
Abstract
Costochondral grafts (CCGs) are widely used for mandibular condyle reconstruction in children due to their growth potential, yet their unpredictable behavior remains a challenge. We present a rare case of progressive CCG overgrowth in a 17-year-old male with hemifacial microsomia, resulting in severe facial asymmetry despite prior corrective surgeries. Clinical assessment revealed a 2.5 cm ramus discrepancy and marked mandibular deviation. Management required staged surgical correction, including graft excision, osteotomies, and genioplasty. This case illustrates the potential for extreme CCG overgrowth beyond skeletal maturity and emphasizes the need for vigilant long-term surveillance and individualized treatment planning.
Introduction
Hemifacial microsomia (HFM) is the second most common congenital craniofacial anomaly after cleft lip and palate, characterized by hypoplasia of structures derived from the first and second branchial arches. The incidence ranges from 1 in 3500 to 1 in 5600 per live births in the United States with several studies suggested 3:2 male predominance and almost 90% cases affected right facial side. 1 Reconstructive treatment of HFM aims to restore facial symmetry, jaw function, and occlusion. Surgical strategies depend on the severity of the craniofacial anomalies and typically involve skeletal and soft tissue reconstruction. A systematic review on the treatment strategies for HFM revealed that maxillofacial surgery is among the most common strategies after orthodontic and orthopedic treatments, especially in severe cases.1,2
Mandibular distraction osteogenesis (MDO) and bone grafting are key surgical options for correcting mandibular hypoplasia in HFM. While bone grafts (eg, costochondral, iliac, or fibular) augment underdeveloped bone, MDO promotes endogenous bone growth by gradually lengthening the mandible, with each method selected based on the patient's anatomy and growth potential.3,4
Costochondral grafts (CCG) are somehow preferred due to their biological compatibility, growth potential, and structural adaptability.5,6 However, CCGs are associated with unpredictable complications, including overgrowth, resorption, ankylosis, and functional impairment.6–8 Although found to be the source of graft with the highest resorption rate (64.1%), 9 overgrowth can be as high as 20% to 50%.6,7,10 Overgrowth is particularly problematic in adolescents, often necessitating revision surgery due to progressive facial asymmetry and malocclusion. 11
This case report details a severe instance of CCG overgrowth in an adolescent with HFM, resulting in profound facial asymmetry and functional deficits that required a staged, multidisciplinary surgical approach. We highlight the challenges in managing extreme graft-related complications and discuss implications for alternative reconstructive strategies.
Case Presentation
A 17-year-old male presented with progressive facial asymmetry and functional impairment due to overgrowth of a CCG placed for reconstruction of the left mandibular condyle. The patient was born with congenital left HFM, characterized by mandibular hypoplasia, moderate soft tissue deficiency, an occlusal cant, a malpositioned left ear lobule, and an absent auricle. At the age of 10 years (Figure 1), he underwent CCG involving 2 costal cartilage grafts—one to reconstruct the left mandibular condyle via a submandibular approach and another to augment the left zygomatic body and temporal bone via a coronal approach. An orthodontic splint was placed postoperatively to guide occlusion.

Index Surgery of CCG Placement at the Age of 10 Years Old: (A) Presentation Before Surgery at 10 Years Old; (B) Intraoperative CCG Placement on Left Mandible and Zygoma; (C) 1 Month After CCG Showed Better Symmetry; (D) Asymmetry Has Been Noted 6 Months After CCG; (E) Worsened Asymmetry 2 Years After CCG; Occlusion (F) Before CCG; (G) Right After CCG; and (H) 2 Years After CCG.
Although initial results were satisfactory, rightward facial deviation was noted as early as 6 months postoperatively. Progressive overgrowth of the CCG continued through adolescence, resulting in a severe asymmetry by age 16. Clinical and radiographic evaluations revealed a 25 mm discrepancy in mandibular ramus length between the left (pseudocondyle) (83 mm) and right (58.6 mm) sides, with the mandible deviated 34.5° toward the right. Preoperative maximal incisival opening (MIO) was 32 mm.
