
Abstract
Cleft lip and/or palate (CL/P) represent one of the most common congenital malformations in the oral and maxillofacial region, and various factors are associated with the development of CL/P and its subtypes. Despite an increased concordance rate in monozygotic twins, mirror-image cleft formations represent a very rare phenotype, for which only very few case reports exist in the literature. The present case report describes a female pair of monozygotic twins from Germany who were born with mirror-image bilateral complete and incomplete cleft lip and alveolus.
Introduction
With a prevalence of approximately 1 in 700 births, 1 cleft lip and/or palate (CL/P) constitute one of the most common congenital anomalies in the craniofacial region. Different forms of complete and incomplete clefts are distinguished, with left-sided clefts being the most frequent manifestation. 2 Bilateral cleft lip (CL) accounts for less than 10% of all CL and represents the rarest form of this congenital anomaly. 2
In general, CL/P occurs either as part of genetic syndromes or as an isolated malformation. The etiology of CL/P is multifactorial, and various genetic and exogenous factors are discussed as causes of orofacial clefts. In their meta-analysis, Acs et al 3 identified maternal underweight or overweight, essential hypertension, and type I diabetes mellitus during early pregnancy as exogeneous risk factors. In addition, maternal nicotine consumption has been shown to be associated with the development of CL/P. 3 Further risk factors include maternal opioid abuse, 4 advanced maternal age,5,6 folic acid deficiency,6,7 chlamydia infection, 8 and maternal stress. 6
Genetic factors contributing to nonsyndromic cleft formation include mutations and aberrations in genes encoding for proteins and signaling pathways involved in facial development, such as the interferon regulatory factor 6 (IRF6),9,10 which is also associated with Van der Woude syndrome. 11 In a meta-analysis by Ludwig et al 10 , an association with nonsyndromic CL/P was confirmed for a total of 6 gene loci, including IRF6.
The vulnerable phases of embryogenesis for facial development occur between the 6th and 12th week of gestation (WG). During the 6th WG, fusion of the maxillary process with the medial and lateral nasal processes takes place, resulting in the formation of the upper lip. 12 Incomplete or absent fusion results in clefts of the upper lip or upper lip and alveolar ridge (CL ± A). From this, it can be concluded that, in the case of an exogenous cause of cleft formation in the twins presented here, the harmful influence must have occurred during this period of development. During further embryonic development, approximation and fusion of the palatal shelves occur in the 8th WG with the formation of the median palatal suture. 13 By the 12th WG, formation of the hard and soft palate is completed. 13
Within routine prenatal care, the current German evidence-based S3-guideline on cleft lip and palate recommends transabdominal ultrasound screening in the second or third trimester for pregnancies at risk (positive family history or suspicious findings on routine prenatal ultrasound) to detect CL/P. 14 In this context, Maarse et al 15 reported detection rates of 60% to 100% using 3-dimensional ultrasound in high-risk pregnancies. When the a priori risk for congenital CL/P was low, detection rates decreased to 9% to 50%. 15 A limiting factor was that only a 2-dimensional ultrasound was performed in the low-risk cohort. At this point, it is worth mentioning that in prenatal ultrasound, a cleft lip with or without cleft palate can be reliably detected, whereas an isolated cleft palate typically remains undetectable.
If CL/P and additional malformations are identified on prenatal ultrasound, prenatal genetic counseling and subsequent genetic testing are recommended. 14 Genetic counseling is also advised in cases of isolated cleft formation with a positive family history —prenatally and/or postnatally.
The overall risk of CL/P in twins is not significantly higher than in singletons; however, the concordance rate in monozygotic twins (50%) is considerably higher than in dizygotic twins (8%). 16
Monozygotic twins account for approximately one-third of all twin pregnancies 17 and arise from the development of 2 embryos from a single zygote. Monochorionic diamniotic twin pregnancies develop between day 4 and 7 post conceptionem. 18 The proportion of monozygotic twins exhibiting mirror-image characteristics is estimated to be approximately 10% to 15%. 18
Only a few case reports of mirror-image clefts in monozygotic twins have been published in the literature. Therefore, reliable data on prevalence or risk are lacking. Beyond CL/P, mirror-image anomalies in monozygotic twins have been described in heterotaxy syndrome (situs inversus), congenital heart defects, 19 and syndromic disorders such as first and second branchial arch syndromes, 20 which in rare cases may also be associated with CL/P.
