
Abstract
This case report aimed to clarify the long-term bone formation from the grafting of octacalcium phosphate granules and atelocollagen complex (OCP/Col) into the alveolar cleft until the completion of orthodontic treatment in 2 patients with unilateral CLA. Both patients underwent OCP/Col grafting at age 9 years and 3 months. Clear bone bridging was observed 6 months or 3 years after grafting, and bone formation was further promoted by the edgewise treatment. The results suggested that the osteogenic induction phase can last for several years in some cases, and it is important to understand this characteristic when formulating treatment plans.
Background
In patients with cleft lip and palate or alveolus (CLP/A), one of the treatments that determines the final outcome is alveolar bone grafting (ABG)—a very important treatment process. Alveolar bone reconstruction in patients with alveolar clefts facilitates the eruption of permanent teeth, stabilizes the upper jaw, and allows for tooth movement.1,2 However, harvesting bone from the ilium or another part of the body is not only surgically invasive but also lowers the quality of life of patients. 3 Therefore, the development of a bone grafting material with functions equivalent to those of autologous bone is desirable.
In patients with CLP/A, using octacalcium phosphate granules and atelocollagen complex (OCP/Col) instead of the bone harvested from the ilium, typically used for bone grafting in the alveolar cleft, reportedly leads to bony bridge formation and cleft-adjacent teeth eruption, suggesting that OCP/Col could be a useful substitute for autogenous bone.4,5 Octacalcium phosphate has been proposed to be a precursor of biological apatite crystals present in bone and teeth.6,7 Octacalcium phosphate promotes osteoblast differentiation, leading to bone regeneration. 8 It has been reported to be more resorbable in vivo than hydroxyapatite or β-tricalcium phosphate (β-TCP). 9 Furthermore, studies of OCP implants using animal models of alveolar bone defects have demonstrated that OCP can fill alveolar cleft defects with new bone. 10 On the clinical trial, OCP/Col were used in cases of sinus floor elevation, socket preservation, cyst, and alveolar cleft procedures, revealing successful clinical results. 5 However, the details of orthodontic treatment intervention and bone formation after OCP collagen grafting, and the final bone formation results after edgewise treatment, remain unclear.
This case report details the long-term prognosis of bone formation during and after orthodontic treatment in 2 patients who were treated with OCP collagen grafting into the alveolar cleft.
Case Presentation
Overview of Clinical Trials of OCP/Col Grafting
The OCP/Col grafting into alveolar clefts was registered in the Japan Medical Information Network (UMIN ID: 000018192) as a phase III clinical trial of guided bone regeneration therapy, and the clinical trial protocol was approved by the Institutional Review Board of the Pharmaceuticals and Medical Devices Agency of Japan (reference Number OCTC14001). Prior to the Phase III clinical trial, preclinical studies were conducted on the safety and bone regeneration of OCP/Col and confirmed that OCP/Col is safe to use, promotes bone regeneration in human bone defects, and retains the potential of an excellent bone replacement material. 11 The Phase III clinical trial was conducted in accordance with the medical protocols and ethical principles of the Declaration of Helsinki, and informed consent and written assent were obtained from all participants. Four patients with CLP/A participated in the clinical trial at Kagoshima University Hospital, but only 2 of them underwent comprehensive treatment, including orthodontic treatment at our hospital, so we report on the long-term progress of these 2 patients.
Postoperatively, observations were made according to predefined trial protocols. Panoramic tomograms and dental radiographs were obtained before and after surgery at 1, 3, 6, and >30 months postoperatively. Further, helical computed tomography (CT) (LightSpeedPlus, GE Healthcare Japan Corporation) was performed preoperatively and at 6 months postoperatively, whereas the digital data of cone-beam CT (CBCT) (3D Accuitomo; J. Morita MFG. Co.) were obtained at 3 months after grafting. For the CT images, excluding the designated helical CT, we used CBCT, which uses fewer X-rays.
In addition to the radiographs specified in the clinical trial protocol, during orthodontic treatment, panoramic tomograms and dental radiographs were taken to confirm the bone formation for tooth movement. After edgewise treatment, to confirm the bone formation and maxillary third molars, panoramic tomograms, dental radiographs, and CBCT were also taken. Although radiographs were taken more frequently than usual during the treatment period, the long-term bone resorption and bone replacement of OCP/Col grafted in the alveolar cleft were unknown, and detailed evaluation of bone formation, including 3-dimensional images, was essential for safe tooth movement. Therefore, we explained the radiation exposure to the patient and obtained their consent. In addition, the purpose of this case report was explained to the patients and their guardians. The patients and guardians were fully informed about the treatment process and the publication of photographs and radiographs, and written consent was obtained.
