
Abstract
Objective
To identify sociodemographic and clinical factors associated with missed outpatient plastic surgery appointments among children with cleft lip and palate (CLP).
Design
Retrospective chart review.
Setting
Single urban academic tertiary pediatric hospital.
Patients/Participants
Children with CLP who underwent cleft lip repair between 2015 and 2025. Exclusion criteria included <5 total outpatient visits during the study period or out-of-state primary residence.
Interventions
Not applicable (observational). Management included routine surgical follow-up.
Main Outcome Measure(s)
Occurrence of ≥1 missed outpatient appointment No-show rate (%) among patients with any missed visit.
Results
The cohort (n = 308) was predominantly Hispanic/Latino (55.2%), with high prevalence of public insurance (61.0%), siblings (71.4%), and household instability (40.6%). Patients attended a mean of 12.0 appointments over 5.2 years of follow-up, with 46.1% missing at least one visit. Among those with ≥1 missed appointment, the mean no-show rate was 8.4%. Hierarchical logistic regression identified Black race, household instability, siblings, and pulmonology care as being associated with appointment no-show. In hierarchical linear regression among patients with ≥1 missed visit, older age at follow-up and greater surgical burden were associated with slightly lower no-show rates, with limited contribution from sociodemographic or care coordination factors.
Conclusions
Disparities in appointment attendance may be driven by household-level and clinical complexity factors. Interventions supporting families facing household instability and high caregiving demands may help reduce missed outpatient plastic surgery visits.
Introduction
Children with cleft lip and palate (CLP) require longitudinal, multidisciplinary care from infancy through adulthood, with cleft team guidelines recommending at least annual follow-up. 1 Effective management necessitates coordination among multiple disciplines, including plastic surgery, orthodontics, speech-language pathology, otolaryngology, audiology, dentistry, and genetics. Many children also have associated syndromes or non-cleft comorbidities that further increase care complexity.2,3 The cumulative demands of this care impose substantial financial, logistical, and psychosocial burdens on patients and families, including challenges with scheduling, transportation, lost wages, school absences, and cross-provider communication.
Given the staged and time-sensitive nature of many cleft treatments, continuity of care is critical for optimizing surgical outcomes, speech and language development, and psychosocial well-being. Despite this, missed outpatient appointments remain a persistent challenge in cleft care. In a rural cohort of children with CLP, approximately one in nine patients experienced delays exceeding 90 days for every scheduled visit, highlighting the frequency of disrupted care. 4 At the systems level, nearly 90% of cleft teams report that patients occasionally or often fail to schedule or attend recommended follow-up appointments. 4 Missed visits not only compromise patient outcomes but also contribute to inefficiencies in clinic operations and strain already limited subspecialty resources.
More broadly, disparities in outpatient appointment attendance have been well documented in pediatric surgical populations. Prior studies have identified race and ethnicity, insurance status, and socioeconomic disadvantage as significant predictors of missed appointments and delayed care. 5 These disparities reflect structural and social determinants of health, including transportation barriers, caregiver availability, language discordance, housing instability, and competing family demands. Children with complex chronic conditions may be particularly vulnerable to these challenges, as the volume and frequency of required appointments magnify existing barriers to care.
Within cleft care, there are associations between sociodemographic disadvantage and adverse clinical outcomes.6–8 Missed or delayed follow-up appointments likely represent an important intermediary mechanism linking social disadvantage to suboptimal care delivery. 9
There exists a paucity of research examining missed surgical follow-up appointments for cleft care, particularly so in demographically diverse urban settings. To address this gap, the present study aims to identify sociodemographic and clinical factors associated with missed outpatient plastic surgery appointments among children with CLP treated at a single urban tertiary children's hospital over a 10-year period. By examining both the occurrence of any missed appointment and patterns of no-show behavior among affected patients, this study seeks to better characterize disparities in surgical follow-up and inform strategies to promote equitable access to longitudinal cleft care.
Methods
Study Design
We conducted a retrospective review of all patients with CLP who underwent primary cleft lip repair at a single urban tertiary children's hospital between January 1, 2015, and August 15, 2025. This study was reviewed by the institutional review board and granted an exemption due to minimal-risk retrospective research. Patients were excluded if they attended fewer than five outpatient plastic surgery appointments during the study period, or if they had a primary residence outside the state. The final cohort included 308 patients. Electronic medical records were systematically reviewed to collect demographic, social, and clinical variables, as well as data on outpatient appointment attendance.
Missed appointments were defined as scheduled visits that were not attended and were neither canceled nor rescheduled in advance. Appointments not completed due to inpatient hospitalization, changes in physician availability, or with advance notification by the caregiver were not classified as missed visits and were excluded from the missed-visit outcome. Thus, only unexcused absences were included in the analysis.
The primary aim of this study was to examine the association between social and clinical factors and missed outpatient appointments in children with CLP. Two outcomes were assessed: (1) whether a patient missed at least one outpatient plastic surgery appointment during the study period, and (2) among patients who missed at least one appointment, the proportion of scheduled appointments that were missed (ie, no-show rate).