Case Report
The mother was 22 years old at the time of conception, and the documented and reported course of the first trimester of pregnancy was unremarkable. This was the mother's first pregnancy. Maternal exposure to teratogenic agents such as alcohol, nicotine, or ionizing radiation during pregnancy was excluded based on medical history. Maternal serum screening demonstrated sufficient immunity and no evidence of infection with teratogenic pathogens, such as chlamydia. At the time of testing, there was no evidence of previous infection or immunity to toxoplasmosis.
At 18 + 1 WG, the routine ultrasound first raised suspicion of a facial malformation. Family history revealed a unilateral CLP in the paternal uncle. Therefore, the parents and the twins met the criteria for referral to genetic counseling. Further medical history obtained during genetic evaluation was unremarkable. Prenatal rapid testing of amniotic fluid cells via fluorescence in situ hybridization has a sensitivity of 97.5% for the detection of numerical chromosomal aberrations 21 and revealed no evidence of trisomy 13, 18, or 21, triploidy, or monosomy X. Chromosomal analysis showed a normal female karyotype (46, XX) in both infants and no evidence of Di-George syndrome. A suspected pseudomosaicism was noted in one infant, which was most likely attributable to a culture artifact. Further investigations of amniotic cells using whole-exome sequencing and chromosomal microarray analysis were declined by the parents. Consequently, limited genetic testing could not identify a genetic cause for the orofacial cleft in the monochorionic diamniotic twins.
The remainder of the pregnancy was largely uneventful; however, intrauterine growth restriction was detected in twin A during the course of gestation. Subsequently, maternal preeclampsia was diagnosed and treated pharmacologically with nifedipine and alpha-methyldopa. Additionally, magnesium was administered for seizure prophylaxis.
Due to maternal preeclampsia, the twins were delivered by cesarean section at 32 + 3 WG. As preterm infants, the two girls had birth weights of 1170 g (2nd percentile, twin A) and 1580 g (22nd percentile, twin B) (percentiles according to Voigt et al 22 ). Additional somatic data at birth are summarized in Table 1. Both children required postnatal intubation due to episodes of decreased peripheral oxygen saturation and were treated and monitored in the neonatal intensive care unit for one day before being transferred to the regular ward in incubators. A hearing screening performed prior to discharge yielded normal results in both infants.
Somatic Characteristics of the Preterm Twins at Birth with Percentiles Calculated According to Voigt et al. 18 .
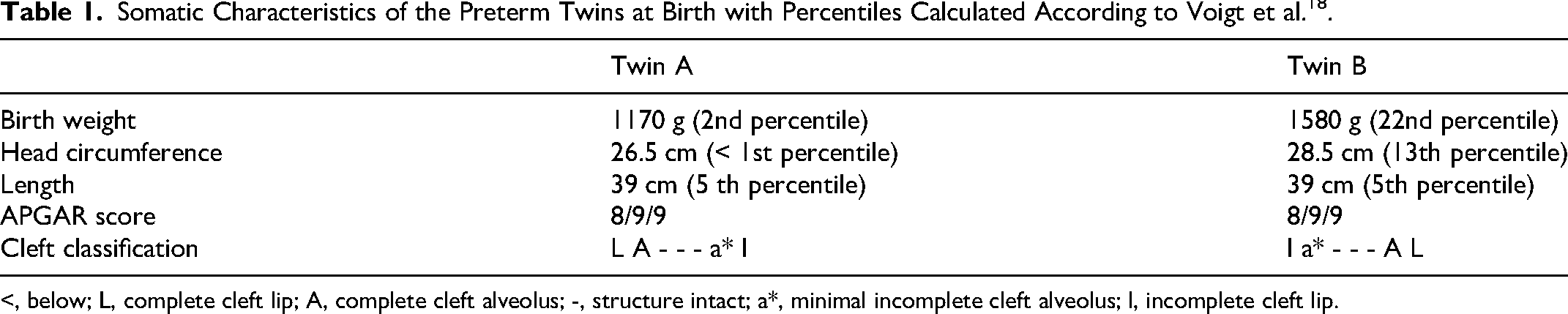
<, below; L, complete cleft lip; A, complete cleft alveolus; -, structure intact; a*, minimal incomplete cleft alveolus; l, incomplete cleft lip.
The twins first presented to our clinic at 2 months of age. Both infants were in good general condition with reduced nutritional status (Figure 1). According to the mother, breastfeeding was unproblematic, and by the scheduled date of surgery, the body weights had increased to 5300 g (8th percentile, twin A) and 6300 g (42nd percentile, twin B), respectively.
