
Abstract
Objective
To compare dentoskeletal, nasal septal, and upper airway changes following rapid maxillary expansion (RME) using Hyrax and fan-type expanders in growing patients with cleft lip and palate (CLP) using cone-beam computed tomography (CBCT).
Design
Prospective comparative clinical study.
Setting
University-based tertiary care dental institution.
Patients
Twenty patients aged 9 to 15 years with repaired unilateral or bilateral CLP and transverse maxillary deficiency.
Interventions
Participants were treated with bonded Hyrax (n = 10) or fan-type expanders (n = 10) according to maxillary constriction pattern. CBCT scans were obtained before expansion (T0) and after a 3-month retention period (T1).
Main Outcome Measures
Anteroposterior, vertical, and transverse dentoskeletal parameters, nasal septum deviation, and oropharyngeal airway volume were evaluated. Intragroup comparisons used the Wilcoxon signed-rank test; intergroup comparisons used the Mann-Whitney U test (P < .05).
Results
Both appliances achieved significant transverse expansion. The fan-type expander showed greater anterior basal widening, whereas the Hyrax demonstrated greater posterior expansion and nasal cavity width increase. Airway volume increased but was not statistically significant.
Conclusions
Both expanders effectively correct transverse maxillary deficiency in CLP patients. Appliance selection should be based on constriction pattern. Airway effects appear limited.
Keywords
Introduction
Cleft lip and/or palate (CLP) is among the most frequent congenital craniofacial anomalies, with a reported global prevalence of approximately 1 in 700 live births, accounting for more than 65% of congenital craniofacial disorders. 1 Disruption of fusion between the maxillary and medial nasal processes and failure of palatal shelf union during weeks 4 to 12 of gestation result in discontinuity of the lip and/or palate, arising from complex multifactorial genetic and environmental interactions.1,2 Genetic susceptibility, gene-environment interactions, and epigenetic factors have been implicated in the etiopathogenesis of CLP.2–4
Epidemiological studies demonstrate considerable geographic and ethnic variation in the prevalence of CLP. 5 In the Indian population, Reddy et al. reported an incidence of 1.09 per 1000 live births in the state of Andhra Pradesh, highlighting CLP as a significant public health concern in South India. 6 Similar regional studies underscore the burden of cleft anomalies in developing countries.5,6
CLP is associated with a wide spectrum of functional, esthetic, and psychosocial impairments, including feeding difficulties, speech disorders, recurrent otitis media with hearing impairment, facial esthetic concerns, and compromised quality of life.1,7,8 These challenges necessitate long-term multidisciplinary management, with orthodontic intervention playing a critical role in restoring maxillary form and function during growth.9,10
Surgical repair of cleft lip and/or palate, although indispensable for restoring function and facial continuity, has been shown to adversely influence maxillary growth, particularly in the anterior region.10–12 Early primary lip and palate surgeries may lead to scar tissue formation across the maxilla and palatal shelves, restricting forward and transverse maxillary development.10–12 This growth inhibition commonly manifests as maxillary hypoplasia, transverse maxillary deficiency, and a high prevalence of skeletal Class III malocclusion.11–13 Maxillary constriction is often associated with posterior crossbite, crowding, dental anomalies, and reduced nasal and oropharyngeal airway dimensions, predisposing to respiratory disturbances.11,14 Consequently, rapid maxillary expansion (RME) is a key component of early orthodontic management.10,11
Longitudinal and cross-sectional studies have demonstrated reduced Sella-Nasion-Point A (SNA) values, deficient maxillary length, and altered craniofacial growth patterns in surgically repaired cleft patients compared with non-cleft individuals.10–12,14 The anterior maxilla is particularly vulnerable due to surgical manipulation during lip repair and palatoplasty.11,12
The severity of maxillary growth restriction is influenced by timing and technique of surgery, extent of cleft, and the number of surgical interventions.10–12,14 Consequently, orthodontic problems such as posterior crossbite, crowding, and sagittal discrepancies are frequently observed during mixed dentition, necessitating early orthopaedic intervention.11,15
Multiple expansion appliances have been used in cleft patients. Quad Helix appliances provide gradual anterior expansion,1,14,16 Haas expanders produce skeletal expansion but may be associated with dental tipping and hygiene challenges,17,18 while Hyrax expanders offer relatively uniform anteroposterior expansion.11,19,20 Fan-type expanders preferentially increase anterior maxillary width and are useful in cases with predominant anterior constriction.21–24
Cone-beam computed tomography (CBCT) enables accurate three-dimensional evaluation of dentoskeletal structures, nasal septum, and airway and is increasingly used to assess RME effects in CLP.11,20,25 However, comparative CBCT data evaluating Hyrax versus fan-type expanders particularly regarding nasal septum deviation and oropharyngeal airway volume remain limited.11,23,24
Therefore, this prospective CBCT study aimed to evaluate and compare dentoskeletal changes, nasal septum deviation, and upper airway modifications following RME using bonded Hyrax and fan-type expanders in growing patients with cleft lip and palate.
Materials and Methods
Study Design and Ethical Approval
This prospective comparative clinical study was conducted in the Department of Orthodontics in collaboration with the Department of Oral and Maxillofacial Surgery at Drs Sudha and Nageswara Rao Siddhartha Institute of Dental Sciences, Chinaoutpalli, Gannavaram. Ethical approval was obtained from the Institutional Ethics Committee, and the study was conducted in accordance with the Declaration of Helsinki and the CONSORT 2010 guidelines.26,27 Written informed consent was obtained from the parents or guardians of all participants.
Study Population
The study population comprised 20 growing patients aged 9 to 15 years with repaired CLP presenting with transverse maxillary deficiency requiring expansion. Of the 20 participants, 12 presented with unilateral cleft lip and palate and 8 with bilateral cleft involvement. All patients had previously undergone primary lip repair in infancy and palate repair within the first year of life in accordance with established institutional cleft management protocols. Maxillary expansion was performed during the mixed dentition phase as part of routine interdisciplinary cleft care. Detailed surgical histories were reviewed from clinical records prior to enrolment to ensure uniformity in treatment background and eligibility. Participants were recruited using a nonprobability purposive sampling technique with consecutive enrolment of eligible patients.
Eligibility Criteria
Inclusion Criteria
Patients aged 9 to 15 years in the mixed dentition stage
Repaired unilateral or bilateral cleft lip and palate
Presence of transverse maxillary deficiency
Cervical vertebral maturation stages CS1-CS4
No prior maxillary expansion therapy
Exclusion Criteria
Syndromic clefts
History of previous orthodontic expansion
Craniofacial anomalies other than cleft lip and palate
Medically compromised patients
Sample Size Estimation
An a Priori sample size estimation was performed using G*power Software Version 3.1.9.4 (Franz Faul, Universität Kiel, Germany). Based on an independent comparison between two groups (Hyrax and fan-type expanders), assuming a moderate-to-large effect size (Cohen's d = 0.80), an alpha level of 0.05, and a statistical power of 80%, the required sample size was calculated as 10 subjects per group. Accordingly, a total of 20 subjects (10 per group) were included in the study.
Due to limited patient availability, the final sample was restricted to 20 subjects (10 per group).11,20,23
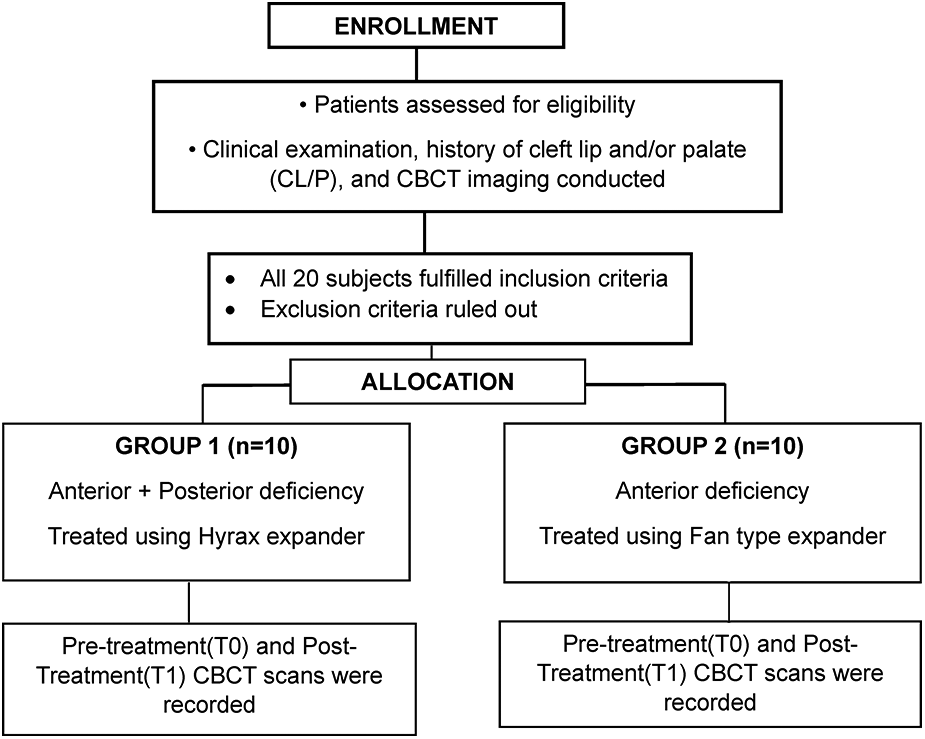
Recruitment, Allocation, and Grouping
Participants were allocated based on maxillary deficiency pattern:
Group I (Hyrax; n = 10): Combined anterior and posterior constriction Group II (Fan-type; n = 10): Predominantly anterior constriction
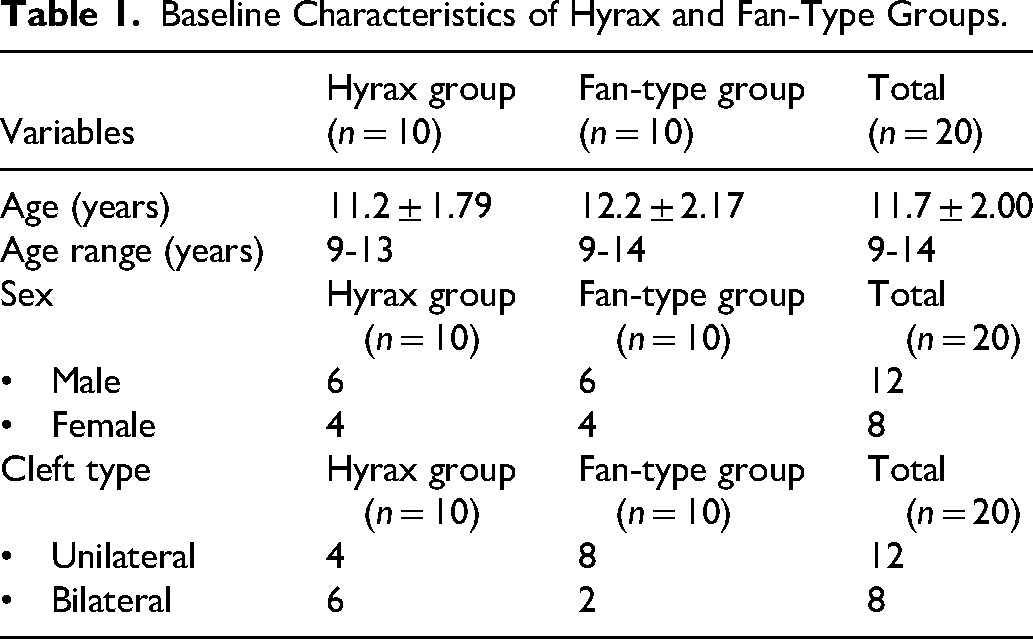
Random allocation was not performed, as appliance selection was based on anatomical requirements.11,15 The baseline demographic and clinical characteristics of the study participants are presented in Table 1.
