
Abstract
Objective
To evaluate maxillary sinus volumetric changes in patients with unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP) undergoing Le Fort I osteotomy.
Design
Retrospective observational study.
Setting
Single tertiary craniofacial rehabilitation center.
Participants
A total of 200 patients aged 18 years or older were included, comprising 100 individuals with UCLP and 100 with BCLP, all presenting preoperative and 1-year postoperative cone-beam computed tomography scans.
Interventions
All participants underwent Le Fort I osteotomy as part of orthognathic surgical treatment.
Main Outcome Measures
Volumetric segmentation of the maxillary sinuses and sinus lesions was performed using ITK-SNAP software. Volumes were measured in cubic millimeters using preoperative and 1-year postoperative cone-beam computed tomography scans.
Results
In UCLP patients, no significant differences were observed in total maxillary sinus volume between preoperative and postoperative periods, although lesion volume was significantly reduced. In BCLP patients, a significant postoperative increase in sinus volume was observed, accompanied by a reduction in lesion volume. In both groups, the cleft side consistently presented smaller sinus volumes.
Conclusions
Maxillary sinus volume remains smaller on the cleft side regardless of surgical intervention. Le Fort I osteotomy does not significantly affect sinus volume in UCLP patients, whereas BCLP patients demonstrate a postoperative volumetric increase.
Keywords
Introduction
