
Abstract
Objective
To determine the prevalence of maxillary third molars developing inferior to the second molars in patients with cleft lip and palate (CLP) and to describe associated clinical and radiographic characteristics.
Design
This retrospective chart review assessed maxillary third molar position using cone-beam computed tomography (CBCT).
Setting
Tertiary cleft and craniofacial center within an academic institution.
Patients/Participants
Patients aged ≥7 years with CLP who underwent CBCT imaging between 2019 and 2025. A total of 104 patients met inclusion criteria (79 unilateral cleft lip and palate (UCLP), 25 bilateral cleft lip and palate (BCLP)).
Interventions
No experimental interventions were performed.
Main Outcome Measure(s)
Prevalence of maxillary third molars positioned inferior to the second molars, defined radiographically by crown position relative to the adjacent second molar. Secondary measures included developmental stage, visibility on 2-dimensional (2D) versus 3-dimensional (3D) imaging, and associated second molar eruption disturbances.
Results
Ectopic third molars were identified in 4 of 104 patients (3.8%), occurring in 3 UCLP and 1 BCLP patient. All ectopic teeth were in early developmental stages (Demirjian A-C), were poorly visible on 2D panoramic reconstructions, and were associated with delayed or failed eruption of the second molar.
Conclusions
Inferior positioning of maxillary third molars is an uncommon but clinically significant eruption disturbance in CLP. When CBCT imaging is obtained for clinical indications in patients with CLP, careful 3D assessment of third molar position may facilitate early identification of ectopic development and help prevent second molar impaction. Further study is needed to optimize timing and indications for early surgical removal.
Introduction
Cleft lip and palate (CLP) is the most common craniofacial anomaly with a prevalence of approximately 1 in 700 live births. 1 Beyond the esthetic and social implications of the condition, individuals with CLP frequently experience functional challenges affecting speech and feeding. 2 Dental and orthodontic manifestations are particularly common and often complicate interdisciplinary treatment planning. These dental anomalies include microdontia, hypodontia, supernumerary teeth, delayed dental development, and tooth impactions.3–5 Such abnormalities contribute to malocclusion and facial asymmetry, impair masticatory efficiency and speech articulation, and affect long-term oral health and psychosocial well-being.
The characteristic CLP pattern of dental disturbances concentrated in the maxillary arch adjacent to the cleft site is due to insufficient mesenchymal tissue and early surgical manipulation disrupting normal dental and skeletal development.6,7 Restricted space and disruption of the nasomaxillary complex contribute to ectopic eruption or impaction of teeth in this region. 8 Accordingly, most of the current literature focuses on the anterior and premolar dentition, especially missing or impacted incisors, canines, and premolars, due to their interference with orthodontic alignment and alveolar bone graft planning. In contrast, posterior dentition, specifically maxillary third molars, have received little attention in the context of CLP.
Third molars are frequently excluded from cleft dental studies because they develop later than the rest of the dentition, show high variability on imaging, and are positioned distant from the cleft site.9,10 Existing studies suggest that third molars in the CLP population frequently exhibit delayed mineralization and a higher prevalence of agenesis compared to non-cleft individuals.11–13 Rare case reports have described ectopic maxillary third molars positioned in locations such as the maxillary sinus or nasal cavity, suggesting that altered maxillary anatomy may influence eruption trajectory.14,15 In our center, we have encountered several patients with CLP who have maxillary third molars which developed directly inferior to maxillary second molars, thereby impacting the second molars. This phenomenon may represent an underrecognized source of dental impaction in patients with CLP which has not been well described in the literature.
Given the importance of maintaining normal second molar eruption for orthodontic and surgical planning, early identification of atypical third molar development is clinically relevant. The purpose of this study was to determine the prevalence of maxillary third molars erupting inferior to the second molars in patients with unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP) and to describe associated clinical and radiographic findings.