Appliances and Expansion Protocol
Maxillary expansion was performed using standardized activation protocols until the required transverse correction was achieved. Following completion of active expansion, the appliances were maintained in situ as passive retainers for a 3-month stabilization period.
The Hyrax expanders consisted of a midpalatal jackscrew incorporated within an acrylic-supported stainless-steel framework.11,17 The fan-type expanders were designed with a posterior hinge mechanism to facilitate differential expansion, allowing greater anterior transverse widening. 21
Activation was initiated 24 h after appliance placement and performed twice daily (0.5 mm per day) for approximately 2 weeks, in accordance with Timms’ protocol. 18 After the active expansion phase, the appliances were retained passively for 3 months to allow stabilization of the skeletal changes.11,17
CBCT Acquisition and Orientation
CBCT scans were obtained at two standardized time points:
T0: Pre-expansion CBCT obtained prior to initiation of active maxillary expansion. T1: Post-expansion CBCT obtained after completion of the active expansion phase (approximately 2 weeks), followed by a standardized 3-month retention period.
The interval between T0 and T1 CBCT scans was therefore approximately 3 months.
All CBCT scans were obtained using standardized head positioning and consistent imaging parameters. Skeletal, nasal, septal, and airway measurements were performed using dedicated three-dimensional imaging software based on predefined anatomical landmarks.
CBCT images were acquired at two time points: T0 (pretreatment) and T1 (following a 3-month retention period) using a CS 9600 unit (Carestream Dental) operating at 90 kV, 120 mA, with a 17-s exposure time and a voxel size of 0.3 mm. Image reconstruction and analysis were performed using CS 3D Imaging software.
Standardized orientation was achieved by:
Aligning the axial plane with the right and left frontozygomatic sutures on frontal view. Aligning the axial plane with the Frankfort horizontal (FH) plane on right lateral view. Aligning the midsagittal plane along the line from crista galli to basion on superior view.
Measurements11,20,25
All measurements were derived from standardized CBCT reconstructions.
Sella-Nasion-Point A angle measured on lateral cephalograms reconstructed from CBCT (Figure 1).
Frankfort Horizontal-Anterior Nasal Spine (FH-ANS): linear distance from the Frankfort Horizontal (FH) plane to the Anterior nasal spine (ANS) on sagittal slices (Figure 2).
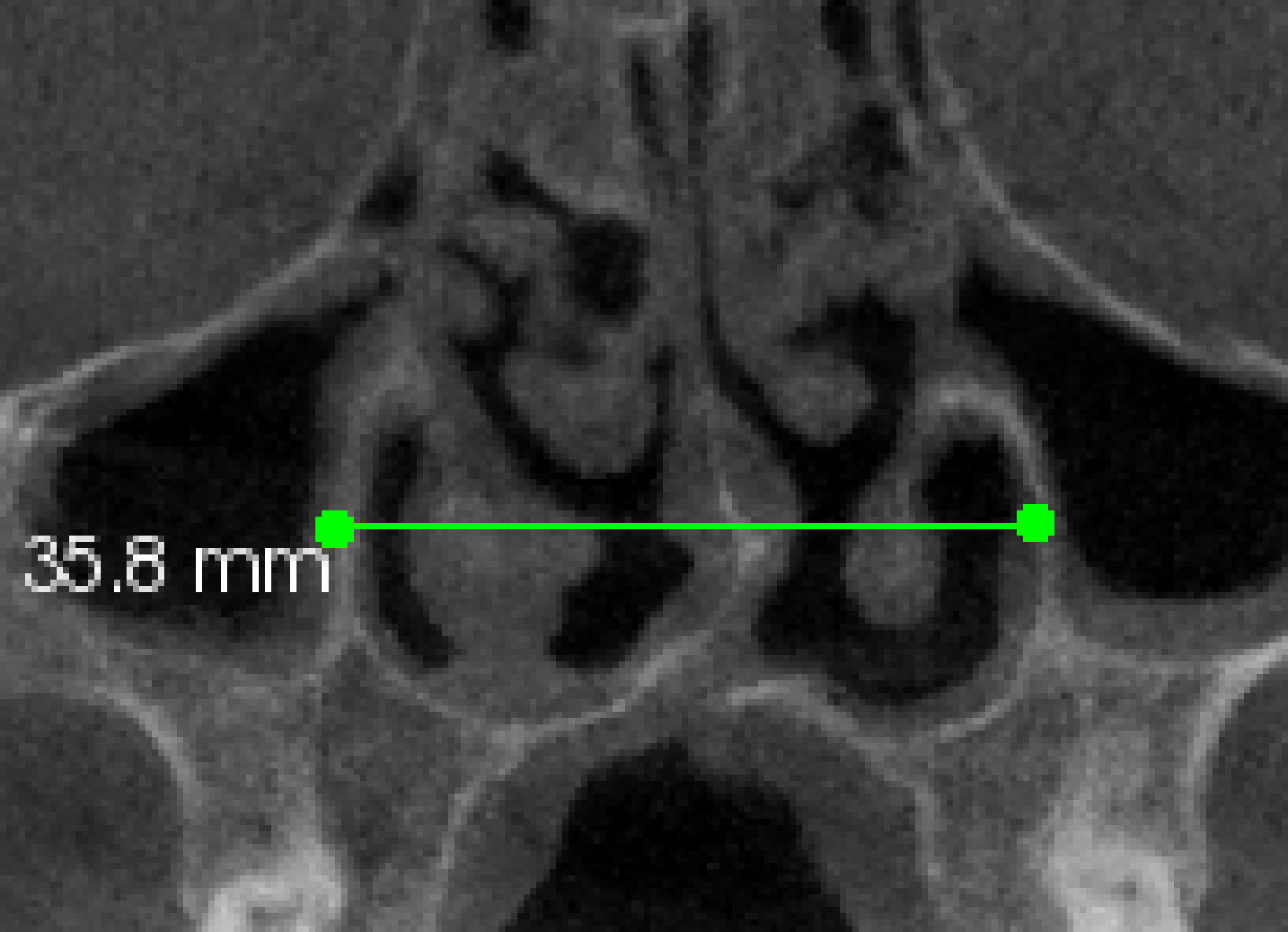
Anterior maxillary basal width (At-MBW): distance between midpoints of palatal roots of right and left first premolars at the level where divergence begins (Figure 3). Posterior maxillary basal width (Pt-MBW): distance between midpoints of palatal root bifurcations of right and left first molars (Figure 3). Nasal cavity width (NCW): distance between the widest points of the right and left lateral nasal walls along a horizontal line parallel to the floor on coronal slices (Figure 4). Dental tipping: angle between a line perpendicular to the axial plane through the root apex and a line from palatal cusp tip to palatal root apex of posterior teeth, measured on cleft and noncleft sides (Figure 5).
Midline angle (MLA): angle between the midsagittal plane (crista galli to anterior contour of foramen magnum) and a line from crista galli to the apex of septal deviation (Figure 6). Distance of the most-deviated point of the nasal septum to the midsagittal plane (DMDP): linear distance from the midsagittal plane to the most deviated point of the septum (Figure 6).