Cleft lip and palate (CLP) is associated with structural alterations of the nasomaxillary complex, including maxillary hypoplasia, facial asymmetry, and changes in the paranasal cavities.1–5 Several studies have shown that individuals with CLP present reduced maxillary sinus volume, increased mucosal thickness, and significant differences between the cleft and non-cleft sides.3–9 However, findings vary according to cleft type, patient age, and the measurement methods employed.1,4,5,7 The advent of computed tomography has enabled more accurate three-dimensional measurements, contributing substantially to the understanding of maxillary sinus morphological variations in this population.4,10,11 Recent studies using this imaging modality have confirmed volumetric asymmetry and a higher prevalence of sinus pathologies in patients with CLP, although considerable heterogeneity in results remains.3–8
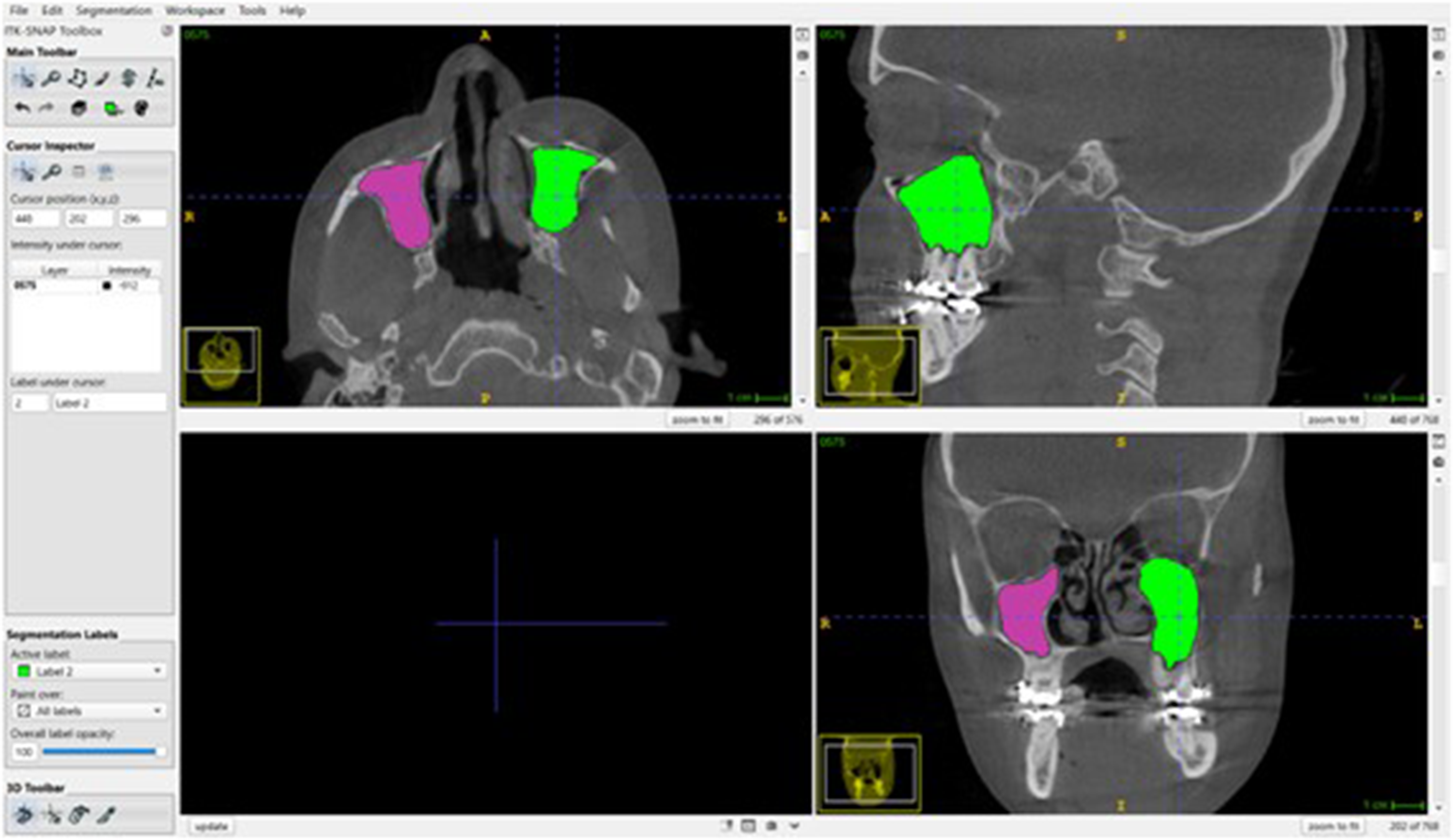
Semi-automatic segmentation of the maxillary sinuses using ITK-SNAP. Axial, coronal, and sagittal views illustrate the identification of the maxillary sinus ostium and the delineation of the region of interest. The right and left maxillary sinuses were segmented separately using the Snake Segmentation tool, with manual refinement as needed. Volumetric measurements were automatically calculated using the Volumes & Statistics module.
Maxillary Sinus and Lesion Volumes in the Unilateral Cleft Lip and Palate (UCLP) Group.
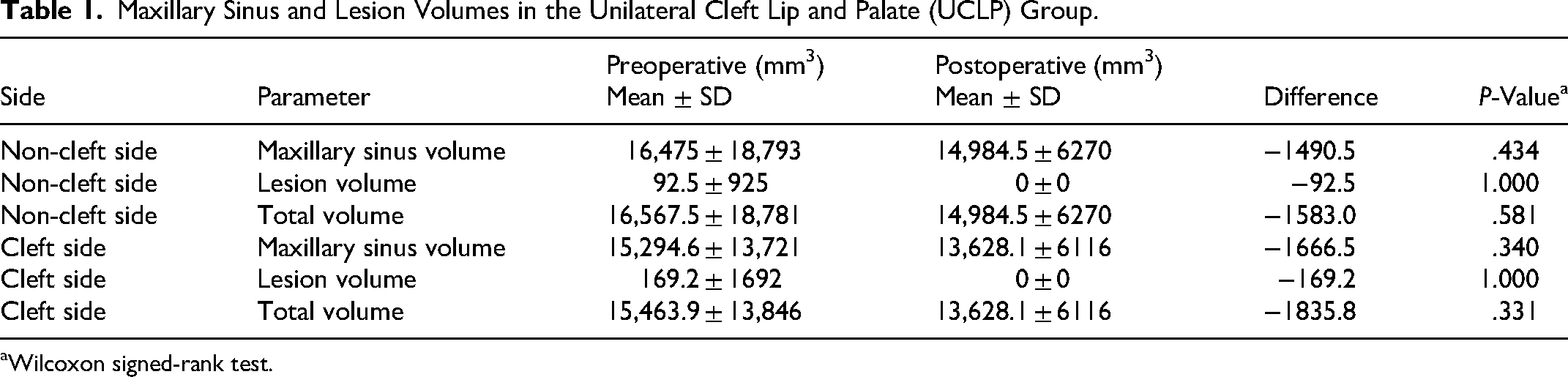
Wilcoxon signed-rank test.