Methods
This IRB-approved retrospective chart and radiographic review was conducted at a tertiary cleft and craniofacial center and included patients with CLP who underwent cone-beam computed tomography (CBCT) as part of routine orthodontic evaluation between 2019 and 2025. Inclusion criteria included age 7 or older, confirmed diagnosis of UCLP or BCLP, and a CBCT scan that adequately captured the maxillary third molar region. Patients were excluded if the scan did not visualize the posterior maxilla due to a limited field of view or inadequate image quality to assess third molar development. CBCT images were taken for clinical diagnostic purposes with the following acquisition parameters: field of view 16 × 10 cm, voxel size 0.3 mm, exposure time 3.7 s, 120 kVp, 5 mA. Per our institutional protocol, all patients with CLP undergo CBCT imaging prior to orthodontic treatment due to the potential for impacted or superimposed teeth which would be difficult to view on a 2-dimensional (2D) panoramic radiograph.
All CBCT scans were reviewed in Dolphin Imaging 12.0 by a craniofacial orthodontist experienced in cleft dental assessment. For each patient, demographic information (eg, age, sex, cleft laterality) and radiographic findings were recorded, including the presence or absence of maxillary third molars, developmental stage, and their positional relationship to the maxillary second molars. An ectopic maxillary third molar was defined as a developing or erupted third molar whose crown was positioned inferior to the crown of the adjacent maxillary second molar, with radiographic potential to interfere with normal second molar eruption. Displaced maxillary third molars located in the same axial plane as maxillary second molars were not labeled as ectopic molars. The primary outcome was the prevalence of ectopic third molars positioned inferior to the second molars in UCLP versus BCLP.
Descriptive statistics were performed using RStudio Version 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 104 patients met the inclusion criteria, including 79 patients with UCLP (76%) and 25 patients with BCLP (24%). The mean age at the time of CBCT imaging was 11.1 years (range: 7-19 years), and 53% of the cohort was male. Patients presented for orthodontic records for phase I or phase II orthodontic treatment. Ectopic maxillary third molars positioned inferior to the maxillary second molars were present in 4 of 104 total patients (3.8%). Three of these patients had UCLP (3.8%), and 1 patient had BCLP (4.0%). Patient demographics are shown in
Patient Demographics.
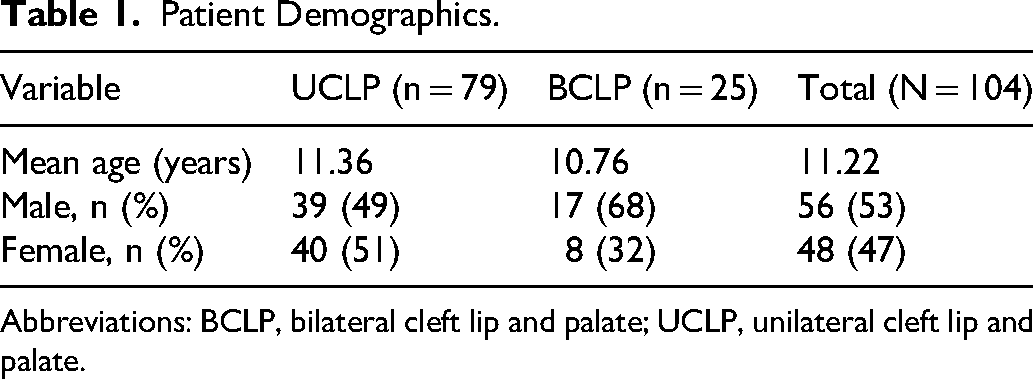
Abbreviations: BCLP, bilateral cleft lip and palate; UCLP, unilateral cleft lip and palate.
Among patients with UCLP, 25 patients (31.3%) were missing both maxillary third molars, 7 patients (8.8%) were missing 1 maxillary third molar, and the remaining 47 patients (59.5%) demonstrated bilateral maxillary third molar development. Among patients with BCLP, 8 patients (32.0%) were missing both maxillary third molars, 2 patients (8.0%) were missing 1 maxillary third molar, and 15 patients (60.0%) demonstrated bilateral maxillary third molar development. Overall, maxillary third molars were radiographically identifiable in 54 patients with UCLP and 17 patients with BCLP. Of which, 4 patients (5.6%) with identifiable third molars had ectopic maxillary third molars positioned inferiorly to maxillary second molars.