Surgical Methods of OCP/Col Grafting
The OCP/Col (Toyobo Co., Ltd.) was prepared in 2 steps. First, OCP was prepared by mixing a solution of calcium hydrate with that of sodium phosphate monobasic. 12 This mixture was then enriched with atelocollagen (Nippon Meat Packers) 13 to maintain the spongy form of OCP. Second, the weight ratio of OCP in the OCP/Col complex was determined to be 77%. Thereafter, the mixture was lyophilized. During lyophilization, the OCP/Col was molded into discs (diameter, 9 mm; thickness, 1.5 mm) and cylinders (diameter, 9 mm; thickness, 10 mm). The packaged OCP/Col was sterilized and used for surgery.
The OCP/Col grafting was performed by an experienced surgeon specialized in ABG. This surgery was performed using the same technique as ABG, except for the iliac cancellous bone, which was changed to OCP/Col.
Evaluation of Bone Formation Using CT and CBCT Images
Using the occlusal plane as a reference, CT or CBCT images presented the horizontal cross-section through (1) the root apex (defined as the nasal cavity area), (2) the center of the root length (the middle of (1) and (3), defined as the middle area), and (3) the cement-enamel junction (defined as the tooth cervical area) of the maxillary noncleft central incisors. The width of the alveolar cleft and the measurable inter-root distance were also displayed, as appropriate. All images were presented on the same scale.
History Before OCP/Col Grafting in Cases 1 and 2
The patients were born with nonsyndromic unilateral CLA on the left side. The lip was repaired at the age of 3 months (Case 1, male) or 4 months (Case 2, female). At the age of 4 years and 0 months (Case 1) or 3 years and 11 months (Case 2), the patient was referred to a surgeon to manage the occlusion and visited the Department of Orthodontics at Kagoshima University Hospital, Kagoshima, Japan. In both cases, the primary purpose of the phase 1 treatment was to perform ABG before maxillary left lateral incisor or canine eruption and alignment of the cleft-adjacent teeth. In phase 1 treatment before ABG, mesial rotation of the cleft-adjacent central incisor (Case 1) and lingual inclination of the maxillary right lateral incisor (Case 2) were both corrected using a lingual arch appliance.
Before the maxillary left lateral incisor (Case 1) or canine (Case 2) eruption, a bone graft in the cleft was considered (Figures 1A and 2A). The patients and guardians were informed about the OCP/Col implantation and normal iliac bone grafting, which are part of a phase III clinical trial of guided bone regeneration therapy; they opted for OCP/Col grafting. In both cases, the patient and guardian were informed that if bone formation was not observed in the grafting area of OCP/Col, bone would be harvested from the ilium and grafted, and if the cleft-adjacent teeth did not erupt, tooth traction would be performed after fenestration. The patient and guardian agreed to this treatment plan.

Facial and intraoral photographs and panoramic radiographs in Case 1: (A) Before OCP/Col grafting (age: 8 years and 6 months); (B) before edgewise treatment (age: 15 years and 4 months); (C) postedgewise treatment (age: 17 years and 2 months). OCP/Col, octacalcium phosphate granules and atelocollagen complex.

Facial and intraoral photographs and panoramic radiographs in Case 2: (A) before OCP/Col grafting (age: 8 years and 2 months); (B) before edgewise treatment (age: 15 years and 10 months); (C) post-edgewise treatment (age: 18 years and 3 months). OCP/Col, octacalcium phosphate granules and atelocollagen complex.
Treatment Objectives After OCP/Col Grafting in Cases 1 and 2
The treatment objective for OCP/Col grafting was to restore function through occlusion with bony continuity in the maxillary arch and space closure by the eruption of the cleft-adjacent central incisor. The treatment plan was as follows: (1) OCP/Col grafting in the clefts, (2) after 3 to 6 months from OCP/Col graft after confirming bone formation with CT or CBCT, wearing lingual arch appliance or edgewise appliance on the maxillary teeth and improvement of the distal lingual inclination of the cleft-adjacent central incisor, (3) alignment of cleft-adjacent lateral incisor or canine as needed (in Case 2, mesial movement of maxillary premolars in the cleft side), (4) edgewise treatment for alignment of all teeth after adolescent growth spurt, and (5) retention after debonding of edgewise appliances (in Case 1, composite resin buildups of the maxillary lateral left incisors).