Maxillary Sinus and Lesion Volumes in the Bilateral Cleft Lip and Palate (BCLP) Group.
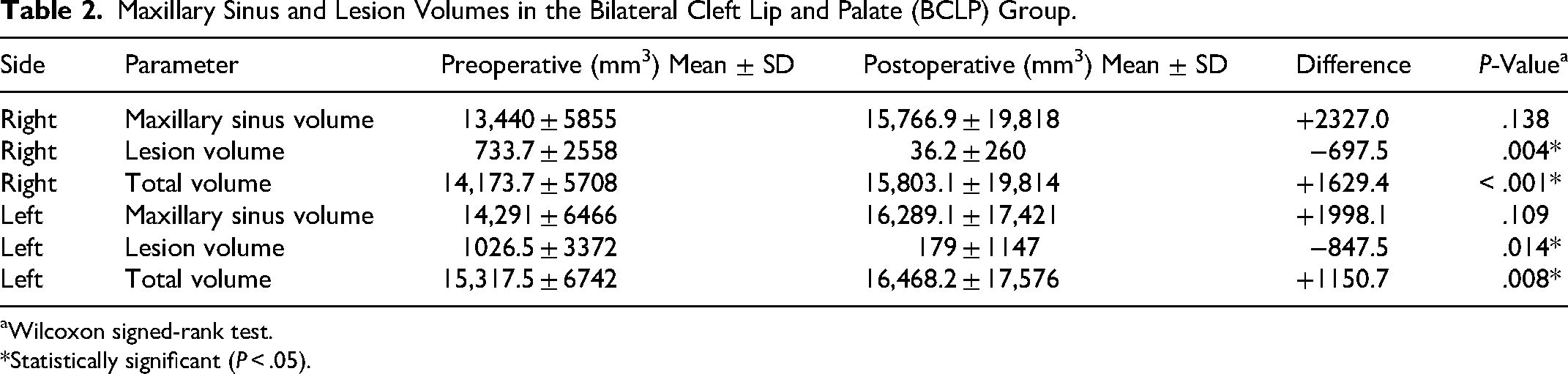
Wilcoxon signed-rank test.
*Statistically significant (P < .05).
Comparison Between Cleft and Non-Cleft Sides in the Unilateral Cleft Lip and Palate (UCLP) Group.