The superior boundary of the oropharyngeal airway was defined by the nasal floor plane through the posterior nasal spine (PNS), parallel to FH; the middle and inferior boundaries were planes through the soft palate tip and the base of the epiglottis, respectively; the anterior boundary was the posterior nasal plane perpendicular to FH and the midsagittal planes. Total oropharyngeal airway volume was calculated by semi-automated segmentation using axial slices; airway length was measured from PNS to the lowest border of C2 (Figure 7).
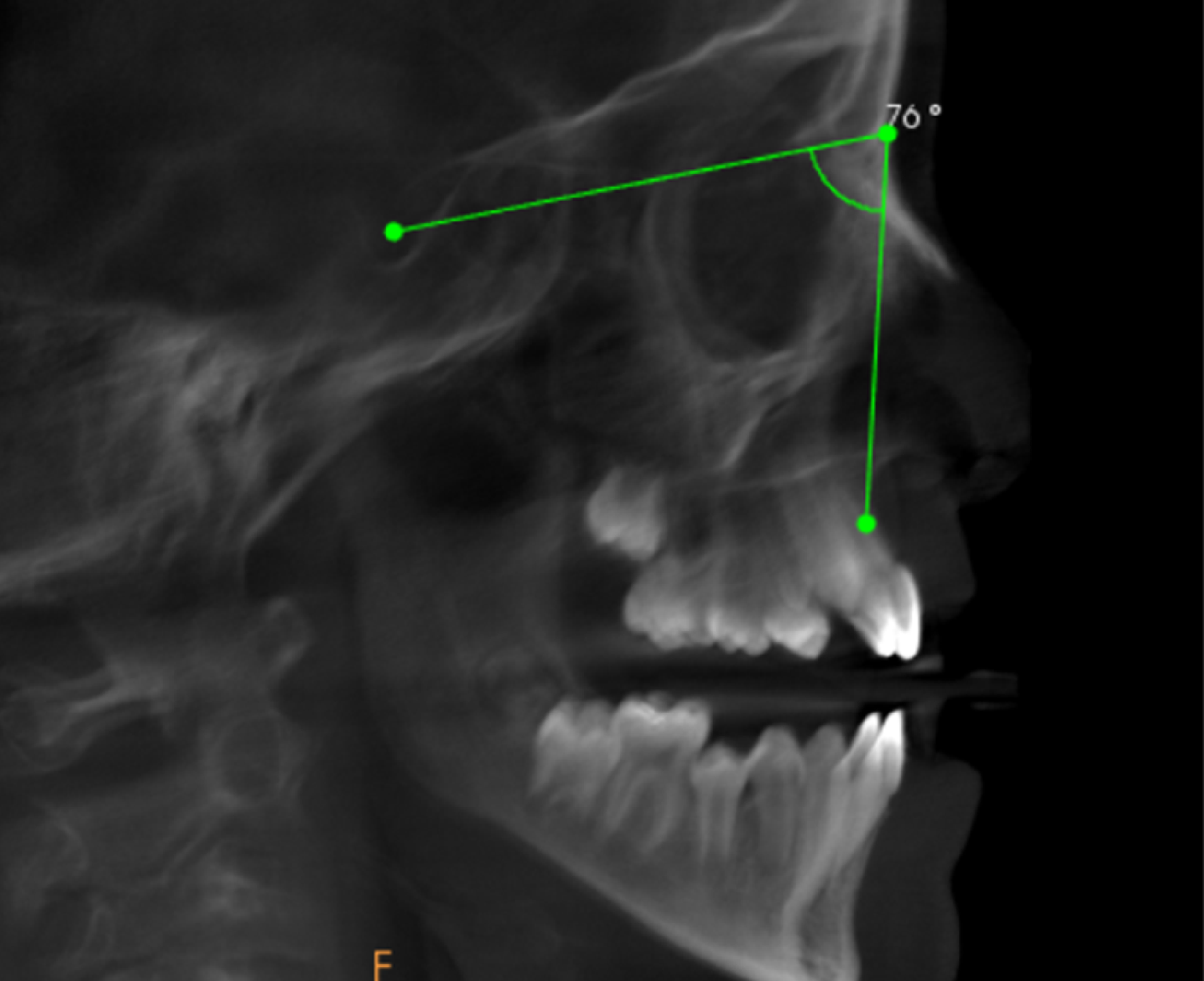
Measurement of SNA angle on CBCT-reconstructed lateral cephalogram.
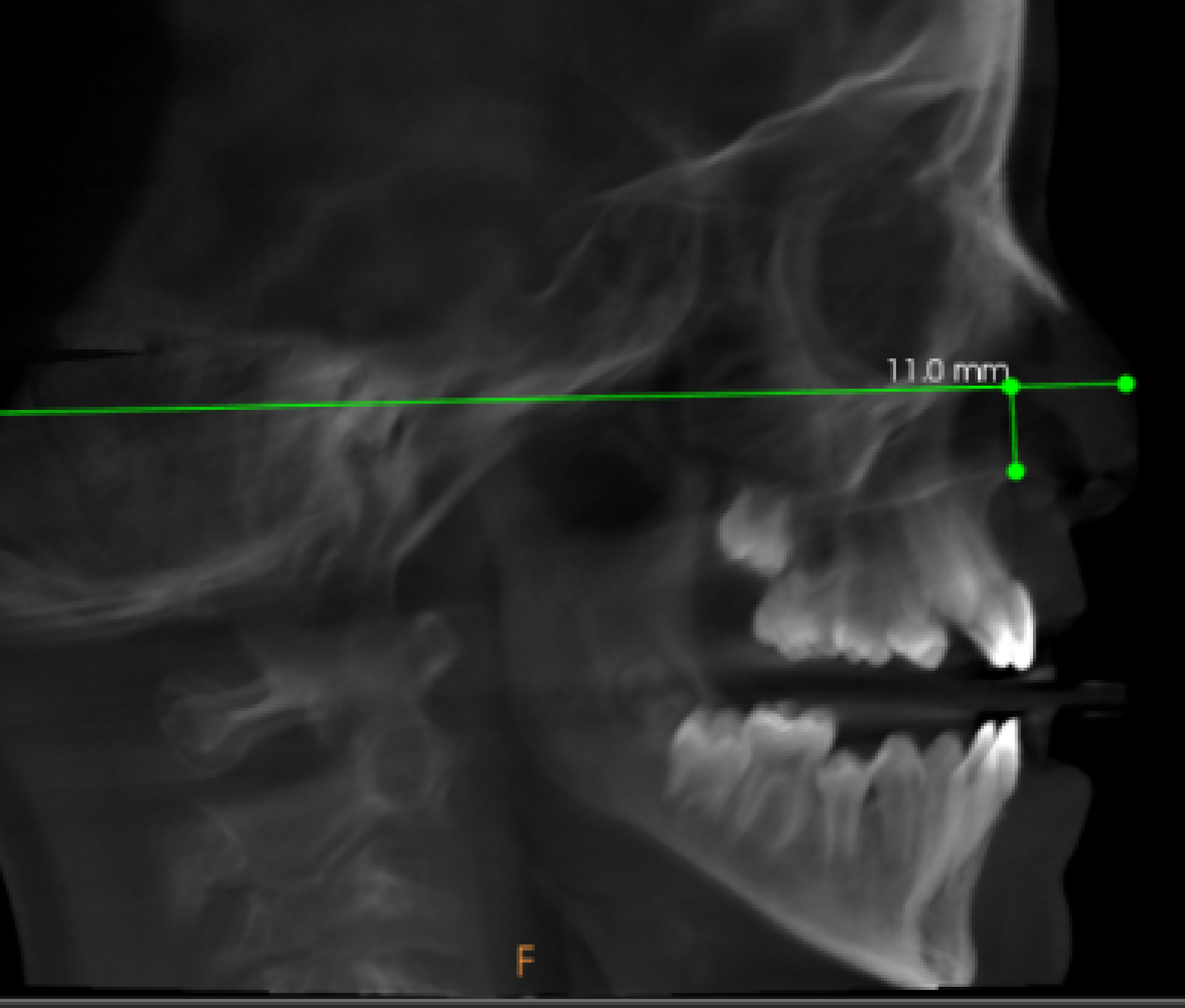
Measurement of FH–ANS linear distance on sagittal CBCT section.

Measurement of anterior maxillary basal width (At-MBW) and posterior maxillary basal width (Pt-MBW).
Measurement of nasal cavity width (NCW) on coronal CBCT section.