Case 1 Presentation
Treatment Progress and Results in Case 1
At the age of 9 years 3 months, we performed an OCP/Col grafting on the cleft (Figure 3A and B). Cleft width was 11.0 mm and 6.6 mm in the nasal cavity area and middle area, respectively. Root formation of the cleft-adjacent lateral incisors was approximately 1/3 (before OCP/Col grafting in Figure 4A-C). At 3 months after grafting, opaque images were observed in the CBCT images, and bone formation was observed; however, no bone bridging was observed (at 3 m after grafting in Figure 4A, C, and D). At 6 months after grafting, CT revealed increased opacity, and bone bridging was confirmed in the cleft middle area. The inter-root distance between the cleft-adjacent teeth was 4.0 mm in the CT images sliced in the middle area (at 6 m after grafting in Figure 4A-C). At 8 months after grafting, correction of distal inclination by lingual arch appliance of the cleft‒adjacent central incisor (at 8 m after grafting in Figure 4A). At 1 year and 2 months after grafting (during retention of the central incisor after correction of distal inclination), root formation in the cleft-adjacent lateral incisor was approximately 1/2 (at 1 year 2 months after grafting in Figure 4A and C).
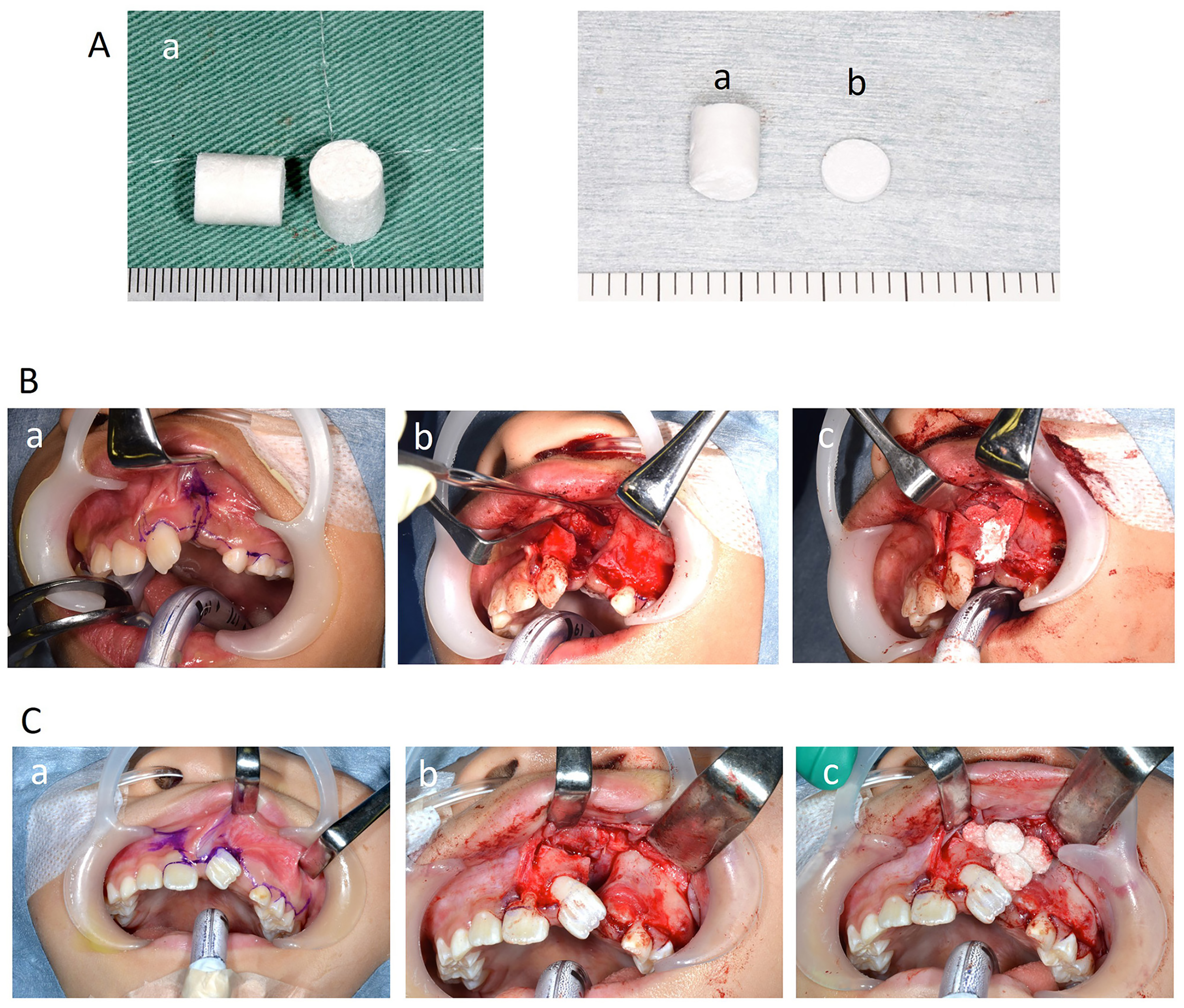
The OCP/Col complex and intraoperative photograph of the OCP/Col complex grafting: (A) OCP/Col complex (a, cylinder-type OCP/Col complex; b: disc-type OCP/Col complex). The minimum scale of the photo ruler is 1 mm. (B) Case 1 (a, Incision line design; b: graft bed formation; c: OCP/Col complex filling); (C) Case 2 (a, Incision line design; b, graft bed formation; c, OCP/Col complex filling). OCP/Col, octacalcium phosphate granules and atelocollagen complex.