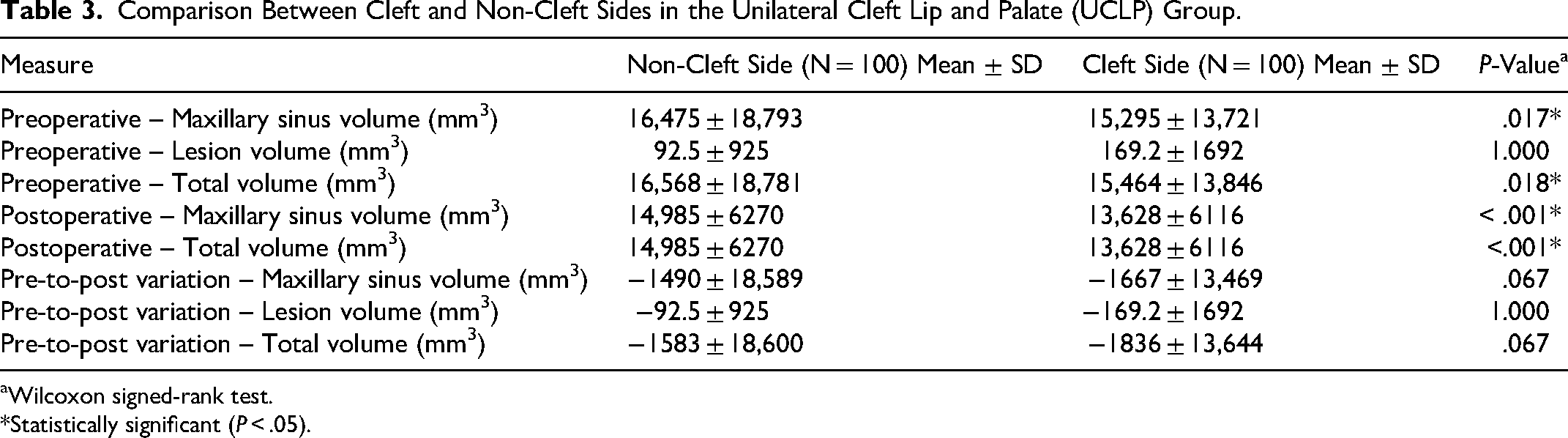
Wilcoxon signed-rank test.
*Statistically significant (P < .05).
Le Fort I osteotomy, widely used to correct maxillary discrepancies in patients with CLP, may modify the position of the sinus walls and potentially alter maxillary sinus volume.2,12–16 Nevertheless, the literature reports conflicting results: while some authors describe significant volumetric changes following surgery,2,14,17 others indicate postoperative stability of maxillary sinus volume.15,16 Given the limited number of studies that jointly address CLP, sinus asymmetry, and the direct impact of orthognathic surgery on maxillary sinus volume, the present study aims to systematically compare pre- and postoperative volumetric changes. Specifically, it seeks to determine whether the presence of the cleft represents an independent determining factor or whether the observed modifications are predominantly attributable to Le Fort I osteotomy.
Methodology
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and the current national regulations for research involving human subjects. This retrospective observational study was conducted at a single center between 2024 and 2025. The research project was approved by the Research Ethics Committee of Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo (protocol no. CAAE: 83599524.9.0000.5441). As cone-beam computed tomography (CBCT) scans were already part of the patients’ routine clinical care for diagnostic and treatment planning purposes, no additional imaging examinations were required specifically for this study.
Study Design and Sample Size Calculation
This retrospective observational study evaluated volumetric changes in the maxillary sinus before and after Le Fort I osteotomy in patients with cleft lip and palate. The primary outcome used for sample size calculation was the change in maxillary sinus volume. A priori sample size calculation was performed using G*Power software (Version 3.1, Heinrich Heine University, Düsseldorf, Germany). Assuming a significance level of 5% (α = 0.05), a statistical power of 80% (β = 0.20), a standard deviation of 5500 mm3 derived from a pilot analysis, and a minimum clinically relevant difference of 1500 mm3, the estimated minimum sample size was 113 patients. However, to ensure a more balanced representation between cleft types and to increase the robustness of the analysis, the final sample was expanded to 200 patients, including 100 patients with unilateral cleft lip and palate (UCLP) and 100 patients with bilateral cleft lip and palate (BCLP).
Image Acquisition
CBCT scans were acquired using an i-CAT system (Imaging Sciences International, Hatfield, PA, USA), with a tube voltage of 120 kVp, a minimum field of view (FOV) of 8 cm, and a voxel size ranging from 0.4 to 0.25 mm. Initial image visualization was performed with i-CAT Vision software (Imaging Sciences International). All analyses were carried out under controlled lighting conditions in a darkened room, using a dedicated CBCT workstation (Dell 2408 LCD flat-panel monitor, 1920 × 1200 pixel resolution, 24 inches; Round Rock, TX, USA).