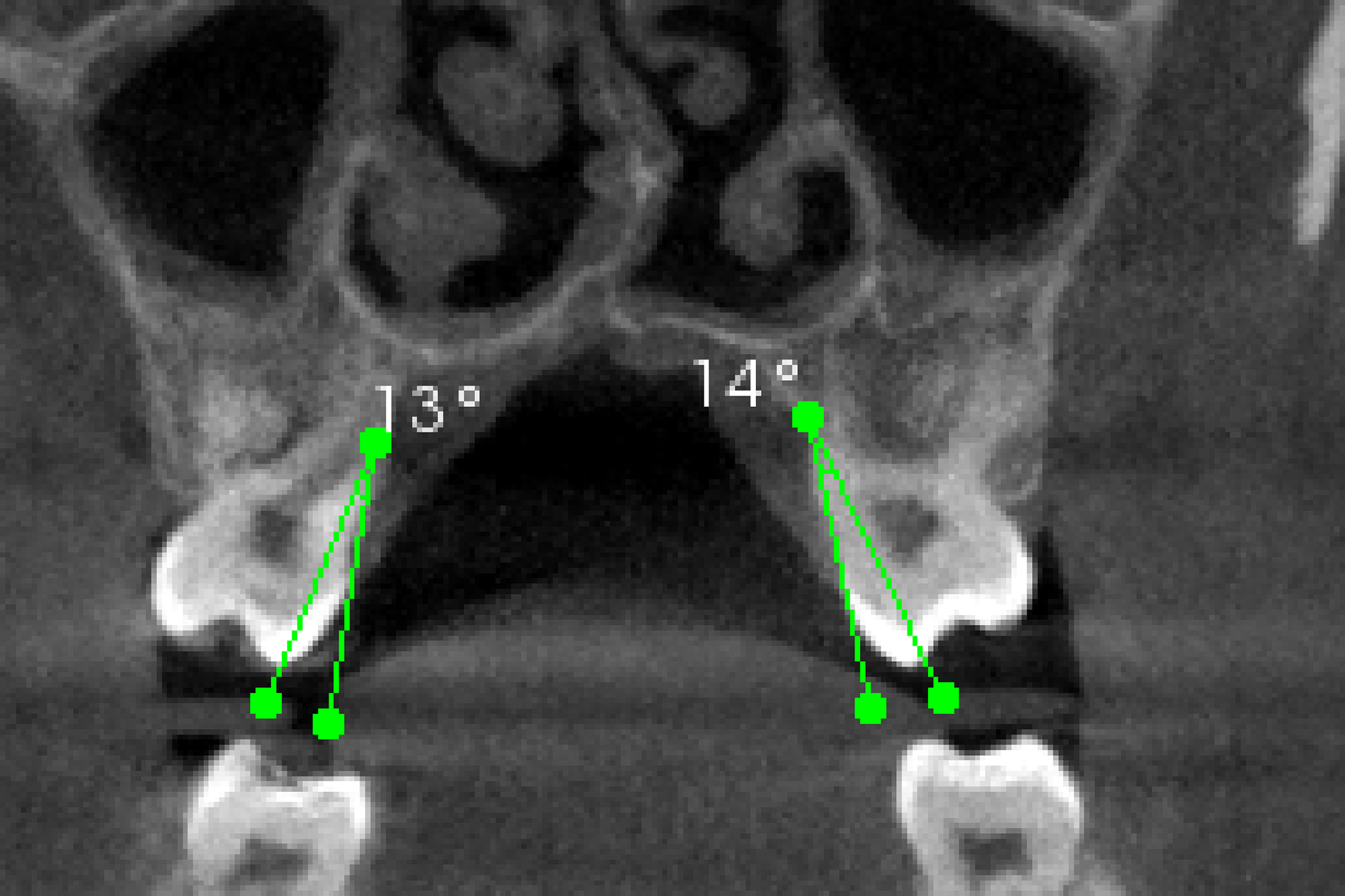
Measurement of dental tipping on cleft and non-cleft sides.
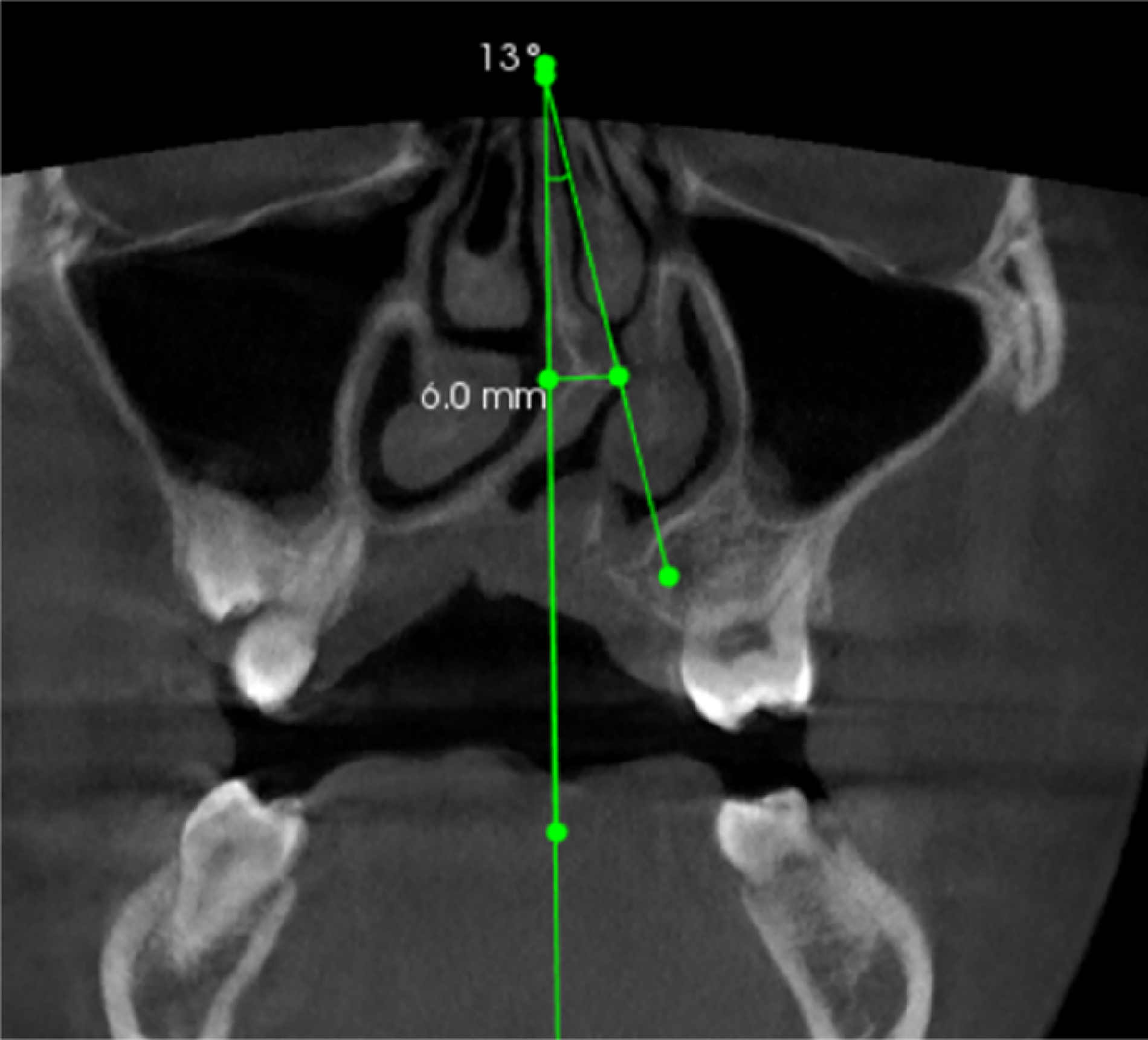
Measurement of nasal septum deviation: Midline Angle (MLA) and Distance of the Most Deviated Point (DMDP).
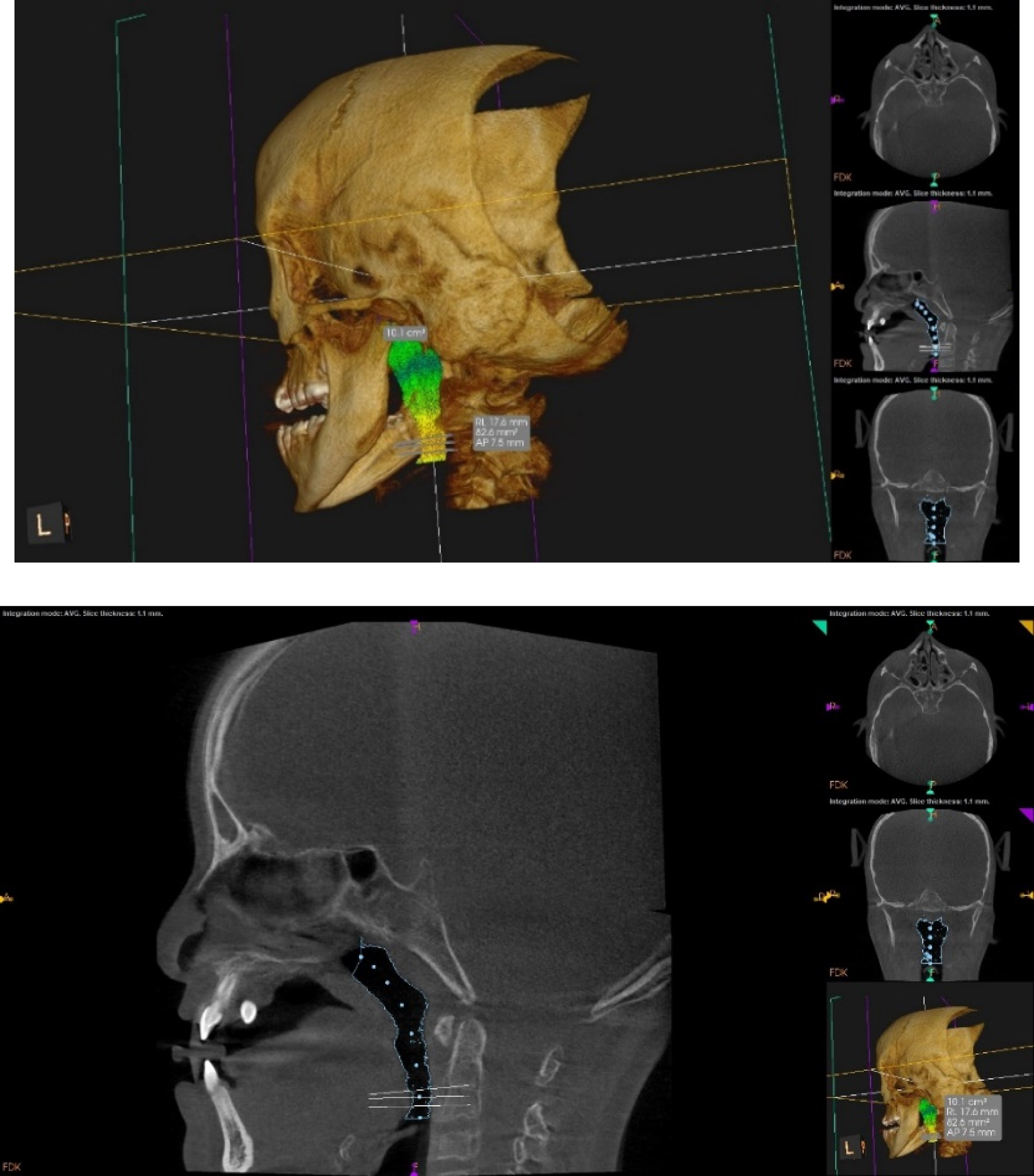
Measurement of oropharyngeal airway volume and airway length.
