
Abstract
Objective
To determine whether initial lip asymmetry predicts long-term symmetry changes in patients with unilateral cleft lip and alveolus (UCLA) and to characterize patterns of region-specific morphic change relevant to orthodontic planning.
Design
Retrospective observational study.
Setting
University-based orthodontic clinic.
Patients
Among 80 UCLA patients treated between 2008 and 2023, 42 with standardized frontal photographs at two treatment stages (before active orthodontic treatment [T1] and before comprehensive orthodontic treatment [T2]) under rest and smile conditions were included.
Main Outcome Measures
Ten lip-related measures (7 linear distances, 3 angular variables) were obtained from frontal images, and left-to-right asymmetry was calculated as the difference between the noncleft and cleft sides (noncleft-cleft). Longitudinal change was defined as Δ = T2 − T1. Paired t tests with effect sizes (Cohen's dz) and false discovery rate adjustment were used, and importance scores were used to visualize the combined magnitude and robustness of changes.
Results
Overall lip symmetry tended to improve from T1 to T2 in both rest and smile conditions. Measure 2 (peak of Cupid's bow to oral commissure distance) and Measure 6 (lower lip width) exhibited negative Δ values with moderate effect sizes (dz = 0.39-0.42) in unadjusted analyses. After adjustment for multiple comparisons, no comparisons remained statistically significant; however, effect-size patterns suggested consistent, moderate improvement in symmetry in regions around the Cupid's bow.
Conclusions
Initial lip asymmetry influences long-term symmetry changes in UCLA patients. Quantitative assessment of region-specific symmetry changes may support interdisciplinary planning focused on individualized soft-tissue outcomes.
Introduction
Cleft lip with or without cleft alveolus is among the most common congenital craniofacial anomalies, and unilateral cleft lip and alveolus (UCLA) is one of the most common clinical subtypes encountered in clinical practice. Individuals with UCLA experience functional and esthetic challenges from birth, including impairments in feeding and speech development as well as marked facial asymmetry. 1 Consequently, primary cheiloplasty plays a critical role in restoring lip form and function and in improving overall quality of life.2–6
Despite advances in surgical techniques, residual asymmetry of the lip and perioral soft tissues frequently persists after repair in patients with UCLA.7–9 Achieving long-term facial harmony therefore remains a clinical challenge. From an orthodontic perspective, treatment planning must extend beyond dental alignment and occlusal correction to encompass growth-related changes in facial soft tissues and overall symmetry throughout development.7–9
The primary goals of cheiloplasty are to reconstruct a lip morphology that is both esthetically pleasing and functionally competent while minimizing psychological burden on the patient.2–6 However, asymmetry may re-emerge or become accentuated during postoperative growth, influenced by craniofacial development and orthodontic intervention.7–9 In particular, changes in lip morphology across different functional conditions—such as rest and smile—during the period before active orthodontic treatment and before comprehensive orthodontic treatment have not been sufficiently characterized.10–12
Previous studies have identified multiple factors influencing postoperative outcomes, including surgical technique, surgeon experience, individual anatomic characteristics, and postoperative management.2–6 However, limited attention has been given to the relationship between initial lip asymmetry at T1 and subsequent longitudinal changes in lip symmetry during growth.7–9,12–14
Therefore, the purpose of this study was to investigate how the severity of initial lip asymmetry at T1 influences longitudinal changes in lip symmetry between T1 and T2 in patients with UCLA, under both rest and smile conditions. From a clinical orthodontic perspective, identifying lip regions that demonstrate greater responsiveness during this early treatment-related growth phase may assist clinicians in anticipating long-term soft-tissue outcomes and in determining the timing and necessity of secondary revision procedures.
Two-dimensional photographic analysis was used as the primary evaluation method in this study. This approach is widely used in clinical practice and enables direct comparison with established assessment criteria, as well as longitudinal tracking of morphologic changes. 11
Materials and Methods
Study Population
This retrospective study included 80 patients with UCLA who were referred to a Dental College-based orthodontic department between April 2008 and March 2023 from 2 tertiary referral centers: Tokyo Dental College Ichikawa General Hospital and Chiba Children's Hospital.
Among these patients, 42 cases with archived standardized frontal facial photographs obtained at both time points—before active orthodontic treatment (T1) and before comprehensive orthodontic treatment (T2)—in two facial conditions (rest and smile) were eligible for analysis.
This study was approved by the Ethics Committee of Tokyo Dental College (Approval No. 1211) and was conducted in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Patients were included if they met the following criteria: (1) diagnosis of nonsyndromic UCLA; (2) availability of standardized frontal facial photographs at both T1 and T2 under rest and smile conditions; and (3) completion of primary lip repair during infancy according to institutional treatment protocols.
Patients were excluded if they had: (1) associated craniofacial syndromes or systemic conditions affecting craniofacial growth; (2) history of secondary alveolar bone grafting between T1 and T2; (3) additional major craniofacial surgical procedures during the observation interval; or (4) incomplete photographic records.
No additional or repeated alveolar bone grafting procedures were performed during the interval between T1 and T2.
All patients were of Japanese ethnicity to minimize variability in soft-tissue characteristics.
Primary lip repair had been performed during infancy by two experienced cleft surgeons at each institution according to standardized institutional protocols. Although minor variations in surgical technique existed, all procedures were based on established rotation-advancement principles.
Facial Photograph Acquisition and Evaluation Stages
Standardized frontal facial photographs were obtained at two distinct time points: T1, defined as before the initiation of active orthodontic treatment, and T2, defined as before the initiation of comprehensive orthodontic treatment. At each time point, photographs were acquired under two facial conditions: rest and smile. Lip symmetry was evaluated separately for each condition.
