
Abstract
Congenital midline cervical cleft (CMCC) is a rare congenital malformation in the anterior region of the neck with an incidence of 1.7-2.0%. CMCC can be associated with other defects in the midline-like cleft of the lower lip, mandible, chin, tongue, and sternum. It may cause micrognathia and contracture of the cervical region. Early diagnosis and surgical excision before 2 years should be done. We present a male neonate who was diagnosed with CMCC at birth. Ultrasound and magnetic resonance imaging of the neck confirmed the diagnosis. The child underwent surgical excision of the lesion at 3 years of age and is doing well.
Introduction
Congenital midline cervical cleft (CMCC) is also known as mentosternal dysgraphia. It is a very rare congenital malformation involving the anterior region of the neck. Very few cases, less than 150 were reported in the literature with the first case been reported by Luschka in 1848 and subsequently documented by Bailey in 1924. Among the congenital cervical malformations, the incidence of CMCC collectively ranges between 1.7 and 2.0% with a higher incidence in girls compared to boys. 1 The length and width of the cleft can vary among children, and it may extend anywhere from mandible to manubrium in the midline. The diagnosis is mainly by clinical examination and needs to be differentiated from thyroglossal duct and branchial anomalies. The primary mode of management is surgical excision. In this case report, we are describing a neonate presenting with CMCC with the description of clinical features, diagnosis, investigations, and clinical course including imaging done.
Case Report
A male neonate born to a 24-year-old primiparous mother at 37 weeks of gestation by normal vaginal delivery with birth weight of 3320 grams (80th centile), length 50 cm (87th centile), and head circumference 35 cm (76th centile). The antenatal period was complicated by pregnancy-induced hypertension and hypothyroidism. Antenatal scans were normal, and there was no history of fever, no family history of similar anomalies. Baby was vigorous at birth with APGAR scores of 7/10, 8/10, 9/10 at 1,5,10 minutes of liferespectively. Neck examination revealed a linear erythematous track (3*1 cm) in the anterior part of the neck, and there was a skin tag at the superior part, and in the lower part, there was a sinus without any discharge from the lesion. On palpation, there was a firm cord-like structure below the track. Examination of the rest of the neck, face, and oral cavity revealed no other sinus/cleft. Systemic examination was normal. There was no airway or feeding difficulty, and the cry was normal.
Ultrasound neck was done, which was suggestive of a hypoechoic area seen in the subcutaneous tissue of the neck in the midline location measuring 6*5 mm with no abnormal calcification and vascularity within the mass. No fistulous tract and no other associated anomalies were visualized. The 2D echo was normal. Pediatric surgeon consultation was taken, and magnetic resonance imaging (MRI) was done to evaluate the CMCC and to look for its internal extension and to diagnose other anomalies in the neck. MRI revealed an oval exophytic dermal lesion measuring 4.5*3*3 mm, in the anterior midline neck region at the level of the hyoid bone with no obvious subcutaneous fat plane extension or fluid-filled sinus tract. No enhancement was seen on post-gadolinium images, and no extension to the sternum or deeper soft tissues was identified. The thyroid was normal in location, size, and enhancement. The baby was under follow-up. Figures 1 and 2 show the image of the baby, and Figure 3 shows images of the MRI neck of the baby. The child was operated on at 3 years of age by the Z plasty technique, and the surgical excision of CMCC was done. Figures 4 and 5 show intraoperative pictures of the child. Post-operative period was uneventful, and the child is doing well.

It shows image of newborn with congenital midline cervical cleft.

It shows image of the affected newborn.

MRI neck images of the affected newborn.

Intraoperative image of the child.

