
Abstract
Objective
To identify the challenges facing comprehensive cleft care in Africa and to propose solutions to some of these challenges
Design
A virtual focus group discussion (FGD) was conducted involving 10 cleft care providers from across the African continent. Thematic analysis was used to analyze the collected data.
Setting
Participants in the FGD were experienced cleft care providers from across Africa including North Africa, Southern Africa, East Africa, West Africa, Central Africa and a representative of Francophone West Africa.
Participants
Ten experienced cleft care providers from across the African continent, who were selected using a purposive sampling technique, based on their specialty and experience in cleft care.
Main outcome measures
Challenges facing comprehensive cleft care in Africa were identified and solutions proffered to some of these challenges.
Results
The main challenges and solutions were categorized under patients’ factors, clinicians’ factors and institutional/other factors. Poverty, low level of awareness, insufficient manpower and poor healthcare systems were some of the major recurring challenges. Other unique challenges identified were language barriers affecting access to cleftcare training in Francophone Africa and the brain drain syndrome, which had resulted in the migration of cleftcare manpower from the continent. Improved patient support systems, enhanced manpower training and motivation and improved healthcare systems were some of the solutions suggested
Conclusion
The main challenges identified were shortage of required manpower and institutional and policy challenges, while the proposed solutions ranged from enhanced manpower training and motivation to improved healthcare systems.
Introduction
Africa is the second largest continent by population and size, with 54 countries and a population of about 1.5 billion people, representing 18.2% of the world's population. It is also the most rapidly growing continent in the world and its growth stands to influence the world system. 1 The African continent faces several challenges, including a high percentage of underserved rural communities, limited access to healthcare and poor infrastructural development among others. 2 Cleft care in Africa is not immune from these challenges.
The prevalence of orofacial clefts in Africa has been reported as 0.57/1000 live births, which is quite low when compared to other continents, such as Asia and Europe. 3 However, these low values may be associated with limited data on out of hospital births and births in rural communities which are rarely captured with the hospital data. 4
Comprehensive cleft care is currently the gold standard for cleft-care worldwide, and its provision across the African continent may play a huge role in significantly improving the quality of cleft care across the continent. There are currently several challenges facing the status of comprehensive cleft care in Africa and although many studies have reviewed these challenges, they have mostly been limited in terms of their spread, capturing only a few countries or regions in the continent.4–12 In addition, very few of these studies have focused on proposed solutions to the identified problems.13–15 However, there is a need for broader studies conducted across the entire continent, which capture the challenges facing cleft care as well as proffer possible solutions to these challenges. This is important, bearing in mind the peculiarities of the African continent, particularly with respect to limited healthcare manpower and infrastructure as well as the large, underserved populations in the continent.2 A broader approach would guide policy making on a continental level for African health organizations in planning for improved cleft care delivery in the continent. This would also be of benefit to national and international funding agencies which support cleftcare in the continent.
Thus, the aim of this study was to assess the challenges facing comprehensive cleft care in Africa and to propose workable solutions to these challenges using a qualitative approach, by capturing the views of cleft care professionals from across the continent.
Methodology
This was a qualitative study and data collection was via a focus group discussion (FGD). Ethical approval for the study was obtained from the Institutional Review Board of the Lagos University Teaching Hospital with approval number ADM/DSCST/HREC/APP/6568. The panel for the FGD included one major cleft care provider from each of the five major regions in the continent: North Africa (Egypt), Southern Africa (South Africa), East Africa (Ethiopia), West Africa (Ghana, Nigeria), Central Africa (Democratic Republic of Congo), a representative of Francophone West Africa (Senegal), a cleft genetic expert with extensive experience in genetic studies involving African populations, and the Vice President of a cleft- focused non-governmental organization (NGO) with significant experience in supporting cleft care in the continent. The participants included two plastic surgeons, a pediatrician, an oral and maxillofacial surgeon, an orthodontist, a cleft genetics expert and a medical practitioner who was a cleft team coordinator. The moderator for the FGD was an orthodontist who had been involved in cleft care in Africa for over 15years. Thus, a total of 10 people took part in the FGD, comprising eight participants, one moderator and a transcriber. The role of the transcriber was to take down notes and key points during the FGD.
Purposive sampling was used to select each participant for the FGD, ensuring that each region of Africa was represented by an experienced cleft care professional who was currently involved in providing comprehensive cleft care. Each selected participant was contacted via email and WhatsApp messages. All the contacted participants indicated their interest in participating in the study. Informed consent was obtained from each participant of the study prior to commencement, and they were informed that participation in the FGD was voluntary and that they could withdraw at any stage of the discussion.
The FGD took place virtually using the Zoom platform and was recorded. The total duration of the meeting was 2 h 15min. A discussion guide was developed for the FGD based on existing research (Supplemental Table 1). The questions were semi-structured but not limited to those that were outlined in the guide. The questions focused mainly on identifying the challenges facing comprehensive cleft care in Africa and proposing workable solutions to these challenges. These were broadly discussed under three main headings namely patients’ factors, clinician factors and other factors, including institutional factors as highlighted in the Discussion guide.
The qualitative data were analyzed using a deductive thematic analysis approach.16 The transcripts were read and relevant portions identified, labelled and organized into codes, subthemes and main themes under each category. Each theme was carefully reviewed and refined to ensure it accurately represented the data and had clear boundaries from other themes. The final themes were presented with direct quotes from participants to support and illustrate each theme and subtheme. The FGD was carried out by IGI.
Although the thematic analysis was deductively guided by pre-existing concepts from the cleft care literature, the study was grounded in an interpretivist paradigm. 17 This allowed the analytical framework to structure coding while still prioritizing participants’ subjective meanings and permitting the emergence of new insights.