Data Collection
Patient demographic information included age at most recent plastic surgery visit, gender, and race/ethnicity. In the electronic medical record used at our institution, “Hispanic/Latino” was recorded as a racial category rather than as a separate ethnic identifier. As a result, race and ethnicity could not be independently ascertained, and patients who may have identified as both Black and Hispanic/Latino could not be categorized in multiple groups. For the purposes of this analysis, race/ethnicity was therefore treated as a single combined variable using the mutually exclusive, patient-reported categories: Asian, Black or African American, Hispanic/Latino, White, and Other/Unreported.
Primary language was documented to identify non-English-speaking patients and families, either based on medical record notation or use of interpreters for communication with patients and/or caregivers. Religious affiliation was recorded if noted in the chart. For patients with a single residence during care, an area deprivation index derived from their zip code was calculated as a composite measure of neighborhood-level socioeconomic disadvantage. Insurance type, either private or public coverage, was also recorded as a socioeconomic marker.
Family and social variables included household composition and stability. Household stability was captured by creating a composite measure that incorporated both family structure (eg, single-parent or divorced households) and residential stability (eg, residence in multiple and/or changing addresses during treatment). This approach allowed us to capture both social and residential instability, which prior studies have identified as important predictors of pediatric healthcare access and adherence, without introducing potential collinearity from closely related variables. Presence of siblings or other children living in the household was also recorded, as caring for multiple children is an important stressor that influences the ease at which caregivers can coordinate scheduling and attending appointments. 10
Clinical variables included: diagnosis of a craniofacial syndrome, cleft lip laterality (ie, unilateral or bilateral), timing of CLP repair, total number of surgical procedures, and whether the patient underwent non-cleft-related operations. Given that some patients received early cleft lip repair (ECLR, repair at <6 weeks) while others received traditionally timed lip repair (TLR, repair at 3-6 months) either with or without nasoalveolar molding (NAM), variable called “cleft lip repair algorithm” was constructed to account for differences in timing and type of initial operative intervention. 11 Information on subspecialty involvement beyond the standard cleft team (ie, plastic surgery, otolaryngology, orthodontics, and speech pathology) was also collected. Additionally, when multiple procedures were performed during the same operation (eg, primary cleft lip repair and myringotomy), they were recorded as a single operation for analysis.
The number of non-standard medical specialties involved in a patient's care was used as a continuous measure to allow for dose-response interpretation. Prior literature has examined the relationship between comorbidities and appointment attendance. However, the term “comorbidity” is vague and has a variable definition in surgical research. To circumvent this issue while still being able to assess the severity of medical complexity in our patients, the authors chose to focus on the number and types of subspecialty providers who treated our cohort. Being under the care of nutritionists, cardiologists, and pulmonologists was accounted for in our regression models as proxies for medical complexity. Social work involvement during care was also documented as a measure of additional support for families navigating complex social and medical situations.
Appointment metrics were collected comprehensively from initial consultation to the most recent follow-up. All outpatient appointments with plastic surgery providers were included, regardless of whether they occurred on multidisciplinary care days or via telehealth communication. If a patient was seen by multiple plastic surgery providers on the same day (eg, having an appointment with both a plastic surgery nurse practitioner and a plastic surgeon during a cleft team visit), the visits were considered a single appointment. The no-show rate was calculated as the number of appointments missed without prior notification divided by the total number of scheduled appointments.
Hierarchical Regression Model
To examine predictors of missed appointments and account for potential confounding, a four-block hierarchical regression model was developed (Figure 1). This methodology was modeled after prior work by Lynn et al in 2018 which examined disparities in cleft-related appointment attendance. 10 The first block included demographic factors such as age at most recent visit, gender, and race/ethnicity.
