
Abstract
Objective
To assess the incidence of Robin Sequence in the United States and evaluate predictors of early morbidity and mortality.
Design
Retrospective cohort study.
Setting
Epic Cosmos database.
Patients, Participants
Patients with Robin Sequence diagnosed within the first year of life from January 2015 to December 2024.
Interventions
Variables including prenatal drug exposure (PDE), prematurity, intrauterine growth restriction (IUGR), concomitant airway diagnoses, genetic syndromes, and anomalies of the cardiopulmonary, gastrointestinal, or central nervous system (CNS) were captured.
Main Outcome Measure(s)
Incidence across a 10-year period and associations with admission to the neonatal intensive care unit (NICU) and length of stay (LOS), 30-day readmission and ED visit, and one-year mortality through a multivariate logistic regression.
Results
3863 patients were identified, for an incidence of 1 in 3713 live births. NICU admission was significantly associated with PDE, prematurity, IUGR, tracheomalacia, laryngomalacia, cleft palate, and presence of a cardiopulmonary or CNS anomaly. NICU LOS was associated with prematurity, bronchomalacia, and the presence of a gastrointestinal anomaly. 30-day readmission was associated with PDE, prematurity, tracheomalacia, laryngomalacia, cleft palate, cardiopulmonary anomalies, and CNS anomalies. 30-day ED visit was associated with prematurity, tracheomalacia, cleft palate, cardiopulmonary anomalies, and CNS anomalies. One-year mortality was associated with prematurity, IUGR, cardiopulmonary anomalies, and CNS anomalies.
Conclusions
Significant associations were identified between morbidity and mortality and perinatal factors, concomitant airway diagnoses, and the presence of cardiopulmonary and CNS anomalies. These findings underscore the importance of an early comprehensive evaluation for patients with Robin Sequence.
Introduction
Robin Sequence is defined by the triad of micrognathia, glossoptosis, and airway obstruction, resulting from mandibular growth failure during embryologic development which causes superior and posterior displacement of the tongue and subsequent airway compromise. 1 Affected patients can exhibit a range of physical and laboratory findings, including persistent inspiratory stridor, severe sternal retraction, hypoxia, and respiratory acidosis, and are at risk for severe complications such as malnutrition, failure to thrive, and delayed development.2,3 Robin Sequence additionally presents within a wide clinical spectrum, and may occur in isolation, in association with genetic syndromes such as Stickler or DiGeorge syndrome, or in conjunction with additional congenital anomalies involving multiple organ systems.3–5
Although morbidity and mortality in Robin Sequence were historically attributed to respiratory obstruction due to mandibular malposition, 1 more recent reports have identified stronger associations between adverse outcomes and cardiac anomalies, central nervous system (CNS) abnormalities, and involvement of multiple organ systems. 4 These findings have prompted care teams to incorporate additional diagnostic tools into their treatment algorithms such as cardiac ultrasonography, head and brain imaging with computed tomography or magnetic resonance imaging, genetic testing, and specialty consultation.3,4 However, the existing evidence is largely derived from small single-institution cohorts, limiting comprehensive analysis of predictors of morbidity on a populational level.
Robust assessment of risk factors in Robin sequence requires comprehensive understanding of its underlying clinical characteristics by capturing the breadth of its clinical presentations. This study utilized a large national database to assess the incidence of Robin Sequence in the United States, characterize the diagnostic profile of the patient population, and examine predictors of early adverse outcomes. In doing so, this investigation aims to improve understanding of Robin Sequence and highlight key factors requiring need for escalated management.
Methods
Study Design
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 6 Epic Cosmos (Epic Systems Corporation, Verona, WI, USA), a dataset created in collaboration with a community of health systems using Epic, representing more than 300 million patient records from over 1883 hospitals and 42,400 clinics as of January 2026, was queried. Data were accessed through the Epic Cosmos Data Science Virtual Machine (DSVM), a secure analytics environment that supports querying and analysis of de-identified, patient-level records from participating health systems. All analyses were conducted within the DSVM using de-identified data, and no direct patient identifiers were accessed or exported. Infants with Robin Sequence were identified using a standardized DSVM search strategy (Perez Rivera et al). 7 The study period spanned January 1, 2015, through December 31, 2024, and patients were included only if their Robin sequence diagnosis was recorded within the first year of life.