Researcher reflexivity was also taken into consideration during the FGD, as well as data analysis. As clinicians involved in cleft care, the authors recognized that their clinical experience could influence how participants’ views on challenges facing cleft care in Africa were interpreted. Thus, to reduce bias, a brief reflexive journal was used as well as a neutral questioning approach during the FGD. In addition to this, the reflections were reviewed during analysis, and the identified themes were reviewed with the co-researcher PB, who was not part of the FGD, but served as a peer reviewer, to ensure the emerging themes reflected participants’ perspectives, rather than the authors’ assumptions.
Results
The following major themes and subthemes were identified under the following broad areas.
Patient Factors in Comprehensive Cleft Care Challenge
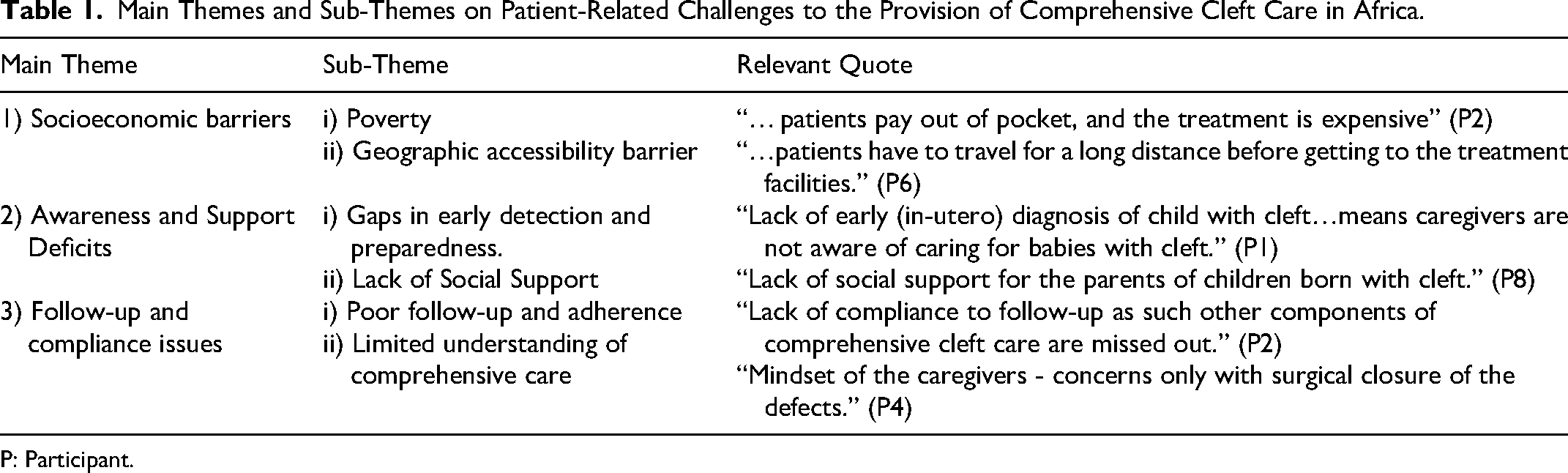
Thematic analysis of patient-related challenges to the provision of comprehensive cleft care in Africa revealed three main themes and six subthemes (Table 1).
Main Themes and Sub-Themes on Patient-Related Challenges to the Provision of Comprehensive Cleft Care in Africa.
P: Participant.
Theme 1: Socioeconomic Barriers
This theme explores the financial and access-related obstacles that patients face in receiving comprehensive cleft care. It delves into how poverty affects patients’ ability to afford treatment and how geographical distances and lack of transportation infrastructure hinder access to cleft care facilities, particularly for those in rural areas.
Poverty
Poverty emerged as a critical barrier to comprehensive cleft care in Africa. Participants consistently highlighted the financial constraints faced by patients, hindering access to and affordability of cleft care services. As Participant 2 noted: “Lack of funds… patients pay out of pocket, and the treatment is expensive.” Similarly, Participant 3 emphasized: “Inability to pay for the cost of treatment” as a significant challenge.
Geographic Accessibility Barriers
Geographic accessibility barriers significantly impeded patients’ access to cleft care centers. Many patients faced difficulties reaching these centers due to their rural locations and lack of transportation options. As Participant 3 pointed out, “Lack of accessibility to the cleft care centres [is a challenge] as most of the patients come from rural communities and the treatment facilities are in urban areas.” Participant 6 shared similar sentiments: “Lack of accessibility to the treatment centre as patients have to travel for a long distance before getting to the treatment facilities.” More so, Participant 7 emphasized that “Lack of accessibility to the cleft care facilities [leads to] late intervention,” underscoring the consequences of delayed care.
Theme 2: Awareness and Support Deficits
This theme encompasses the multifaceted challenges stemming from insufficient knowledge and inadequate social support systems in comprehensive cleft care. It explores how limited awareness about cleft conditions, from prenatal diagnosis to long-term care requirements, intersects with the lack of emotional and community support for patients and their families.
Gaps in Early Detection and Preparedness
The absence of early diagnosis, particularly in-utero, significantly hindered proper preparation and immediate care for newborns with cleft. This knowledge gap affected caregivers’ ability to provide optimal care. Participant 1 noted that “Lack of in-utero diagnosis of patients with cleft…results in parents giving birth at home or where no hospital is available, leaving them uncertain about what to do with the patient regarding feeding and how to take care of the patients with cleft.” Similarly, Participant 6 noted, “Lack of early (in-utero) diagnosis of child with cleft…means caregivers are not aware of caring for babies with cleft.”
Lack of Social Support
Patients and caregivers often lacked adequate emotional and social support systems, leading to profound psychological impacts on patients, caregivers, and families of children with clefts. Caregivers are often “alone on their own with no social support” (Participant 8), highlighting the emotional isolation that accompanies caregiving. This isolation is compounded by the lack of community resources, as Participant 8 further emphasized, “lack of community settings to provide therapy for the parents/patients.” Echoing this sentiment, Participant 6 stated that “Lack of social support for the parents of children born with cleft” has a profound psychological impact on patients and families.