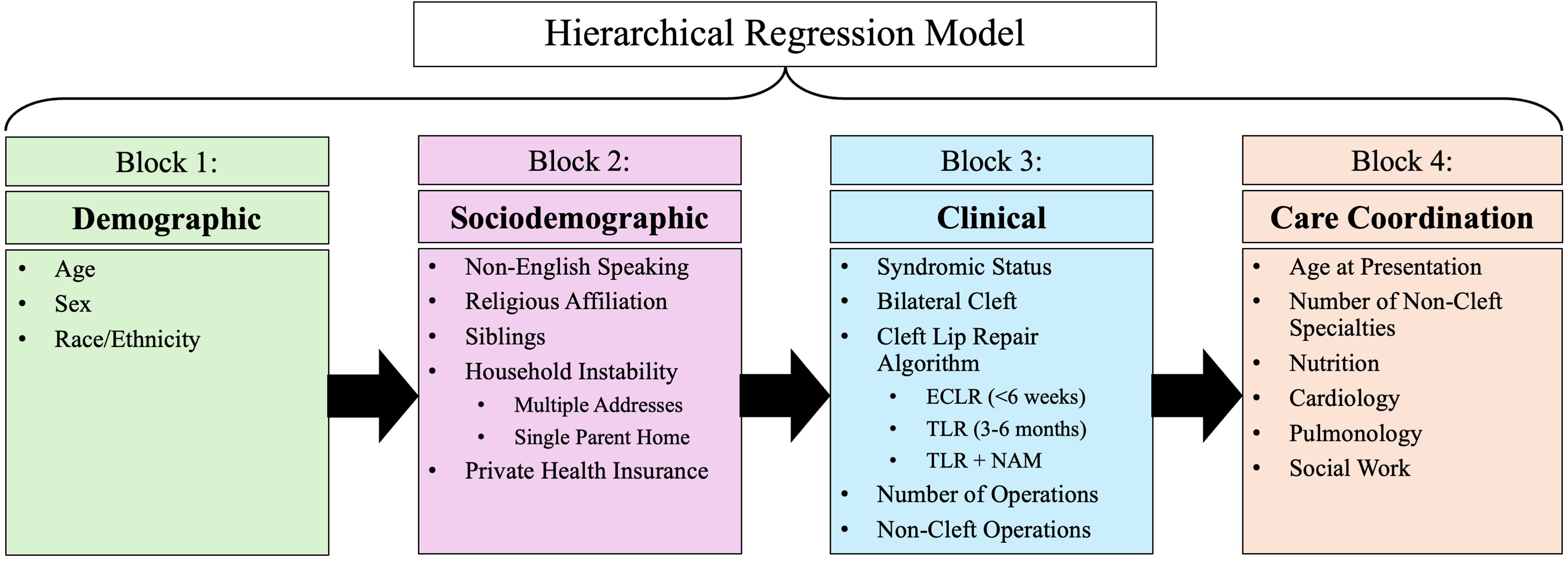
Four-block hierarchical regression model. Variables were entered sequentially in four conceptual blocks—demographic, sociodemographic, clinical, and care coordination—to evaluate predictors of missed appointments using logistic and linear regression models as appropriate.
The second block incorporated sociodemographic and economic indicators, including language, religious affiliation, family composition, address stability, and insurance type. Public health insurance coverage was included as a marker of socioeconomic disadvantage, consistent with previous research showing that children covered by government programs may experience barriers to appointment adherence. 10 Measures of Area Deprivation Index were not included in regression analyses due to collinearity with the use of public insurance and the high prevalence of patients with multiple and/or changing addresses. We also decided against measuring the impact of residential distance from the outpatient clinic due to the variability in patient addresses.
The third block captured clinical variables, including syndromic status, cleft lip laterality, cleft lip repair algorithm, total number of surgical interventions, and non-cleft operations. These variables were chosen because clinical complexity and treatment timing may influence appointment adherence, both through increased healthcare demands on families and through variability in the perceived urgency of care.
The fourth and final block represented care coordination factors, including age at initial presentation with a plastic surgery provider, the number of non-standard specialties following the patient, and the involvement of nutrition, cardiology, pulmonology, and social work in patient care. This block was intended to capture organizational and system-level factors influencing patient adherence. In addition, recording the number of subspecialties allowed us to assess whether broader multidisciplinary involvement was associated with differential appointment attendance.
A four-block hierarchical logistic regression model was used to evaluate predictors of missing at least one appointment. The same 4-block hierarchy was used for a linear regression model examining predictors of the rate of missed appointments among patients with at least one no-show. All analyses were conducted using Stata 19 (StataCorp LLC, College Station, TX), with statistical significance defined as a two-sided P-value <0.05.
Results
Cohort Overview
A total of 308 patients met inclusion criteria for analysis. At the start of the study period, the mean patient age was 6.5 ± 2.6 years, and the cohort was predominantly male (63.3%). Over half of patients identified as Hispanic or Latino (55.2%), followed by White non-Hispanic (24.4%), Asian (10.4%), other or unreported race (6.2%), and Black or African American (3.9%).
Sociodemographic characteristics revealed that 12.7% of patients and/or caregivers primarily communicated in a language other than English, and religious affiliation was documented in 62.7% of the cohort. Having multiple addresses and/or changing residences during the study period was common (40.6%), as was being the child of a single caregiver or a child of divorced parents (22.1%). Siblings or other children were present in the home for 71.4% of patients, and 61.0% were covered by public health insurance.
Operative management included ECLR (repair at <6 weeks) in 40.9% of patients, TLR (repair at 3-6 months) with NAM in 21.1%, and TLR without NAM in 38.0%. Overall, 11.4% of patients had syndromic diagnoses and 33.4% presented with bilateral cleft lip. The median age at cleft lip repair was 4.9 months (IQR 3.2-8.2) for patients with syndromic diagnoses, 3.9 months (IQR 3.1-5.4) for patients with bilateral clefts, and 1.6 months (IQR 1.0-3.7) for patients with unilateral, non-syndromic cleft lip. Patients with syndromic diagnoses (P < 0.001) and those with bilateral clefts (P < 0.001) underwent lip repair at significantly older ages compared with their counterparts.
Within the unilateral, non-syndromic cohort, there was no significant difference in age at lip repair based on ADI (P = 0.328), household instability (P = 0.391), presence of siblings (P = 0.328), or English-speaking status (P = 0.832). However, consistent with prior literature, patients with public insurance underwent repair at significantly older ages compared with those with private insurance (median 2.3 vs 1.2 months, P < 0.001). 7
Although not statistically significant, there was a trend toward older age at cleft lip repair among patients belonging to racial/ethnic minority groups compared with White patients (P = 0.053). For example, Asian patients underwent primary lip repair at a median of 3.4 months (IQR 1.0-4.0) compared with 1.3 months (IQR 0.7-3.1) in White patients. The mean age at palate repair was 14.2 ± 6.5 months.