Incidence of Robin Sequence in the United States was determined by calculating the average number of newborns diagnosed throughout the study period among all births documented in Epic Cosmos. Diagnoses were captured using ICD-10 code groupings supplemented by diagnosis name–based terms when necessary to improve sensitivity and reduce misclassification, particularly for conditions without a single uniquely specific ICD-10 code. The search strategy was organized by clinical domains, including perinatal factors, syndromic diagnoses (e.g., Stickler syndrome, Treacher-Collins syndrome, and DiGeorge syndrome), and congenital anomalies by organ system (including cardiopulmonary, CNS, and gastrointestinal [GI] anomalies). Primary outcomes included admission to the neonatal intensive care unit (NICU), NICU length of stay (LOS), inpatient readmission within 30 days of discharge (30-day readmission), emergency department visit within 30 days of discharge (30-day ED visit), and mortality in the first year of life. A subgroup analysis was additionally performed, consisting of patients diagnosed with isolated Robin Sequence, defined by the absence of a concomitant genetic syndrome or congenital anomaly.
Statistical Analysis
Descriptive statistics were utilized to summarize cohort characteristics, including the prevalence of syndromic diagnoses and congenital anomalies by organ system. Categorical variables were reported as counts and percentages, and continuous variables were summarized using mean with standard deviation. Associations between predictors (demographics, syndromic status, and organ-system anomalies) and binary outcomes (NICU admission, 30-day readmission, 30-day ED visit, and mortality within the first year of life) were evaluated through a multivariate logistic regression using grouped variables (e.g., presence of any genetic syndrome, presence of any cardiopulmonary anomaly) to estimate adjusted odds ratios (aORs) with 95% confidence intervals (CIs). Predictors of NICU LOS were assessed among NICU-admitted infants using the same multivariate regression methodology. Since death would shorten NICU LOS, the primary LOS analysis was performed only among patients who did not pass away during their stay in the NICU. P values < .05 were considered statistically significant. Statistical analyses were performed using R (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Incidence and Demographics
In the study period, 9974 patients with a recorded diagnosis of Robin sequence were identified. After limiting the sample to infants diagnosed within the first year of life, the final cohort consisted of 3863 patients receiving care across 307 U.S. institutions. A total of 14,342,918 live births were documented in the study period, corresponding to an incidence of 2.69 per 10,000 live births, or 1 in 3713 live births. Sex was nearly evenly distributed, with 1935 (50.1%) female and 1927 (49.9%) male patients. Race was documented as White for 2298 (59.5%) patients, Black or African American for 228 (5.9%), Asian for 80 (2.1%), Multiracial for 664 (17.2%), and Other or unknown for 593 (15.4%). A total of 1970 infants (51.0%) met criteria for isolated Robin Sequence.
Concomitant Diagnoses
A total of 3265 (84.5%) patients had a cleft of the palate (with or without a cleft of the lip). Airway diagnoses affecting the respiratory tract included laryngomalacia in 688 (17.8%), tracheomalacia in 331 (8.6%), tracheal stenosis in 126 (3.3%), and bronchomalacia in 124 (3.2%) patients. The most frequently documented genetic syndromes were Stickler syndrome (354; 9.16%), DiGeorge syndrome (84; 2.17%), and Treacher-Collins syndrome (69; 1.79%). Chromosomal abnormalities included trisomy 21 (38; 0.98%), trisomy 18 (29; 0.75%), trisomy 13 (7; 0.18%), and chromosomal translocation (25; 0.65%). Several syndromes were rare (≤0.5% each), and no patients were identified with TAR syndrome, Bruck syndrome, or chromosomal deletion (Table 1). Cardiopulmonary anomalies were present in 1029 (26.6%) patients, most commonly atrial septal defect (excluding patent foramen ovale) (712; 18.43%) and ventricular septal defect (407; 10.54%). CNS anomalies were present in 882 (22.8%), including congenital hypotonia (357; 9.24%), microcephaly (327; 8.46%), and cerebral palsy (162; 4.19%). Gastrointestinal anomalies were less frequent, occurring in 103 (2.7%) patients, most commonly intestinal malrotation (51; 1.32%) and anorectal malformation (28; 0.72%) (Table 2).
Syndromic Diagnoses among Infants with Robin Sequence (N = 3863).