The patient underwent a first corrective surgery, which included Le Fort I osteotomy with open reduction and internal fixation (ORIF), vertical ramus subsigmoid osteotomy (VRSO), right coronoidectomy, and excision of the overgrown left CCG with mandibular fixation. Postoperative assessment showed a significant improvement, with the mandibular deviation reduced by 25.9°, from 34.5° to 8.6° (Figure 2), reduction of pseudocondyle length to 69.1 mm, and postoperative MIO 25 mm. However, residual asymmetry remained, including midline shifts of 3.5 mm in the maxilla and 8 mm in the mandible. Due to persistent deformity and malocclusion, a second corrective surgery was performed 4 months after the first procedure. Plate fracture on the left mandible was found intraoperatively. The second surgery involved an intermediate occlusion wafer, extraction of selected teeth, re-osteotomy and plating of the left ramus and pseudocondyle, ORIF of Le Fort I osteotomy, osseous genioplasty with plating, and placement of a final occlusion wafer. Clinical and radiological evaluation on pre and post the second corrective surgery were given on Figures 3 and 4.

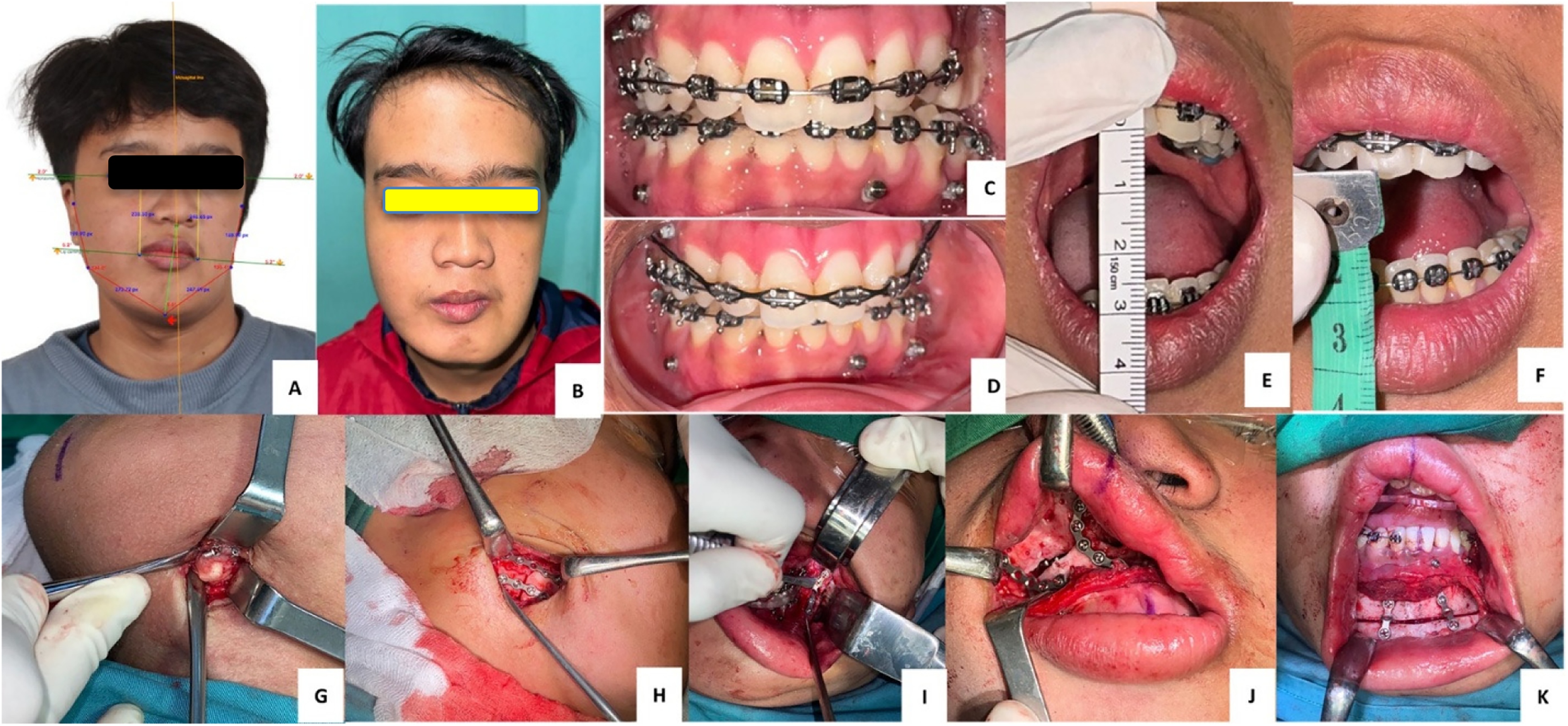
Clinical Features Before and After the First Reconstruction Surgery Due to CCG Overgrowth: (A) Severe Asymmetry at 17 Years Old With Right Jaw Deviation Up to 34.5 Degrees; (B) Better Symmetry and Less Deviation on the Third Month After the First Reconstructive Surgery (CCG Excision); (C) Occlusion Before Surgery; (D) Occlusion After the First Surgery (Before Second Surgery); (E) MIO Before First Reconstruction 32 Mm; (F) MIO After 25 Mm; (G) Le Fort I Osteotomy; (H) and (I) Right VRSO and Coronoidectomy; and (J) and (K) CCG Excision and Mandible Plating.
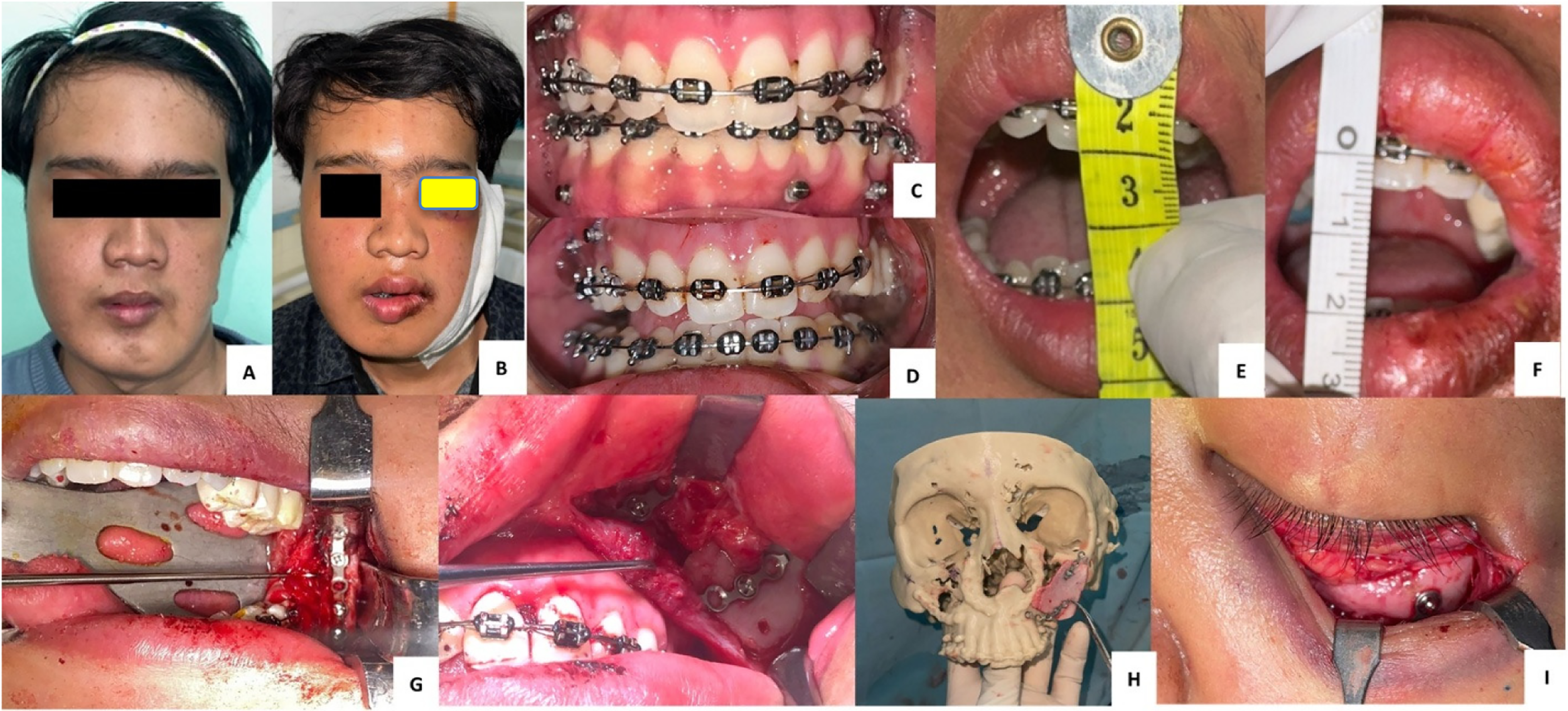
Clinical Features Before and After the Second Reconstruction Surgery: (A) Facial Features Before Surgery; (B) Better Symmetry 3 Months After Second Reconstructive Surgery; (C) Occlusion Before Surgery; (D) Occlusion After Surgery; MIO (E) Before Surgery 25 Mm; (F) After Surgery 15 Mm; (G) Molar (M3) Extraction on Left Mandible; (H) Right VRSO and ORIF; (I) Osteotomy of Ramus and Pseudocondyle, Re-ORIF Due to Plate Fracture; (J) Le Fort Osteotomy and ORIF; and (K) ORIF Genioplasty.
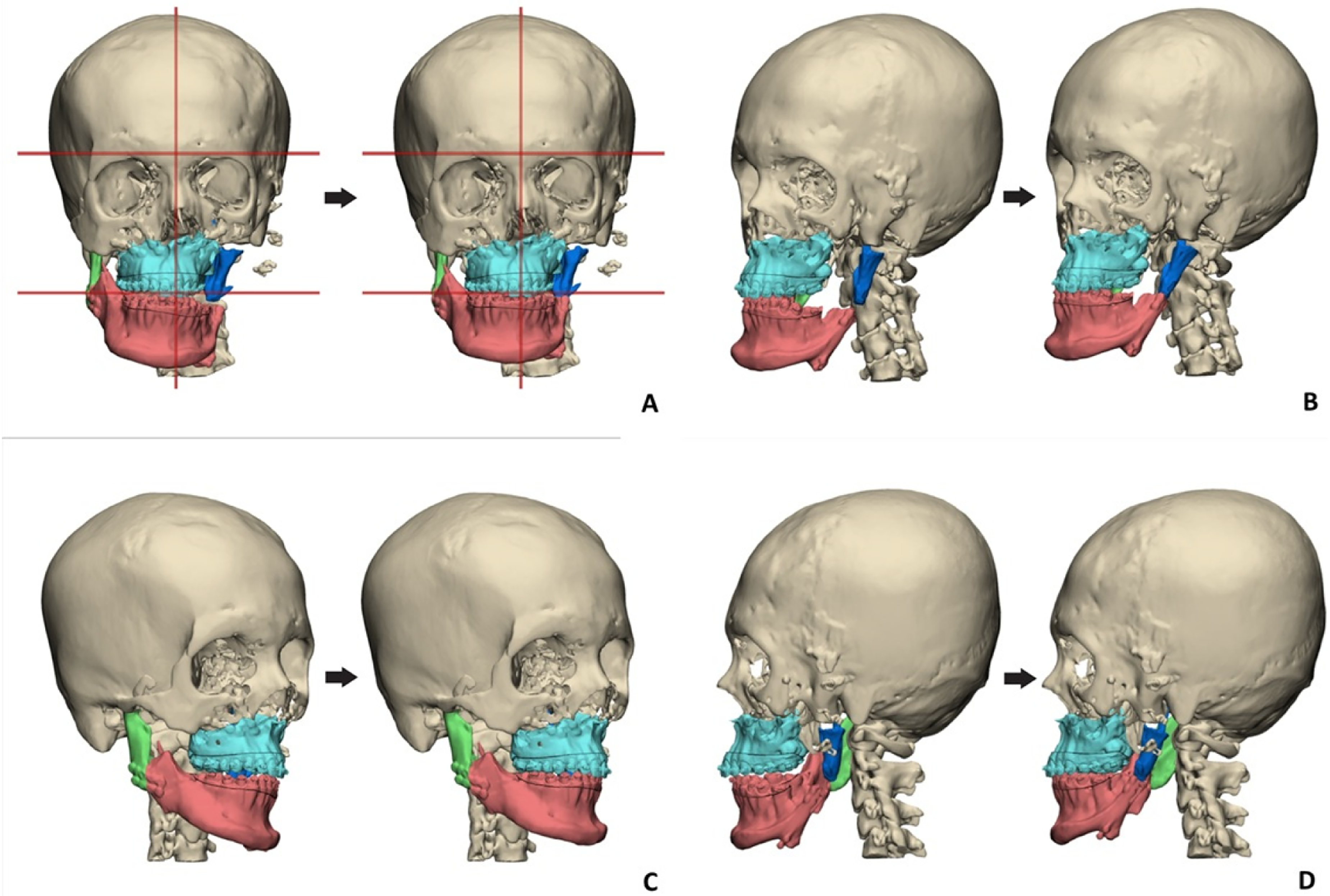