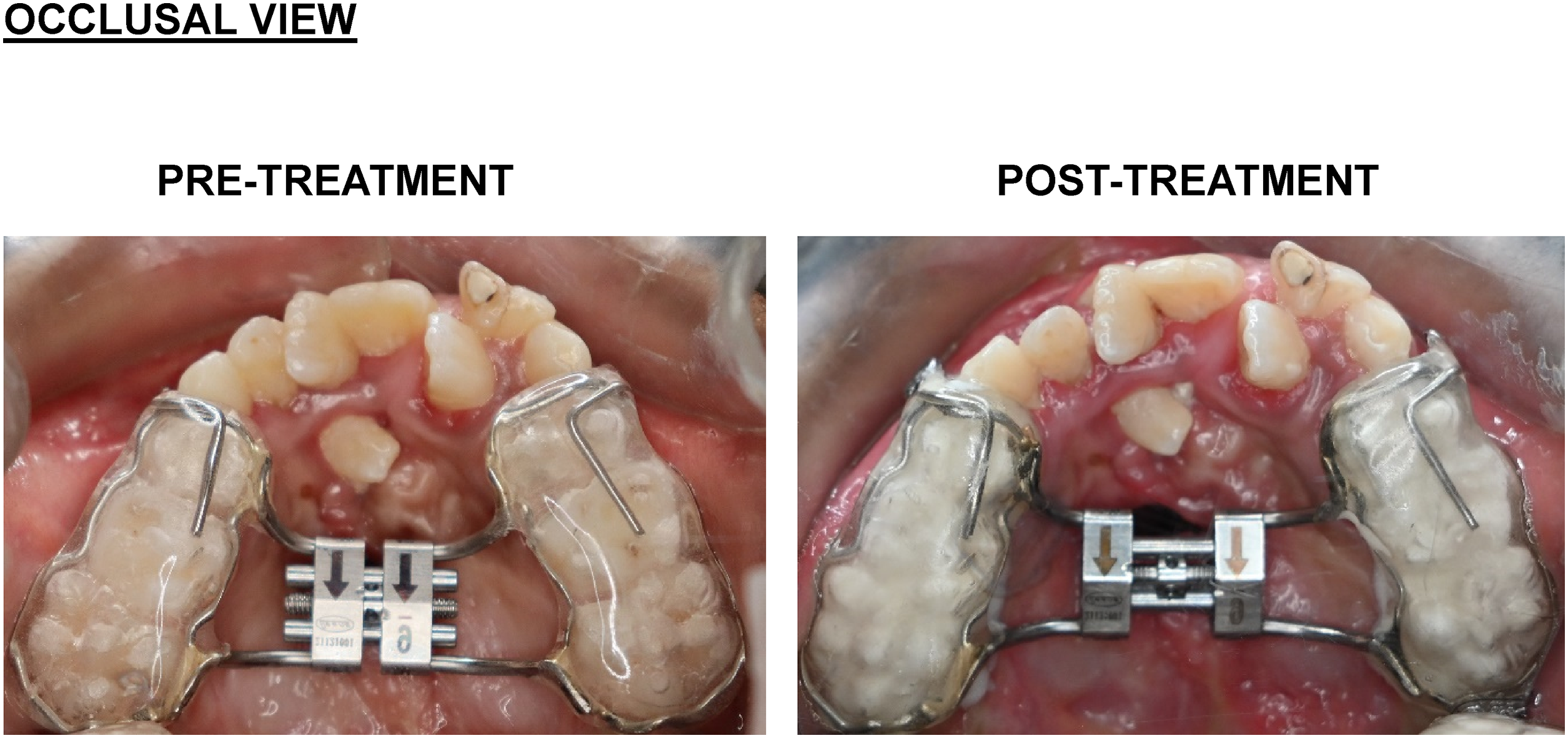
Pre- and post-treatment views of the Hyrax expander.
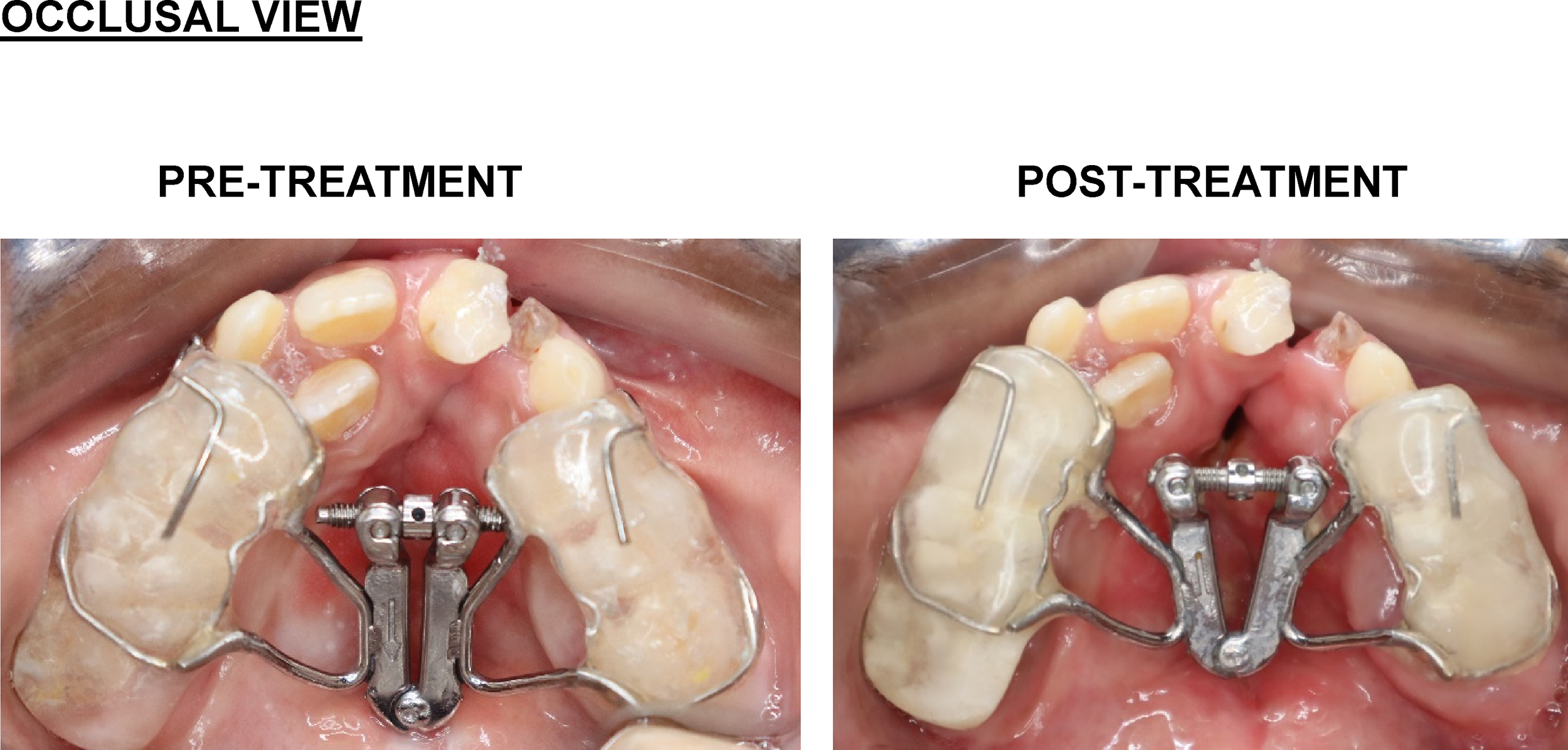
Pre- and post-treatment views of the fan-type expander.
Statistical Analysis
All statistical analyses were performed using the statistical package for the social sciences (SPSS), Version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for all variables and expressed as mean ± standard deviation.
Normality of data distribution was assessed using the Shapiro-Wilk test. As several variables did not demonstrate normal distribution, non-parametric statistical tests were applied. Intragroup comparisons were performed using the Wilcoxon signed-rank test, and intergroup comparisons were conducted using the Mann-Whitney U test.20,23 a P-value <.05 was considered statistically significant.
To ensure measurement reliability, a single-blinded study design was adopted, wherein the examiner performing all CBCT measurements was blinded to group allocation. A subset of 20% of the scans was randomly selected and re-evaluated after a 2-week interval to assess reproducibility. Measurement error was calculated using Dahlberg's formula (ME = √(Σd2/2n), where d represents the difference between repeated measurements and n represents the number of double measurements). In addition, intra-examiner reliability was evaluated using Intraclass Correlation Coefficients (ICC), with values greater than 0.80 considered indicative of excellent reliability.