Patients underwent a mean of 2.45 ± 0.82 surgical procedures during the study period, with 22.7% undergoing at least one non-cleft-related operation. The mean age at initial plastic surgery evaluation was 43.2 days. Care coordination was substantial, with patients managed by a mean of 2.0 ± 2.4 non-cleft medical subspecialties; the most common included genetics, psychology, nutrition, cardiology, pulmonology, and ophthalmology. Social work was involved in 27.9% of cases.
Over a mean follow-up duration of 5.2 ± 2.7 years, patients attended an average of 12.0 ± 4.5 plastic surgery clinic visits. Nearly half of the cohort (46.1%) missed at least one scheduled appointment. Among patients with one or more missed visits, the mean missed-appointment rate was 8.4% ± 2.8% (Table 1).
Demographic, Social, and Clinical Description of Cohort of Cleft Lip and Palate Patients (n = 308).
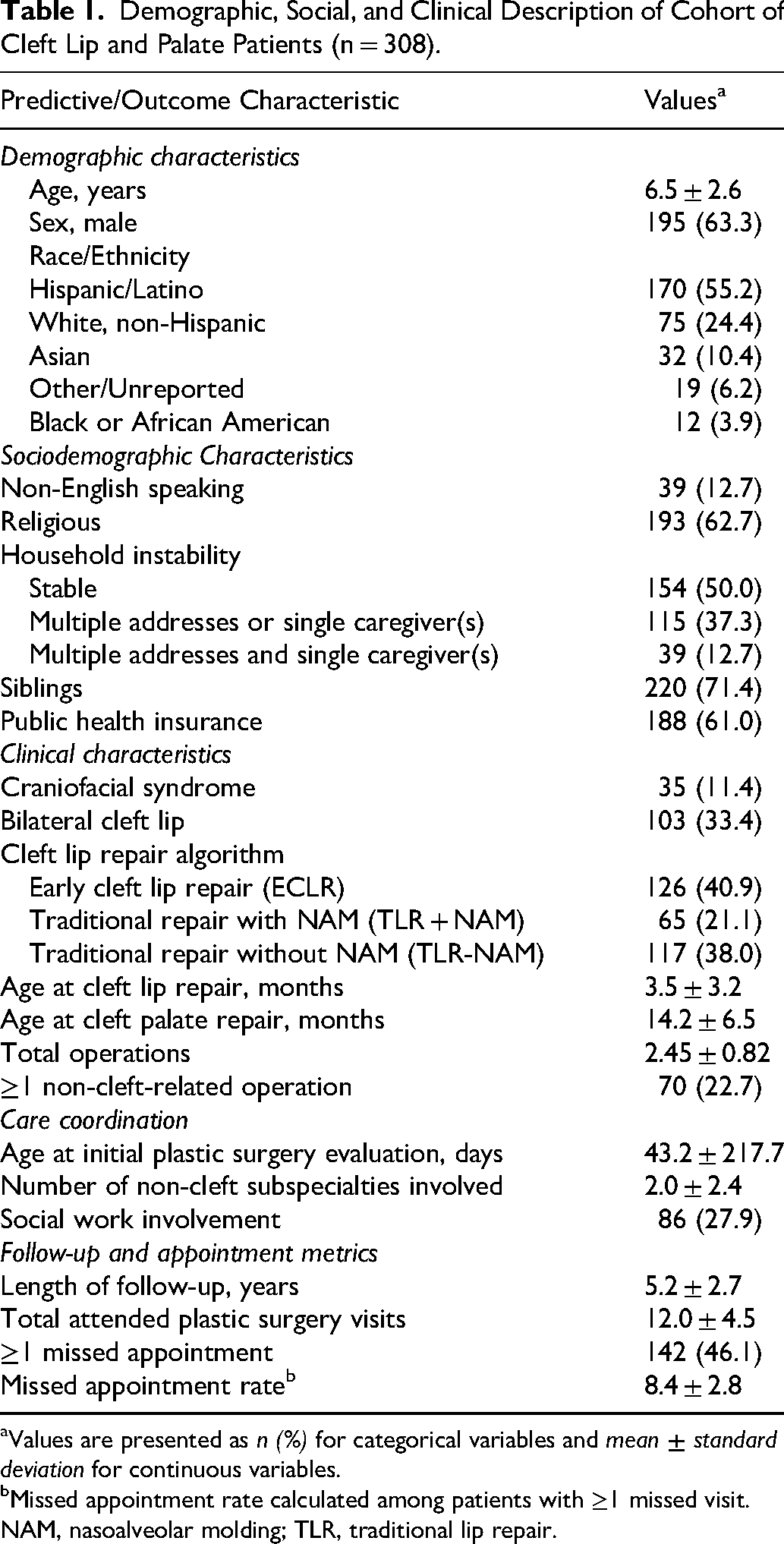
Values are presented as n (%) for categorical variables and mean ± standard deviation for continuous variables.
Missed appointment rate calculated among patients with ≥1 missed visit.