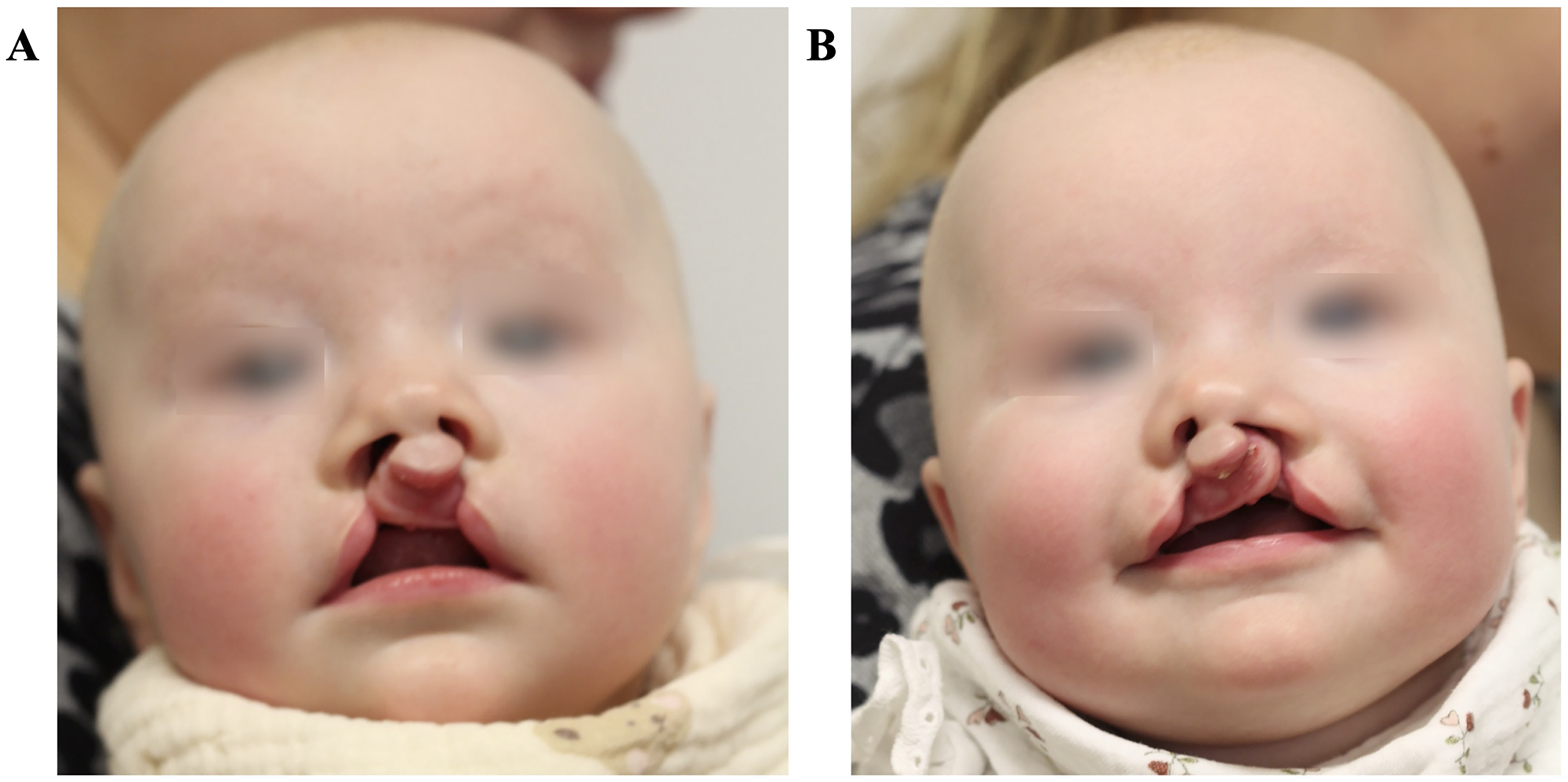
Images of twin A (
At 6 months of age, lip repair according to the Veau-Axhausen technique was performed under general anesthesia (Figure 2). Both girls underwent surgery on the same day. The postoperative course was uneventful. No postoperative hemorrhage occurred, and only minimal swelling was noted in the operative site. Under adequate analgesia, oral feeding with a bottle was well tolerated in both girls. At follow-up 7 weeks and 3 months after surgery, both children showed well-healed wounds without any major signs of irritation (Figure 3). Only twin A exhibited slightly erythematous scars. However, the erythema is expected to diminish during the subsequent course of healing. Following reconstruction of the orbicularis oris muscle, functional activity (eg, drinking, smiling, crying) will lead to a harmonization of lip morphology. Furthermore, an asymmetric left-sided nasal opening was observed in twin B. This asymmetry may be compensated for by continued growth or corrected at a later stage by means of a secondary surgery. In conclusion, both girls demonstrated an aesthetically satisfactory outcome at the given time point.
