacial Association Parameters of Care that SLPs should assess consonant production to make recommendations for speech therapy to increase consonant accuracy and perform perceptual evaluation to assess velopharyngeal function. Asessment of consonant accuracy and perceptual parameters should be reported separately in clinical reporting and reported in speech outcomes research. 57 Future research is needed with input from people with cleft conditions and their caregivers on which composite outcome(s), speech acceptability and/or intelligibility, they feel would be most valuable to discuss during speech evaluations and cleft team visits. Future research should also assess what measures SLPs and surgeons find most useful to drive treatment planning and monitor progress.
Limitations
Participants in the present study were recruited from a single cleft-team in one region of the United States, which may limit generalization of findings. This study also included children with a variety of surgical histories, Veau cleft palate types, and linguistic backgrounds so there was not homogeny in the study sample; however, the present sample was reflective of children that are seen by a cleft team for assessment. Additional multisite research is needed to assess factors that impact speech acceptability and intelligibility across a larger sample size and geographical area,58,59 as a larger sample size may reveal demographic characteristics and other speech characteristics such as audible nasal emission that may impact speech acceptability and intelligibility that were not captured in this study.
A care-giver reported measure was used in the present study to assess speech intelligibility. Findings from the present study may not generalize to other measures of speech intelligibility such use of single-word intelligibility tests60,61 or SLP ratings of speech understandability as described in the universal parameters for reporting speech outcomes in individuals with cleft palate. 57
Conclusions
In the present study, speech acceptability ratings were impacted by hypernasality and PCC while speech intelligibility was impacted by PCC; however, children with moderate and severe hypernasal resonance had lower PCC scores and used more nonoral compensatory misarticulation errors. Speech-language pathologists on cleft teams need to assess articulation as a part of the clinical evaluation to make appropriate recommendationsfor speech therapy to increase consonant accuracy. Increasing consonant accuracy may improve both speech acceptability and intelligibility. Cleft teams also need to identify children who require surgical intervention to address moderate to severe hypernasality, which may be impacting consonant production.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251400868 - Supplemental material for Examining Factors That Impact Speech Acceptability and Intelligibility in 4- to 7-Year-Old Children With Cleft Palate
Supplemental material, sj-docx-1-cpc-10.1177_10556656251400868 for Examining Factors That Impact Speech Acceptability and Intelligibility in 4- to 7-Year-Old Children With Cleft Palate by Jessica L. Chee-Williams, Julie Liss, Kelly Nett Cordero and Nancy J. Scherer in The Cleft Palate Craniofacial Journal
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Dental and Craniofacial Research (grant number 3U01DE029750, DE026252).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.