3D Reconstruction Before and After the Second Surgery (Left Pseudocondyle Osteotomy and ORIF) From Different Positions: (A) Front; (B) 45° Right; (C) 45° Left; and (D) Left; Note the Shifting and the Improvement of the Mandible (Red) Position Towards the Left Pseudocondyle (Blue).
Three months after the second corrective surgery, postoperative evaluation showed improved facial symmetry and occlusion, although some degree of malocclusion persisted, particularly maxillary incisor protrusion with limited MIO of 15 mm. A third corrective surgery was conducted at that time to optimize outcomes, including re-ORIF plating of the left mandible, insertion of an onlay iliac bone graft to the left maxilla, ORIF of the left infraorbital rim and lateral buttress, and reconstruction of the left auricle using costal cartilage graft. Following the third corrective surgery, the patient demonstrated significant improvement in facial symmetry and occlusion (Figure 5), highlighting the complexity and multidisciplinary demands of managing extreme CCG overgrowth in craniofacial reconstruction. From the patient's perspective, he reported better quality of life and self-confidence after the third reconstruction, including better speech due to better occlusion.
Clinical Features Before and After the Third Reconstruction Surgery: (A) Facial Features Before Surgery; (B) After Surgery; (C) Occlusion Before Surgery; (D) Occlusion After Surgery; MIO (E) Before Surgery 15 Mm; (F) After Surgery 15 Mm; (G) Re-ORIF of Left Mandible; (H) Iliac Bone Graft of Left Maxilla (In Vivo) and on 3D Model; and (I) ORIF of Left Inferior Orbital Rim.
Discussion
This case exemplifies the unpredictable and progressive nature of CCG overgrowth following mandibular reconstruction in HFM. The patient, initially treated at age 10 with CCG for condylar and zygomaticotemporal reconstruction, developed significant facial deviation within 6 months postoperatively. By age 17, overgrowth of the left mandibular CCG resulted in a 2.5 cm ramal length discrepancy and 34.5° mandibular deviation, underscoring the graft's uncontrolled growth potential. The corrective journey—spanning 3 surgeries—highlights the surgical complexity of managing severe CCG-related deformities and the limitations of conventional reconstruction.