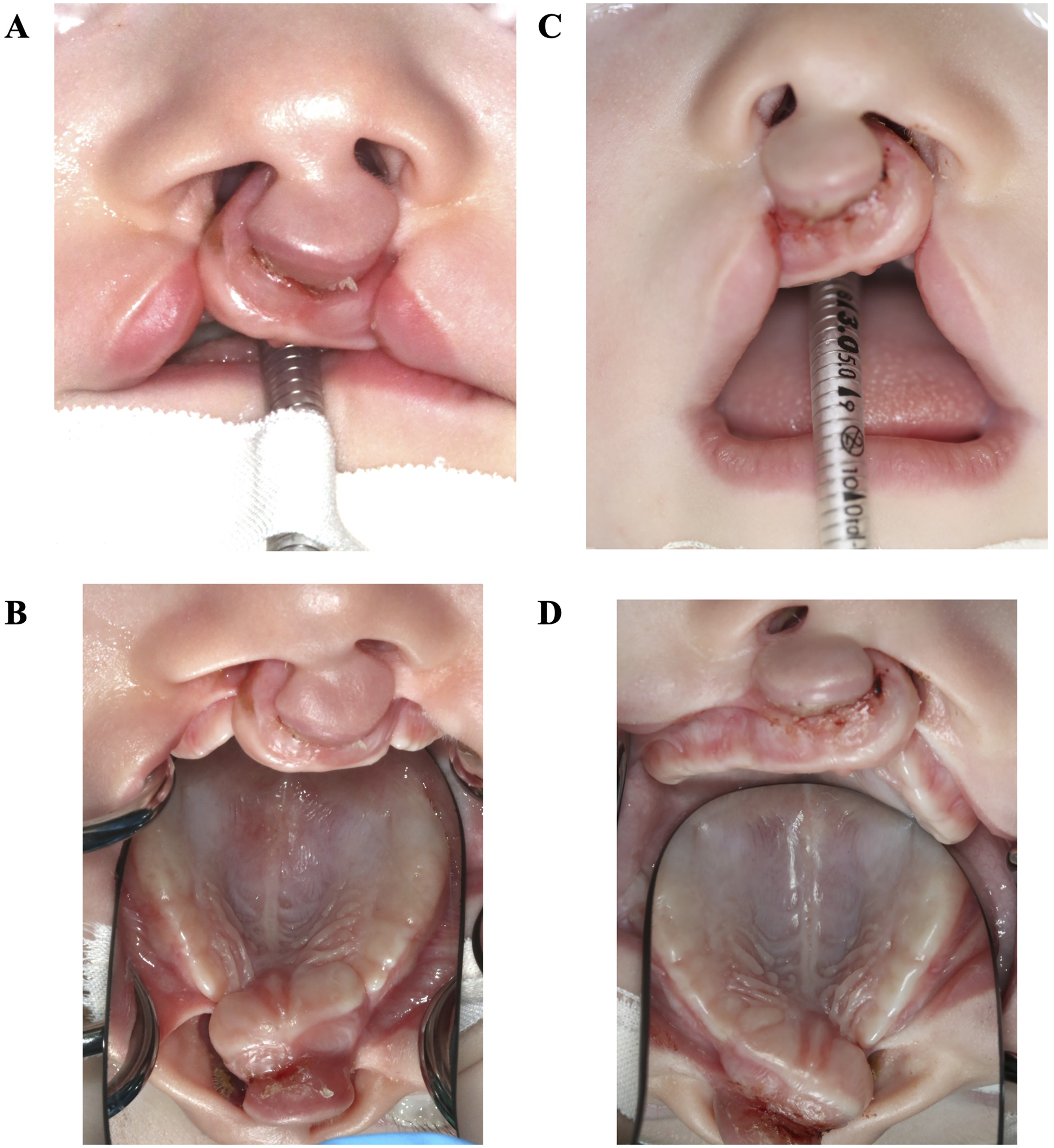
Intraoperative images of twin A (
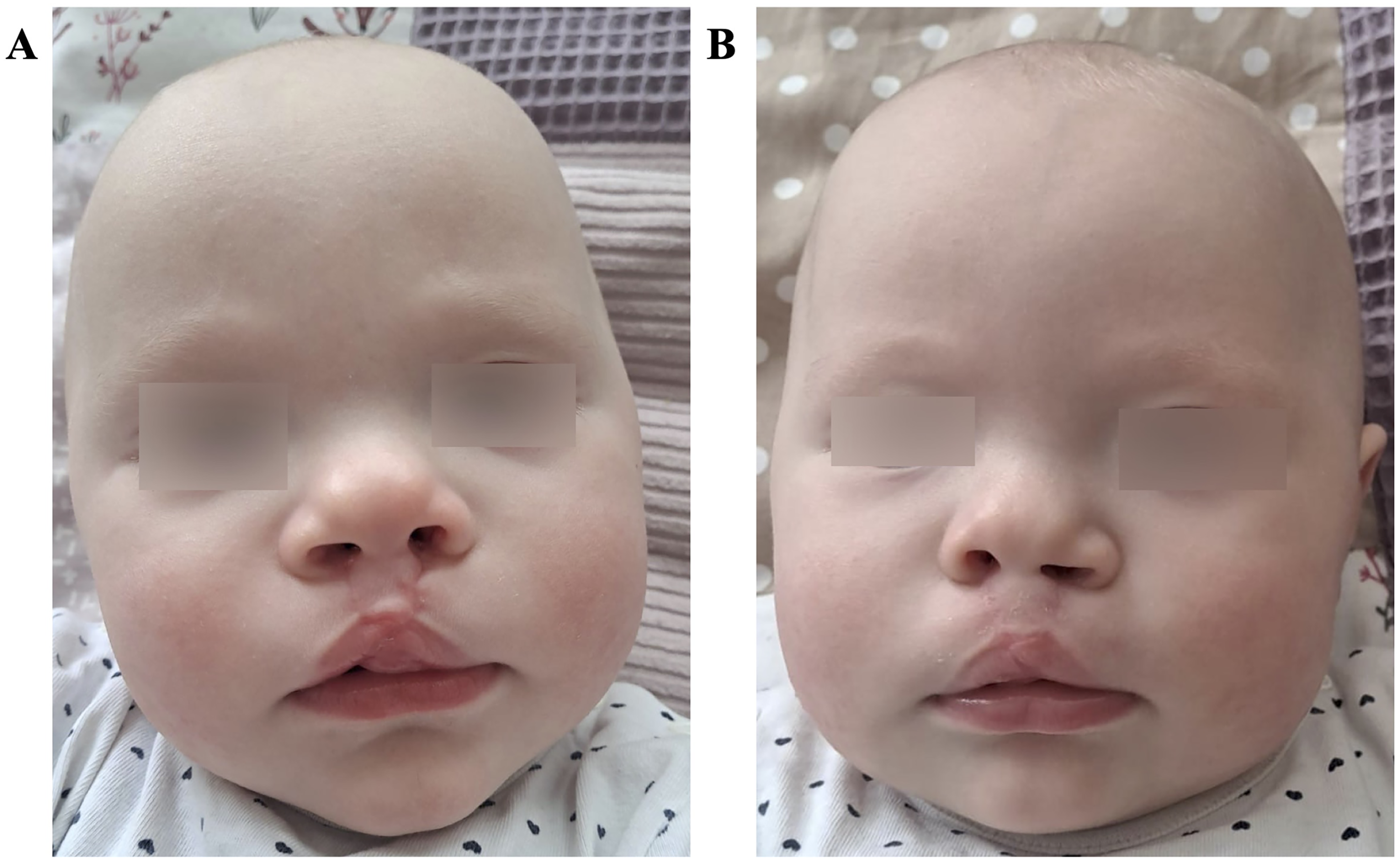
Images of twin A (
The children will continue to attend annual follow-up visits in our clinic in order to plan necessary secondary procedures at an early stage. Alveolar bone grafting is planned between 9 and 11 years of age.