Developing third molar buds were more easily visible in the 3-dimensional (3D) rendering of the CBCT and were very difficult to view on the 2D panoramic radiograph extracted from the CBCT. In all cases of ectopic third molars, the third molars were identified during early formation stages, corresponding to Demirjian Stage A-C.
16
These molars were associated with delayed eruption or impaction of the adjacent second molar. Each case was referred for surgical removal of the ectopic third molar. All ectopic cases are shown in
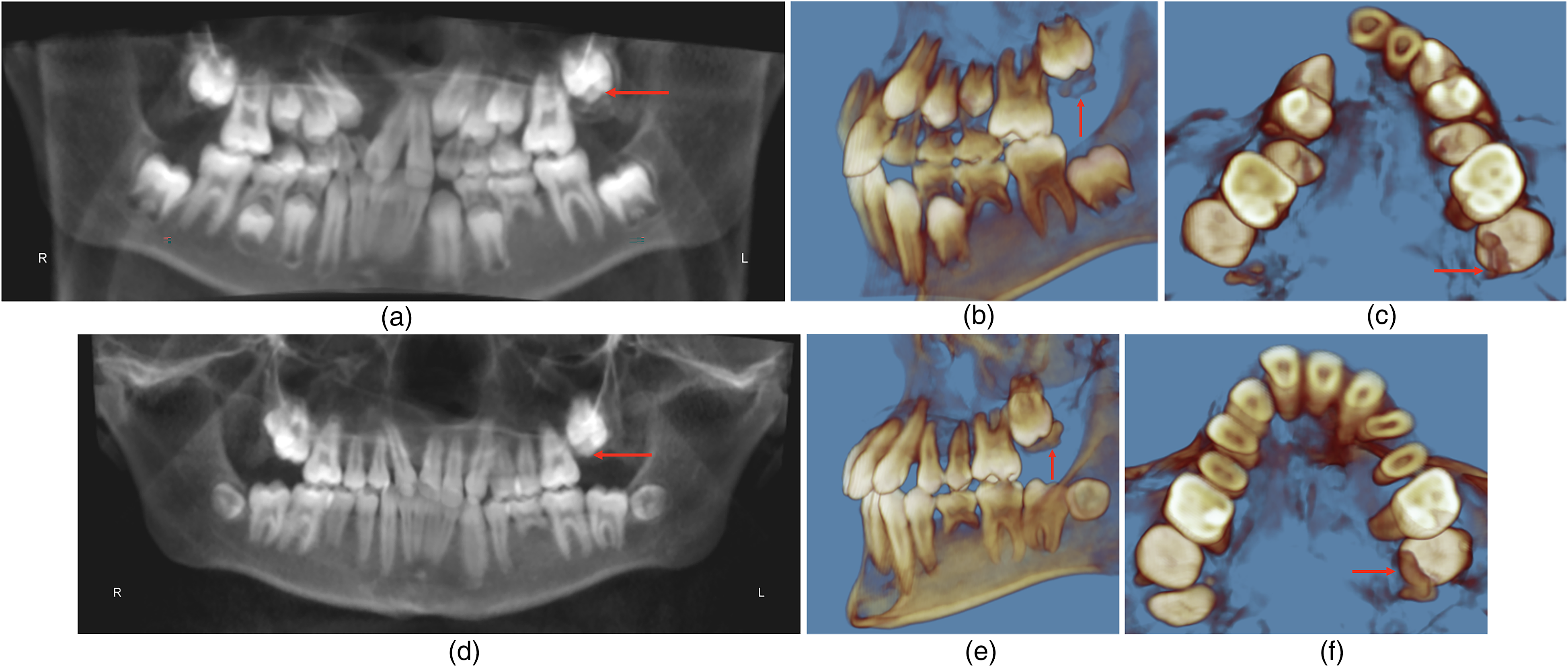
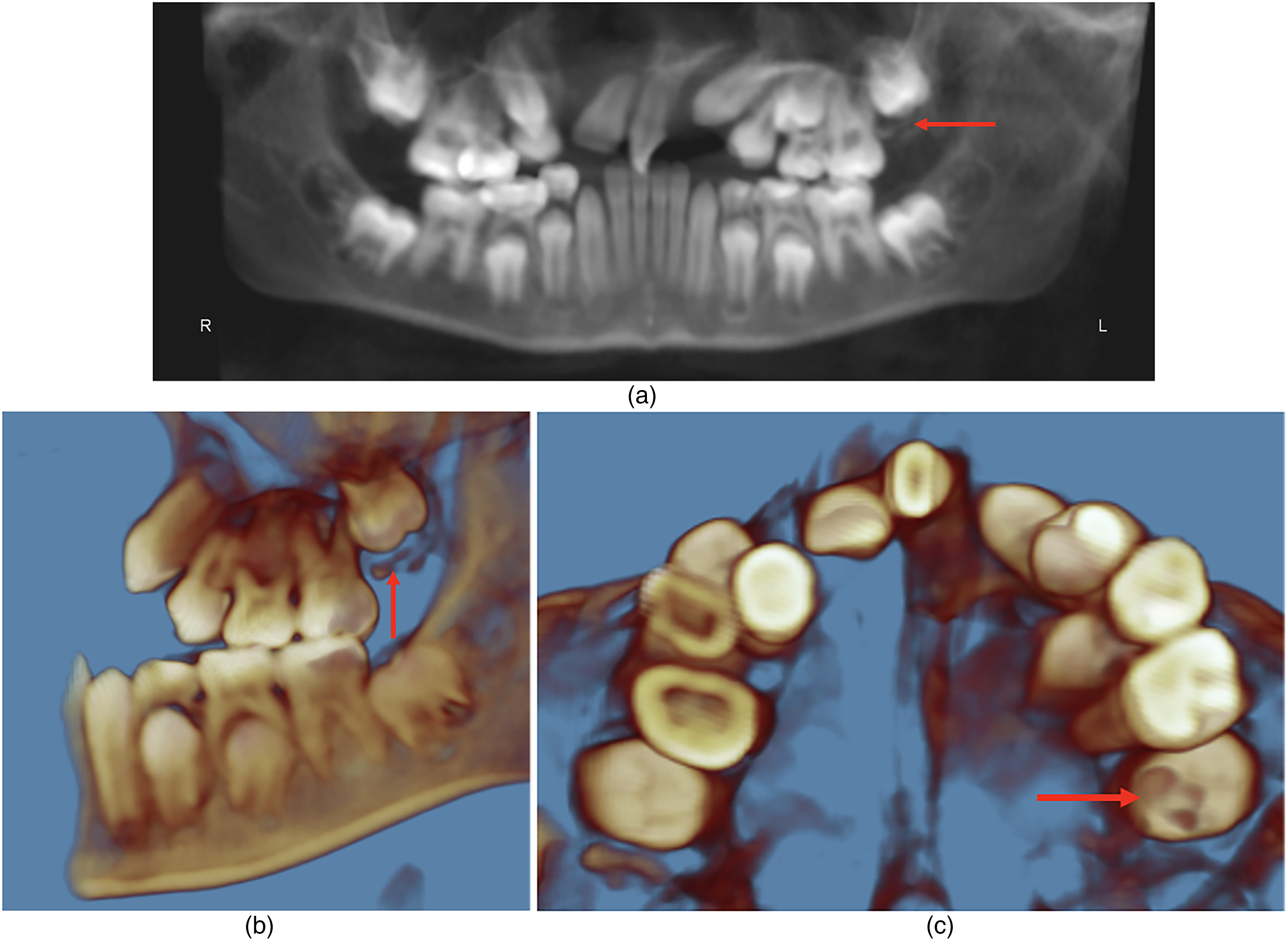
Case 1—(a) panoramic rendering of CBCT, (b) left lateral view, (c) axial view at 9 years 3 months. Note the ectopic maxillary third molars, and the position of the maxillary left third molar inferior to the permanent maxillary second molar. The maxillary third molars were recommended for extraction. (d) Panoramic rendering of CBCT, (e) left lateral view, (f) axial view at 12 years, 11 months. Maxillary third molars were not previously extracted due to difficulty during the surgical procedure. Note that the permanent maxillary left second molar is impacted and is positioned more apically compared to the permanent maxillary right second molar. The patient was referred again for extraction.