Accordingly, four evaluation categories were defined:
T1-R: rest at T1 T1-S: smile at T1 T2-R: rest at T2 T2-S: smile at T2
All frontal facial photographs were obtained using a standardized clinical photography protocol at each institution. Subjects were positioned in natural head position with the Frankfort horizontal plane oriented parallel to the floor. A fixed camera-to-subject distance and consistent focal length were maintained to minimize perspective distortion.
Photographs were taken under uniform lighting conditions with patients instructed to maintain a relaxed lip posture for rest images and a natural posed smile for smile images. Images were cropped to include the nasal base and perioral region while excluding extraneous facial structures to reduce measurement bias.
Prior to measurement, images were standardized for scale by adjusting for interpupillary distance to ensure consistency across time points. All measurements were performed using calibrated digital image analysis software, with pixel-based scaling applied to allow reproducible quantification of linear and angular parameters.
Importantly, the interval between T1 and T2 represents a clinically meaningful phase in which orthodontic intervention begins to modify the dentoalveolar foundation supporting the lip, rather than reflecting physiologic growth alone.
Measurement Variables
A total of 10 lip-related variables were assessed, comprising 7 linear distances and 3 angular measurements. To quantitatively evaluate postoperative lip growth patterns, the following anatomical landmarks were identified on frontal facial photographs: subnasale (A), peak of the Cupid's bow (B), midpoint of the Cupid's bow (C), oral commissure (D), and the point on the lower vermilion border showing the maximum vertical distance from the intercommissural line (E) (Figure 1A).
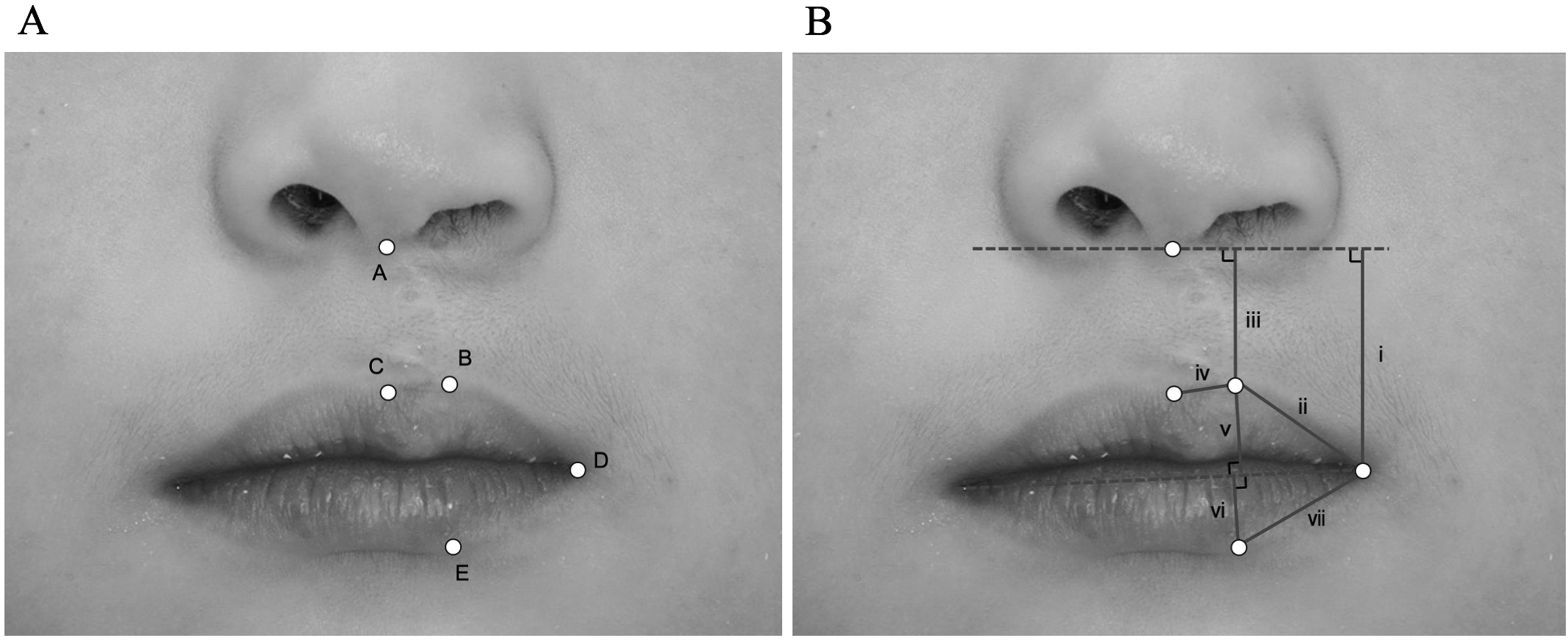
Anatomical landmarks and measurement definitions used for lip asymmetry analysis. A: Standardized frontal facial photograph illustrating the anatomical landmarks used for quantitative assessment of lip morphology: (A) subnasale; (B) peak of the Cupid's bow; (C) midpoint of the Cupid's bow; (D) oral commissure; and (E) the point on the lower vermilion border showing the maximum vertical distance from the intercommissural line. Landmarks were identified bilaterally where applicable. B: Schematic representation of the linear (i–vii) and angular (viii–x) measurements used to quantify lip asymmetry.