Flow Chart of Patient Selection and Allocation
Results
In the Hyrax group (Table 2), the mean SNA angle increased from 76.60 ± 2.30° to 78.40 ± 2.07°, representing a statistically significant forward movement of the maxilla (Z = 2.041, P = .041). FH-ANS increased from 11.94 ± 3.15 mm to 12.98 ± 2.93 mm, but this vertical change was not significant (P = .225).
Baseline Characteristics of Hyrax and Fan-Type Groups.
Comparison of Clinical Parameters at Different Time Intervals in the Hyrax Group.
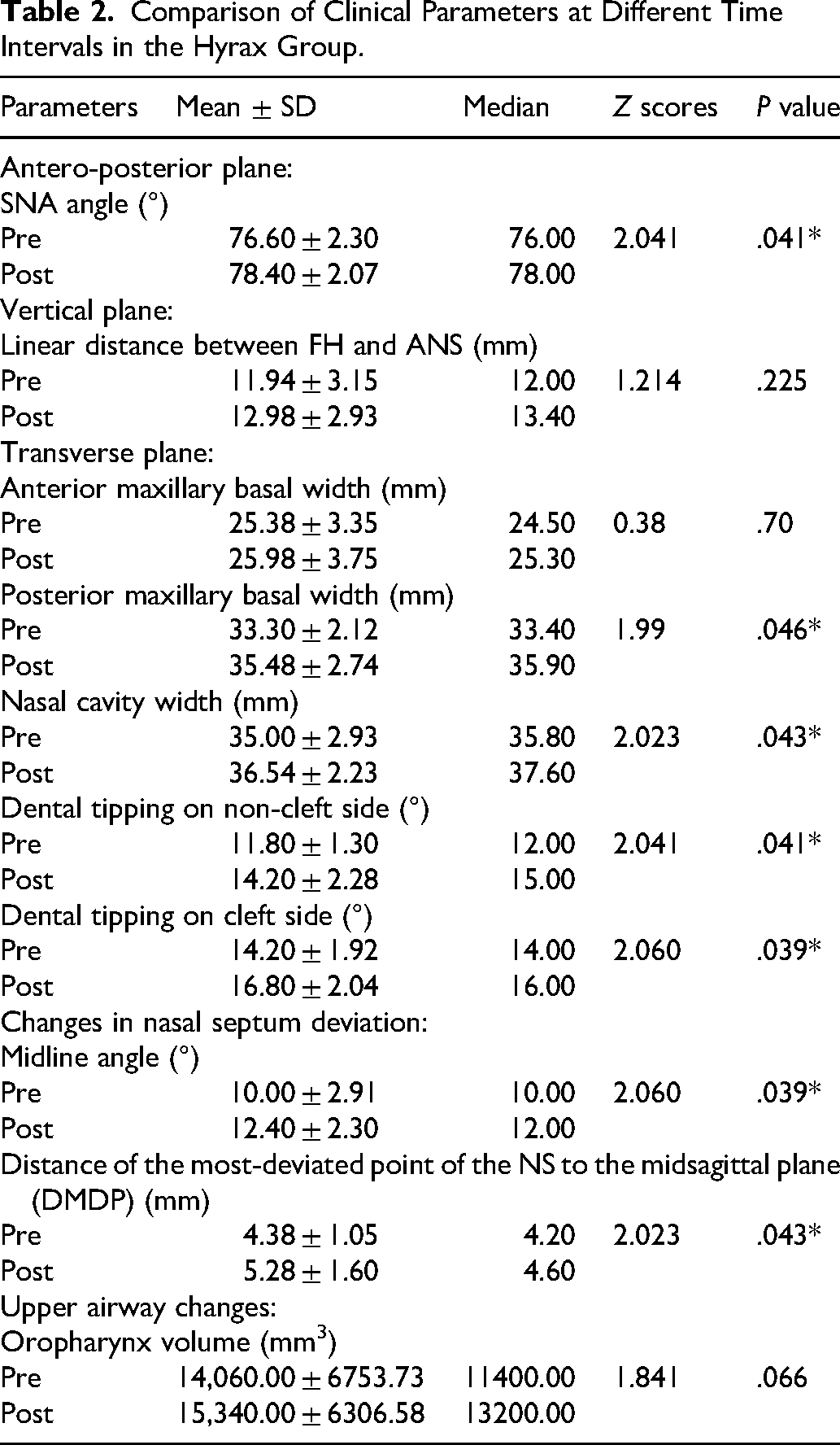
At-MBW showed a small, non-significant increase from 25.38 ± 3.35 mm to 25.98 ± 3.75 mm (P = .70), whereas Pt-MBW increased significantly from 33.30 ± 2.12 mm to 35.48 ± 2.74 mm (Z = 1.99, P = .046). NCW increased from 35.00 ± 2.93 mm to 36.54 ± 2.23 mm, with a significant difference (Z = 2.023, P = .043).
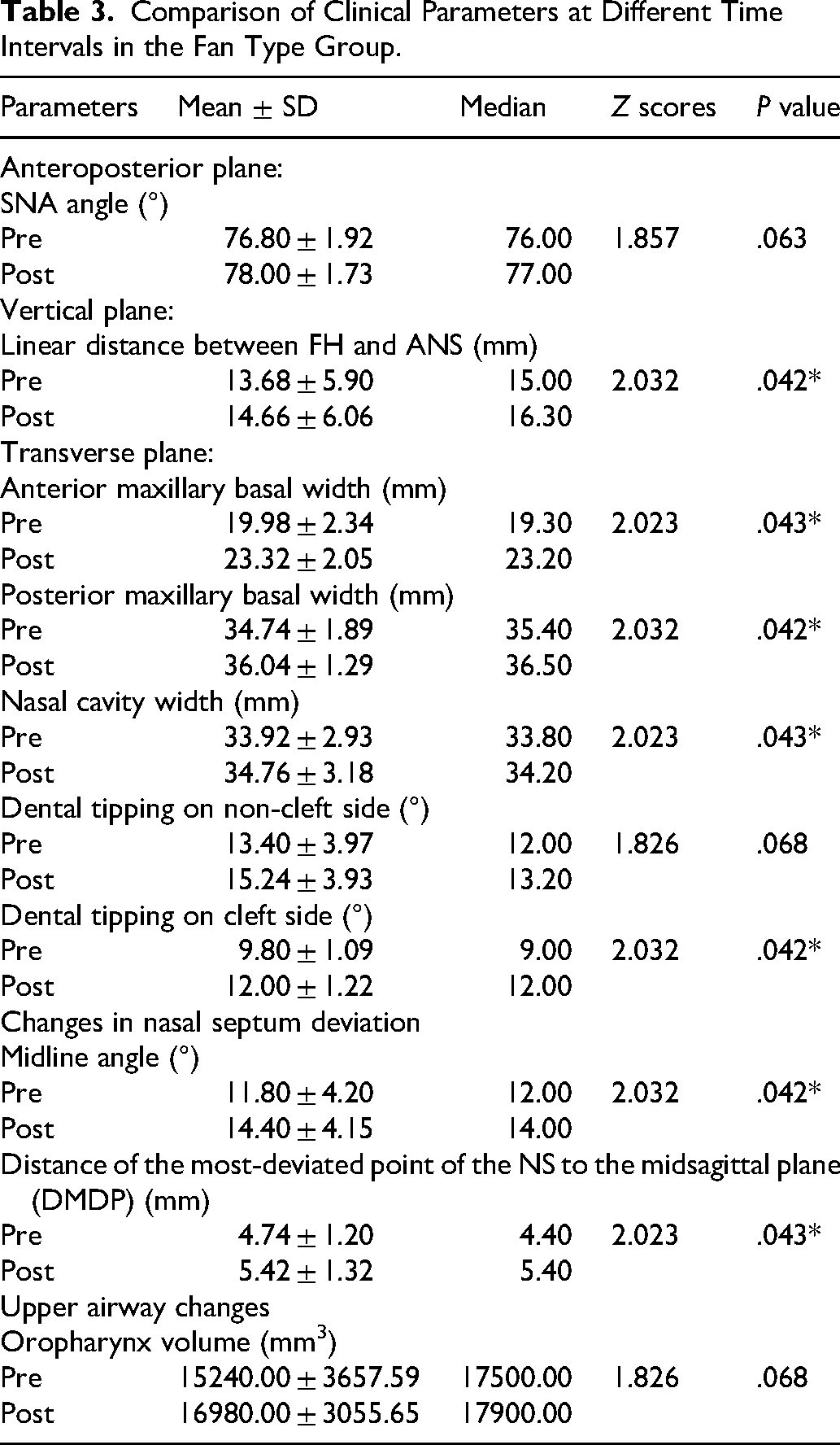
Comparison of Clinical Parameters at Different Time Intervals in the Fan Type Group.
Dental tipping on the noncleft side increased significantly from 11.80 ± 1.30° to 14.20 ± 2.28° (Z = 2.041, P = .041), and on the cleft side from 14.20 ± 1.92° to 16.80 ± 2.04° (Z = 2.060, P = .039). MLA increased from 10.00 ± 2.91° to 12.40 ± 2.30° (Z = 2.060, P = .039), and DMDP from 4.38 ± 1.05 mm to 5.28 ± 1.60 mm (Z = 2.023, P = .043).
Mean oropharyngeal airway volume increased from 14,060.00 ± 6753.73 mm3 to 15,340.00 ± 6306.58 mm3, but this change was not statistically significant (Z = 1.841, P = .066) (Table 4).