Inclusion and Exclusion Criteria
Inclusion Criteria
Patients with UCLP or BCLP, aged 18 years or older, who underwent orthognathic surgery with Le Fort I osteotomy were included. All patients had both preoperative and postoperative CBCT scans available, with the postoperative examination performed approximately 1 year after surgery. CBCT scans were required to present an adequate FOV allowing complete visualization of the maxillary sinus and paranasal sinus region, as well as sufficient image quality without artifacts that could interfere with the volumetric analysis.
Exclusion Criteria
Patients with a history of craniofacial trauma, intracranial tumors, or paranasal sinus pathologies—such as polyps or tumors—were excluded. Individuals presenting syndromic clefts or other associated craniofacial anomalies were also excluded from the analysis.
Surgical Procedure
All patients included in the study underwent orthognathic surgery involving a Le Fort I osteotomy for maxillary repositioning. The surgical procedure was performed according to the individual treatment plan established through multidisciplinary evaluation, including orthodontic preparation and facial analysis. Maxillary repositioning aimed to correct maxillomandibular discrepancies and improve occlusal relationships and facial balance. The direction and magnitude of maxillary movements varied according to each patient's surgical planning. Although the direction and magnitude of maxillary movements were individualized, most patients underwent maxillary advancement with or without vertical repositioning. Quantitative data regarding surgical movements, although available in clinical records, were not systematically collected for the purposes of this study and are acknowledged as a limitation. No additional orthognathic procedures, such as bilateral sagittal split osteotomy or genioplasty, were performed in the patients included in this study.
Image Processing and Volumetric Analysis
CBCT datasets were exported in DICOM format and analyzed using ITK-SNAP software (Version 3.8.0). Prior to segmentation, all images were manually oriented according to the Frankfurt horizontal plane (Bjerin, 1957) to ensure standardized positioning.
Maxillary Sinus Segmentation in ITK-SNAP
Volumetric segmentation of the maxillary sinuses was performed using ITK-SNAP software (Version 3.8, University of Pennsylvania, Philadelphia, PA, USA). Initially, demographic data, including age and sex, were recorded. CBCT images in DICOM format were imported into the software, and the anatomical identification of the maxillary sinus ostium was used as a reference point for segmentation (Figure 1).
The region of interest corresponding to each maxillary sinus was delineated, and semi-automatic segmentation was performed using the active contour (“Snake”) segmentation method with threshold adjustments. Manual refinement was performed when necessary to ensure accurate delimitation of sinus boundaries.
The region of interest corresponding to each maxillary sinus was delineated, and semi-automatic segmentation was performed using the active contour (“Snake”) method with threshold adjustments. Threshold values were defined based on gray-scale intensity to differentiate air-filled spaces from surrounding bone and soft tissues. Manual refinement was performed when necessary to ensure accurate delimitation of sinus boundaries, particularly in areas with mucosal thickening or image artifacts.
The right and left maxillary sinuses were segmented separately and assigned distinct color labels to facilitate comparative analysis. After segmentation, volumetric measurements were automatically obtained in cubic millimeters (mm3) using the Volumes & Statistics tool. The same segmentation protocol was applied to both preoperative and 1-year postoperative CBCT scans. All volumetric data were recorded in a spreadsheet for subsequent statistical analysis.
Analysis of Maxillary Sinus Lesions
In cases where sinus lesions were identified on CBCT scans, a specific segmentation protocol was applied. Lesions were first identified on axial, coronal, and sagittal reconstructions and subsequently segmented separately from the maxillary sinus using distinct labels. Semi-automatic segmentation with manual refinement was performed to delineate lesion boundaries, followed by three-dimensional verification to ensure volumetric continuity. The volumes of the right and left maxillary sinuses as well as the identified lesions were calculated using the Volumes & Statistics tool. When present, the lesion volume was included in the total maxillary sinus volume, and the percentage of lesion occupancy relative to the corresponding sinus volume was also calculated.