The linear measurements included:
vertical distance from the oral commissure to subnasale, distance from the peak of the Cupid's bow to the oral commissure, vertical distance from the peak of the Cupid's bow to subnasale, distance from the peak to the midpoint of the Cupid's bow, upper lip width, lower lip width, and distance between the oral commissure and the point of maximum distance from the intercommissural line on the lower vermilion border.
The angular measurements included:
(viii) the angle at the peak of the Cupid's bow, (ix) the angle at the oral commissure, and (x) the angle formed between the line connecting the cleft-side and noncleft-side points of maximum distance from the intercommissural line on the lower vermilion border and the line connecting the oral commissure to the same point (Figure 1B). The selected anthropometric landmarks and measurement variables were based on established craniofacial anthropometric methodologies and previous studies of lip morphology in cleft patients.13,15
Presurgical Severity Classification
Presurgical severity was classified according to a previously described method. 16 As in the original report, presurgical photographs were primarily used for assessment. When presurgical photographs were unavailable, sketches and panoramic radiographs were additionally referenced. Each morphological component was evaluated and categorized based on the predefined scoring criteria.
Outcome Measures
The primary outcome was left-right asymmetry, calculated as the difference between the noncleft and cleft sides (noncleft-cleft) for each measurement. Longitudinal change in asymmetry was defined as Δ = T2 − T1. Negative values indicate greater measurements on the cleft side. Negative values of Δ indicate a reduction in asymmetry and thus an improvement in symmetry.
Statistical Analysis
Paired t tests (two-tailed, α = 0.05) were performed to compare asymmetry between T1 and T2 for each measurement under both facial conditions (rest and smile). Effect sizes were calculated as Cohen's dz.
To integrate both the magnitude of change and statistical robustness, an importance score was calculated as −log10(q) × |dz|. This composite index should be interpreted as a complementary exploratory metric rather than a definitive statistical test and was used to facilitate intuitive visualization of region-specific change patterns by jointly considering effect magnitude and statistical robustness.
To control for multiple comparisons, the Benjamini–Hochberg false discovery rate (FDR) procedure was applied, and adjusted P values (q values) were obtained. The Benjamini–Hochberg procedure was selected as a widely accepted method to control for multiple comparisons while maintaining statistical power. 17
The analytical workflow included visualization of data distribution using scatter plots, paired t tests for each measurement under rest and smile conditions, calculation of effect sizes (Cohen's dz), FDR adjustment for multiple comparisons, and visualization of importance scores.
Given that the primary objective of this study was to evaluate within-subject longitudinal changes between T1 and T2, paired statistical analyses were selected a priori as the most appropriate method to account for intra-individual variability. This investigation was designed as an exploratory longitudinal study rather than a comparative interventional trial.