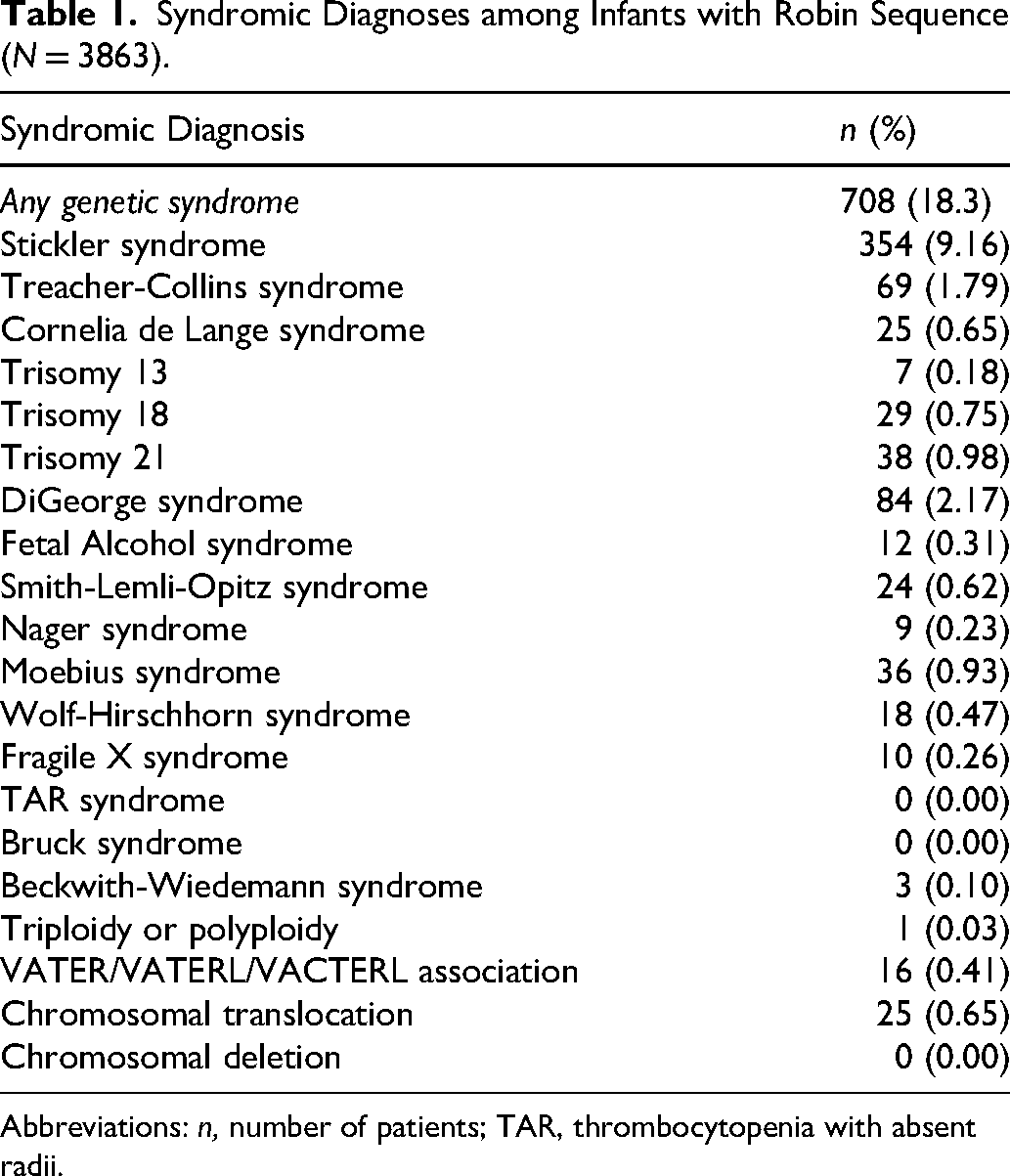
Abbreviations: n, number of patients; TAR, thrombocytopenia with absent radii.
Congenital Anomalies among Infants with Robin Sequence (N = 3863).
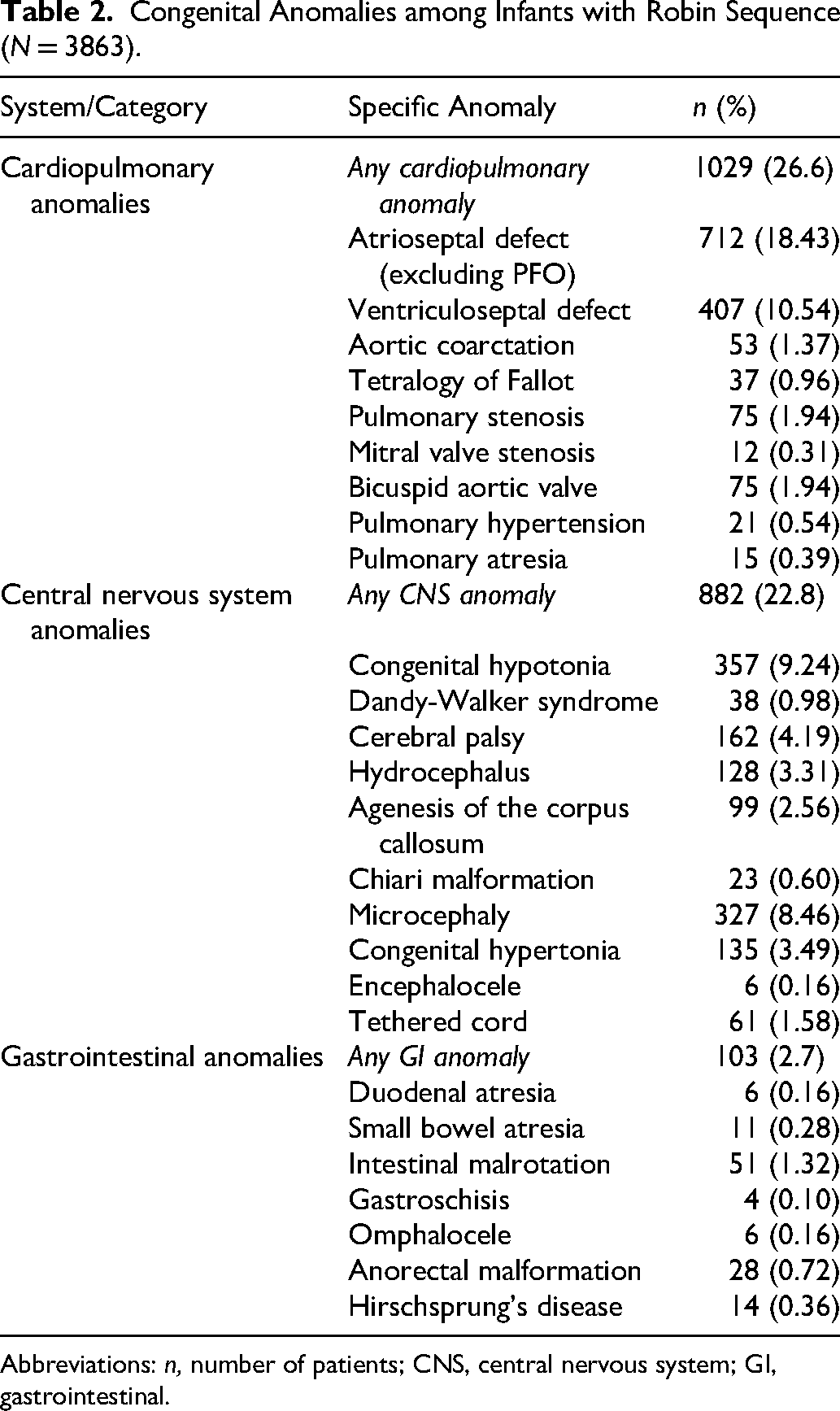
Abbreviations: n, number of patients; CNS, central nervous system; GI, gastrointestinal.
Perinatal Factors and Early Outcomes
Prematurity was recorded in 793 infants (20.5%), intrauterine growth restriction (IUGR) in 183 (4.7%), and in utero drug exposure in 390 (10.1%). Overall, 1387 infants (35.9%) had a NICU admission. Among NICU-admitted infants, mean NICU LOS was 31.52 ± 36.23 days while mean total hospital LOS was 38.49 ± 45.32 days. Mortality within the first year of life occurred in 103 infants (2.7%), and 19 infants (0.5%) died during the NICU admission. Of the 1368 infants discharged from the NICU, 389 (28.4%) had an inpatient readmission within 30 days and 181 (13.2%) had an emergency department visit within 30 days. Among infants who died, the mean age at death was 1.23 ± 1.92 years (Table 3). Cause of death was recorded for only 27 patients; the most common causes of death were respiratory failure in nine infants (33.3%) and cardiac or cardiopulmonary arrest in 6 patients (22.2%).
Perinatal Factors and Early Outcomes (N = 3863).