Treatment progress in Case 1 from before OCP/Col grafting to alveolar cleft until 1 year and 2 months after grafting: (A) intraoral photographs; (B) helical CT images (a, nasal cavity area; b, middle area; c, tooth cervical area); (C) Periapical radiographs, (D) CBCT images (a, nasal cavity area; b, middle area; c, cervical area). OCP/Col, octacalcium phosphate granules and atelocollagen complex; CT, computed tomography, CBCT, cone-beam computed tomography.
At 2 years and 2 months after grafting, the cleft-adjacent lateral incisor erupted (at 2 years 2 months after grafting in Figure 5A). At 2 years and 7 months after grafting, opaque images indicating bone formation were observed in the CBCT images, and bone bridges were confirmed in the nasal cavity, middle, and tooth cervical areas. The inter-root distance between the cleft-adjacent teeth was 2.7 mm in the CBCT images sliced by the middle area (at 2 years 7 months after OCP/Col grafting in Figure 5B and C). At 6 years and 0 months after grafting, sufficient opacity was observed on dental images before edgewise treatment (at 6 years 0 month after grafting in Figure 5A and C). At 6 years and 5 months after grafting (age of 15 years 8 months), edgewise treatment was started (Figure 1B, at edgewise treatment in Figure 5A). Alignment of the maxillary teeth was initiated using a preadjusted edgewise appliance (0.018 × 0.025 inches). After leveling (0.016 × 0.022 NiTi), discrepancies in the left class II and midline were corrected using midline and left class II elastics (0.016 × 0.022 SS). The total duration of the edgewise treatment was 17 months. The maxillary left lateral incisor was repaired using composite resin buildups for enamel defects or esthetic improvement of the tooth shape (Figure 1C). In the CBCT images, although the bone was thin on the labial side of the maxillary left lateral incisor, sufficient bone bridges were confirmed in the nasal cavity and middle and tooth cervical areas, other than the incisive canal. The inter-root distance between cleft-adjacent teeth was 2.8 mm in the CBCT images sliced by the middle area (at 7 years 10 months to 8 years 1 month after grafting and postedgewise treatment in Figure 5A-C).

Treatment progress in Case 1 from 2 years and 2 months after OCP/Col grafting to the alveolar cleft until postedgewise treatment: (A) Intraoral photographs; (B) CBCT images (a, nasal cavity area; b, middle area; c, tooth cervical area); (C) Periapical radiographs. The brackets in the figure indicate the age at the time of the radiograph. OCP/Col, octacalcium phosphate granules and atelocollagen complex; CBCT, cone-beam computed tomography.
Case 2 Presentation
Treatment Progress and Results in Case 2
At the age of 9 years 3 months, OCP/Col grafting was performed on the cleft (Figure 3A and C). Cleft width was 11.0 mm and 4.0 mm in the nasal cavity area and middle area, respectively. Root formation in the cleft-adjacent canines was approximately 2/3 (before OCP/Col grafting in Figure 6A-C). At 3 months after grafting, a cleft-adjacent canine erupted, and opaque images showing bone formation in the CBCT images were observed; however, bone bridging was not confirmed. Since there was a bone distal to the apex of the cleft-adjacent central incisor, correction of distal inclination was initiated using a lingual arch appliance (at 3 m after grafting in Figure 6A, C, and D). At 5 months after grafting, we used a sectional arch to improve the distal inclination of the cleft-adjacent central incisor. At 6 months after grafting, CT images showed increased opacity, and bone formation was confirmed in the middle area of the alveolar cleft; however, the bone bridge was very thin. Inter-root distance between cleft-adjacent teeth was 10.2 mm and 7.2 mm in the CT images sliced by the nasal cavity and middle area, respectively (at 6 m after grafting in Figure 6A-C). At 11 months after grafting, the distal inclination of the cleft-adjacent central incisor had improved. There was no depression in gingival morphology; however, no bone formation was observed in the distal part of the root of the cleft-adjacent central incisor in the periapical radiographs (at 11 months after grafting in Figure 6A and C). While the central incisor adjacent to the cleft with improved distal inclination was retained using a lingual arch appliance, the erupted maxillary left premolar was moved mesially. At 2 years and 0 months after grafting, bone formation was observed distal to the root of the central incisor in the periapical radiograph (at 2 years 0 month after grafting in Figure 6A and C).