Furthermore, interim orthodontic procedures represented routine early-phase management rather than protocol-driven interventions; therefore, subgroup statistical comparisons were not performed to avoid overinterpretation of secondary findings.
All statistical analyses were performed using SPSS Statistics (version 27; IBM Corp., Armonk, NY, USA).
Results
Participant Characteristics
Among the 42 patients with UCLA included in this study, 12 were referred from Tokyo Dental College Ichikawa General Hospital and 30 from Chiba Children's Hospital (Table 1). No significant differences were observed between institutions with respect to age or developmental stage at either T1 or T2 (T1: P = .755; T2: P = .139). In contrast, the sex distribution differed significantly between institutions, with a higher proportion of female patients in Tokyo Dental College Ichikawa General Hospital (P = .03).
Demographic Characteristics of Patients With Unilateral Cleft Lip and Alveolus by Institution.
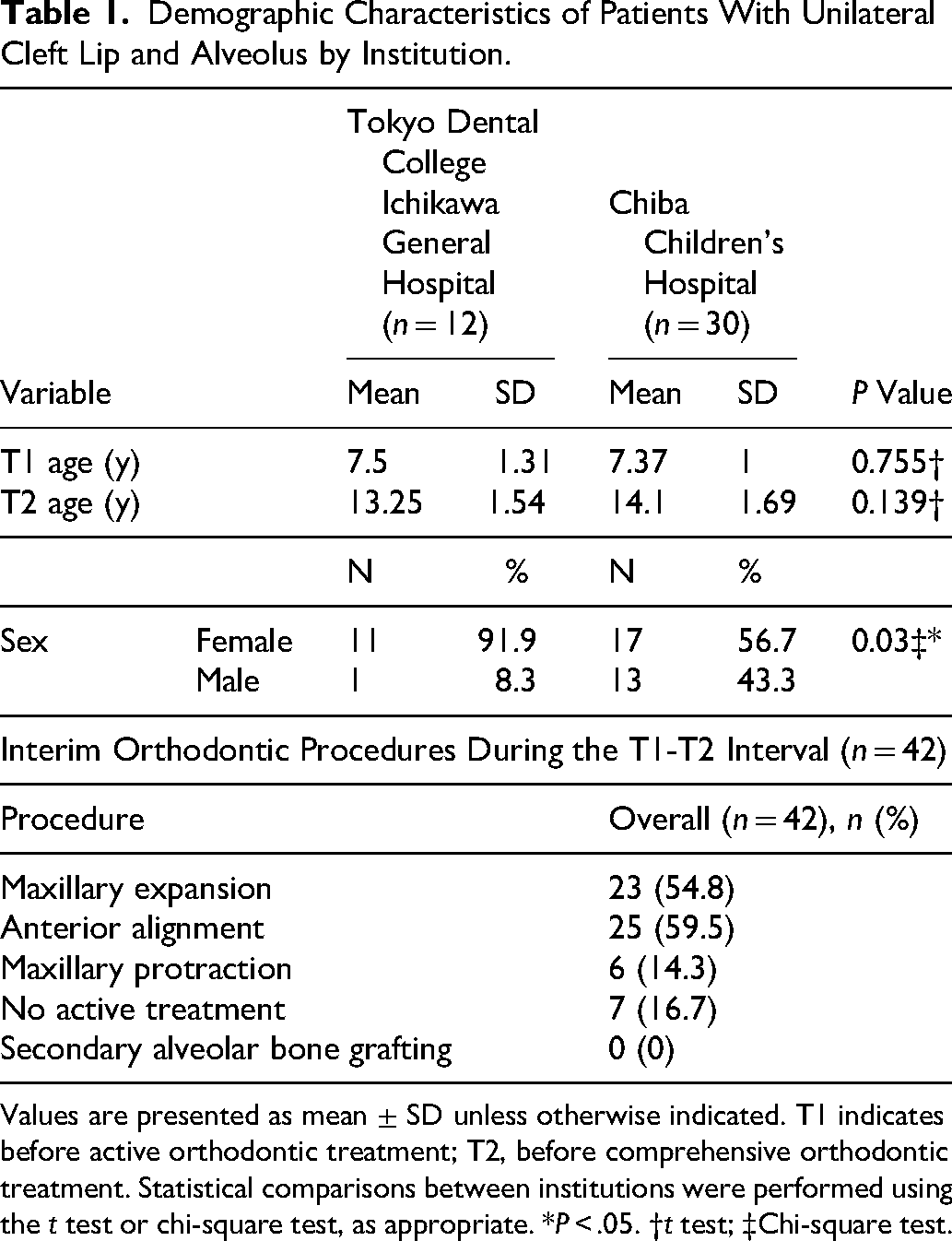
Values are presented as mean ± SD unless otherwise indicated. T1 indicates before active orthodontic treatment; T2, before comprehensive orthodontic treatment. Statistical comparisons between institutions were performed using the t test or chi-square test, as appropriate. *P < .05. †t test; ‡Chi-square test.
Measurement Reliability
To assess measurement reliability, all variables were measured twice by a single examiner with more than 10 years of clinical experience. Ten randomly selected cases were re-evaluated at a 2-week interval. Intra-observer reliability was assessed using intraclass correlation coefficients (ICC), which ranged from 0.88 to 0.94, with a mean ICC of 0.92, indicating excellent reproducibility. Measurement error was calculated using Dahlberg's formula. The errors ranged from 0.19 to 0.29 mm for linear measurements and from 0.20° to 0.41° for angular measurements, indicating acceptable reliability for all variables.
Statistical Power
An a priori power analysis was conducted using G*Power software (version 3.1) to confirm that the available sample size was sufficient to detect clinically meaningful within-subject changes in paired comparisons (assuming a large effect size dz = 0.8, α = 0.05). This analysis was performed to verify the adequacy of the sample size for detecting large, clinically relevant effects, rather than to ensure detection of small regional differences.
Primary Outcomes: Changes in Left-Right Asymmetry
Across all 10 measurements, left-right asymmetry generally tended to shift toward improved symmetry from T1 to T2 under both rest and smile conditions. Descriptive statistics for left-right asymmetry at T1 and T2 are provided in Tables 2 and 3, respectively. Table 2 presents primary descriptive statistics, whereas Table 3 provides complementary analyses for condition-specific patterns. In particular, Measure 2 (Cupid's bow peak—commissure distance) and Measure 6 (lower lip width) demonstrated negative Δ values, indicating a reduction in asymmetry, with moderate effect sizes (dz = 0.39-0.42) (Tables 2 and 3). These reductions were observed consistently under both rest and smile conditions and reached statistical significance in unadjusted analyses (P < .05).
Left-Right Lip Asymmetry at T1 Under Rest and Smile Conditions.