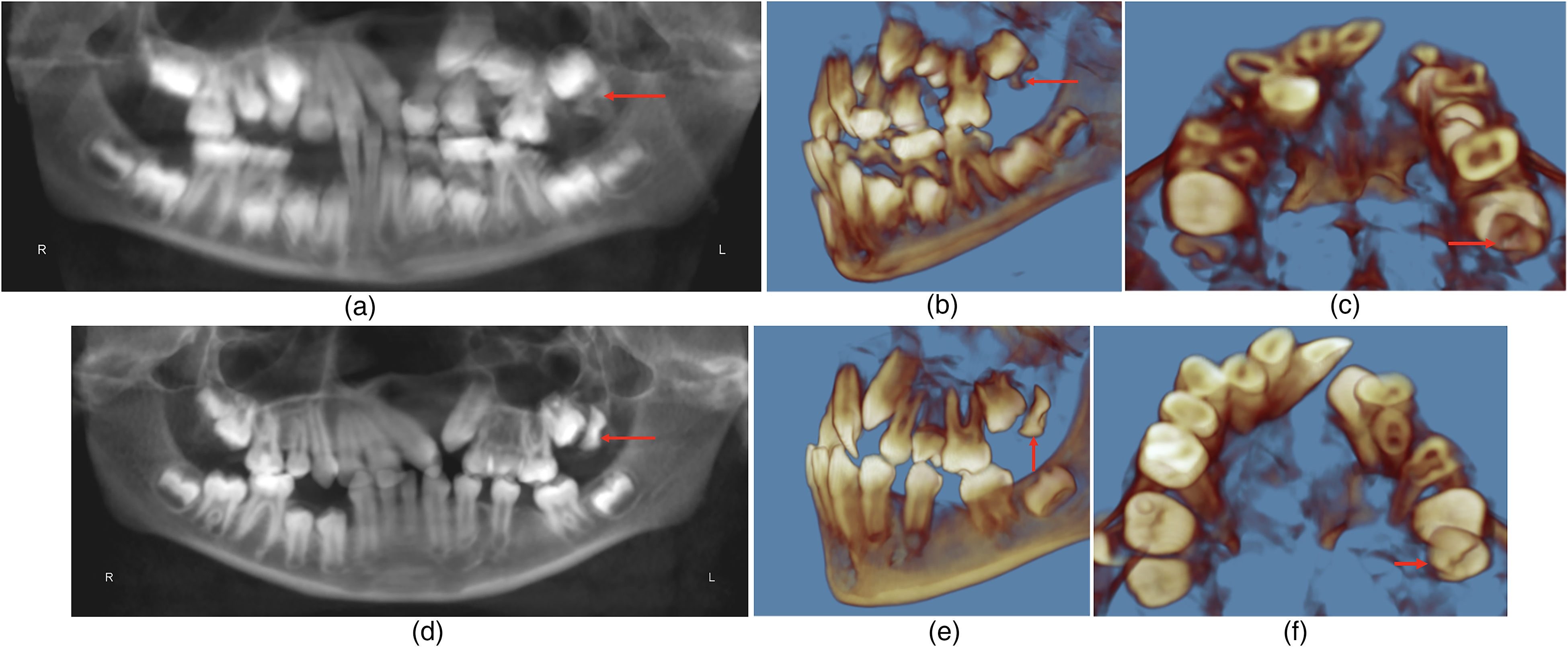
Case 2—(a) panoramic rendering of CBCT, (b) left lateral view, (c) axial view at 9 years, 2 months old. The maxillary left third molar is inferior to the second molar. The patient was referred for extraction of the maxillary left third molar. (d) Panoramic rendering of CBCT, (e) left lateral view, (f) axial view at 11 years, 2 months old. The maxillary left third molar was not extracted due to patient-related factors. Note further development of the maxillary left third molar and impaction and distal angulation of the maxillary left second molar.