NAM, nasoalveolar molding; TLR, traditional lip repair.
Predictors of Any No-Show
Hierarchical logistic regression was used to identify factors associated with missing at least one outpatient plastic surgery appointment (Table 2). In the final model, household-level variables demonstrated the strongest and most consistent associations with non-attendance. The presence of siblings in the household was associated with more than twice the odds of missing at least one appointment, and household instability exhibited a graded relationship with non-attendance, with the highest odds observed among patients with multiple instability indicators.
Hierarchical Logistic Regression Model: Effect of Sociodemographic and Care Variables at Block Entered and in Final Model on Missing ≥1 Plastic Surgery Appointment. a
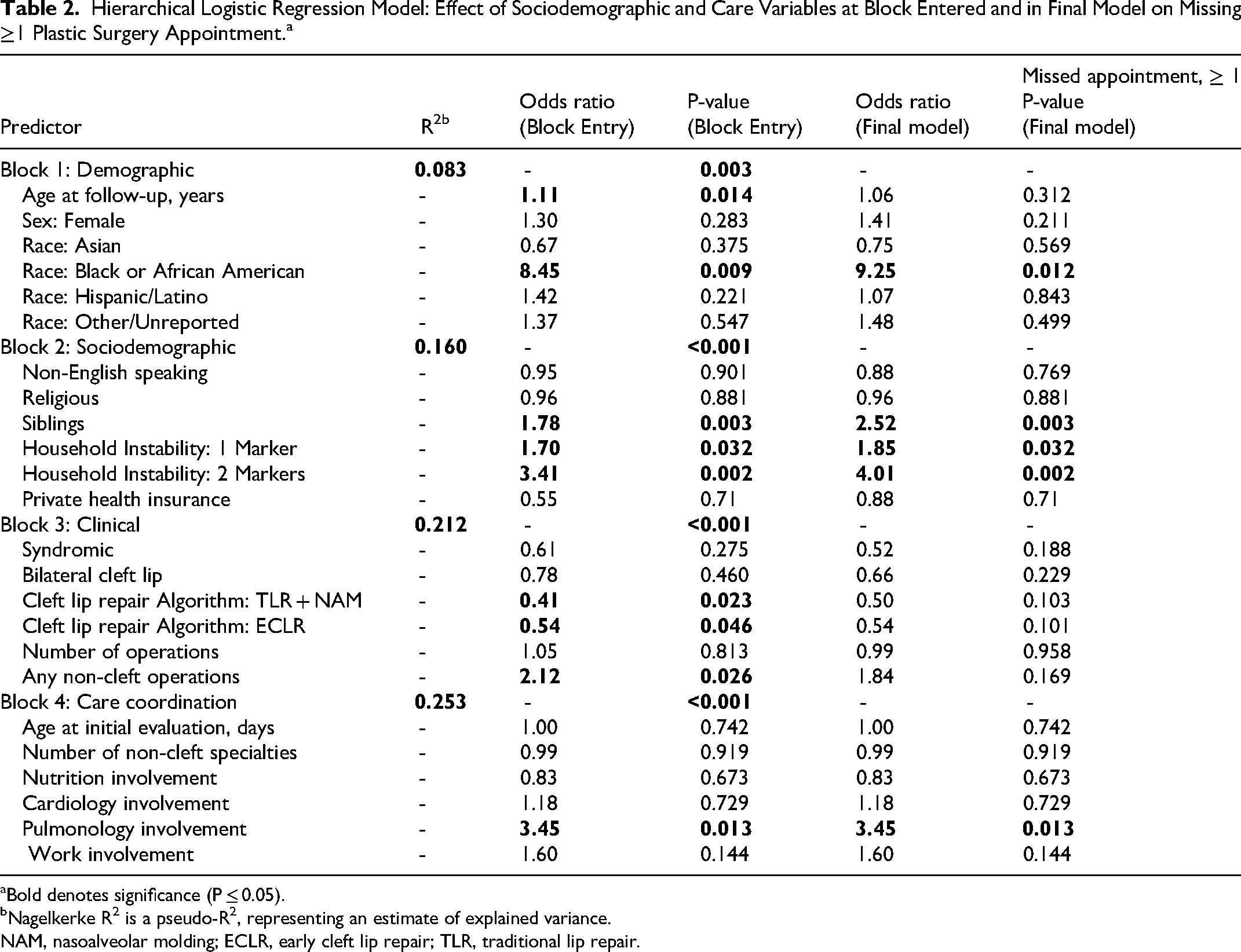
Bold denotes significance (P ≤ 0.05).
Nagelkerke R2 is a pseudo-R2, representing an estimate of explained variance.
NAM, nasoalveolar molding; ECLR, early cleft lip repair; TLR, traditional lip repair.
Black or African American race remained independently associated with substantially higher odds of missing at least one appointment across all model specifications, including the fully adjusted model. In contrast, age, sex, insurance status, primary language, and religious affiliation were not independently associated with attendance in the final model.