It shows Z plasty technique of surgical correction.
Discussion
CMCC is one of the less commonly seen malformation but it can be diagnosed easily after birth, but can be misdiagnosed as anomalies of the brachial cleft or thyroglossal duct or dermoid cyst. Many theories were postulated based on embryonic development of different neck structures, but the commonly accepted theory is defective fusion of the branchial arches in the midline. During development, the branchial arches grow medially and fuse in a craniocaudal direction. Figure 6 shows pharyngeal arches and their development. The first or mandibular arch fuses before the second or hyoid arch, and the lower arches fuse sequentially. Before fusing, mesodermal tissue migrates between the arches, pushing the ectoderm outward to flatten the ventral furrow. Disruption of this process results in various deformities. Some mechanical factor or vascular anomaly may result in ischemia or necrosis and interfere with these normal processes and lead to the development of CMCC. Other hypothesis is that CMCC may occur due to increased pressure in the cervical region from the developing pericardial roof, amniotic adhesions. Some theories like external protrusion of remnant of thyroglossal duct or pericardial roof causing increased pressure in the cervical area causing CMCC during embryo development are also postulated. On histopathological examination, there is the presence of stratified keratinized squamous epithelium with hyperkeratosis in the cleft, and there may be dermal fibrosis with or without skin appendages.
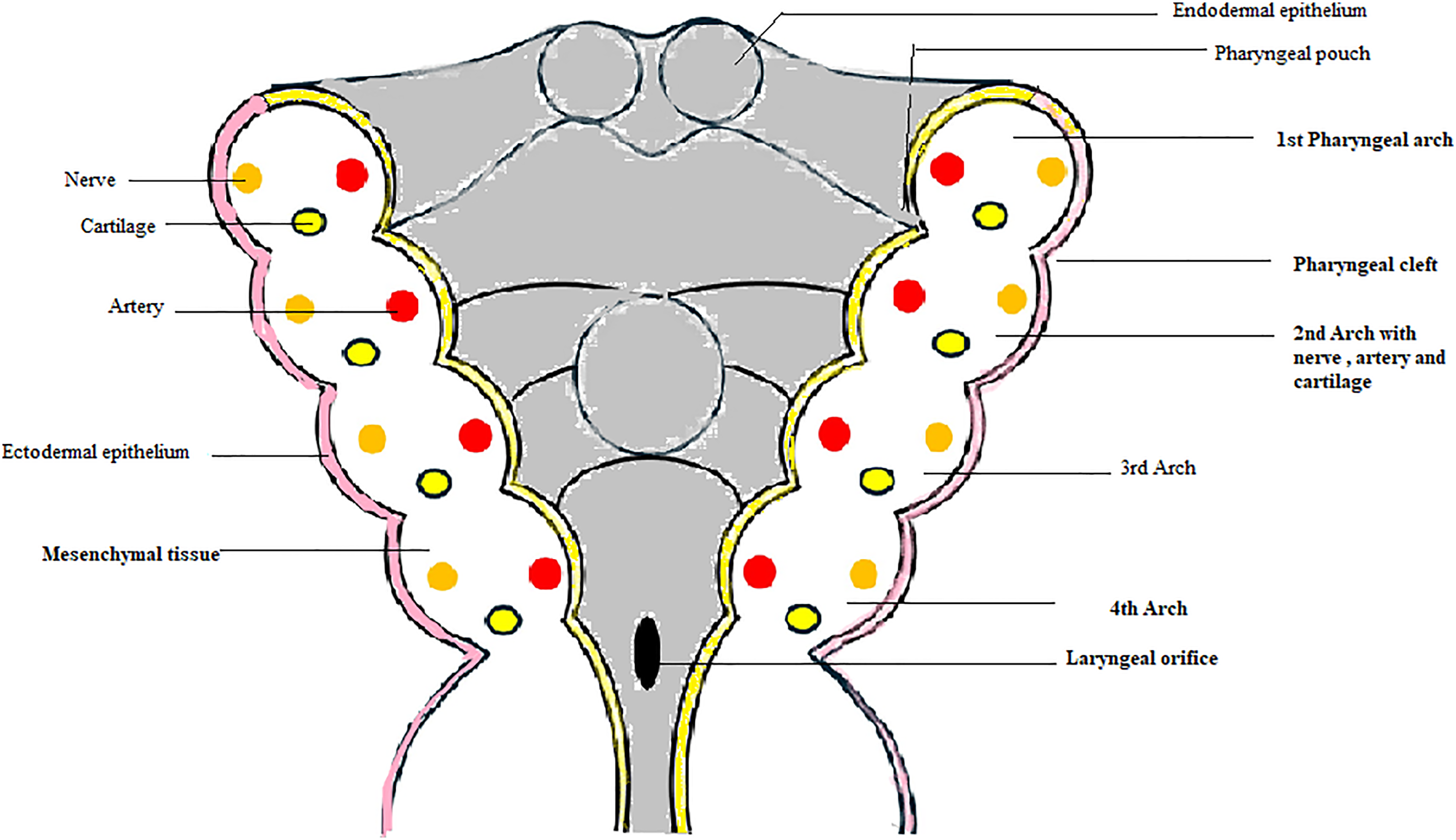
It shows development of pharyngeal archesi.
CMCC most commonly presents as a red strip of atrophic skin between the chin and the sternal notch occurring at any level, a skin tag at the superior part appearing like a nipple and as a sinus tract at the distal end with mucoid discharge.2,3
CMCC can be associated with other defects in the midline-like cleft of the lower lip, mandible, chin, tongue, and sternum and midline abdominal web or scar-like raphe, midline hemangioma and cardiac anomalies. CMCC must be differentiated from thyroglossal duct anomalies, brachial anomalies, and dermoid cysts. 4 Diagnosis is mainly by clinical examination, and the treatment of choice is surgical excision. CT or MRI helps to differentiate CMCC from other anterior cervical anomalies and to diagnose any associated anomalies. MRI is the best imaging technique to diagnose CMCC and to evaluate the extension of the tract, associated neck and ear anomalies and to plan of surgery.
CMCC if not treated in the long term can lead to a scar causing contracture of the neck and restrict full extension of the neck, can lead to micrognathia and torticollis, and increase the risk of infection. Z-plasty is the recommended treatment for the correction of CMCC. The surgical procedure involves transposition of two triangular skin flaps, interchanging each other, to obtain an increase in the length of a linear scar contracture. The technique reorients the central scar, lengthens contracted tissue, and redistributes tension along more favorable lines. In midline cleft deformities, it plays a crucial role in improving both functional and esthetic outcomes by redistributing tension, lengthening contracted tissues, and reorienting scars. The functional outcomes of Z-plasty are satisfactory in the long term, and there is an improvement in neck extension in all planes. There are no definite recommendations about the appropriate age for surgical correction of CMCC. Many authors prefer surgery to be performed in early infancy, usually before the age of 2 years and when no inflammation is present to avoid contractures. 5 Many reports have shown that surgery can be performed during the neonatal period with a successful outcome.
Conclusion
CMCC is a rare congenital anomaly of the neck and should be considered in any child with cervical lesions or anomalies in the midline and must be distinguished from other common neck anomalies. Recognizing CMCC is very important for pediatricians/ neonatologists and pediatric surgeons as early diagnosis and treatment lead to a better outcome.
Footnotes
ORCID iDs
Ethical Approval and Informed Consent Statements
Appropriate consent has been obtained from parents for publishing images and other clinical information.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.