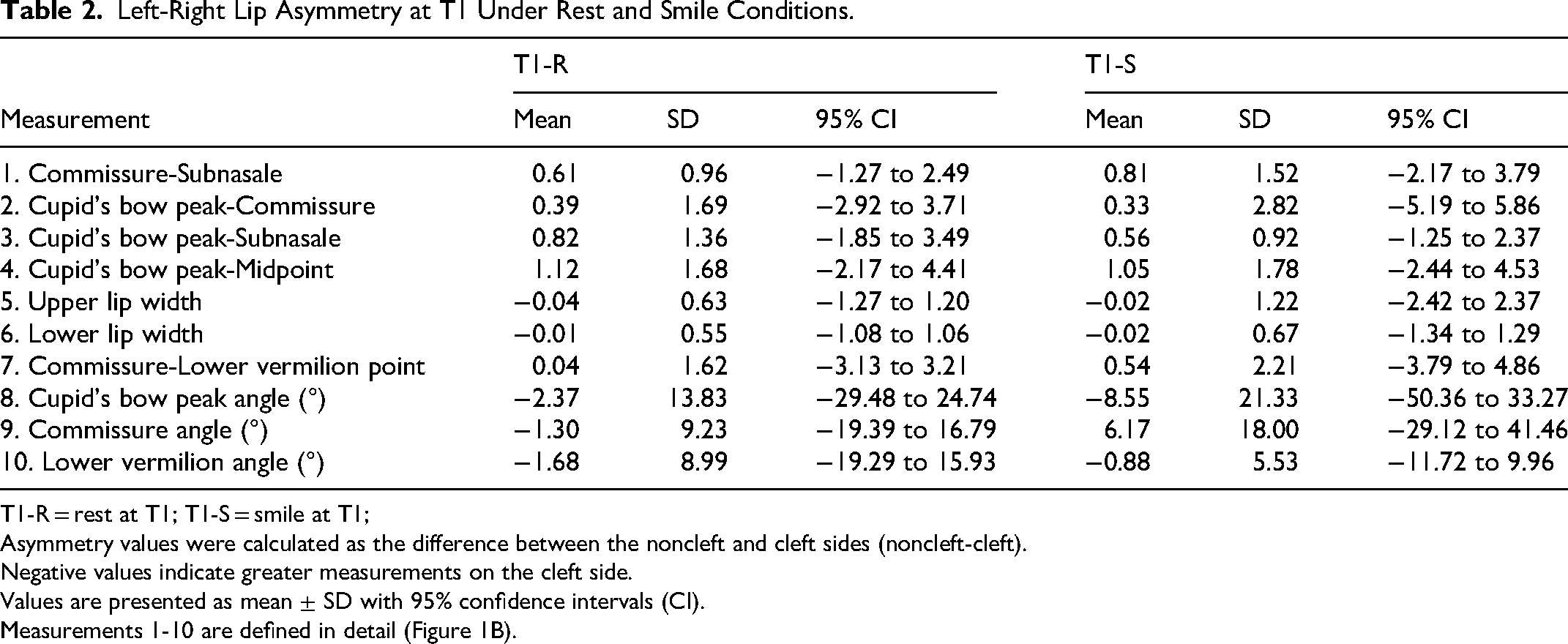
T1-R = rest at T1; T1-S = smile at T1;
Asymmetry values were calculated as the difference between the noncleft and cleft sides (noncleft-cleft).
Negative values indicate greater measurements on the cleft side.
Values are presented as mean ± SD with 95% confidence intervals (CI).
Measurements 1-10 are defined in detail (Figure 1B).
Left-Right Lip Asymmetry at T2 Under Rest and Smile Conditions.
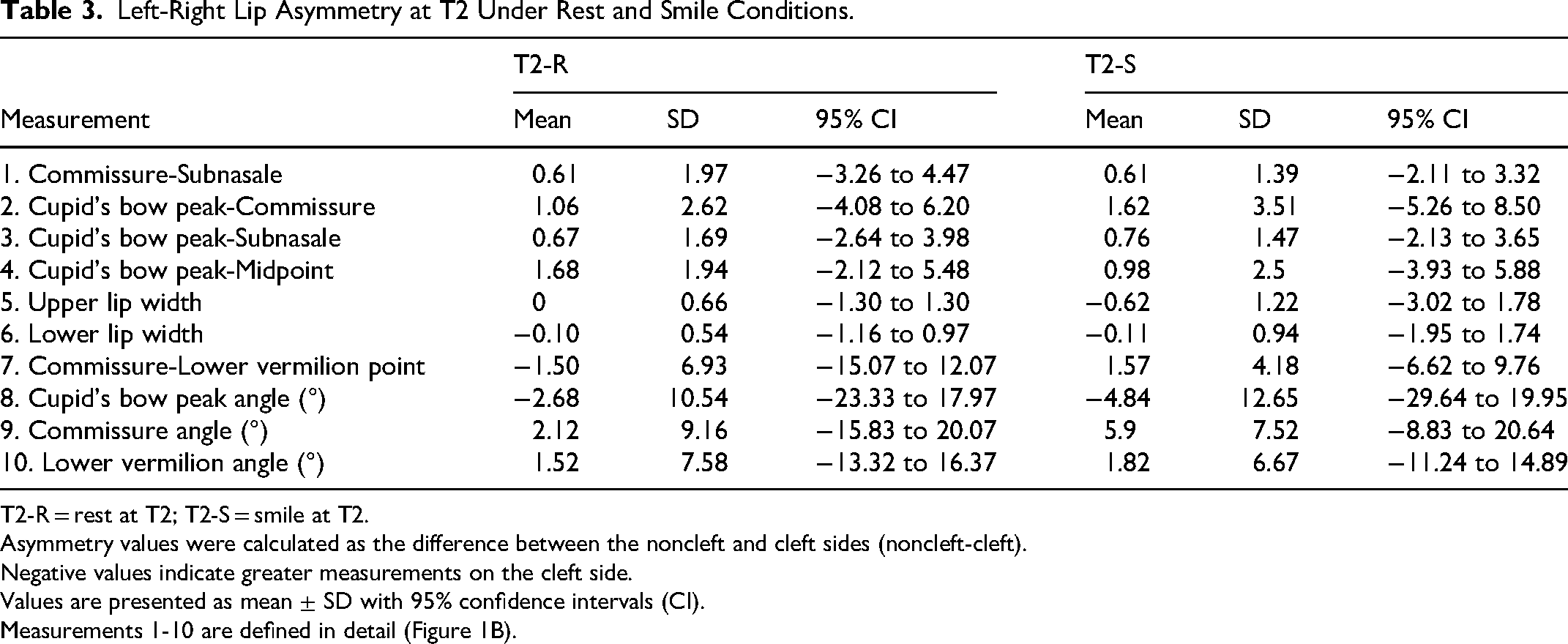
T2-R = rest at T2; T2-S = smile at T2.
Asymmetry values were calculated as the difference between the noncleft and cleft sides (noncleft-cleft).
Negative values indicate greater measurements on the cleft side.