Among clinical factors, pulmonology involvement emerged as a significant predictor of missed appointments, whereas other subspecialty involvement and syndromic diagnosis were not. Treatment paradigm, including both ECLR (repair at <6 weeks) and TLR (repair at 3-6 months) with NAM, was initially associated with lower odds of missed appointments; however, these effects were no longer statistically significant after adjustment for clinical complexity and care coordination variables. Measures of care coordination, including the number of non-cleft subspecialties involved and social work engagement, were not independently associated with attendance.
Sequential model comparisons demonstrated that the addition of sociodemographic variables significantly improved model fit over the demographic-only model. The inclusion of clinical and care coordination variables further explained variance in the data, although few of these variables were independently associated with missed appointments in the final model.
Predictors of No-Show Rate
Hierarchical linear regression was performed to examine predictors of appointment no-show rate among patients with at least one missed visit (Table 3). In the final model, demographic and clinical factors accounted for the majority of explained variance, while sociodemographic and care coordination variables contributed minimally.
Hierarchical Linear Regression Model: Effect of Sociodemographic and Care Variables in Final Model on Plastic Surgery Appointment No-Show Rate. a
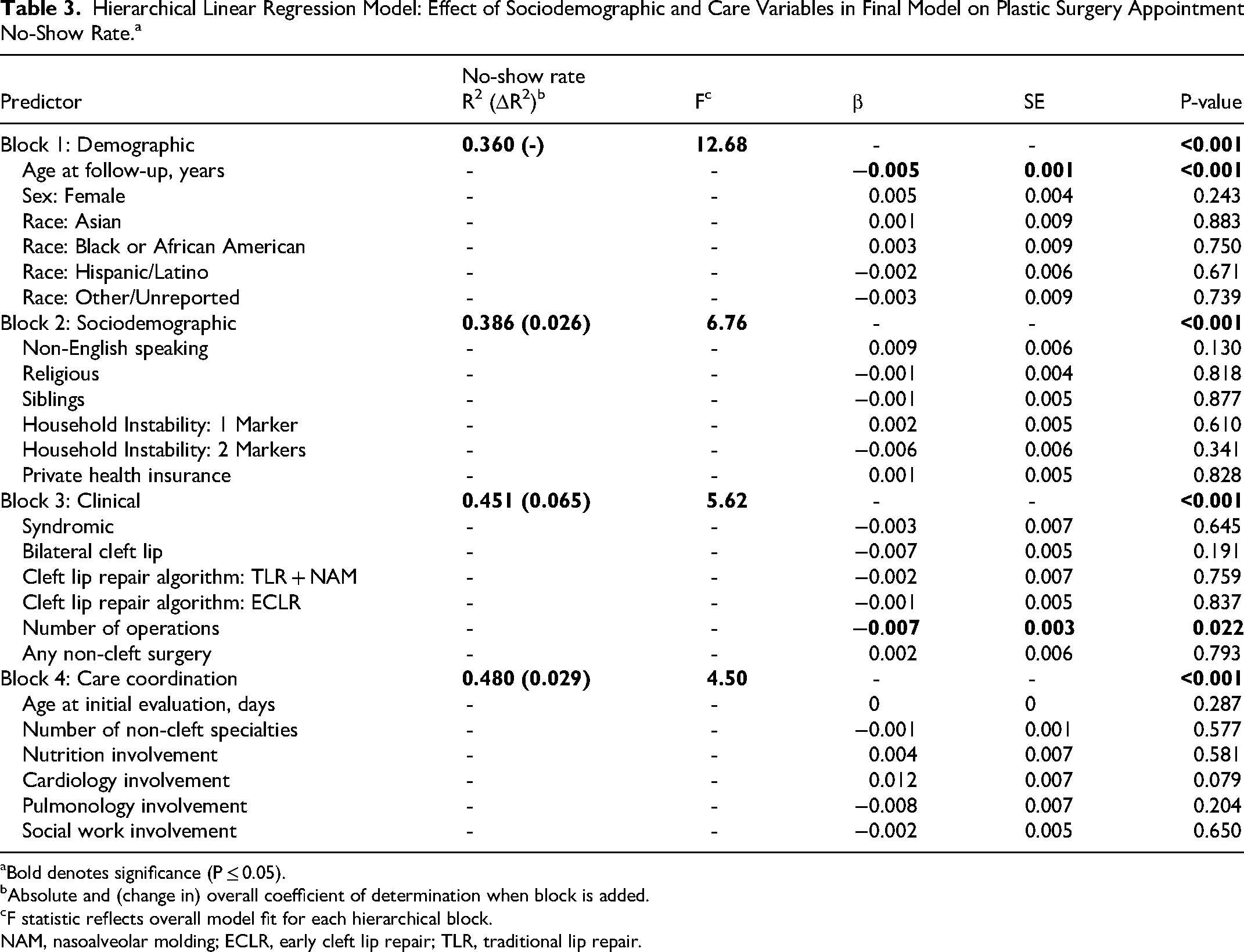
Bold denotes significance (P ≤ 0.05).
Absolute and (change in) overall coefficient of determination when block is added.
F statistic reflects overall model fit for each hierarchical block.
NAM, nasoalveolar molding; ECLR, early cleft lip repair; TLR, traditional lip repair.