Evaluation of Sinus Alterations
During segmentation, the anatomical boundaries of the maxillary sinus were carefully identified to ensure consistent volumetric measurements. The superior boundary corresponded to the orbital floor, the inferior boundary to the alveolar process of the maxilla, the medial boundary to the lateral wall of the nasal cavity, and the lateral boundary to the zygomatic process of the maxilla. Posteriorly, the boundary was defined by the posterior wall of the maxillary sinus, and anteriorly by the anterior sinus wall. These anatomical landmarks were used to standardize sinus segmentation across all CBCT scans. The following sinus alterations were assessed in both the preoperative and 1-year postoperative (PO1) periods:
Presence and degree of sinus mucosal thickening; Location of the maxillary ostium; Presence or absence of an accessory maxillary ostium; Presence of sinusopathies, including partial or total maxillary sinus opacification, sinus polyps, and mucous retention pseudocysts.
Statistical analysis was performed using SigmaPlot software (Systat Software Inc., San Jose, CA, USA). Data normality was assessed using the Shapiro-Wilk test. Intragroup comparisons between the preoperative and 1-year postoperative (PO1) periods were conducted using the paired Student's t-test for normally distributed variables and the Wilcoxon signed-rank test for nonparametric data. Intergroup comparisons between patients with UCLP and BCLP, as well as comparisons between sides with and without cleft, were performed using the independent Student's t-test or the Mann-Whitney U test, according to data distribution. Results were expressed as mean ± standard deviation, and the level of statistical significance was set at 5% (P < .05).
Statistical analysis was performed using SigmaPlot software (Systat Software Inc., San Jose, CA, USA). Data normality was assessed using the Shapiro-Wilk test. Comparisons of maxillary sinus volume and intrasinus lesion volume between the preoperative and 1-year postoperative (PO1) periods were conducted using the paired Student's t-test for normally distributed variables and the Wilcoxon signed-rank test for nonparametric data. Comparisons between UCLP and BCLP groups, as well as between cleft and non-cleft sides, were performed using the independent Student's t-test for normally distributed data and the Mann-Whitney U test for nonparametric data. Results were expressed as mean ± standard deviation, and the level of statistical significance was set at 5% (P < .05).
Results
Sample Selection and Group Characterization
A total of 200 patients were randomly selected from a population of 935 eligible individuals. Of these, 100 were allocated to the UCLP and 100 to the BCLP group, according to the established inclusion and exclusion criteria (Table 1). Randomization was performed using Microsoft Excel with the = RAND() function, followed by list sorting and sequential allocation of participants to each group, minimizing selection bias.
Patients’ ages ranged from 19 to 42 years (mean: 28.9 years), with detailed age and sex distribution presented in Table 2. In the UCLP group, 46 patients were female and 54 were male, whereas in the BCLP group, 33 were female and 67 were male.
Volumetric Analysis in the Unilateral Cleft Lip and Palate Group
In the UCLP group, no statistically significant differences were observed between the preoperative and postoperative periods for maxillary sinus volume or total volume, on either the cleft or non-cleft side (P > .05). In contrast, lesion volume showed a significant reduction after surgery, reaching null values in the postoperative period (P < .05).
Side-to-side comparison revealed that maxillary sinus volume was significantly smaller on the cleft side in both the preoperative and postoperative periods (P = .017). However, the volumetric variation between the two time points did not differ significantly between sides (P > .05), indicating a similar longitudinal behavior. The detailed volumetric outcomes for maxillary sinus volume, total volume, and lesion volume in both groups are presented in Table 3.
Volumetric Analysis in the Bilateral Cleft Lip and Palate Group
In the BCLP group, a significant reduction in lesion volume was observed in both the right and left maxillary sinuses after surgery (P < .05). Total volume showed a statistically significant increase on both sides in the postoperative period (P < .05). Conversely, isolated maxillary sinus volume did not show significant differences between the preoperative and postoperative periods (P > .05).
Comparison Between the Unilateral Cleft Lip and Palate and Bilateral Cleft Lip and Palate Groups
No statistically significant differences were found between groups for maxillary sinus volume or total volume in the preoperative period (P > .05). However, lesion volume was significantly greater in the BCLP group compared with the UCLP group preoperatively (P = .002).