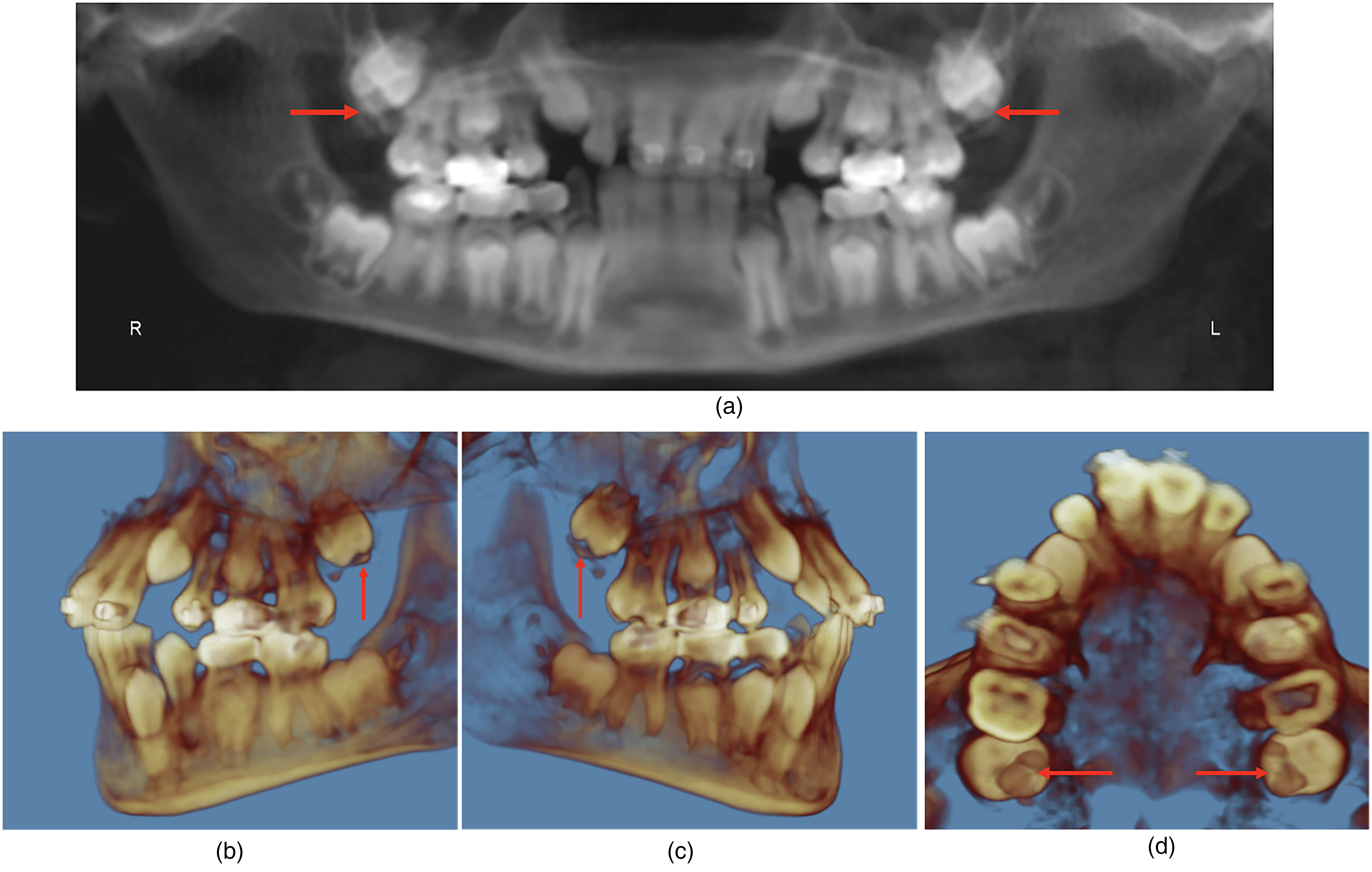
Case 3—(a) panoramic rendering of CBCT, (b) left lateral view, (c) right lateral view, (d) axial view at 10 years, 1 month with bilateral ectopic maxillary third molars impacting the second molars.