Theme 3: Follow-Up and Compliance Issues
This theme explores the challenges related to ensuring continuity of care for cleft patients, including problems with poor adherence to follow-up appointments and limited understanding of comprehensive, long-term care.
Poor Follow-Up and Adherence
Patients often fail to return for follow-up care after initial treatment, hindering comprehensive cleft care. This issue was highlighted by Participant 2, who noted that “Lack of compliance to follow-up as such other components of comprehensive cleft care are missed out.” Similarly, Participant 3 observed “Lack of patients follow-up after surgical closure of the primary defect” to undermine the effectiveness of treatment.
Limited Understanding of Comprehensive Care
Patients and caregivers often focus solely on surgical repair, neglecting other essential aspects of comprehensive care. Participants pointed out that caregivers’ mindsets are often limited to “concerns only with surgical closure of the defects” (Participant 4). This narrow focus overlooks crucial aspects of care, which are vital for optimal outcomes.
Clinician Factors in Comprehensive Cleft Care Challenge
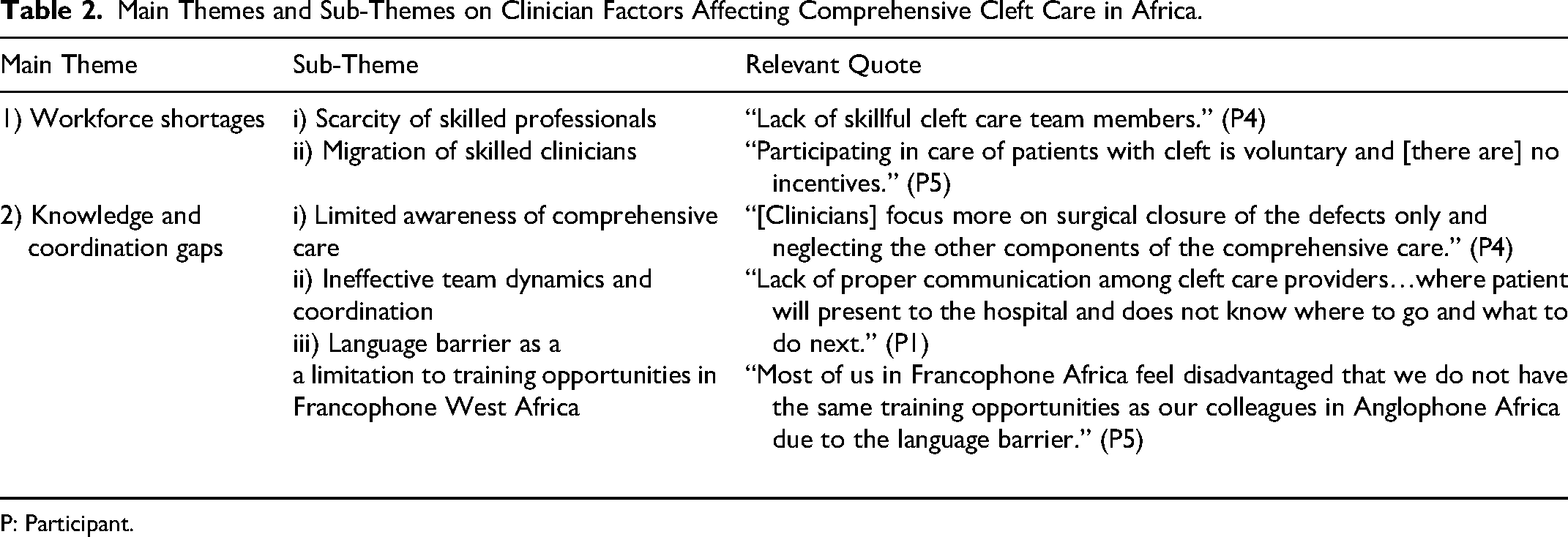
Thematic analysis of clinician factors affecting comprehensive cleft care in Africa generated two main themes and five subthemes (Table 2).
Main Themes and Sub-Themes on Clinician Factors Affecting Comprehensive Cleft Care in Africa.
P: Participant.
Theme 1: Workforce Shortages
This theme explores the issue of insufficient specialized healthcare professionals in the field of cleft care across Africa. It examines the scarcity of trained cleft team members, the lack of interest among clinicians in pursuing cleft care as a specialty, and the impact of brain drain on the availability of skilled clinicians.
Scarcity of Skilled Professionals
There was a significant shortage of skilled professionals across various aspects of cleft care. Participant 4 noted, “Lack of skillful cleft care team members,” a sentiment echoed by Participant 5. Furthermore, participants observed a general lack of interest among clinicians in pursuing cleft care as a specialty, with Participant 1 stating, “Few numbers of surgeons [are] interested in cleft care.” Consequently, this disinterest compounds the workforce shortage, undermining the development of skilled professionals.
Migration of Skilled Clinicians
Theme 2: Knowledge and Coordination Gaps
This theme explores the disconnect between the multifaceted nature of cleft care and the often-limited perspective of clinicians, who may focus primarily on surgical interventions while overlooking other essential aspects of treatment. It also examines how inadequate specialist representation and poor team coordination possess a challenge to comprehensive cleft care.
Limited Awareness of Comprehensive Care
A knowledge gap exists among clinicians regarding the full spectrum of comprehensive cleft care. Participant 1 highlighted this issue, stating, “Lack of awareness on comprehensive cleft care among clinicians.” Furthermore, respondents noted that clinicians often prioritize surgical closure, overlooking other vital aspects of cleft care. Participant 4 emphasized this imbalance, stating, “[Clinicians] focus more on surgical closure of the defects only and neglecting the other components of the comprehensive care.” This limited understanding compromises patient outcomes.