In the postoperative period, no significant differences were observed between groups for maxillary sinus volume, lesion volume, or total volume (P > .05). Regarding the pre- to postoperative changes, only the reduction in lesion volume remained significantly greater in the BCLP group (P = .012).
Discussion
The hypothesis that the presence of cleft lip and palate would be associated with a significantly greater postoperative reduction in maxillary sinus volume was not confirmed by the findings of the present study. Volumetric analysis demonstrated that both the cleft-affected side and the contralateral side exhibited similar reductions in maxillary sinus volume after Le Fort I osteotomy, regardless of the presence of the malformation. These results indicate that the primary factor responsible for postoperative sinus anatomical changes is the surgical manipulation of the nasomaxillary complex itself rather than the etiology of the cleft.1–4
These findings are consistent with recent studies, such as those by Ahn 1 and Altun, 4 which also reported no statistically significant differences between sides regarding sinus volumetric response following orthognathic surgery. Conversely, they partially diverge from isolated reports, such as those by Bin et al, 18 who attributed greater volumetric impact to the presence of cleft lip and palate. Such discrepancies may be explained by methodological differences, segmentation criteria, and heterogeneity of the analyzed samples.
In the present study, patients with UCLP exhibited a slight postoperative reduction in mean maxillary sinus volume, without statistical significance, whereas the volume of intrasinus lesions was significantly reduced. In contrast, patients with BCLP demonstrated a significant postoperative increase in total sinus volume, accompanied by a marked reduction in lesion volume, although the isolated sinus volume did not change significantly. When comparing cleft and non-cleft sides, the cleft side consistently presented smaller volumes both preoperatively and postoperatively; however, the volumetric variation over time did not differ significantly between sides, indicating a similar surgical response regardless of cleft presence.
These results corroborate previous investigations evaluating maxillary sinus volumetric changes after Le Fort I osteotomy or bimaxillary surgery. Akbulut et al 2 reported sinus volume reduction associated with increased mucosal thickness, suggesting that surgery alters sinus anatomy without necessarily exacerbating pre-existing asymmetries. Similarly, Bin et al 18 observed decreased maxillary sinus volume following orthognathic surgery, independent of cleft involvement.
The significant reduction in intrasinus lesions observed in this study is also consistent with the literature. Eshghpour et al 12 and Othman et al 15 emphasized that Le Fort I osteotomy may contribute to normalization of abnormal sinus spaces, improving ventilation and sinus function. Maxillary repositioning may further enhance physiological drainage and clearance of retained secretions, explaining the postoperative reduction in lesion volume.
Moreover, the absence of significant differences in volumetric variation between cleft and non-cleft sides aligns with the findings of Ahn 1 and Altun, 4 who noted that congenital structural alterations of the nasomaxillary complex in cleft patients are not fully corrected by orthognathic surgery alone. Studies by Koç 13 and Li 14 demonstrated that the magnitude and direction of maxillary movement directly influence sinus volumetric changes, particularly with vertical or anteroposterior displacement. Nevertheless, such movements do not completely eliminate congenital anatomical differences, such as the smaller volume consistently observed on the cleft side.