Reconstruction of HFM depends on patient's age, severity of symptoms, and the specialist who initiates the treatment although the comprehensive management requires multidisciplinary team: orthodontists, dentofacial orthopedists, and maxillofacial surgeons. In some cases, it necessitates a broader multidisciplinary team. Treatment aims include enlarging the mandible and associated soft tissues on the affected side, restoring temporomandibular joint (TMJ) function when absent, correcting maxillary deformities, improving dental positioning and occlusion, enhancing smile esthetics, addressing dental canting, and increasing the range of mouth opening when restricted.2,12
As management may differ based on severity, classification is important. The most used classification system is the Pruzansky-Kaban
2
:
Grade I: minimal mandibular hypoplasia; all TMJ components are present with normal morphology but variably hypoplastic. Grade II: the TMJ functions but the condyle and glenoid fossa are malformed (Type IIA allows functional movement despite hypoplasia/malposition, whereas Type IIB shows a hypoplastic, abnormally shaped, and malpositioned ramus causing TMJ dysfunction). Grade III: the ramus, condyle, and TMJ are absent with absent muscular insertions.
In Grades I and IIA, where the TMJ is present and functional, management often focuses on orthodontic correction of occlusal plane abnormalities, sometimes combined with osteotomy or MDO during growth, with the option of delaying definitive orthognathic surgery until skeletal maturity. In Grade IIB, where mandibular ramus deformity causes TMJ dysfunction, MDO combined with orthodontics is frequently used, though additional reconstruction may be necessary. In the most severe Grade III cases, where the ramus, condyle, and TMJ are absent, reconstruction requires grafting (costochondral, iliac bone, or fibula free flap) to restore mandibular continuity and TMJ function, often staged to reduce complications such as ankylosis; adjunctive procedures may address associated auricular, soft tissue, and nerve deficits. 12 Currently, no standardized treatment protocol for HFM has been established.
The CCG remains a preferred autogenous option for TMJ reconstruction, particularly in growing patients, due to its unique biological properties that closely mimic the native mandibular condyle. The primary advantage lies in its physiological basis and superior biocompatibility. 13 As an autograft harvested from the patient's own rib, it eliminates risks of rejection, foreign body reaction, and chronic infection associated with alloplastic materials. Histologically, the graft's structure of hyaline cartilage capping a bony segment is a close analog to the condylar anatomy. This biological similarity allows the living graft to become fully integrated with the native mandible through the process of creeping substitution, where host osteoblasts and blood vessels invade the graft. 14 Once healed, it functions as a vital structure capable of remodeling in response to functional biomechanical forces, adhering to Wolff's Law, which synthetic implants were unable to do in the past. 15
Its inherent growth potential is the most appreciated reason for its usage in pediatrics. The cartilaginous cap of the graft contains active chondrocytes that can continue to proliferate post-transplantation, serving as a replacement growth center for the resected or absent mandibular condyle. This appositional growth is crucial for maintaining vertical ramus height, preventing facial asymmetry, and avoiding the development of a deformity on the affected side during childhood and adolescence.13,16
From a technical standpoint, the CCG offers several practical advantages. The procedure for harvesting the fifth, sixth, or seventh rib is a well-established technique with which maxillofacial surgeons are familiar, and it provides a corticocancellous bone block of adequate length, strength, and a natural curvature that can be easily contoured to approximate the ramus-condyle unit.13,17 Furthermore, it is highly cost-effective compared to custom-fabricated total joint prostheses. For a young patient, a successful graft can last a lifetime, avoiding the multiple revision surgeries often required for prosthetic joints due to wear, loosening, or mechanical failure over decades. 18