Ineffective Team Dynamics and Coordination
Cleft care teams face challenges in providing comprehensive care due to inadequate specialist representation and communication breakdowns. Participant 2 noted the absence of crucial specialists, such as orthodontists, stating, “Lack of having an orthodontist in the cleft care team.” Furthermore, effective communication among providers is sometimes lacking, hindering patient care coordination. As Participant 1 observed, “Lack of proper communication among cleft care providers…where patient will present to the hospital and does not know where to go and what to do next.” These gaps compromise seamless care for cleft patients.
Language Barrier for Cleftcare Workers in Francophone Africa
Cleft care providers in Francophone Africa reported that they felt disadvantaged in terms of their access to training opportunities, because of the language barrier, when compared to their colleagues in Anglophone Africa. Indeed, participant 5 noted, “Most of us in Francophone Africa feel disadvantaged that we do not have the same training opportunities as our colleagues in Anglophone Africa due to the language barrier.”
Institutional and Governmental Factors in Comprehensive Cleft Care Challenge
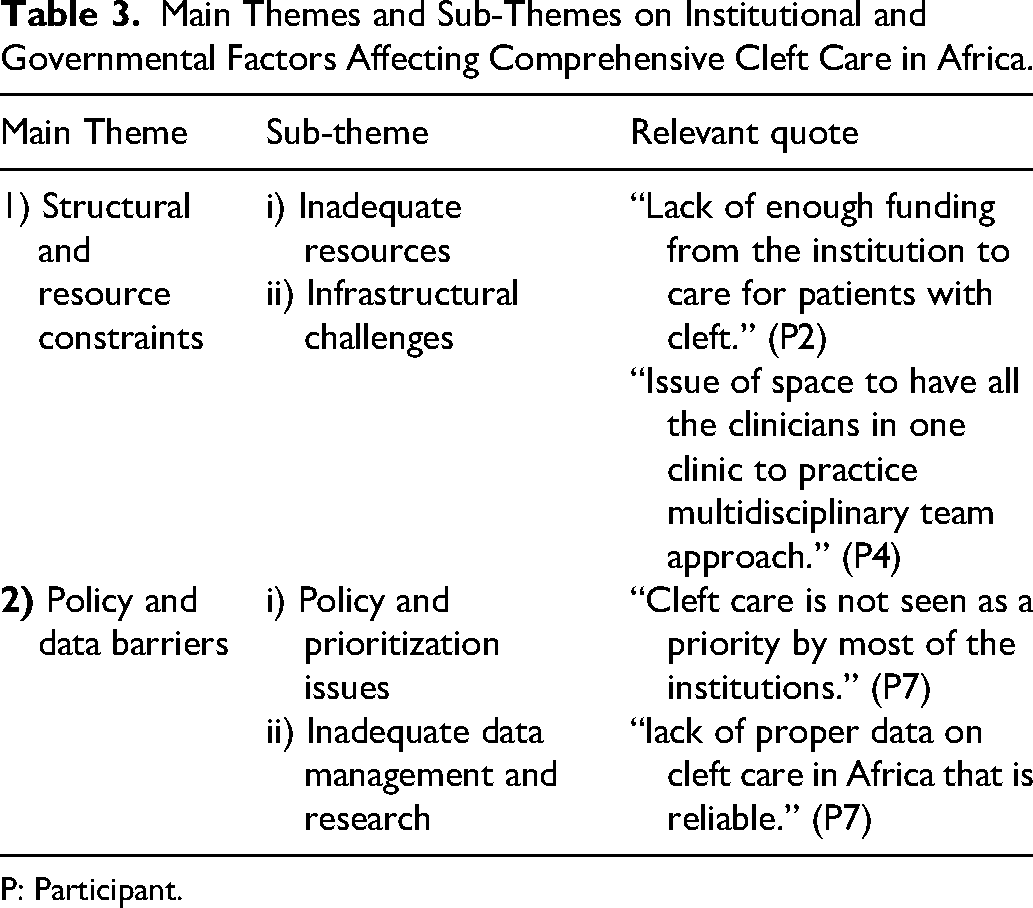
Table 3 shows the two main themes and four subthemes that emerged from the thematic analysis of the institutional and governmental factors affecting comprehensive cleft care in Africa.
Main Themes and Sub-Themes on Institutional and Governmental Factors Affecting Comprehensive Cleft Care in Africa.
P: Participant.
Theme 1: Structural and Resource Constraints
This theme explores the multifaceted resource limitations, including financial constraints, inadequate equipment and consumables, and supply chain issues that hinder effective care delivery. It also addresses the infrastructure challenges to the provision of quality cleft care.
Inadequate Resources
Institutions face significant resource challenges in providing comprehensive cleft care. Financial constraints hinder effective care delivery, with Participant 2 noting, “Lack of enough funding from the institution to care for patients with cleft.” Furthermore, facilities struggle to acquire necessary equipment and consumables, as Participant 3 stated, “Lack of surgical equipment and consumables.” Moreover, supply chain issues, including increased import duties on essential instruments, exacerbate these challenges: “governments increase import duties on most of the instruments and equipment and these are being mostly supplied by donor agencies, so these increments pose a serious challenge in having such materials to work with” (Participant 7).
Infrastructure Challenges
Institutions face challenges in providing suitable spaces for multidisciplinary cleft care teams. Participant 4 noted, “Issue of space to have all the clinicians in one clinic to practice multidisciplinary team approach.” This limitation hinders effective teamwork and coordination.
Theme 2: Policy and Data Barriers
This theme examines how the lack of prioritization of cleft care by institutions and governments, coupled with the absence of political will, creates an environment where comprehensive care is difficult to implement. It also delves into the issues of inadequate data management and insufficient research.