Comparison between unilateral and bilateral cleft patients revealed that although maxillary sinus and total volumes did not differ significantly between groups, preoperative lesion volume was significantly greater in the bilateral group. This finding suggests that bilateral cleft patients present more pronounced congenital alterations, reflecting greater compromise of the nasomaxillary complex.3–5 Postoperatively, these differences were no longer significant, indicating that orthognathic surgery promotes similar volumetric changes regardless of cleft extent.6,10,12 However, lesion volume variation remained significantly greater in the bilateral group, suggesting more pronounced residual alterations in specific sinus regions.7,16,19
Another relevant aspect concerns the role of sinus mucosal thickness in the interpretation of volumetric findings. Recent studies have demonstrated that mucosal thickening—often associated with chronic inflammatory processes in cleft patients—may interfere with volumetric measurements and mask true changes in maxillary sinus air space.8,9 Additionally, the direction of maxillary repositioning influences external nasal morphology and upper airway patency, which may indirectly affect sinus ventilation.11,20
The interindividual variability of sinus volumes observed in this study may be attributed to factors such as age, sex, facial pattern, and the presence of sinus septa, as reported by Okşayan, 21 Gosau, 10 and Paknahad et al. 19 This heterogeneity highlights the importance of individualized assessment during surgical planning and postoperative follow-up, particularly in bilateral cleft patients, who tend to exhibit more severe and diffuse alterations.3–5
In addition to the exclusion criteria adopted in this study, it is important to acknowledge that other factors may influence maxillary sinus volume. Variables such as age, sex, individual anatomical variability, nasal airflow patterns, and the presence of subclinical inflammatory conditions may affect sinus morphology and volume. Furthermore, variations in surgical technique and postoperative healing responses may also contribute to volumetric changes. Although efforts were made to standardize the sample, these potential confounding factors should be considered when interpreting the results.
In the bilateral group, the postoperative increase in total sinus volume may be explained by the significant reduction of intrasinus lesions, which freed air space, as well as by the magnitude of surgical movements, including transverse and vertical maxillary expansion.13,14 Furthermore, improved postoperative ventilation may have stimulated physiological sinus expansion, as suggested by recent studies. 9 Conversely, in unilateral cleft patients, the reduction in total sinus volume may be related to smaller surgical movements and to trauma to the respiratory epithelium during Le Fort I osteotomy, which may temporarily or permanently compromise mucociliary function.2–5,18
Therefore, maxillary sinus volumetric changes following Le Fort I osteotomy should be interpreted as the result of a complex interaction among congenital anatomical factors, magnitude and direction of surgical movements, impact on sinus mucosa, and pre-existing functional conditions. Although orthognathic surgery does not completely eliminate structural asymmetries associated with cleft lip and palate, it may promote relevant anatomical and functional improvements, particularly regarding reduction of intrasinus lesions and improved ventilation.
Finally, this study has limitations that should be acknowledged. Despite the relatively large sample size, the investigation was conducted at a single center, which may limit generalizability. In addition, inter-observer reliability was not assessed, as all segmentations were performed by a single examiner, which may limit the external reproducibility of the measurements. The absence of functional respiratory assessments and long-term follow-up also restricts understanding of the clinical impact of the observed anatomical changes. Future studies, preferably prospective, multicenter, and integrating volumetric and functional analyses, are needed to further elucidate the effects of orthognathic surgery on the maxillary sinus in cleft lip and palate patients.
Conclusion
Pre- and postoperative volumetric analysis demonstrated that Le Fort I osteotomy resulted in a significant reduction of intrasinus lesion volume, particularly in patients with BVLP, whereas total maxillary sinus volume exhibited changes of smaller magnitude. The cleft-affected side consistently presented lower volumes compared with the contralateral side in both evaluated periods; however, volumetric variation between preoperative and postoperative assessments was similar between sides, indicating a comparable surgical response regardless of cleft presence. These findings suggest that orthognathic surgery plays a relevant role in remodeling paranasal structures and improving maxillary sinus anatomical conditions in cleft lip and palate patients, although it does not completely eliminate congenital structural asymmetries.
Footnotes
Acknowledgements
The authors gratefully acknowledge the financial support provided by the Coordination for the Improvement of Higher Education Personnel (CAPES), Brazil, through a graduate scholarship granted to one of the authors. This study was financed in part by CAPES – Finance Code 001.
Ethical Approval and Informed Consent Statements
This study was approved by the Ethics Committee of the Hospital for Rehabilitation of Craniofacial Anomalies at the University of São Paulo. All individuals in this research agreed to participate in the research and signed the informed consent form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES, (grant number 88887.008018/2024-00).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.