However, despite the theoretical growth potential of CCG, it often results in unpredictable growth patterns, including excessive growth in 54% of patients and graft resorption in 25%, with only 38% achieving symmetrical ramus-condyle unit (RCU) 4 years post-surgery. Furthermore, studies on HFM patients treated with CCG reported a 93% rate of secondary surgery for symmetry maintenance due to prevalent undergrowth a decade post-TMJR. Complications like re-ankylosis (9%), fracture, and unpredictable graft overgrowth (13.7%) are also well-documented with CCG. 16 Overgrowth is a well-documented complication, attributed to the persistent growth activity of the costochondral junction, which may respond aberrantly to biomechanical stimuli or hormonal changes during adolescence, and excess height of a cartilaginous cap.19,20 In animal studies, growing animals showed higher graft growth. 21 Active growth instead of adaptive remodeling of the condylar head is hypothesized to cause overgrowth. 22 It is unclear whether a larger or smaller cartilage cap is preferred to prevent overgrowth. 23
Our case aligns with these findings, as the graft elongated to 83 mm at age 16, necessitating excision and osteotomies. The residual asymmetry after the first surgery (8.6° deviation and 8 mm mandibular shift) illustrates the difficulty in achieving complete correction, likely due to soft tissue scarring, muscular forces, and adaptive skeletal changes. Furthermore, the left mandible plate fracture that was found on the second reconstruction surgery was due to the residual growth of the CCG. The timing of reconstruction at the age of 17 was chosen considering the time when epiphyseal plates generally close. However, the residual growth adds further complexity to the unpredictability of CCG. Skeletal maturity is one of the main considerations for the timing of reconstruction to achieve optimal esthetic outcomes. 12
The need for multiple revisions in this patient echoes available literature emphasizing the high complexity of the condition and its possibility of recurrence.22,24 Staged interventions—Le Fort I, VRSO, genioplasty, and iliac bone grafting—were essential to address multidimensional asymmetry. The third surgery, incorporating auricular reconstruction with a second CCG, this graft showed no overgrowth at short-term follow-up, suggesting that technical factors (eg, fixation, positioning) or patient age may influence outcomes.7,19 Nevertheless, the persistence of mild malocclusion post-correction underscores the challenge of restoring ideal function in complex HFM cases.
Although unpredictable, preventing overgrowth has been suggested in literature by keeping the length of the cartilage 2 to 4 mm. 25 Other sources suggested limiting the cartilage height to only 1 to 2 mm. 26 Yadav et al. in their case series of 20 children (age 9-12 years old) that underwent TMJ reconstruction due to ankylosis reported no single CCG overgrowth. It is hypothesized that manipulation of mandible to correct chin deviation intraoperatively causes excessive stress and strain in the muscular functional matrix.
One of the earliest cases of CCG overgrowth in 21-year-old male was reported by Samman in 1995. The patient underwent the first surgery (bilateral subsigmoid ramus osteotomies of the mandible) to correct the asymmetry for traumatic chin injury at 16 years old, yet the asymmetry returned. Clinical and radiographic evaluation revealed left condylar hyperplasia with maxillary canting and class III malocclusion. Surgical management involved a combined approach: Le Fort I osteotomy, right subsigmoid ramus osteotomy, left condylectomy with reconstruction using a right CCG, and genioplasty. Postoperative recovery was uneventful, with early radiographs confirming correction of asymmetry and equal ramus height. However, 3 years later, asymmetry due to CCG overgrowth was observed evidenced by chin deviation, elongation of the left ramus, and increased radionuclide uptake in the grafted condyle. Conservative management was done as the patient remained asymptomatic with preserved occlusion. 27
Another case of CCG overgrowth after TMJ ankylosis reconstruction on a 17-year-old male was corrected through Le Fort 1 osteotomy, condylectomy, and coronoidectomy 28 in a similar way to our case. In other case, genioplasty was performed for better facial symmetry and occlusion 29 as was done in our case. Condylar shaving may also be performed to limit further growth.