Policy and Prioritization Issues
Participants reported that cleft care often takes a backseat due to institutions and governments not prioritizing it. As one participant pointed out, “Cleft care is not seen as a priority by most of the institutions” (Participant 7). This lack of priority is exacerbated by the absence of political will to support comprehensive cleft care: “Most of the institutions lack the political will to take care of such patients” (Participant 8). Furthermore, institutional policies can hinder the formation of comprehensive care teams, as noted by Participant 2: “In Durban, the institution does not work with NGO'S which makes it difficult to institute a multidisciplinary team care approach.”
Inadequate Data Management and Research
Institutions face challenges in maintaining proper patient records and data, hindering effective cleft care. Participant 5 noted, “lack of proper records for patients with cleft.” Moreover, Participant 7 echoed this concern, observing the “lack of digital data to track the care offered to patients with cleft.” Additionally, participants highlighted the “lack of research” and the “lack of proper data on cleft care in Africa that is reliable” (Participant 7) as barriers to evidence-based decision-making and quality cleft care.
Proposed Solutions to the Challenges Facing Comprehensive Cleft Care in Africa
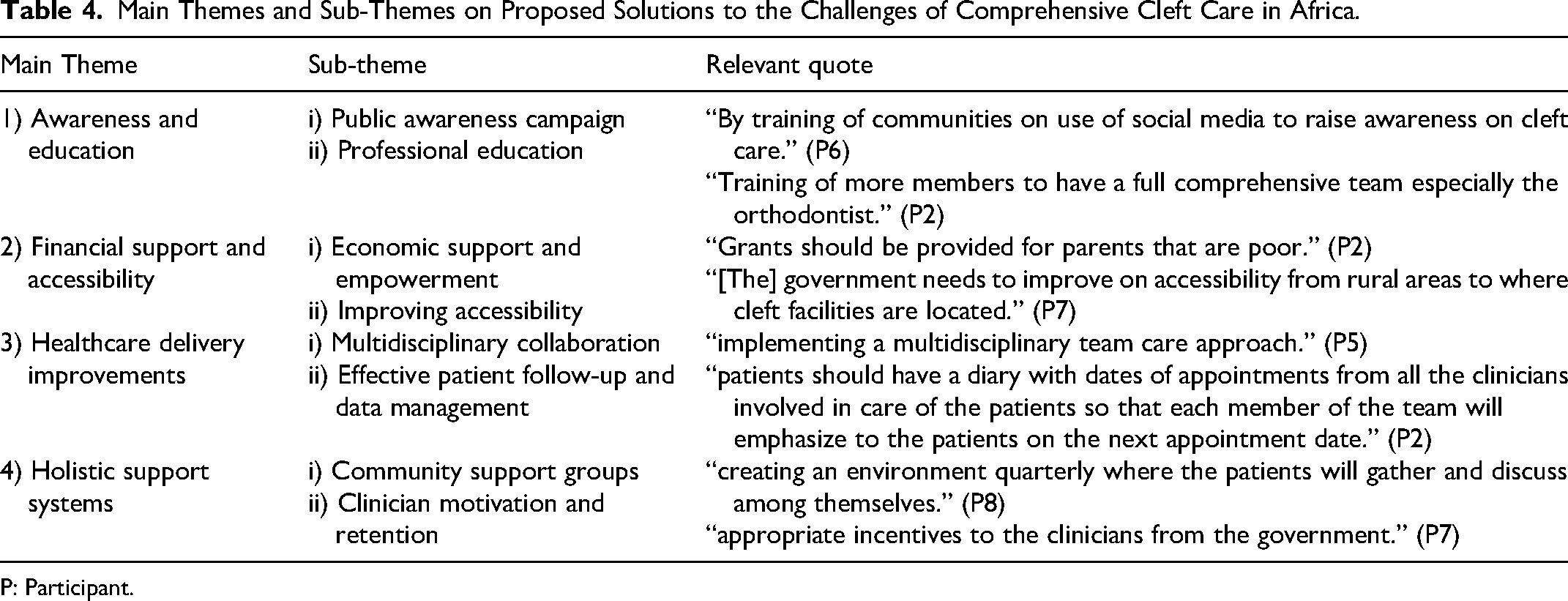
Thematic analysis of the proposed solutions to the challenges in comprehensive cleft care in Africa revealed four main themes and eight subthemes as shown in Table 4.
Main Themes and Sub-Themes on Proposed Solutions to the Challenges of Comprehensive Cleft Care in Africa.
P: Participant.
Theme 1: Awareness and Education
This theme addresses the critical need for knowledge dissemination and skill development in comprehensive cleft care across Africa. This theme encompasses two key areas: public awareness campaigns and professional education. It highlights the importance of educating both the public and healthcare professionals to improve early intervention, enhance the quality of care, and build a more robust, multidisciplinary approach to cleft management.
Public Awareness Campaigns
Participants emphasized the importance of increasing public awareness and promoting early intervention. Various methods were suggested, including workshops at the community level and leveraging social media, as suggested by one participant: “By training of communities or use of social media to raise awareness on cleft care” (Participant 6). Additionally, advocacy on early intervention through prenatal and neonatal counseling was proposed by some participants: “Initiating neonatal counselling at birth in the hospital” (Participant 3). They opined that such an approach was key to “improving and accelerating early diagnosis to reduce burden of care” (Participant 5).
Professional Education
Participants emphasized the importance of training healthcare professionals to enhance knowledge and skills in cleft care. Some opined that one emphasis of such professional development should be multidisciplinary collaboration, with an aim to increase the number of trained professionals in cleft care. As Participant 2 noted, there is a need for “training of more members to have a full comprehensive team, especially the orthodontist.” The scope of training was suggested to extend beyond just the core team, with participants recommending “training of hospital sub-staffs on cleft care…[and] training of nurses for speech therapy” (Participant 1).