Older age at follow-up and greater number of surgical procedures were independently associated with modestly improved attendance. No-show rates decreased by approximately 0.5% per additional year of follow-up. Similarly, each additional operation was associated with a 0.7-0.8% absolute reduction in no-show rates, suggesting that greater cumulative engagement with surgical care may reinforce longitudinal follow-up. Race, household structure, and measures of household instability were not significantly associated with no-show rate in the fully adjusted model.
The addition of care coordination variables also improved overall model fit; however, no individual care coordination variable was independently associated with no-show rate in the final model. Overall, predictors of repeat non-attendance were weaker and less consistent than predictors of missing any appointment.
Discussion
In this retrospective cohort study of children with CLP followed at a large urban tertiary children's hospital, nearly half of patients missed at least one outpatient plastic surgery appointment over a mean follow-up of more than 5 years. Missed appointments were not randomly distributed across the cohort but were associated with household-level social context and selected markers of clinical complexity. Importantly, predictors of any missed appointment differed meaningfully from predictors of repeat non-attendance, suggesting that missed visits in pediatric cleft care may reflect episodic vulnerability rather than persistent disengagement from care. These findings have important implications for how cleft teams identify families at risk for missed visits and how they intervene to support longitudinal attendance.
This study builds upon prior work examining appointment adherence in cleft populations. Lynn et al identified sociodemographic predictors of missed cleft-related appointments using a composite outcome that included visits with multiple types of medical specialists, a common strategy in the existing literature.10,12,13 In contrast, the present study focused specifically on outpatient plastic surgery visits and distinguished between initial and repeat non-attendance, allowing for a more granular examination of attendance behavior within surgical care.
The observed no-show rate of 8.4% among patients with at least one missed visit is on the lower end of rates reported in prior cleft studies, which range from approximately 9% to over 20% depending on the population and care setting.10,12 This finding is consistent with evidence that non-surgical cleft-related visits, such as pediatric dentistry and speech therapy, exhibit higher no-show rates than surgical follow-up. For example, no-show rates of 22.4% have been reported for pediatric dental visits in cleft populations, and adherence to speech therapy follow-up has been reported as low as 50.6% after initial evaluation.14,15 These differences likely reflect variation in perceived urgency, visit frequency, and logistical burden across domains of care.
Household-level factors emerged as the strongest predictors of missing any outpatient plastic surgery appointment. The presence of siblings and household instability were both independently associated with initial no-show. These variables likely capture aspects of family life that are not fully reflected by traditional socioeconomic indicators such as insurance status or neighborhood deprivation. In practical terms, our composite metric of household instability may represent frequent moves, inconsistent transportation access, changes in caregiving arrangements, or financial stressors that complicate appointment planning. Similarly, caring for multiple children increases the logistical complexity of attending clinic visits, particularly in families with limited external support.
Notably, these household factors predicted the occurrence of at least one missed appointment but were not associated with higher no-show rates among patients who had already missed a visit. This pattern suggests that such stressors may exert their greatest influence during periods of acute overload rather than acting as persistent barriers to care. A caregiver navigating competing demands may miss a single appointment due to unforeseen circumstances but subsequently re-engage once the immediate disruption resolves. This interpretation aligns with broader pediatric adherence literature indicating that missed appointments often reflect situational challenges rather than intentional noncompliance. 13
The association between Black or African American race and missed appointments warrants careful interpretation. This finding is consistent with prior studies demonstrating higher rates of attrition from long-term multidisciplinary cleft and craniofacial follow-up among Black patients compared with other racial and ethnic groups.12,16 Importantly, this association persisted in a cohort characterized by substantial racial and ethnic diversity and a majority Hispanic/Latino population.
Although not a primary focus of this study, we observed a trend toward older age at cleft lip repair among racial and ethnic minority patients compared with White patients. This relationship did not reach statistical significance in our analysis; however, similar trends in the timing of cleft lip repair have been reported in prior literature.6,7 This finding should be interpreted cautiously but may suggest differences in access to timely surgical care that warrant further investigation. Future studies specifically designed to examine disparities in surgical timing are needed to better characterize this relationship.
The urban, Hispanic-majority composition of this cohort further distinguishes it from prior cleft studies, which have typically included Latino populations comprising less than 5% of participants.10,12 Despite this difference, Black race remained a significant predictor of missed appointments, reinforcing the consistency of this association across diverse healthcare environments. In contrast, other sociodemographic factors previously associated with missed visits (eg, insurance status, area deprivation index, and geographic distance) were not confirmed as significant in this population.10,12,17 These discrepancies may reflect differences in healthcare infrastructure, transportation access, or clinic-level support mechanisms in various geographic settings.
Clinical variables demonstrated a more nuanced relationship with appointment attendance. Pulmonology involvement emerged as an independent predictor of missing at least one appointment, potentially reflecting the substantial care burden faced by patients with respiratory comorbidities early in life. 18
In contrast, among patients with at least one missed appointment, a greater total number of surgical procedures was associated with lower no-show rates. One plausible explanation is that increased surgical burden heightens caregivers’ perception of the importance of perioperative planning and postoperative follow-up, reinforcing attendance once families are engaged in care. This finding suggests that perceived urgency and salience of surgical visits may mitigate repeat non-attendance, even in the presence of social or logistical challenges.