Values are presented as mean ± SD with 95% confidence intervals (CI).
Measurements 1-10 are defined in detail (Figure 1B).
For the remaining measurements, the magnitude of asymmetry reduction was smaller, indicating variability in responsiveness among different lip regions.
After adjustment for multiple comparisons using the Benjamini–Hochberg FDR procedure, none of the comparisons remained statistically significant; however, Measure 2, corresponding to the region around the Cupid's bow, maintained a moderate importance score (−log10(q) × |dz|), reflecting a combination of effect magnitude and statistical robustness (Tables 2 and 3).
Importance Score Analysis and Heatmap Visualization
Heatmaps of importance scores were used to visualize region-specific patterns of longitudinal change across all 10 measurements under rest and smile conditions (Figure 2). Warmer colors represent greater magnitudes of asymmetry change combined with higher statistical robustness. The analysis identified Measure 2 as a consistently high-scoring region across both facial conditions, indicating a relatively pronounced reduction in asymmetry from T1 to T2.
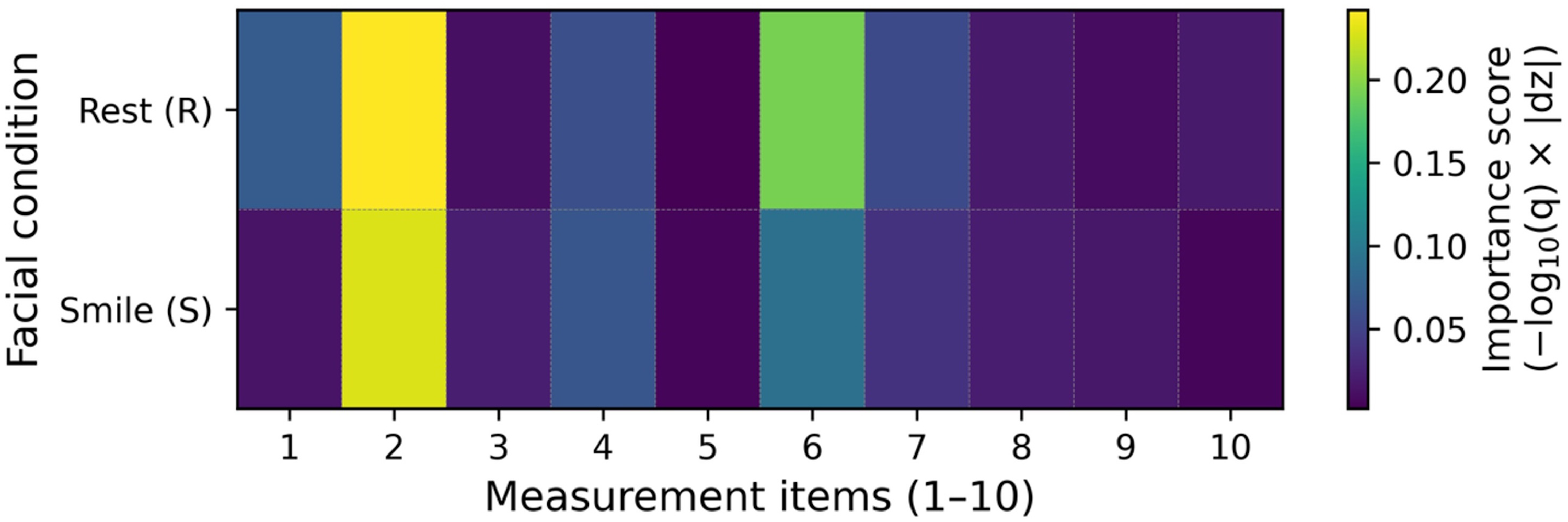
Heatmap visualization of importance scores for longitudinal changes in lip asymmetry. Heatmaps illustrating importance scores for longitudinal changes in left-right lip asymmetry across 10 measurement items under rest (R) and smile (S) conditions. Importance scores were calculated as −log10(q) × |dz|, integrating effect size magnitude (Cohen's dz) and statistical robustness after false discovery rate (FDR) adjustment. Warmer colors indicate greater combined magnitude and reliability of asymmetry change.
Association Between Initial Asymmetry and Longitudinal Change
Using Measure 2 (distance from the peak of the Cupid's bow to the oral commissure) as a representative variable, the relationship between initial asymmetry at T1 and the change in asymmetry from T1 to T2 was examined. A tendency was observed whereby cases with greater asymmetry at T1 exhibited more negative Δ values, indicating larger reductions in asymmetry over time (Figure 3).