Case 4—(a) panoramic rendering of CBCT, (b) left lateral view, (c) axial view at 9 years, 4 months old. The maxillary left third molar is inferior to and impacting the maxillary left second molar.
Characteristics of Patients with Ectopic Maxillary Third Molars Positioned Coronal to the Second Molar.

Abbreviations: BCLP, bilateral cleft lip and palate.
Discussion
This study reports maxillary third molars developing inferior to the second molars in patients with CLP. Among 72 screened patients, we found the prevalence of ectopic third molars to be 5.6%. This is comparably higher than a previous case series reporting the incidence of ectopic third molars in non-cleft patients with a prevalence of 0.16%. 17 Furthermore, there remains a paucity of literature specifically addressing this phenomenon in patients with CLP. In this context, our findings suggest a potentially underrecognized eruption disturbance in patients with CLP, a population already predisposed to maxillary growth and dental development abnormalities. Importantly, the findings in the present study occurred in both patients with UCLP and BCLP at nearly identical rates. Additionally, 3 of the 4 patients had UCLP, yet 2 of those patients demonstrated ectopic molars on the contralateral side of the cleft. This suggests that the occurrence of this anomaly is not dependent on cleft laterality, but rather on cleft-associated maxillary growth disturbances. All ectopic cases were associated with eruption delay and impaction of the adjacent second molar. Additionally, given the young age of many patients in this cohort, third molar development may not yet be radiographically apparent in some individuals, which may underestimate true prevalence.
In patients with CLP, dental anomalies involving the incisors, canines, and premolars have been extensively studied as they play a critical role in cleft management.3–5 In contrast, third molars are frequently excluded from cleft-related dental analyses because they develop later, are distant from the cleft, and are often difficult to detect unless specifically evaluated.9,10,17 This was particularly evident in the present study where in every ectopic case, the maxillary third molars were difficult to visualize on panoramic reconstruction and could only be reliably identified on 3D CBCT. Despite their low prevalence and limited representation in the literature, the clinical consequences of ectopic third molars should not be understated, as their inferior position can directly interfere with normal second molar eruption. Clinicians should therefore specifically assess for ectopic third molars in patients with CLP and should evaluate CBCT imaging in 3 dimensions when available rather than simply viewing a 2D rendering generated from a CBCT, as panoramic reconstructions may obscure early third molar development depending on slice selection. To note, we do not advocate obtaining CBCT imaging solely to evaluate third molar development; however, when imaging is performed for routine cleft care, third molar position should be carefully assessed.
Impaction of the second molar can predispose patients to loss of arch length, tipping or rotation of adjacent teeth, asymmetric eruption, and malocclusion leading to compromised masticatory efficiency.18,19 If the second molar remains unerupted, the dental follicle has the potential for cystic change and may increase caries risk and periodontal inflammation.18,20 Similarly, ectopic third molars have also been associated with increased risk of periodontal disease and dental caries, which is particularly relevant in patients with CLP who already demonstrate elevated susceptibility to oral health complications. Additionally, in CLP treatment sequencing, delayed second molar eruption may also postpone comprehensive orthodontic care and orthognathic preparation. Therefore, early recognition and management of ectopic third molars and secondary impaction of adjacent second molars may offer an additional early intervention opportunity in these complex cases.
We hypothesize this eruption pathway to largely be a consequence of impaired maxillary growth and subsequent decreased arch length. Patients with CLP typically have a smaller maxilla, resulting from a combination of intrinsic maxillary hypoplasia and scarring from early surgical repair.21–24 Reduced maxillary volume leading to crowding and displacement of teeth adjacent to the cleft has been well described in the literature;3,8,25 however, the effects on the pathway of the third molar are less understood. The typical third molar tooth germ originates from the dental lamina and forms posterior to the developing second molar. As crown formation progresses, it mineralizes distally and continues root development through adolescence, eventually erupting into occlusion distal to the second molar. 26 However, in the setting of maxillary hypoplasia, due to a lack of anterior-posterior arch length, the tooth bud may instead initiate mineralization inferior to the unerupted second molar. Because this phenomenon occurs before the second molar erupts, the third molar occupies the second molar's eruption path, leading to delayed eruption or impaction.