Treatment paradigms such as ECLR (repair at <6 weeks) and TLR with NAM were initially associated with lower odds of missed appointments; however, these associations attenuated after adjustment for clinical complexity and care coordination. This suggests that overall care complexity, rather than the surgical algorithm itself, may play a greater role in appointment attendance.
Care coordination variables, including the number of non-cleft subspecialties involved and social work engagement, did not meaningfully improve model fit beyond sociodemographic and clinical factors. This finding may reflect limitations in how care coordination was operationalized rather than a lack of true effect. The number of subspecialties involved may inadequately capture the intensity or timing of healthcare demands, while social work involvement may preferentially identify families already experiencing significant challenges.
Prior research has demonstrated that logistical factors such as high monthly healthcare burden, multiple same-day appointments, and travel demands may mediate the relationship between sociodemographic characteristics and appointment adherence. 13 In this context, household composition and instability may serve as more sensitive proxies for logistical complexity than traditional demographic measures. Future studies incorporating more granular assessments of scheduling burden, transportation access, and caregiver availability may better elucidate these relationships.
Clinic-level practices may also shape repeat attendance. Although not directly measured in this study, standardized reminder systems, flexible scheduling, and proactive outreach after missed appointments may promote re-engagement and help explain why predictors of repeat non-attendance were relatively weak. These system-level factors likely interact with family-level vulnerabilities in determining attendance patterns. While changing family availability for specific appointments is often difficult, reducing the friction of communicating with the clinic is much more feasible. For example, text- or app-based reminders can allow families to confirm or reschedule with a single click.
Taken together, these findings suggest that missed appointments should be interpreted as opportunities for targeted support rather than indicators of intentional poor engagement. Because household instability and caregiving burden were associated with an initial missed visit but not with sustained high no-show rates, interventions may be most impactful when deployed early. From an implementation perspective, our findings support a tiered, risk-stratified approach to improving appointment adherence. For example, screening for markers of household instability at intake could trigger enhanced outreach, including direct phone contact, assessment of transportation or childcare barriers, and facilitated rescheduling within a short time frame. Embedding structured workflows, such as automatic alerts to care coordinators after a first no-show, may help operationalize this process.
For families experiencing ongoing logistical strain, clustering same-day multidisciplinary appointments, offering extended-hours clinics, using telehealth for appropriate follow-up visits, and providing transportation or parking assistance may reduce structural barriers. Given the persistent association with Black race, parallel efforts to ensure culturally responsive communication, address implicit bias in outreach practices, and incorporate community-informed patient navigation are also warranted. Importantly, these interventions should be framed as supportive rather than punitive and should reinforce partnership with families during periods of episodic vulnerability.
Strengths of this study include a large, well-characterized cohort, extended longitudinal follow-up, and the use of hierarchical modeling to disentangle the contributions of demographic, social, and clinical factors. Several limitations warrant consideration in this single-center retrospective study. Reliance on electronic medical record data limited the ability to assess appointment cancelations, rescheduling patterns, or delays relative to recommended follow-up intervals. The study did not directly examine the relationship between missed appointments and clinical outcomes, such as surgical timing, complication rates, or functional results. Additionally, the study period spanned a decade, over which time our institution's appointment scheduling and reminder systems may have evolved. This study also spans the COVID-19 pandemic, during which substantial disruptions to outpatient care occurred, and subgroup analyses were not performed to isolate pandemic-related effects.
Finally, this analysis focused exclusively on plastic surgery visits, a useful subset of patient visits for plastic surgeons to analyze, even though cleft care is intentionally and importantly multidisciplinary. Families may prioritize surgical care differently from other aspects of cleft management, potentially contributing to the observed differences in no-show behavior.
Future research may prospectively evaluate appointment adherence across multiple cleft care disciplines and assess the impact of missed visits on clinical outcomes. Studies examining targeted interventions such as enhanced reminder systems, transportation assistance, or flexible scheduling would be helpful for determining whether early support following a first missed appointment can improve long-term engagement. Addressing patient- and caregiver-reported barriers is essential for designing equitable and effective strategies to support families navigating the complex demands of cleft care.
Conclusion
Missed outpatient plastic surgery appointments are common among children with CLP and were primarily associated with household-level social context in this cohort. Nearly half of patients missed at least one visit during long-term follow-up, with predictors of an initial missed appointment differing from those associated with repeat non-attendance. These findings suggest that missed visits often reflect episodic social or logistical vulnerability rather than chronic nonadherence.
Household instability, the presence of siblings, and Black or African American race were associated with increased odds of missing at least one appointment, while repeat non-attendance was weakly explained by sociodemographic and clinical factors. Greater surgical burden was associated with improved attendance among patients with prior missed visits, suggesting that perceived urgency of care may reinforce engagement with plastic surgery clinics.
These results support interpreting missed appointments as opportunities for targeted support rather than indicators of poor medical engagement. Early identification of families experiencing increased caregiving or logistical burden may enable timely, supportive interventions to improve continuity of care in pediatric cleft populations.
Footnotes
Acknowledgments
None.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Children's Hospital Los Angeles (no. 24-00011), with the need for written informed consent waived.
Informed Consent Statements
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.