This case also raises questions about alternatives to CCG in TMJ reconstruction. While CCG remains a common choice due to its biological compatibility, limited donor site morbidity, and perceived growth potential, alternatives like coronoid process grafts (CPG), revascularized fibula transfer (RFT), and transport distraction osteogenesis (TDO) offer different approaches to restoring functionality and addressing anatomical deficiencies. 16 The CPG has gained attention as an alternative to CCG in TMJ ankylosis and severe retrognathia, offering the benefit of avoiding a secondary donor site while providing greater cortical density and better load-bearing capacity. Clinical outcomes have shown improved masticatory efficiency, bite force, and mandibular mobility, with relapse rates lower than CCG (2.98% vs ∼8%). However, the lack of a growth center limits its long-term utility in children, often requiring secondary procedures to restore mandibular height and length. Complications include graft resorption (36.3%) and temporary nerve paresis (8.7%), while recurrence of ankylosis appears higher in adults treated with CPG compared to CCG or distraction osteogenesis. RFT is well established for segmental mandibular reconstruction, with high graft survival and enhanced precision through CAD/CAM-assisted planning. Despite structural strength, the absence of articular cartilage, donor-site morbidity (ankle stiffness, instability), and lack of growth potential restrict its use in younger patients. Alarmingly, re-ankylosis rates as high as 63% have been reported in immature HFM patients undergoing RFT, compared to lower rates with CCG.
TDO represents a distinct alternative by stimulating new bone and soft tissue through gradual segmental distraction, thereby avoiding the need for graft harvesting. Advantages include controlled directional bone elongation, concurrent tissue expansion, and improved stability, with meta-analyses suggesting lower re-ankylosis rates than CCG. TDO also requires prolonged treatment and high patient compliance. 16 Although TDO offers controlled elongation with lower overgrowth risk, but is unsuitable for condylar replacement in severe HFM with absent ramal remnants, although suitable for type IIb and type III HFM cases. 30 Overall, while CCG remains the only option with intrinsic (though unpredictable) growth potential, CPG, RFT, and TDO expand the reconstructive armamentarium, each balancing benefits of reduced donor morbidity, mechanical strength, or biological regeneration against the challenges of growth limitations, relapse risk, and recurrence of ankylosis.
Alloplastic joints (eg, total TMJ prostheses) provide stability in skeletally mature patients but carry infection and prosthetic failure risks.18,29 Alloplastic joints may prevent further asymmetry, occlusal cant, and cross bite as even in young adults, CCG is still growing. 28
Multidisciplinary collaboration was pivotal in managing such case, integrating orthodontics (occlusal wafers), oral and maxillofacial surgery, and otolaryngology. Long-term follow-up is crucial, as CCG overgrowth can recur until skeletal maturity. 25 This case adds to the limited literature by documenting progressive CCG overgrowth persisting beyond skeletal maturity in HFM, underscoring the necessity for multidisciplinary individualized surgical planning and long-term surveillance. 31
Conclusion
This case highlights the complex and unpredictable nature of CCG overgrowth in the treatment of HFM. Despite initial success, the graft continued to elongate through adolescence, resulting in severe mandibular asymmetry and functional impairment. Surgical correction required a staged, multidisciplinary strategy involving osteotomies, graft excision, genioplasty, and soft tissue reconstruction. While substantial improvement was achieved, mild residual deformities remained, underscoring the limitations of current techniques. This case reinforces the importance of long-term surveillance following CCG placement in pediatric patients and supports ongoing investigation into alternative reconstructive methods that offer greater predictability and stability.
Footnotes
Acknowledgments
The authors would like to thank all authors for their expertise and assistance throughout all aspects of the study.
Ethical Considerations
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed as a service evaluation in our hospital, and ethical approval was not required.
Informed Consent
Informed consent was obtained prior to performing the procedures, including permission for publication of all photographs and images included herein.
Author Contributions
LZ conceptualized the case, drafted the manuscript, and finalized the report. CAW assisted in patient data collection and performed the initial literature review. LZ, MRH, and AA conducted the final analysis, involved in planning, and were responsible for the overall project supervision. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.