Surgical management of a third molar positioned inferior to the second molar typically requires extraction, but removal during early development poses unique challenges. The first barrier to extraction is the limited access to the ectopic third molar. Due to the confinement of the surgical field, visualization of the tooth is restricted, and instrument angulation is often limited making it difficult to create a pathway for removal. Thus, bone removal is often necessary during third molar extraction to gain proper access. 27 Bone removal is typically performed over the occlusal aspect of the tooth and along the buccal bone adjacent to the crown. Only enough bone should be removed to provide visibility and access to perform sectioning. 27
Surgical extraction of the immature third molar may also damage the follicle of the developing second molar. 28 The dental follicle is a layer of loose connective tissue surrounding the developing tooth. It contains stem cells that eventually differentiate into osteoblasts, cementoblasts, and periodontal fibroblasts, which form the alveolar bone, cementum, and periodontal ligament. During tooth eruption, the dental follicle initiates resorption of bone to create an eruption pathway. 29 Surgical disruption of the second molar follicle can result in impaction of the second molar or lead to other eruption anomalies. Previous animal studies have shown surgical removal of the dental follicle to impair root elongation and eruption. 30 Alternative management strategies may be considered depending on patient age, degree of displacement, and second molar development. These include delayed extraction of the third molar to allow further maturation of the second molar, orthodontically guided eruption of the second molar following third molar removal, and, in severe cases of second molar displacement, extraction of the second molar.
These factors underscore the importance of long-term radiographic monitoring in cleft populations and careful surgical planning when intervention becomes necessary, especially when ectopic development is identified early. To optimize patient care, the treatment team should keep in mind the several considerations. The risks of early extraction should be discussed with the patient during the initial consultation, emphasizing the limited surgical access and potential for injury to the developing second molar. Due to the physical restrictions, there exists no definitive timeline for the optimal age for extraction. Effective coordination between orthodontists and surgeons is essential for identifying the optimal extraction timing for each patient, thus balancing the need to prevent second molar impaction with the importance of avoiding the surgical risks associated with removing third molars too early.
Limitations
This study is limited by its retrospective design performed at a single institution and the small number of ectopic cases. The rarity of these findings limits statistical power; however, the aim of this study was to establish prevalence and describe the radiographic pattern, not to demonstrate causation. Additionally, although all CBCT scans were obtained using a standardized institutional protocol, minor variability in image appearance was observed, likely reflecting patient-related factors such as positioning or movement rather than differences in imaging technique. Future studies with larger, multicenter cohorts are needed to further characterize the prevalence and natural history of ectopic third molars in patients with CLP and to help establish evidence-based management algorithms incorporating patient age, degree of impaction, and second molar development.
Conclusion
In summary, inferior positioning of maxillary third molars is a rare but clinically meaningful eruption disturbance in patients with CLP. Because third molar development is highly variable, clinicians should evaluate third molar position in patients with CLP to diagnose ectopic third molars in a timely fashion and prevent second molar impaction. In our cohort, ectopic third molars were identifiable on the 3D view of the CBCT and were difficult to view on a 2D rendering, emphasizing that routine 2D imaging may fail to reveal this anomaly. Early recognition is critical, as the inferior third molar position occupies the eruption path of the second molar and can result in delayed eruption or impaction. Surgical management is often necessary; however, early surgical removal of the maxillary third molar may need to be postponed because of the risks of damaging the second molar or surrounding alveolar structures. Clear and consistent communication between orthodontists and surgeons is critical to establish the most appropriate extraction timing for each patient.
Footnotes
Acknowledgements
Not Applicable
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (no. IRB00530344) on November 5, 2025.
Consent to Participate
Not Applicable.
Consent for Publication
Not Applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data supporting the findings of this study are not publicly available, but may be shared upon reasonable request.