Discussion
The present case represents an extremely rare manifestation of mirror-image cleft lip and alveolus (CLA) in monozygotic twins, although CL/P in twins in general has been investigated by other research groups. Mansilla et al 23 investigated 21 twin pairs with nonsyndromic CL/P, including 13 discordant monozygotic twin pairs, using genome sequencing to screen for mutations in 18 genes, exons, and regulatory genomic regions. Despite the discordant phenotypes in 17 of the 21 twin pairs, no seminal genomic differences were detected in the cohort. Only 2 missense mutations were identified in one discordant monozygotic twin pair. Based on these findings, the authors suggested that additional factors such as gene penetrance, X-chromosome inactivation in female idividuals, and other genetic mechanisms, including imprinting, may play a role in cleft formation. 23 Furthermore, anatomical, vascular (twin-to-twin transfusion syndrome), and positional factors were proposed as possible contributing causes. 23 In the present case, prenatally no evidence of twin-to-twin transfusion syndrome was observed. The gene loci identified in the meta-analysis by Ludwig et al 10 as being associated with an increased risk of CL/P could have been examined by whole-exome sequencing, potentially providing further insight into possible genetic aberrations or etiological factors. In this context, Yan et al reported an improvement in prenatal CL/P diagnostics using whole-exome sequencing. However, clinically significant genetic variants were detected in only a relatively small proportion of 11.2% of the individuals studied. 24 Taken together with the data from Mansilla et al, 23 it can be assumed that in the monozygotic twin pair described in this case report, no relevant differences in genomic sequence were present that could account for the mirror-image manifestation of the orofacial clefts.
Independent of CL/P, other studies have postulated that the occurrence of mirror-image anomalies in monozygotic twins may be related to delayed development in early pregnancy, particularly in female embryos. 18 It has been hypothesized that prior to X-chromosome inactivation, female embryos exhibit slower growth compared with male embryos, which may result in critical developmental time points or thresholds being reached later or even too late. 18 Whether this hypothetical developmental delay influences orofacial cleft formation at a much later stage of embryogenesis remains to be clarified by further scientific investigation.
A suspected pseudomosaicism was noted in one twin. It cannot be excluded with absolute certainty that true genetic mosaicism was present. This hypothetical scenario would be consistent with other communications, suggesting that mosaicism may be a mechanism underlying the development of monozygotic twins,18,25 as the original blastocyst cells may recognize mosaic cells as foreign, thereby triggering division of the cell mass and the development of two embryos. With regard to whether a potential mosaicism influenced the mirror-image cleft formation, only speculative assumptions can be made.
Overall, the etiology of mirror-image malformations in monozygotic twins requires further investigation. Based on current scientific knowledge, the findings discussed above, together with the concordance rate of 50% in monozygotic twins, 16 suggest a multifactorial pathogenesis for the mirror-image cleft formation described here. Potential contributing factors include genetic aberrations, possible cellular damage during blastocyst division, and environmental influences such as differences in embryonic position within the uterus during exposure to environmental factors or variations in vascularization during the susceptible phase of facial development.
Conclusion
Mirror-image CLA in monozygotic twins represents a rare subset of CL/P. Nevertheless, they merit significant scientific interest, as potential genotypic and phenotypic differences in monozygotic twins are of great value for further research into gene–environment interactions, the molecular mechanisms of craniofacial development, and the identification of genetic—and potentially predisposing—factors. In particular, the identification of risk genes through human genetic testing can contribute to more sensitive prenatal (genetic) diagnostics for CL/P, since only clefts involving the upper lip—rather than isolated clefts of the palate—can be reliably detected on prenatal ultrasound.
Since monozygotic twins share the same genes, mirror-image cleft formations in such twins might allow for further research into the mechanisms of cleft development beyond genetic alterations.
From the perspective of expectant parents, early diagnosis with sufficient time before delivery is desirable, as it allows for careful consideration of the anticipated malformation in their child. This interval also enables comprehensive counseling and planning of postnatal management prior to the estimated date of birth.
Regardless, the ethically grounded right not to know must be respected and protected. Therefore, any further diagnostic procedures during pregnancy—when there is a justified suspicion of an orofacial cleft—should only be initiated after thorough counseling and joint decision-making between the treating physicians and the parents.
Footnotes
Acknowledgments
We would like to thank the parents for their trust, for providing the data, and for granting permission to publish the photographs presented here. All authors have read and agreed to the published version of the manuscript.
Informed Consent
The parents of the patients provided informed consent for the use and publication of the patients’ data and photographs included in this publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Further data cannot be shared publicly because of its sensitive nature.