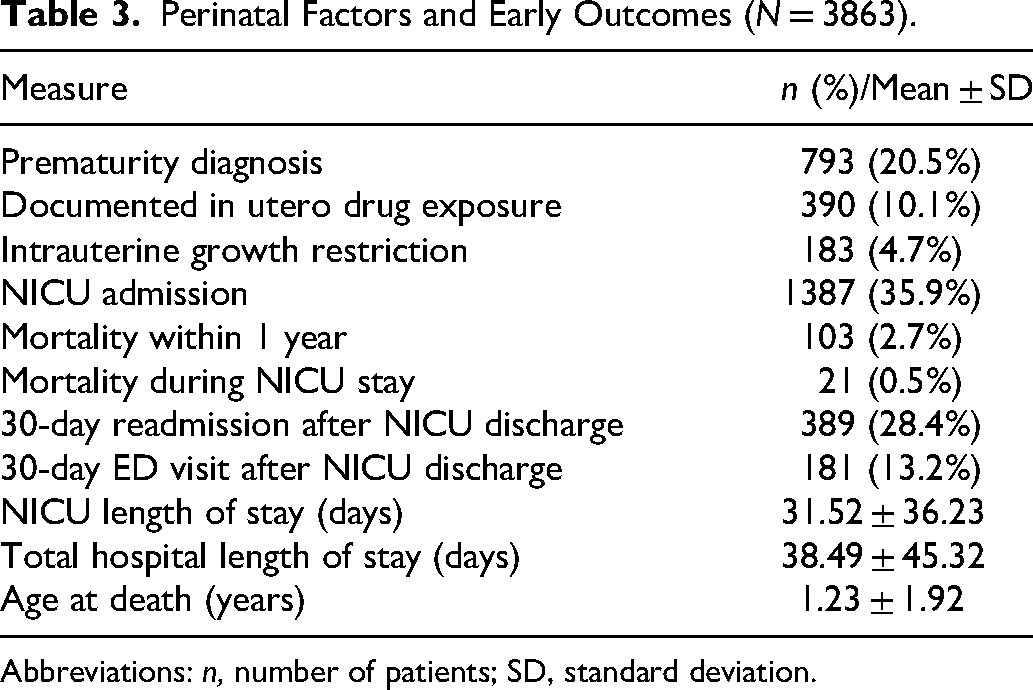
Abbreviations: n, number of patients; SD, standard deviation.
Predictors of Morbidity and Mortality
On multivariable logistic regression adjusting for perinatal factors and comorbidity burden, NICU admission was significantly associated with documented in utero drug exposure, prematurity, IUGR, diagnosis of tracheomalacia, laryngomalacia, or cleft palate, and presence of a cardiopulmonary or CNS anomaly. Among infants with Robin sequence who had a NICU stay and survived to discharge (N = 1366), multivariable analysis demonstrated that prematurity was the strongest independent predictor of longer LOS, in addition to the presence of bronchomalacia or a GI anomaly. On assessment of factors independently associated with 30-day readmission, PDE, prematurity, tracheomalacia, laryngomalacia, cleft palate, cardiopulmonary anomalies, and CNS anomalies were statistically significant. 30-day ED visit was associated with prematurity, tracheomalacia, cleft palate, cardiopulmonary anomalies, and CNS anomalies. One-year mortality was significantly associated with prematurity, IUGR, cardiopulmonary anomalies, and CNS anomalies Multiple diagnostic characteristics exhibited statistically significant inverse relationships with morbidity and mortality. Bronchomalacia was associated with a lower likelihood of NICU admission, 30-day readmission or 30-day ED visit, whereas both the presence of a cleft palate and laryngomalacia exhibited an inverse association with one-year mortality (Table 4).
Multivariate Regression Analysis Demonstrating Associations Between Perinatal Factors and Concomitant Diagnoses with Early Morbidity and Mortality Among Patients with Robin Sequence (N = 3863).
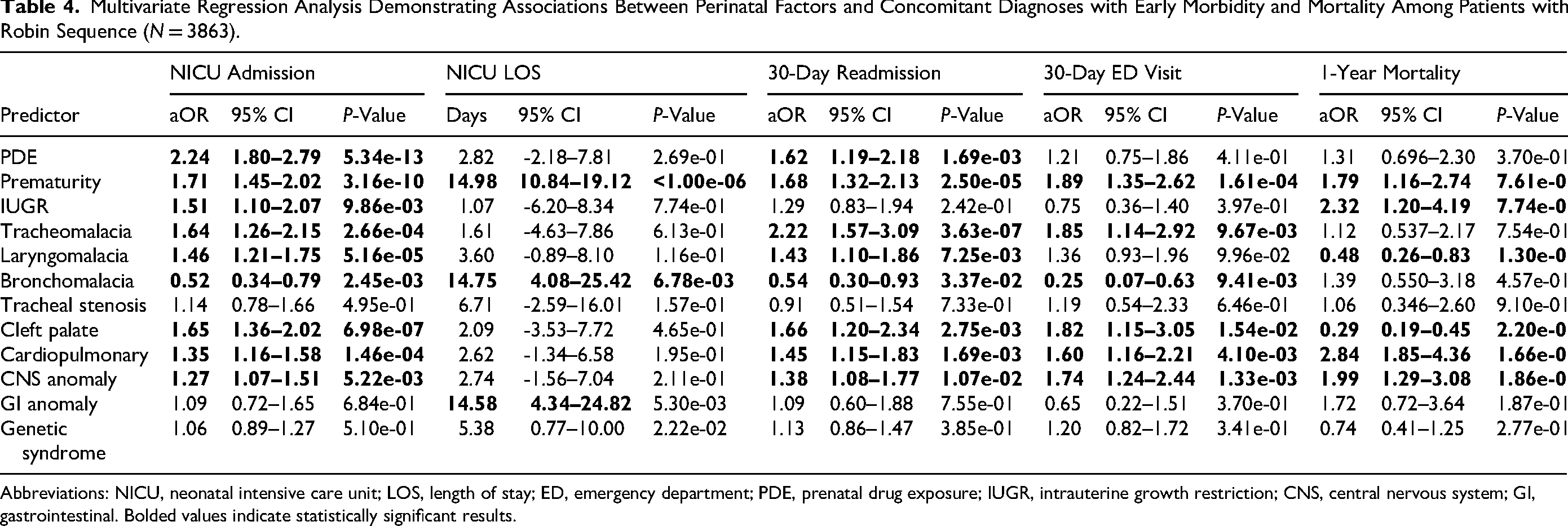
Abbreviations: NICU, neonatal intensive care unit; LOS, length of stay; ED, emergency department; PDE, prenatal drug exposure; IUGR, intrauterine growth restriction; CNS, central nervous system; GI, gastrointestinal. Bolded values indicate statistically significant results.