Treatment progress in Case 2 from before OCP/Col grafting to alveolar cleft until 2 years after grafting: (A) Intraoral photographs; (B) helical CT images (a, nasal cavity area; b, middle area; c, tooth cervical area); (C) Periapical radiographs, (D) CBCT images (a, nasal cavity area; b, middle area; c, cervical area). The brackets in the figure indicate the age at the time of the radiograph. OCP/Col, octacalcium phosphate granules and atelocollagen complex; CT, computed tomography; CBCT, cone-beam computed tomography.
At 3 years and 0 months after grafting, the mesial movement of the premolars with the lingual arch appliance continued. Bone bridges were observed in the CBCT images sliced by the cleft middle and tooth cervical areas; however, no bone bridges were observed in the nasal cavity area. Although bone formation was observed in the middle of the cleft area—excluding the incisive canal—it was not observed at the distal apical area of the root of the cleft-adjacent central incisor, particularly in the palatal side of the tooth cervical area. Inter-root distance between cleft-adjacent teeth was 8.4 mm and 5.4 mm in the CBCT images sliced by the nasal cavity and middle area, respectively (at 3 years 0 month after OCP/Col grafting in Figure 7A-C). Dental images before edgewise treatment at 6 years and 7 months after grafting showed opacities comparable to those observed 3 years after grafting (Figure 2B, at 6 years 7 months after grafting in Figure 7A and C). At 6 years and 11 months after grafting (age 16 years and 2 months), edgewise treatment was initiated (at edgewise treatment in Figure 7A). The alignment of the teeth was initiated using a preadjusted edgewise appliance (0.018 × 0.025 inches). After leveling (0.016 × 0.022 NiTi) was completed, the maxillary space was closed with an elastic chain (0.016 × 0.022 SS). After edgewise treatment, optimal occlusion was established (Figure 2C). The total duration of the edgewise treatment was 24 months. On the CBCT images, bone bridges were confirmed in the areas from the nasal cavity to the tooth cervical area. In the nasal area image of the CBCT, there was a part where bone formation was not observed at the distal root apex of the central incisor, but in the nasal cavity area and tooth cervical area images, new bone formation was clearly confirmed after edgewise treatment. Inter-root distance between cleft-adjacent teeth was 4.1 mm and 2.4 mm in the CBCT images sliced by the nasal cavity and middle area, respectively (at 8 years 11 months after grafting and post edgewise treatment in Figure 7A-C).

Treatment progress in Case 2 from 3 years after OCP/Col grafting to the alveolar cleft until postedgewise treatment: (A) Intraoral photographs; (B) CBCT images (a, nasal cavity area; b, middle area; c, tooth cervical area); (C) Periapical radiographs. The brackets in the figure indicate the age at the time of the radiograph. OCP/Col, octacalcium phosphate granules and atelocollagen complex; CBCT, cone-beam computed tomography.
Discussion
Root Distance Between the Cleft-Adjacent Tooth and the Timing of Bone Formation
In both cases, the first bone formation in the cleft after OCP/Col grafting began from the vertical center between the nasal and cervical sides of the alveolar cleft. In Case 2, bone formation was slower than in Case 1. Cleft width was almost the same between Cases 1 and 2; however, Case 1 had a lateral incisor while Case 2 did not. Six months after grafting, the root-to-root distance of the cleft adjacent teeth in Case 2 (7.2 mm) was greater than that in Case 1 (4.0 mm), probably because the canine in Case 2 erupted with a greater mesial inclination than the lateral incisor in Case 1. The success of ABG is associated with the eruption status of the adjacent teeth in the alveolar cleft at the time of surgery. Because tooth germs adjacent to the alveolar cleft erupt from the newly formed bone, they are thought to contribute to the suppression of grafted bone resorption.14,15 Therefore, the closer the root-to-root distance is to the alveolar cleft, the greater the likelihood of bone formation within the cleft, suggesting a similar situation for the OCP/Col grafting. In Case 1, the formation of a bone bridge was observed approximately 6 months after OCP/Col implantation, and bone formation continued smoothly thereafter, with the lateral incisor adjacent to the alveolar cleft also erupting. It has been reported that OCP/Col facilitates bone regeneration better than OCP alone, 16 and OCP granules in OCP/Col are completely converted to bone-like apatite within 6 months after grafting. 10 Therefore, although careful confirmation of bone formation is necessary, it was suggested that in cases where the root-to-root distance of the cleft adjacent teeth is narrow, bone formation may be observed approximately 6 months after OCP/Col grafting.