The suggested modes of training were diverse, including virtual or in-person training, as well as hands-on experience through site visits. Participant 4 advocated for “training…through webinars, seminars and exposing practitioners to centres that practice multidisciplinary team approach.” The establishment of an African center of excellence for cleft care was proposed to facilitate a comprehensive approach to professional education: “developing a centre of excellence in Africa with the aim of training clinicians to acquire skills on care of children with clefts” (Participant 4).
Theme 2: Financial Support and Accessibility
This theme addresses the need to overcome socioeconomic and geographical barriers that impede comprehensive cleft care. It discusses economic support and empowerment for families affected by cleft conditions and improving accessibility to cleft care services. It highlights the importance of addressing poverty-related challenges through direct financial assistance and economic empowerment, while also focusing on bringing services closer to communities and integrating cleft care into national health policies.
Economic Support and Empowerment
Participants proposed providing direct financial assistance to parents with children with cleft to address poverty-related challenges in comprehensive cleft care in Africa: “Grants should be provided for parents that are poor” (Participant 2). Employing parents and caregivers through economic self-sufficiency was recommended: “Training of parents or the care givers to earn an income while on admission so as to be self-sufficient” (Participant 1).
Improving Accessibility
To address geographical barriers in comprehensive cleft care, participants emphasized the need to bring services closer to communities. As Participant 3 succinctly put it, “by bringing the services closer to the communities.” An alternative approach would be to improve accessibility from rural areas to cleft care facilities located in urban areas. This sentiment was echoed by Participant 7, who stated, “[The] government needs to improve accessibility from rural areas to where cleft facilities are located.”
Some participants further noted that access to comprehensive cleft services would be improved if cleft care was incorporated into the national health insurance policy. Participant 8 advocated for this approach, suggesting that “cleft should be incorporated as a component of universal health care coverage.”
Theme 3: Healthcare Delivery Improvements
This theme explores delivering comprehensive and continuous cleft care in Africa through multidisciplinary care models and effective patient follow-up/data management systems. It highlights coordinated efforts, a comprehensive care mindset, robust patient engagement, and efficient data management as crucial for improved care delivery.
Multidisciplinary Collaboration
Participants emphasized the importance of collaborative care involving various healthcare professionals in comprehensive cleft care. Specifically, implementing and strengthening multidisciplinary teams was identified as crucial for effective care. This sentiment was echoed by multiple participants, with Participant 2 advocating for “instituting a multidisciplinary team approach,” and Participant 5 similarly recommending “implementing a multidisciplinary team care approach.” Furthermore, participants also recognized that achieving this collaborative model requires a shift in perspective across multiple stakeholders. As Participant 4 noted, “clinicians, patients and government must change their mindset on comprehensive care on clefts.”
The concept of collaboration was extended to encompass inter-country cooperation. This approach aims to alleviate immediate workforce shortages and contribute to capacity building by facilitating knowledge transfer between countries: “by sending clinicians from one country to another to treat backloads while providing training” (Participant 8).
Effective Patient Follow-Up and Data Management
Improving patient follow-up was stressed as crucial to ensure continuity of care in comprehensive cleft treatment, with Participant 1 explicitly emphasizing the importance of “addressing the issue of follow-up.” To achieve this, there was a need for coordinated communication and patient engagement. Participant 2 offered a practical suggestion: “to improve compliance to follow up – patients should have a diary with dates of appointments from all the clinicians involved in care of the patients so that each member of the team will emphasize the patients on the next appointment date.” This approach not only helps patients keep track of their appointments but also ensures that all team members are aligned in reinforcing the importance of follow-up care. Additionally, participants recommended implementing a more robust data management system to aid in tracking patients from birth. Participant 3 suggested “having a comprehensive birth registry” as part of this effort.
Theme 4: Holistic Support Systems
This emphasizes the importance of creating a supportive ecosystem that extends beyond medical treatment, addressing both the psychosocial needs of those affected by cleft conditions and the professional needs of healthcare providers. By focusing on community engagement and clinician retention, this approach aims to enhance the overall quality and sustainability of cleft care services.
Community Support Groups
Participants highlighted the importance of establishing community support networks for patients and caregivers. This included instituting support groups to foster emotional support, shared experiences, and community engagement. As Participant 5 recommended “developing community support groups for parents/patients with clefts.” To facilitate these interactions, a regular, structured approach was proposed: “creating an environment quarterly where the patients will gather and discuss among themselves” (Participant 8). These support networks were envisioned to go beyond emotional support, encompassing practical education and health promotion: “psychological support to the parents encouraging them on breastfeeding so as to tackle malnutrition” (Participant 1).
Clinician Motivation and Retention
Participants strongly recommended providing incentives for clinicians to boost retention and dedication in cleft care services. This strategy was seen as crucial for encouraging clinicians to deliver high-quality care and remain committed to cleft care services over the long term. The importance of incentives was echoed by multiple participants: Participant 6 succinctly stated the need for “giving incentives to clinicians,” and Participant 4 added: “motivation for clinicians in form of incentives.” Participant 7 specifically called for “appropriate incentives to the clinicians from the government,” underscoring the role of governmental support in sustaining these incentives.
Discussion
The findings from this study will play a key role in understanding the challenges facing comprehensive cleft care in Africa. Beyond this, it has also proposed solutions to many of the problems highlighted. A major advantage of this study is the involvement of cleft care professionals from across the continent with representation from different regions of the continent.
It is instructive to note that many of the challenges facing comprehensive cleft care in Africa which were reported in this study have previously been reported in many other national or regional studies in the continent.9,12,18–21 However, this study provides a broader context in describing these challenges, as well as providing possible solutions, which is a major difference from previous studies in this regard. In addition to these, it has also brought to fore unique challenges such as the language barriers affecting access to training in cleftcare, as well as the current ‘brain drain syndrome’ which is depleting the availability of cleftcare manpower in the continent.