Among patients with isolated Robin Sequence (N = 1970), NICU admission was significantly associated with PDE, prematurity, IUGR, tracheomalacia, laryngomalacia, and cleft palate, while NICU LOS was associated with prematurity (and bronchomalacia on multivariable regression. 30-day readmission was independently associated with prematurity, IUGR, tracheomalacia, laryngomalacia, and cleft palate, whereas 30-day ED visit was associated with prematurity, tracheomalacia, and cleft palate. Bronchomalacia was inversely associated with NICU admission, and cleft palate was inversely associated with 1-year mortality (Table 5).
Multivariate Regression Analysis Demonstrating Associations Between Perinatal Factors and Concomitant Diagnoses with Early Morbidity and Mortality Among Patients with Isolated Robin Sequence (N = 1970).
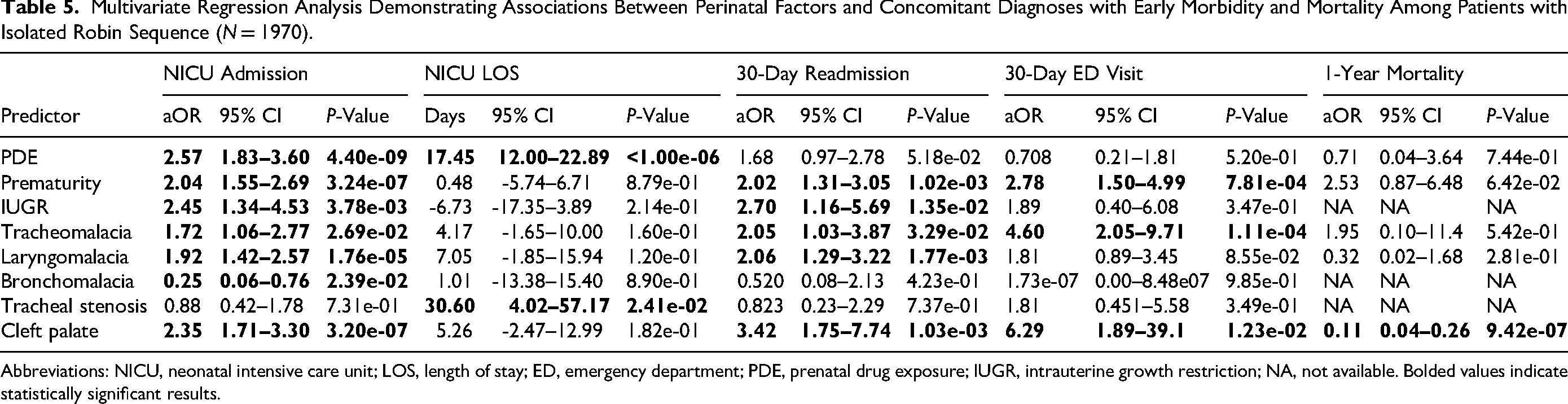
Abbreviations: NICU, neonatal intensive care unit; LOS, length of stay; ED, emergency department; PDE, prenatal drug exposure; IUGR, intrauterine growth restriction; NA, not available. Bolded values indicate statistically significant results.
Discussion
Previous studies investigating comorbidities and their impact on early outcomes in patients with Robin Sequence are either small or single-institution studies. Through this study, we leveraged the Epic Cosmos database to comprehensively characterize a cohort of 3863 patients with Robin Sequence in the United States. This investigation estimated the incidence of Robin Sequence in the United States and the rates of concomitantly diagnosed genetic syndromes and congenital anomalies and examined patient-level associations with early morbidity and mortality.