Bone Formation Over Several Years
In contrast, in Case 2, sufficient bone bridging was not observed even at 6 months after grafting. It has been reported that the OCP granules in OCP/Col are completely transformed into bone-like apatite within 6 months of implantation in an in vivo study. 10 However, bone formation in Case 2 was clearly delayed, and the cause was unclear.
The slow bone formation observed in Case 2, which occurred over several years after OCP/Col grafting into alveolar clefts during the growth period, is a phenomenon not observed in grafted bone after ABG. For successful bone grafting using iliac bone harvest in patients with CLP, it has been reported that the iliac cancellous bone must be able to withstand pressure from the surrounding soft tissues and scar tissue during the early stages of bone formation, as compression can lead to bone resorption. 17 The OCP/Col provides a scaffolding necessary for bone formation that can withstand soft tissue pressure, suggesting the possibility of bone formation while undergoing slow resorption.13,18 In Case 2, sufficient bone formation was still insufficient even 1 year later after OCP/Col grafting. However, the usual gingival depression was not observed, suggesting that OCP/Col may prevent soft tissue compression and maintain the scaffold necessary and high space-making capacity for bone remodeling. In addition, after OCP/Col grafting, orthodontic treatment was performed to shorten the inter-root distance near the alveolar cleft within the range of the existing bone. 19 Between 1 and 3 years after grafting, little tooth movement was observed around the alveolar cleft; however, bone formation was confirmed. These results suggest that if OCP/Col grafting is performed on an alveolar cleft during the period of active bone remodeling during growth, bone formation after OCP/Col grafting is likely to be slower than 6 months in cases with a large root distance of cleft-adjacent teeth, such as in Case 2. On the other hand, the OCP/Col scaffold may induce bone remodeling through growth, and it was also suggested that narrowing the inter-root distance between the alveolar clefts through orthodontic treatment may also contribute to the promotion of bone formation over several years.
Three years after grafting, good bone bridging was observed in Case 1; however, although bone bridging was observed in Case 2, incomplete bone formation was observed on the nasal or palatal sides of the dental cervical region. After OCP/Col grafting, bone formation first occurred in the vertical center of the alveolar cleft, and slowly progressed to the apical and dental cervical regions over the course of 2 to 3 years after grafting. In Case 2, the radiographic findings before edgewise treatment were similar to those seen 3 years after grafting. Regarding the relationship between ABG and bone formation due to tooth movement, it has been suggested that functional stress caused by tooth movement using edgewise appliances may improve some of the poor bone bridges. 20 After edgewise treatment, although there were some areas on the nasal side where bone formation was insufficient, bone formation was clearly promoted, demonstrating that the opacity image on the radiographic image was bone formation, and also indicates that normal remodeling due to orthodontic forces occurred in these bones.
Clinical Implications for Long-Term Bone Formation
These results suggest that OCP/Col grafting into the alveolar cleft is an effective bone substitute material that can replace autogenous bone during the growth phase in patients with cleft lips and alveolus. On the other hand, when planning treatment, it is important to be aware that a long-term osteogenic induction period spanning several years may be required. In procedures such as dental implant placement, rapid bone formation is desired at the site where the bone filler is grafted; therefore, slow bone formation is undesirable. However, in patients with growing alveolar clefts, if bone formation in the cleft area is achieved to a certain extent by the time the pubertal growth spurt of the jawbone has ended and permanent teeth have erupted, before edgewise treatment to establish final occlusion, there are often no major treatment problems. When autologous bone grafting is performed on alveolar clefts before the eruption of the lateral incisors and canines adjacent to the cleft, tooth movement must be initiated early to prevent resorption of the grafted bone.21–24 However, the slow bone formation of OCP/Col allows ample time for tooth movement to begin in the bone-forming area after grafting, which means there is a high possibility that the frequent hospital visits required in the early stages after grafting, which are required for autologous bone grafting, can be reduced. In some cases, this may reduce the burden on the patients and surgeons, and it has been suggested that OCP/Col might be useful as a bone-inducing material for alveolar clefts during the growth period. However, since bone formation after OCP/Col grafting is slow, transplantation of this bone filler is not suitable if you want to start tooth movement early; thus, we need to select cases that fit the treatment plan.