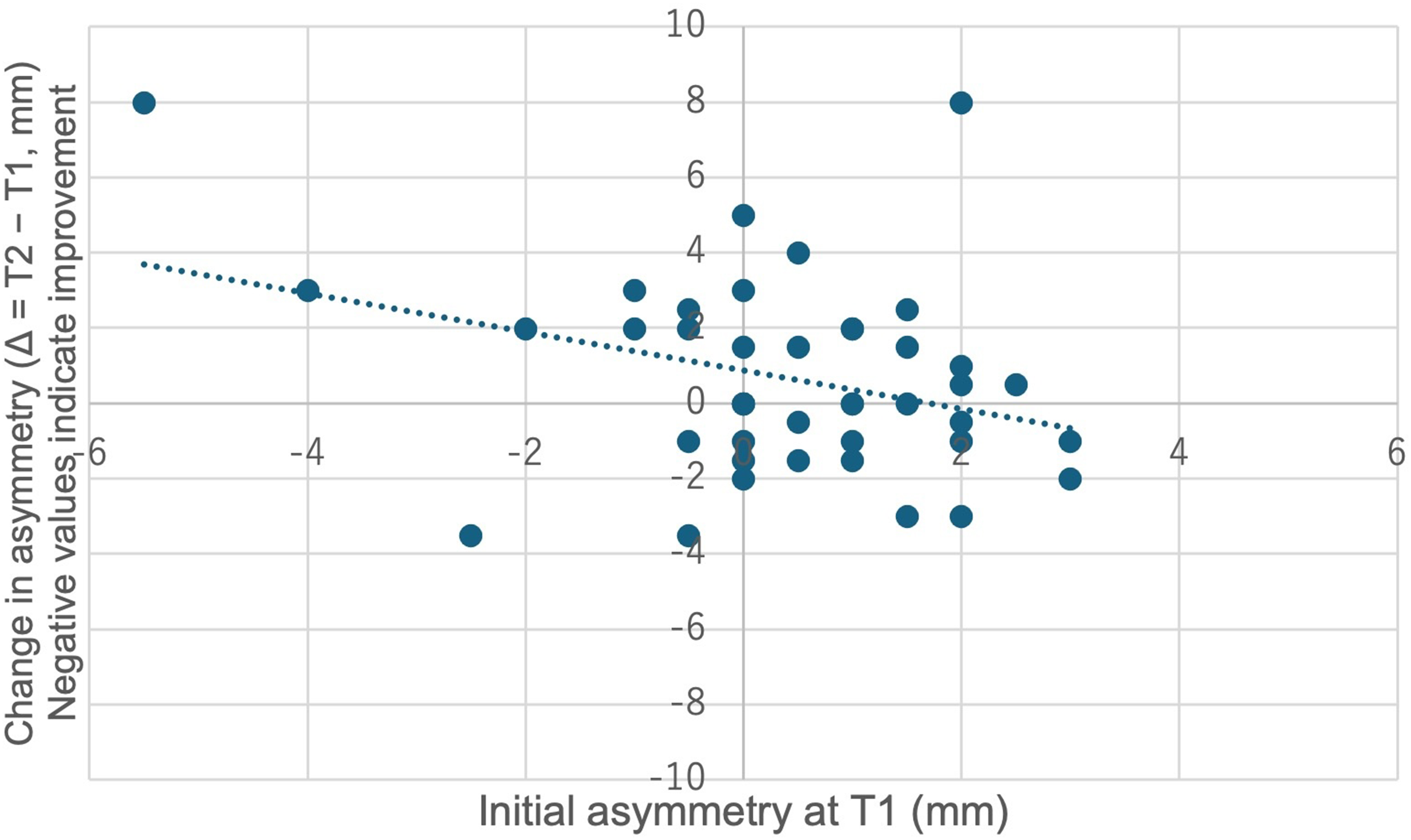
Relationship between initial lip asymmetry and longitudinal change in asymmetry. Scatter plot showing the association between initial asymmetry at T1 and longitudinal change in asymmetry (Δ = T2 − T1) for Measure 2 (distance from the peak of the Cupid's bow to the oral commissure). Each point represents an individual patient. The dashed line indicates the fitted linear regression line.
Simple linear regression analysis demonstrated a weak negative association between initial asymmetry at T1 and Δ (r = −0.33, R2 = 0.11).
Discussion
The present study examined longitudinal changes in lip symmetry in patients with UCLA during the interval between T1 and T2, a period that represents more than simple physiologic growth. Rather, this interval corresponds to a clinically meaningful stage during which orthodontic intervention begins to influence the craniofacial complex. At T1, before the initiation of active orthodontic treatment, alveolar and dental arch asymmetry related to the cleft condition remains largely uncorrected. By contrast, T2 represents the stage before comprehensive orthodontic treatment, during which progressive orthodontic modifications—such as transverse expansion of the alveolar arch, reduction in asymmetry of anterior tooth alignment, and normalization of maxillary arch form—have already occurred. In patients with UCLA, constriction of the cleft-side alveolar segment and distortion of the dental arch are known to exacerbate asymmetrical support of the upper lip. Therefore, reduction in asymmetries in alveolar width and arch form from T1 to T2 may contribute to a more balanced hard-tissue foundation, resulting in enhanced symmetry of the upper lip soft tissues, particularly in the region of the Cupid's bow.7–9,12–14
Although some orthodontic interventions were performed between T1 and T2, these procedures were limited to early interceptive treatments such as maxillary expansion and anterior alignment. Comprehensive orthodontic treatment had not yet been initiated at T2. Therefore, the observed changes likely reflect a combination of early orthodontic intervention and natural growth rather than the effects of comprehensive orthodontic treatment.
The mean age at T1 was 7.4 years, whereas the mean age at T2 was 13.9 years, representing an average observation period of approximately 6.5 years. This relatively long interval allowed evaluation of longitudinal changes in lip symmetry during a critical period of facial growth prior to comprehensive orthodontic treatment.