In terms of patient factors, poverty has been widely cited as a major barrier to cleft care in Africa and this has been reported in many similar studies. 18 Africa is the poorest continent in the world and most of the poorest countries the world can be found in Africa. 22 This high level of poverty is associated with a large percentage of underserved populations and rural populations with limited access to quality healthcare. 23 Poverty limits the resources available to seek healthcare. Indeed, due to poverty many parents are unable to access quality healthcare services and by extension comprehensive cleft care. In addition to this, it is often linked to a low level of education and awareness. 9
In addition to poverty, geographical barriers affecting access to healthcare is also a major challenge for cleft care. A large percentage of these patients live in rural areas with very limited access to healthcare facilities. This is further compounded by the fact that most comprehensive cleft care facilities are in urban centers, within secondary or tertiary healthcare facilities. The high level of poverty is further compounded by the absence of universal healthcare, which is not available in most African countries. All these increase the challenges faced by these patients in accessing comprehensive cleft care. Taiwo et al. 15 in a related study, noted that absence of accessible surgical services with integrated cleft surgical care, was one of the major challenges particularly by patients in rural and underserved communities. The limited access to healthcare also makes it difficult for early detection or in-utero diagnosis for mothers of children with clefts. Although the use of ultrasonography in the diagnosis of cleft lip or cleft lip and palate has been shown to be very reliable, this is not as commonly used in the African population, compared to European and North American populations.24,25
One of the key findings of this study is that lack of emotional and social support for the caregivers of children with clefts in the African population is a major challenge. A similar finding was reported in a study carried out in Northern Nigeria and other parts of Sub-Saharan Africa. 21 This is despite the huge social stigma associated with clefts in the Africa.7,26–28 The absence of psychosocial support may further worsen this stigma. The social stigma associated with clefts may also be responsible for the poor psychosocial support received from the community. Indeed, many studies have reported that patients with clefts and their caregivers receive very limited psychosocial support in this environment.29,30 The frequent hospitalization associated with patients with clefts is often associated with parental feelings of stress, fear, anxiety and helplessness particularly prior to the surgical repair of the cleft. 31 A very recent study in Nigeria reported poorer mental health and quality of life for caregivers of patients with clefts, compared with controls. 32 Thus, psychosocial support plays a key role in managing the psychological challenges that caregivers of children with clefts face.24,25,33 A Ghanaian study reported that spousal support was the major social support received, while emotional support was received from the cleft team. 34 However, there is still limited information on formal psychological support as part of the comprehensive team care patients of children with clefts in Africa.
Poor adherence to follow-up appointments, particularly with non-surgical care such as orthodontic care has previously been reported in a study carried out in Nigeria. 35 In the African environment, greater emphasis is placed by caregivers on correcting the surgical defect, over other aspects of comprehensive cleft care such as speech therapy and orthodontic care. Many reasons have been adduced to this, ranging from ignorance, to a low threshold of satisfaction for postoperative appearance to, the predominant availability of surgical care over the other aspects of comprehensive cleft care in this environment.10,12,36 Indeed, the huge emphasis on surgical repair particularly of cleft lip is due to the stigma associated with the appearance of the child at this stage. A study carried out in 33 African countries revealed that more patients were interested in the aesthetic outcomes of surgery compared with functional outcomes, thus resulting in fewer follow-up visits. 13
Many clinician-related factors were identified as challenges facing the provision of cleft care in Africa and key among this is the shortage of skilled professionals. This has been further worsened by the increased migration of healthcare workers to more advanced countries, due to better remuneration and working conditions. Both conditions are further hampered by a relative scarcity of non-surgical cleft care specialists ranging from speech therapists, orthodontists, pediatric dentists, nutritionists, psychologists and nurses among others in the African continent particularly in Sub-Saharan Africa.9,10,13,36 Another major challenge that was identified in this study was that few clinicians were interested in cleft care. This may be because they do not find it financially rewarding, while another reason may be the huge burden of non-cleft patients, which may reduce the time available to treat patients with clefts and this has been previously reported. 37 Poor team coordination and absence of certain specialties such as orthodontics, speech therapy and nutrition in many cleft centers across the continent is also a major challenge which has been previously cited in literature.7,10,36,6
A major finding from this study was the language barrier reported in Francophone Africa, in terms of accessing training opportunities. This is mainly due to the fact most of the training opportunities for cleftcare providers in Sub Saharan Africa are provided solely in English language or in English-speaking countries. Indeed, research has shown that Francophone, Spanish and Lusophone researchers often face greater challenges in accessing training opportunities and grants which are predominantly available in English. 38 These findings are quite worrisome, when it is noted that French language is the main language of education in many countries in Africa. 39 These Francophone African countries include Togo, Benin, Senegal, Ivory Coast, Burkina-Faso, Cameroon, Niger, Guinea and Chad. Another major language spoken in the continent is Portuguese with six Lusophone countries in the continent namely Angola, Cape Verde, Guinea Bissau, Mozambique, Sao Tome and Principe and Mozambique. Language barriers in Africa have also been shown to affect research visibility and access to research grants, with most health related research such as infectious disease studies, authored by Anglophone African authors, and research grants significantly skewed to the English-speaking African researchers.38,40 It is interesting to note that in 2022 over 90% of the NIH funding in Africa went to English speaking African countries. 41 Thus, these findings highlights the need for intentional actions to be taken to limit the significant disparities in access to training and research opportunities in the African continent which have been driven by language barriers in the continent. Some of the proposed solutions to these challenges include planning equitably distributed healthcare training programs in Anglophone, Francophone and Lusophone Africa; increased use of online learning and training platforms with adequate language translations, leveraging artificial intelligence for real time language translations during training sessions and an intentional approach to ensure adequate language translations in healthcare publications by healthcare journals. 40 All these recommendations can also be directly implemented to address these challenges in cleft care.