Long-Term Treatment Outcomes of Other Major Bone Graft Materials Used in Alveolar Cleft Reconstruction
β-Tricalcium Phosphate
Previous studies have used several artificial materials for ABG in patients with CLP. 2 Specifically, β-TCP has been widely reported as an artificial material that does not interfere with the eruption of adjacent lateral incisors and canines and allows for successful orthodontic treatment. Clinical studies, in which β-TCP was transplanted into growing patients with CLP evaluated by CBCT imaging, have described average bone formation rates of 65% and 73% at 6 or 12 months after β-TCP transplantation in the alveolar cleft, respectively.25,26 Moreover, β-TCP transplantation efficiency for alveolar bone defects has been suggested to be potentially enhanced by tissue engineering techniques that combine β-TCP with growth factors, mesenchymal stem cells, or other transplant materials, and by modifying the physical properties of β-TCP. 2 In a clinical study using bone marrow mononuclear cells (BMMNC) and β-TCP granules to repair alveolar clefts, the mean bone formation rate in the BMMNC/β-TCP transplant group was 54.9% after a 12-month follow-up. 27 Although the rate of bone formation after β-TCP grafting in alveolar clefts varies among studies, no differences have been reported in bone formation rate compared to ABG using the iliac bone, demonstrating the effectiveness of β-TCP grafting in alveolar cleft reconstruction.25–27 However, the longest follow-up period observed using 3D evaluation after β-TCP transplantation for the alveolar cleft was 12 months.
Decalcified Bovine Matrix
Decalcified bovine matrix (DBM), displaying a porous structure and promoting bone formation through bone conduction, has also been considered an alternative to autogenous bone grafting for alveolar clefts. 2 A study evaluating long-term DBM and iliac crest graft effects in autogenous bone grafting in growing patients with unilateral CLP/A using CBCT at 14 days and 6 months postgraft, 28 described bone retention rates of 70% and 69% in the DBM and iliac crest graft groups, respectively, leading to the conclusion that in the short term, DBM and iliac crest grafts yield similar bone formation. Although this study included long-term follow-up, distinguishing between existing and newly formed bones was not possible at an average of 63 months postgraft, making the bone volume assessment method used in the short term inapplicable. Therefore, a different score was used. Bone formation evaluation using CBCT 63 months later (on average) yielded no statistically significant difference between DBM and iliac crest grafts. However, DBM grafts were suggested to induce less bone formation in the clefts compared to iliac crest grafts. 28 This study appears to represent the longest follow-up period in a study involving BDM transplantation in the alveolar cleft.
Resorbable Collagen Matrix With Recombinant Human Bone Morphogenetic Protein-2
In maxillofacial surgery, recombinant human bone morphogenetic protein-2 (rhBMP-2) application has been widely studied, including that in alveolar cleft repair. It has been used in combination with various scaffold materials.29–32 In a randomized clinical trial of growing patients with unilateral CLA who received grafting of an rhBMP-2-containing absorbable collagen matrix, bone graft rates after rhBMP-2 assessed using CBCT after 12 months, were 74.4% and 75.1%, alongside the reported result that bone formation by absorbable collagen matrix containing rhBMP-2 transplantation is comparable to that achieved by iliac bone grafting at 12 months postsurgery.31,32 Furthermore, DBM could reportedly serve as a suitable carrier for rhBMP-2, an osteoinducible material for alveolar clefts. 29 This described a success rate of 97.2% for alveolar cleft repair using rhBMP-2/DBM at 2 years posttransplantation, being significantly higher than the 84.2% success rate of iliac crest grafts. However, caution is required in interpreting these results as they involve a 2D rather than 3D evaluation. Another study, in growing patients with unilateral or bilateral CLP/A, alveolar cleft repair using rhBMP-2/DBM scaffold material has reported comparable bone formation 6 to 9 months post-DBM/BMP-2 transplantation to that observed with iliac crest grafts, although the bone replenishment rate by CBCT assessment was 32%. 33 These results indicate certain variation in the bone formation degree as research biases, such as cleft type and evaluation timing, cannot be eliminated. However, in short-term evaluations of 6 to 12 months, all studies indicated that BMP-2 induced bone formation in alveolar clefts equivalent to or better than that in iliac crest grafts, indicating that BMP-2 is a useful bone graft material. However, no 3D reports on long-term prognosis beyond 12 months were identified concerning BMP-2.
Comparison of OCP/Col and Other Materials
Among patients with CLP/A who underwent OCP/Col transplantation to the alveolar cleft, one case had a bone regeneration rate of 0.32 at 6 months post-CT evaluation, although the average was 0.87 ± 0.27, indicating generally favorable results. 5 Another study compared OCP/Col and iliac crest grafting, yielding no significant difference. 4 These results suggest that the degree of bone formation from OCP/Col at 6 months posttransplantation in growing patients with cleft might be comparable to that of β-TCP, DBM, and rhBMP-2. However, no clinical studies compared these under the same conditions, and few studies reveal long-term treatment outcomes. Therefore, further clinical research would be required. However, in this case report, bone formation after OCP/Col grafting for alveolar cleft grafting continued over a long period, and interestingly, bone formation was promoted even after 12 months. This phenomenon has not been reported with other materials. To reliably evaluate the long-term clinical outcomes of alveolar bone reconstruction, a follow-up period of at least 12 months is recommended; however, a longer follow-up period may be necessary for OCP/Col grafting in alveolar clefts. In addition, because 2D evaluations may overestimate the status of the bone graft when assessing the effectiveness of alveolar bone reconstruction, 34 3D imaging techniques using CT and CBCT should be used to carefully observe long-term bone formation.35,36
When selecting a bone-inducing material for alveolar clefts, the characteristics of each artificial material must be considered. Long-term results suggest that OCP/Col is useful as a bone-inducing material to replace the iliac bone. However, only 2 unilateral CLA cases have completed long-term follow-up studies up to the end of orthodontic treatment. In the future, it will be necessary to increase the number of cases, and also check the progress of unilateral CLP and bilateral CLP cases, and consider long-term evaluations of bone formation depending on the condition of the alveolar cleft and the timing of the orthodontic treatment intervention.