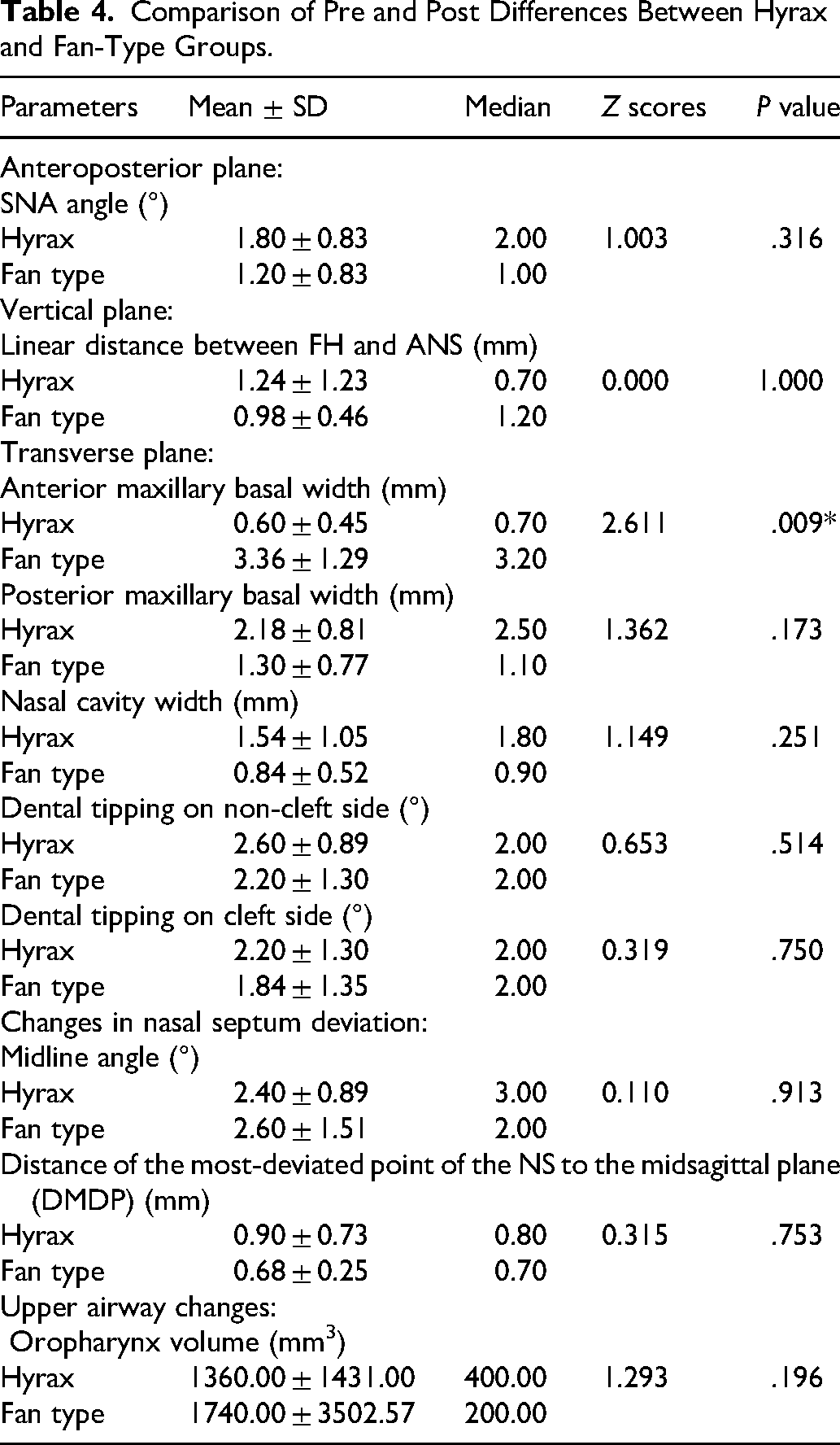
Comparison of Pre and Post Differences Between Hyrax and Fan-Type Groups.
In the fan-type group (Table 3), SNA increased from 76.80 ± 1.92° to 78.00 ± 1.73°, without reaching statistical significance (Z = 1.857, P = .063). FH-ANS increased significantly from 13.68 ± 5.90 mm to 14.66 ± 6.06 mm (Z = 2.032, P = .042).
At-MBW increased significantly from 19.98 ± 2.34 mm to 23.32 ± 2.05 mm (Z = 2.023, P = .043), and Pt-MBW from 34.74 ± 1.89 mm to 36.04 ± 1.29 mm (Z = 2.032, P = .042). NCW increased from 33.92 ± 2.93 mm to 34.76 ± 3.18 mm, also significant (Z = 2.023, P = .043).
Dental tipping on the noncleft side increased from 13.40 ± 3.97° to 15.24 ± 3.93°, but the change was not statistically significant (Z = 1.826, P = .068). Tipping on the cleft side increased significantly from 9.80 ± 1.09° to 12.00 ± 1.22° (Z = 2.032, P = .042).
MLA increased from 11.80 ± 4.20° to 14.40 ± 4.15° (Z = 2.032, P = .042), and DMDP from 4.74 ± 1.20 mm to 5.42 ± 1.32 mm (Z = 2.023, P = .043). Oropharyngeal volume increased from 15,240.00 ± 3657.59 mm3 to 16,980.00 ± 3055.65 mm3, but this change was not significant (Z = 1.826, P = .068).
Intergroup comparisons are presented in Table 4. The mean increase in SNA was greater in the Hyrax group (1.80 ± 0.83°) than in the fan-type group (Table 4) (1.20 ± 0.83°), but this difference was not significant (Z = 1.003, P = .316). Changes in FH-ANS were similar between groups (1.24 ± 1.23 mm vs 0.98 ± 0.46 mm, P = 1.000).
The fan-type group demonstrated significantly greater anterior basal expansion than the Hyrax group (ΔAt-MBW 3.36 ± 1.29 mm vs 0.60 ± 0.45 mm; Z = 2.611, P = .009). Posterior basal width changes favored the Hyrax group (2.18 ± 0.81 mm vs 1.30 ± 0.77 mm) but were not statistically different (Z = 1.362, P = .173).
The Hyrax group showed a larger mean increase in NCW than the fan-type group (1.54 ± 1.05 mm vs 0.84 ± 0.52 mm), but without statistical significance (Z = 1.149, P = .251). Differences in changes in dental tipping on noncleft and cleft sides between groups were not significant (noncleft: 2.60 ± 0.89° vs 2.20 ± 1.30°, P = .514; cleft: 2.20 ± 1.30° vs 1.84 ± 1.35°, P = .750).
Differences in changes in MLA (2.40 ± 0.89° vs 2.60 ± 1.51°, Z = 0.110, P = .913), DMDP (0.90 ± 0.73 mm vs 0.68 ± 0.25 mm, Z = 0.315, P = .753), and oropharyngeal airway volume (1360.00 ± 1431.00 mm3 vs 1740.00 ± 3502.57 mm3, Z = 1.293, P = .196) were not statistically significant between Hyrax and fan-type groups. Representative pre- and post-treatment views of the Hyrax and fan-type expanders are shown in Figures 8 and 9, respectively.
Discussion
Maxillary transverse deficiency is a well-recognized and consistent feature in patients with CLP, resulting from altered embryologic development, disrupted muscular balance, and scar formation following early surgical repair.1,7,10 These factors impair normal sutural growth and contribute to maxillary constriction, posterior crossbite, and compromised nasal and airway dimensions.8,11,14 Consequently, RME remains a cornerstone of early orthodontic intervention in cleft patients, aiming to restore transverse maxillary relationships, improve arch coordination, and facilitate subsequent alveolar bone grafting.8,10,15
The present prospective CBCT study evaluated and compared the dentoskeletal, nasal septal, and upper airway effects of bonded Hyrax and fan-type expanders in growing CLP patients. Both appliances produced transverse dentoskeletal changes; however, appliance-specific expansion patterns were observed.
Sagittal and Vertical Skeletal Effects
Neither appliance produced significant sagittal advancement of the maxilla, as reflected by minimal changes in SNA angle. This finding is consistent with previous CBCT and longitudinal studies in surgically repaired cleft patients, which have demonstrated limited anteroposterior skeletal response to expansion alone due to scar-related restriction of circummaxillary sutures.10–12,14 Figueiredo et al. 11 and Peterson et al. 12 similarly reported that RME in CLP primarily induces transverse changes, with negligible sagittal advancement unless combined with maxillary protraction protocols.
Vertical skeletal changes assessed by FH-ANS distance were modest and comparable between groups. This aligns with earlier reports suggesting that vertical response following RME is influenced more by growth pattern, anchorage design, and occlusal coverage than by expander type alone.11,17 The bonded appliance design used in both groups may have contributed to improved vertical control.
Transverse Maxillary Response
A principal finding of this study was the greater increase in anterior maxillary basal width observed in the fan-type expander group compared with the Hyrax group. This outcome is consistent with the biomechanical design of the fan-type expander, which incorporates a posterior hinge mechanism to concentrate expansion forces anteriorly. 21 Similar anterior-predominant expansion patterns have been reported in cleft patients by Almeida et al. 22 and Sebaey et al., 23 supporting the suitability of fan-type expanders in cases with predominant anterior constriction.
In contrast, the Hyrax expander produced a more uniform anterior-posterior expansion pattern, consistent with CBCT findings reported by Figueiredo et al. 11 and Garib et al. 17 Pugliese et al. 24 also demonstrated relatively parallel transverse expansion with Hyrax-type appliances in cleft patients, attributable to symmetric force distribution across the midpalatal suture.