The structural and resource constraints affecting the provision of cleft care in this study such as inadequate funding for healthcare in most African countries and inadequate infrastructure have been previously cited in other studies.5,11,18,42 It is also important to note that the absence of a clear policy for cleft care management is a major challenge, which is further compounded by the absence of data for planning and research.
One of the unique features of this study is that the participants presented workable solutions to many of the identified problems. Increasing the awareness of members of the public continues to be a major focus for9,18 addressing the challenges of poor levels of awareness. The use of social media platforms to raise awareness about treatment for clefts was also suggested, as many more people in Africa have access to social media and this has also been advocated by many studies.15,43,44 The importance of increased prenatal counselling on cleft lip and palate was also proposed. Indeed, counselling patients who attend antenatal clinics on this would also aid to increase awareness. Beyond this, there is also a need to train and counsel nurses and traditional birth attendants who often attend to pregnant women particularly in underserved communities.
The importance of professional education of team members on comprehensive cleft care was also highlighted reported in this study. This training of team members is very critical particularly in the African environment with limited specialists available to provide the team care required. There is a need for continuous training of individual team members in the various aspects of cleft care provided, bearing in mind the peculiarities and challenges in the African continent. Equally important is the need for training on the importance of a team approach and this can be used to enhance the quality of cleft care provided.5,14,45 The use of webinars and increased collaboration across African cleft teams would also help to enhance training across the continent. The development of regional centers of excellence across the continent to enhance training and cleft care provision will also go a long way. 5 In addition to this, the need for training of health care professionals such as dentists to provide basic cleft orthodontic care and nurses, doctors and other interested health care professionals to provide speech therapy care may also help to bridge the gap of a shortage of key specialists such as orthodontists and cleft speech therapists required to provide comprehensive cleft care. This approach has been successfully implemented in speech care in Nigeria where some centers have effectively trained nurses to provide basic cleft speech therapy care.
An important solution proffered by the panel was in the area financial support and accessibility to care. The importance of provision of grants to support cleft care was emphasized, while improving accessibility to care particularly for patients in the rural communities. The need for reducing the out-of-pocket cost for pediatric surgical care to patients in Sub-Saharan Africa via increased funding by local governments and international agencies as well as improved health insurance schemes has previously been reported. 19 An interesting suggestion that also came up was encouraging parents and caregivers to be self-sufficient during treatment by empowering them to learn a trade or start a business that could sustain the family in the long run, even beyond the period of care.
Another important area that was highlighted in the study was the need for effective patient follow-up and data management. One of the suggestions from the study participants, which may be very valuable, particularly in resource-limited environments like Africa, is the use of personal patient diaries to record treatment received by different specialists and to help team members monitor the care received. The use electronic medical records would also be very useful in this area although the cost may be a challenge in many African nations due to resource limitation.
The holistic support systems recommended for patients, such as community support groups which would create opportunities for parents and caregivers to provide emotional and psychological support to one and other, are very important.30 Indeed, many caregivers and parents of children with clefts receive significant psychological support from the informal opportunities created for them to interact with one another such as in waiting rooms on clinic days, in centers with regular multidisciplinary clinic days. Thus, creating frequent informal patient interaction opportunities such as quarterly patient meetings, where patients can interact with each other, share experiences and receive health education talks on cleft care in a very friendly and informal atmosphere will go a long way in achieving this. In addition to this, establishing online social media platforms such as WhatsApp groups may also allow for increased patient interaction and peer-support.
There is currently a massive brain drain in Africa with many skilled healthcare professionals migrating from Africa to developed countries 46 and to address this, the panelists recommended improved incentives and remuneration for healthcare workers across the continent. In addition to this, they also recommended better welfare packages and more conducive working environments. African governments have a key role in implementing this and other welfare packages to arrest the brain drain.
This study has several limitations. Firstly, it captures only the perceptions and views of cleft care providers without reflecting the viewpoints of patients. It is also important to note that the panel for the focus group did not include all key specialists involved in cleft care such as speech language pathologists. In addition to this, it was a FGD and some of the challenges of focus groups such as poor participation by a few members may also have affected the quality of the data collected. However, in order to reduce bias in this regard, contributions from all the participants-including quieter members, were considered during the FGD, to avoid a dominance of the views of the more vocal members of the group, thus enhancing the credibility of the findings Furthermore, the study treats Africa as a monolithic region and does not capture the challenges facing cleft care in each of the different regions of Africa. Thus, there is a need for future quantitative studies which will identify the challenges facing cleft care in the different regions of Africa, while proffering solutions to these challenges. The findings of these studies should be shared with political, academic and healthcare leaders in the continent with the aim of addressing the identified challenges.
Conclusion
There are challenges facing the practice of comprehensive cleftcare across the African continent which range from poverty, awareness, clinician factors and institutional factors. However, these challenges can be overcome by increasing patient awareness, improved training and remuneration of healthcare workers and improved Government support and the right policies to support improved cleftcare across the continent.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261428993 - Supplemental material for What Are the Challenges Facing Comprehensive Cleft Care in Africa? A Qualitative Study Involving Cleft Care Providers Across Africa
Supplemental material, sj-docx-1-cpc-10.1177_10556656261428993 for What Are the Challenges Facing Comprehensive Cleft Care in Africa? A Qualitative Study Involving Cleft Care Providers Across Africa by Ikenna Gerald Isiekwe and Puneet Batra in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Approval
Ethical approval for the study was obtained from the Health Research Ethics Committee of the Lagos University Teaching Hospital, Lagos, Nigeria, with approval number: ADM/DSCST/HREC/APP/6568.
Informed consent
Informed consent was obtained from all the study participants.
Author Contributions
The study was conceptualized and designed by Prof Ikenna Gerald Isiekwe and Prof Puneet Batra was involved in the final write-up of the paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.