Long-Term Prognosis-Related Adverse Events
No OCP/Col and β-TPC-related cleft grafting failure rates have been described. For DBM grafting, 3 out of 13 cases reportedly required rebone grafting using autogenous bone. 37 Regarding BMP-2, a meta-analysis was performed due to the high number of cases involving transplantation to the cleft, revealing no different failure rates from those for iliac crest transplantation. 38 Concerning other adverse events, BMP receptors are present in cancer cells, raising concerns about the possibility of cancer induction after rhBMP-2 treatment. Recombinant human bone morphogenetic protein-2 is frequently used in orthopedic surgery to promote bone regeneration after lumbar fusion; studies on the related risk of cancer are thus ongoing. In this retrospective cohort study, following patients for at least 3 years, rhBMP-2 administration during lumbar fusion was not associated with an increased subsequent risk of cancer. 39 Moreover, no studies of malignant transformation after rhBMP-2 grafting for the alveolar cleft have been published. 40 The average rhBMP-2 dose commonly used for clefts is 1.5 to 4.2 mg, 40 being considerably below the 40 mg dose associated with an increased risk of malignant transformation, potentially explaining why malignant transformation has not been reported with the use of rhBMP-2 in reconstructive surgery for the alveolar cleft. Nonetheless, the underlying details remain unclear. Similar to rhBMP-2, no cases of malignant transformation have been reported after transplantation to the alveolar cleft with other materials such as OCP/Col. However, reports on long-term prognosis remain scarce; careful follow-up would thus be necessary.
Conclusions
In 2 patients with cleft lip and alveolus, OCP/Col was grafted into the alveolar cleft at the age of 9 years during the growth period, and long-term follow-up observation was performed. In both cases, sufficient bone bridging was confirmed during orthodontic treatment, suggesting that OCP/Col could serve as an effective autologous bone substitute for grafting into alveolar clefts. However, the osteogenic induction phase can last for several years in some cases, and it is important to understand this characteristic when formulating treatment plans.
Footnotes
Acknowledgments
The authors would like to express our deepest gratitude to Professor Emeritus Shinji Kamakura and Professor Osamu Suzuki for their efforts in the development of OCP/Col. Moreover, the authors are grateful for the assistance of the clinical staff at Kagoshima University Hospital.
Ethical Approval and Informed Consent
The 2 patients whose progress is described in this case report participated in a phase III clinical trial of bone regeneration induction therapy using OCP/Col, which was registered with the Medical Information Network in Japan (UMIN ID: 000018192). The clinical trial protocol was approved by the Institutional Review Board of the Pharmaceuticals and Medical Devices Agency of Japan (reference Number OCTC-14001). The patients and their guardian(s) were informed of the publication of the images associated with the 2 cases, and written consent was obtained.
Authors’ Contributions
Aya Maeda-Iino contributed to writing—original and revised drafts, project administration, investigation, methodology, resources, and validation. Kanako Marutani and Shoko Nakagawa contributed to writing—original and revised drafts, investigation, resources, and validation. Toshiro Kibe contributed to writing—original and revised drafts, funding acquisition, investigation, methodology, resources, and validation. Hideto Saijo contributed to writing—original and revised drafts, investigation, resources, and validation. Norifumi Nakamura contributed to writing—original and revised drafts, funding acquisition, project administration, investigation, methodology, resources, and validation. Shouichi Miyawaki contributed to writing—original and revised drafts, project administration, investigation, methodology, resources, validation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Grant-in-aid for Scientific Research 23K09373 from the Japan Society for the Promotion of Science.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The data used in this case report were obtained from patients who participated in a clinical trial of OCP/Col grafting, conducted with clinical trial implementation costs provided by Toyobo Co., Ltd.
Data Availability
The dataset analyzed during current case report contains personal patient information, so only the data necessary for analysis are made public, but are available upon reasonable request from the corresponding author.