The incidence of Robin Sequence in the study period was 2.69 in 10,000 live births, or 1 in 3713 live births. Scott and Nader previously examined a cohort of 529 patients with Robin Sequence and identified an incidence of 1.8 in 10,000 live births for isolated Robin Sequence, and 1.4 in 10,000 live births for syndromic Robin Sequence. 8 Separately, Chocron et al. observed an incidence of 5.15 in 10,000 live births in the United States using the Healthcare Cost and Utilization Project (HCUP) Kids’ Inpatient Database (KID), 9 though the authors defined Robin Sequence by the presence of micrognathia and airway obstruction, excluding glossoptosis as a required diagnostic criterion, which may have led to an overestimation. Although the true incidence of Robin Sequence may never be known, this large-scale calculation represents one of the most robust estimations of its incidence in the United States.
Prior populational studies had reported the incidence of syndromic Robin Sequence with great variability, ranging from 6% to 56%.9–12 The most common genetic syndromes identified in the study population were Stickler syndrome (9.2%), DiGeorge syndrome (2.2%), and Treacher-Collins syndrome (1.8%), with patients diagnosed with a genetic syndrome comprising 18.3% of the study population. Previous studies have described significant associations between genetic syndromes and additional markers of morbidity and mortality. Chocron et al. observed a 36.7% rate of syndromic Robin Sequence, and the presence of a genetic syndrome was associated with mortality, longer hospitalizations, and increased rates of tracheostomy. 9 Santoro et al. examined 1294 cases of Robin Sequence across a large network of European centers and estimated the rates of congenital anomalies (19.3%), chromosomal anomalies (6.0%), and genetic syndromes (6.0%). 10 In a clinical consensus report outlining expert recommendations for the evaluation of children with Robin Sequence, Breugem et al. recommend comprehensive assessment of the etiology of Robin Sequence with complete parental history and physical examination, three-generation family pedigree, and longitudinal follow-up with a clinical geneticist. 13
Perhaps the most challenging aspect of caring for infants with Robin Sequence is the complex diagnosis and evaluation of the severity of airway obstruction. Consensus guidelines recommend comprehensive evaluation with diagnostic airway endoscopy, 13 given that endoscopy is often necessary to diagnose dynamic obstruction of the upper airway (laryngomalacia) or obstruction of the lower airway (bronchomalacia), and the presence of secondary airway abnormalities can influence surgical management.14–16 In the study cohort, laryngomalacia, tracheomalacia, tracheal stenosis, and bronchomalacia were identified in 17.8%, 8.6%, 3.3%, and 3.2% of patients, respectively. These concomitant airway diagnoses were significantly associated with early morbidity and mortality, validating the importance of a comprehensive airway evaluation by a pediatric airway specialist. Furthermore, the presence or absence of these commonly associated findings may inform the type of intervention best suited for an affected patient.
Midline anomalies affecting the cardiac and CNS have been significantly associated with morbidity and mortality in patients with Robin Sequence. 4 Although the subset of specific anomalies captured across the literature has varied, prior reports have estimated the incidence of cardiac congenital malformations between 18 and 31%.4,9,17,18 In the current study, the observed rate of cardiopulmonary anomalies was 26.6%, most commonly due to an atrial septal defect (18.4%) or ventricular septal defect (10.5%). In the study cohort, the presence of a cardiopulmonary anomaly was not only significantly associated with early adverse outcomes but was also the strongest predictor of one-year mortality. These findings are consistent with a prior report by Costa et al., who observed a fivefold increased risk of mortality in the presence of cardiac anomalies in a cohort of 181 infants with Robin Sequence. 4
The incidence of abnormalities of the CNS was 22.8%, most commonly congenital hypotonia (9.2%) and microcephaly (8.5%), similar to prior estimates of the burden of CNS comorbidities which have ranged between 7% and 25%.4,9,19 In the present study, CNS anomalies were significantly associated with increased morbidity as well as one-year mortality. This pattern has also been observed in prior literature, including the study by Costa et al. which identified a threefold increased risk of mortality with CNS abnormalities; the authors have since adopted cardiac and cranial ultrasonography as part of the initial assessment of all infants with Robin Sequence at their institution. 4 Separately, in a review of 117 patients with Robin Sequence, Holder-Espinasse et al. proposed cardiac imaging with ultrasonography, and head imaging with computed tomography or magnetic resonance imaging for all patients given the high comorbidity burden. 3
An association between prenatal exposure to teratogenic agents and presence of Robin Sequence has been previously described. In a regional study of the incidence and clinical characteristics of Robin Sequence, Wright et al. observed that 17% of patients with Robin Sequence had intrauterine exposure to teratogenic agents, most commonly methadone. 20 Similarly, in a population-based investigation of multiple national registries, Cleary et al. found that Robin Sequence was over twelve times more likely in methadone-exposed pregnancies. 21 This finding has also been observed in populations with cleft lip and palate specifically, as patients with a cleft and known PDE have exhibited high rates of concomitant Robin Sequence. 22 In the present investigation, PDE was present in 10.1% of the study population. Intrauterine drug exposure was significantly associated with admission to the NICU and 30-day readmission across the overall cohort, as well as an increased LOS in the NICU among patients with isolated Robin Sequence. Although further research on the mechanism and implications of PDE in Robin Sequence is warranted, this finding has significant implications for neonatal patient management and triage, as patients with prenatal exposure to teratogenic agents may not only be at greater risk of Robin Sequence, but may represent a more vulnerable subset of the Robin Sequence patient population.