The observation of a moderate reduction in asymmetry of lower lip width is also noteworthy. Although the lower lip is less directly affected by the cleft itself than the upper lip, it is highly responsive to functional adaptation associated with occlusal relationships and overall dental arch morphology. Orthodontic changes occurring between T1 and T2, including maxillary arch expansion and reduction in asymmetry in anterior tooth alignment, may alter occlusal vertical dimension and perioral muscle activity during lip closure. Such functional adaptations may, in turn, contribute to a reduction in left-right asymmetry of the lower lip. These findings suggest that orthodontic treatment can influence soft-tissue morphology even in regions not directly targeted by surgical intervention, through indirect effects mediated by changes in the dental and occlusal environment.18–23
In addition, analysis focusing on Cupid's bow-related measurements demonstrated a relationship between the magnitude of presurgical asymmetry at T1 and subsequent changes in symmetry from T1 to T2. Specifically, cases with greater initial asymmetry tended to exhibit larger reductions in asymmetry over time. This finding indicates that pronounced presurgical asymmetry does not necessarily predict unfavorable long-term soft-tissue outcomes.7–9,12–14,24
Rather, lip morphology in patients with UCLA appears to retain a degree of plasticity that allows for improvement in lip symmetry under appropriate growth guidance and orthodontic environmental modification. From an orthodontic perspective, this suggests that even patients presenting with marked initial asymmetry may achieve meaningful improvement in lip symmetry when treatment planning adequately considers growth and dentoalveolar development.7–9
Although statistical significance was no longer observed after FDR adjustment, effect size–based evaluation revealed clinically relevant improvements in lip symmetry in specific regions. This highlights the importance of avoiding overreliance on P values alone when interpreting longitudinal morphologic changes, particularly in studies involving multiple correlated measurements. Effect sizes provide complementary information regarding the magnitude of change and may better reflect clinically meaningful reduction in soft-tissue symmetry.25,26
To further integrate statistical robustness and effect magnitude, the present study employed an importance score defined as −log10(q) × |dz|. This composite index enables identification of anatomical regions that demonstrate both relatively large changes and greater statistical reliability. Visualization of these scores using heatmaps facilitated intuitive, region-specific interpretation of treatment-related changes and proved useful for highlighting areas, such as the Cupid's bow, that may be particularly responsive during the orthodontic treatment phase. 27
The findings of this study underscore the need to evaluate lip symmetry in patients with UCLA not solely from a surgical standpoint, but within the broader context of orthodontic treatment and craniofacial growth. The interval between T1 and T2 represents a stage during which orthodontists are deeply involved in treatment planning and intervention. Quantitative assessment of morphologic changes in regions such as the Cupid's bow and oral commissures during this period may provide valuable insight into future esthetic outcomes. Understanding how soft-tissue morphology responds to orthodontic environmental changes allows orthodontists to design treatment strategies that consider not only dental and occlusal objectives but also long-term facial soft-tissue harmony.13,15,17–20
The site- and condition-specific symmetry evaluation framework used in this study may also serve as a shared reference for interdisciplinary communication between orthodontists and plastic surgeons. Such quantitative information could assist in decisions regarding secondary revision surgery and in determining optimal timing for intervention during growth. 15 Although sex distribution differed between institutions, the present study was not powered to evaluate sex-specific effects on longitudinal changes in lip symmetry. Moreover, the primary analyses emphasized intra-individual longitudinal changes rather than between-institution comparisons, thereby reducing the potential impact of baseline demographic imbalance on the overall findings. Variations in primary surgical technique between institutions may represent an additional source of heterogeneity; however, because the present study emphasized intra-individual longitudinal changes rather than comparisons of surgical outcomes, the potential impact of surgical variability on the main findings is likely limited.
Several limitations of this study should be acknowledged. Although the number of analyzed cases was limited to 42, strict inclusion criteria requiring standardized frontal photographs at both T1 and T2 under rest and smile conditions were applied to ensure reliable longitudinal comparisons. First, the analysis was based on two-dimensional frontal facial photographs, and three-dimensional assessment of soft-tissue morphology was not performed. Nevertheless, standardized two-dimensional photographs remain the most widely used assessment tool in routine clinical practice, offering high accessibility and reproducibility without the need for specialized equipment. From a clinical applicability standpoint, the present methodology prioritizes feasibility and relevance to daily practice over maximal measurement precision. Future studies incorporating three-dimensional imaging may further elucidate volumetric and spatial soft-tissue changes and provide a more comprehensive understanding of lip morphology in patients with UCLA.10,11
Conclusions
Initial lip asymmetry at T1 may be associated with the distribution and degree of long-term improvement in lip symmetry in patients with UCLA. Quantitative assessment of site-specific patterns of improvement in lip symmetry during the growth period in which orthodontic intervention is initiated may aid in predicting postoperative growth-related outcomes and in determining the optimal timing for secondary revision procedures.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Department of Orthodontics, Tokyo Dental College, for their clinical support and assistance with data collection.
Ethics Approval
This study was approved by the Ethics Committee of Tokyo Dental College (Approval No. 1211) and was conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
Conceptualization: Y.K., T.Ishii, T.M.; Methodology: Y.K., T.Ishii, T.M., D.A., M.N., M.W., S.Y., A.W., T.S., T.Ishigaki, Y.N.;
Data curation: Y.K., T.Ishii, D.A., M.N., M.W., S.Y., A.W., T.S., T.Ishigaki, Y.N.; Formal analysis: Y.K., T.Ishii, T.M.; Investigation: Y.K., T.Ishii, T.M., D.A., M.N., M.W., S.Y., A.W., T.S., T.Ishigaki, Y.N.; Writing—original draft: Y.K., T.Ishii; Writing—review and editing: Y.K., T.Ishii, T.M., D.A., M.N., M.W., S.Y., A.W., T.S., T.Ishigaki, Y.N.; Supervision: T.Ishii, T.M., M.N., M.W., S.Y., A.W., T.S.; All authors have read and approved the final manuscript.
Funding
This study was supported by research funds from the Department of Orthodontics, Tokyo Dental College.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.