Dentoalveolar Effects
Both expanders produced buccal tipping of posterior teeth, a known dentoalveolar effect associated with tooth-borne expansion appliances, particularly in anatomically compromised cleft maxillae.11,17 Although the Hyrax group demonstrated slightly greater tipping, intergroup differences were not statistically significant. These findings are consistent with previous CBCT studies evaluating dentoalveolar responses to RME in cleft patients.11,17
Nasal Cavity and Nasal Septum Changes
Although statistically significant changes in nasal septum deviation were observed following expansion, the magnitude of these changes was modest and did not differ significantly between the Hyrax and fan-type groups. The greater increase in nasal cavity width, particularly in the Hyrax group, is consistent with previous CBCT-based studies demonstrating that appliances producing more parallel posterior expansion result in greater lateral displacement of the nasal walls.11,20
Mordente et al. 20 similarly reported nasal cavity widening following Hyrax-based expansion in cleft patients. However, cleft lip and palate patients inherently exhibit septal asymmetry due to embryologic disruption and postsurgical scarring, which may limit the capacity for true septal remodeling.
Costa et al. 32 found no significant alteration in nasal septum deviation following rapid maxillary expansion in unilateral cleft lip and palate patients, suggesting that expansion-induced changes are predominantly dentoalveolar rather than structural within the septal cartilage. Likewise, Akay et al. 33 demonstrated greater baseline septal deviation in cleft individuals compared with non-cleft controls but did not establish evidence that orthopaedic expansion alone produces meaningful septal correction. In the present study, the observed increases in midline angle and distance of the most deviated point likely represent mechanical displacement secondary to transverse skeletal widening rather than true septal remodeling. Therefore, although CBCT revealed measurable positional changes, their direct clinical relevance in terms of functional respiratory improvement remains uncertain.
Furthermore, the short-term follow-up period of 3 months limits conclusions regarding long-term stability. Collectively, these findings suggest that the primary orthopaedic benefit of rapid maxillary expansion in cleft patients lies in transverse skeletal correction rather than substantial septal realignment, supporting a cautious interpretation of septal outcomes.
Upper Airway Effects
In the present study, both Hyrax and fan-type expanders demonstrated a modest increase in oropharyngeal airway volume following expansion; however, these changes did not reach statistical significance, and no significant intergroup differences were observed. Airway compromise in CLP patients is multifactorial, involving congenital maxillary deficiency, midface retrusion, postsurgical scar formation, altered muscular attachments, and aberrant craniofacial growth patterns.1,25 CBCT-based investigations have consistently demonstrated reduced airway dimensions in CLP populations compared with non-cleft controls, particularly within the nasopharyngeal and oropharyngeal regions. 25 Recent large-sample analyses further confirm significantly decreased airway area and volume in unilateral and bilateral cleft patients, underscoring the inherent anatomical restriction in this population. 34
Systematic reviews evaluating CBCT-based airway assessment in cleft subjects have reported heterogeneity in volumetric findings and a lack of consensus regarding the magnitude of airway differences. 35 Mordente et al. 20 reported increased nasal cavity dimensions following maxillary expansion but observed no statistically significant change in oropharyngeal airway volume, findings consistent with the present results. Similarly, comparative studies evaluating fan-type and Hyrax expanders in cleft patients have demonstrated measurable transverse skeletal expansion with limited oropharyngeal volumetric alteration. 23
Importantly, volumetric changes alone may not fully represent functional respiratory improvement. Using computational fluid dynamics (CFD), Lo Giudice et al.37 demonstrated that rapid maxillary expansion can modify airflow velocity, pressure distribution, and airway resistance, even in the absence of large volumetric changes. Their findings suggest that functional airflow improvement may occur despite modest structural expansion, particularly when craniofacial growth patterns are considered. However, the extent of functional improvement may vary depending on baseline skeletal morphology and developmental status.
Furthermore, static CBCT imaging does not account for neuromuscular tone, head posture, soft tissue adaptation, or velopharyngeal competence, all of which influence airway patency. Multidisciplinary cleft care guidelines emphasize comprehensive longitudinal airway evaluation and functional assessment rather than reliance solely on volumetric measurements. 36
Therefore, although a trend toward increased airway volume was observed following expansion, the present findings suggest that rapid maxillary expansion in cleft patients primarily corrects transverse skeletal deficiency, with limited and variable impact on oropharyngeal airway dimensions. While functional airflow improvements may occur, as suggested by CFD-based analyses, 37 the clinical significance of such changes in cleft populations requires further longitudinal and function-based investigation. These results support a cautious interpretation of airway benefits and reinforce the need for long-term respiratory assessment to determine true clinical relevance.
Clinical Implications and Limitations
The present study provides a prospective three-dimensional evaluation of dentoskeletal, nasal, septal, and airway changes following rapid maxillary expansion in growing patients with repaired cleft lip and palate. Both Hyrax and fan-type expanders effectively achieved transverse skeletal correction, which remains the principal orthopaedic benefit of expansion therapy in this population. The fan-type expander demonstrated a greater tendency toward anterior expansion, whereas the Hyrax appliance produced a more uniform transverse effect across anterior and posterior regions, consistent with previous comparative investigations of differential-opening expanders.8,10,15,24 These findings highlight the clinical importance of appliance selection based on the pattern of transverse maxillary deficiency. Fan-type expanders may be particularly advantageous in cases with predominant anterior constriction, whereas Hyrax expanders may be preferred when uniform posterior expansion and greater nasal cavity widening are desired.
Several limitations should be considered when interpreting these findings. Although the sample size was determined through an a priori power analysis and was sufficient to detect clinically meaningful skeletal differences, the relatively modest cohort may limit detection of smaller effect sizes, particularly with respect to airway-related outcomes. Larger multicentre studies may enhance statistical precision and external validity.
The absence of an untreated control group represents a methodological limitation. However, inclusion of an untreated group in growing patients with repaired cleft lip and palate presenting with transverse maxillary deficiency was not ethically justifiable. Rapid maxillary expansion is widely recognized as a standard interceptive orthopaedic procedure in cleft patients during growth and forms an integral component of comprehensive multidisciplinary management.7,10,15,29 Contemporary cleft care protocols emphasize timely orthodontic intervention coordinated with secondary alveolar bone grafting and overall treatment sequencing.28,30,31 Delaying treatment for research purposes would therefore conflict with established clinical standards and ethical principles governing patient care. 27 To minimize the potential influence of physiological growth, only patients within comparable cervical vertebral maturation stages (CS1-CS4) were included, and post-expansion evaluation was conducted after a standardized 3-month retention period. Each participant also served as an internal control through pre-expansion (T0) and post-expansion (T1) comparisons.
Although both unilateral and bilateral cleft cases were included, further stratification according to cleft severity was not performed due to sample size considerations. Variations in anatomical presentation between cleft subtypes may influence treatment response and should be explored in future research.
With respect to nasal septum deviation, the statistically significant changes observed should be interpreted cautiously. The magnitude of septal modification may not directly correspond to immediate functional respiratory improvement, suggesting that septal remodeling represents a secondary structural adaptation rather than the primary therapeutic objective of maxillary expansion.
Similarly, the upper airway changes were modest and did not reach statistical significance. Given the complex craniofacial morphology, postsurgical scar tissue, and soft-tissue constraints characteristic of cleft patients, transverse expansion alone may exert limited influence on pharyngeal airway dimensions. Future multicentre studies with larger cohorts and longer follow-up are recommended to evaluate the stability of skeletal and airway changes and to incorporate functional outcomes such as speech performance, nasal airflow, and quality of life measures.
Despite these limitations, the prospective comparative design, standardized CBCT acquisition protocol, and incorporation of a priori power analysis strengthen the methodological rigor of the study and support its contribution as an original clinical investigation in cleft orthodontics.
Conclusions
Both Hyrax and fan-type bonded rapid maxillary expanders produced significant transverse maxillary gains and increases in nasal cavity width in growing CLP patients.
Hyrax expanders yielded greater posterior maxillary basal expansion and significant SNA increase, suggesting a tendency toward posterior skeletal widening with mild forward maxillary displacement.
Fan-type expanders produced significantly greater anterior maxillary basal expansion and are particularly suitable for managing predominant anterior transverse deficiencies.
Both appliances induced modest, statistically non-significant increases in oropharyngeal airway volume and minor changes in nasal septum deviation, whose clinical relevance requires further investigation.
Appliance selection in CLP should be individualized, with fan-type expanders preferred for anteriorly constricted arches and Hyrax expanders for generalized or posterior constriction.
Footnotes
Acknowledgments
I sincerely thank my guide, Dr. Kanuru Ravi Krishna, Professor, for his constant guidance, encouragement, and academic support throughout this study. I extend my gratitude to the Head of the Department and all faculty members of the Department of Orthodontics and Dentofacial Orthopaedics for their valuable suggestions and cooperation. I also thank the statistician for assistance with data analysis and all the patients who willingly participated in this study. I am deeply grateful to my family for their unwavering support and encouragement.
Ethical Approval and Informed Consent
Ethical approval for this study was obtained from the Institutional Ethics Committee of Drs. Sudha and Nageswara Rao Siddhartha Institute of Dental Sciences, affiliated with Dr. NTR University of Health Sciences, Vijayawada, Andhra Pradesh, India.
Consent of Participants
Written informed consent was obtained from all participants and/or their legal guardians prior to inclusion in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Anonymity Statement
All identifying information related to the authors, institutions, ethics committees, and funding sources has been removed from the blinded version of the manuscript to ensure anonymity during the peer-review process.