In the current study, the presence of a cleft palate was inversely associated with one-year mortality in both the overall cohort and in patients with isolated Robin Sequence. This finding is consistent with a prior investigation by Wenger et al., which observed that patients with a U-shaped cleft palate were at lower risk of mortality. 23 However, the prevalence of cleft palate was significantly greater among patients with isolated Robin Sequence in comparison to patients with concomitant genetic syndromes. For that reason, if there is a true colinear relationship between non-syndromic Robin Sequence and cleft palate status, the observed inverse association with morbidity and mortality may be due to confounding. Stratified analyses evaluating associations between palatal morphology and infant morbidity and mortality could help determine the unique impact of cleft palate status on adverse outcomes.
This investigation identified statistically significant associations between comorbidities of the airway, cardiopulmonary system, and CNS, and early morbidity and mortality. These findings support consideration of a pediatric otolaryngology consultation for all patients with Robin Sequence for evaluation of the airway including endoscopic endoscopy (as indicated). Considering the common incidence of a secondary airway anomaly, early airway assessment can potentially identify and address additional airway pathology affecting clinical outcomes. Cardiac and cranial ultrasonography may additionally be of considerable benefit given that anomalies of the cardiopulmonary and CNS have been consistently demonstrated to be some of the strongest predictors of early morbidity and mortality in the Robin Sequence patient population.
This study utilized the Epic Cosmos dataset, which has previously demonstrated utility in examining populations with cleft and craniofacial conditions in the United States.24–26 However, this tool has seldom been employed for more comprehensive analysis of patients with complex craniofacial diagnoses, which are also often limited to small, single-institution cohorts. The current study presents a framework for the potential of Epic Cosmos to leverage the breadth of treatment centers using Epic electronic medical records to study complex and understudied craniofacial conditions. There are notable limitations, however, with use of Epic Cosmos, as the database only includes patients treated at institutions using Epic electronic medical records. This may limit the generalizability of these findings, as patients treated at other institutions may systematically differ from those included in this study. Additionally, the current investigation evaluated associations between diagnostic variables and early outcomes across a large multi-center cohort, with infants potentially undergoing a variety of management strategies and interventions. Therefore, variability in treatment algorithms may have introduced confounding in the dataset, as infants managed with distinct protocols may exhibit variable outcomes. In the future, this large database could be leveraged to explore outcomes when using non-invasive therapeutic modalities like prone positioning or nasopharyngeal airway, or surgical interventions such as mandibular distraction osteogenesis and tongue-lip adhesion.
Although a large patient population was characterized and the incidence of many different genetic syndromes and congenital anomalies were identified, it is possible that some diagnoses were not captured in the analysis. This study did not evaluate the impact of demographic factors such as race, ethnicity, and socioeconomic status on early outcomes; however, given that prior studies have identified racial disparities associated with increased mortality among hospitalized infants with micrognathia, 27 these variables represent an important area of further study. Moreover, since this study only examined patients Robin Sequence in the United States, the burden of comorbidities may be distinct in other countries, and alternative factors may be associated with morbidity and mortality in a global context.
Conclusions
This study presents a robust characterization of the incidence and diagnostic profile of the Robin Sequence patient population in the United States, as well as an analysis of factors associated with morbidity and mortality. The incidence of Robin Sequence across the 10-year study period was one in every 3713 live births. Significant associations were identified between morbidity and mortality and perinatal factors including prematurity and IUGR, concomitant airway diagnoses, and the presence of cardiopulmonary and CNS anomalies. These findings highlight the importance of an early, comprehensive, and multidisciplinary evaluation for all patients with Robin Sequence.
Footnotes
Ethical Considerations
This study accessed the Epic Cosmos database, which is fully de-identified and compliant with the Health Insurance Portability and Accountability Act. This study was therefore exempt from institutional review board approval.
Consent to Participate
Only de-identified patient data were used; patient consent was not applicable.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Not applicable.