
Abstract
Objective
This study describes behavior and quality of life (QoL) in youth with cleft lip and palate (CLP) during treatment for class III malocclusion.
Design
Prospective cohorts followed at baseline, maximal correction, treatment completion with debanding, and 1-year follow-up.
Participants
Youth with CLP (n = 64-114) undergoing protraction (58%) or orthognathic surgery (42%) and their caregivers (n = 47-97).
Main Outcome Measure(s)
Child/Adult Behavior Checklists (C/ABCL) and Youth Quality of Life—Facial Differences (YQOL-FD).
Results
C/ABCL Externalizing, Internalizing, and Total Problems and YQOL-FD Negative Consequences, Negative Self-Image, and Stigma were significantly lower than norms across time points (Cohen's d = −0.22 to −0.93). Highest proportions above clinical cutoffs were for Internalizing (10%-17%) and Negative Self-Image (13%-15%). There were a few changes over time, and no differences based on treatment outcome.
Conclusions
Youth with CLP had overall positive adjustment during treatment for class III malocclusion. Supports may target internalizing and self-image concerns.
Introduction
In the United States (US), cleft lip and palate (CLP) occurs in about 1 in 1560 live births. 1 Interdisciplinary cleft care begins in infancy, and individuals with CLP can have an average of 9 surgeries by adulthood.2,3 Class III malocclusion is significantly more frequent among individuals with CLP compared to general population rates of 4% to 11%, which vary based on ethnicity.4,5 Both maxillary protraction and orthognathic surgery are common interventions for class III malocclusion.6–9 Reports of psychosocial adjustment based on orthodontic treatment for class III malocclusion have been mixed, with both no changes in self-esteem, quality of life (QoL), or appraisals of appearance and social interactions, as well as reports of increased QoL.10–12 After stressors during the immediate postoperative period decrease, improvements in confidence, self-esteem, perceived facial appearance, and social functioning have been reported in reviews of the treatment of class III malocclusion with orthognathic surgery.13,14
Within the context of overall similar adjustment as their peers, individuals with CLP can have increased risk for some concerns, such as social stressors and anxiety, and class III malocclusion has been associated with lower oral-health related QoL.15–21 Over the past 20 years, caregiver reports using the same behavior checklist selected for this study have shifted from higher internalizing and externalizing problems to show similar or fewer concerns than peers more recently.22–26 A measure of self-report of QoL related to having a facial difference for youth with a cleft was also included in this study.27–30 In US studies with this measure, low coping and positive consequences of having a cleft were reported with about a fifth of youth experiencing teasing and a third reporting staring.27,28 In a Japanese sample with the same measure, about a fifth of participants had high scores for stigma with experiences of staring and teasing, while 15% had high negative self-image and negative consequences related to having a cleft.29,30
The purpose of this study was to describe caregiver-reported behavioral functioning and self-reported QoL related to having a facial difference in individuals with CLP throughout treatment for class III malocclusion compared to measure norm groups, over time, by treatment group, and by treatment outcome. A greater understanding of behavioral functioning and QoL during a common treatment period in cleft care can help inform screening and interventions.
Method
This study was approved by the Institutional Review Boards at Children's Hospital Los Angeles and Seattle Children's Hospital (ClinicalTrials.gov NCT02789787). Eligibility criteria included patients with non-syndromic unilateral or bilateral CLP with class III malocclusion. Exclusion criteria were: maxillary mandibular cant, mandibular asymmetry, mandibular prognathism requiring bimaxillary surgery, non-grafted alveolar cleft, or history of therapeutic radiation treatment to the maxilla or mandible. Study participation took place from April 2015 through May 2021, with treatment based on patient choice and age for maxillary protraction (ages 11-14) or orthognathic surgery (ages 16-21). The protraction group completed treatment for 18 to 24 months with a modified Alternative Rapid Maxillary Expansion and Constriction (Alt-RAMEC) protocol with a Hyrax expander, reverse-pull facemask, and class III elastics. The surgery group underwent orthodontic treatment and LeFort I single-jaw orthognathic surgery by board-certified maxillofacial surgeons who are Fellows of the American College of Surgeons with over 15 years of practice in orthognathic surgery. The surgical complication rate was 5%, including periodontal bone loss at the cleft site during segmentation. Study visits were at baseline (Time 1), maximal correction (Time 2), treatment completion (Time 3), and 1-year follow-up (Time 4). Study participation lasted around 3 years with Time 2 taking place 2-7 months after Time 1, Time 3 was about 12-18 months after Time 2, and Time 4 was about 12 months after Time 3.
Measures
At each time point, the Great Ormond Street London and Oslo (GOSLON) yardstick described occlusion based on anteroposterior, vertical, and transverse positioning. 31 GOSLON ratings were made by 2 raters with a third rater to achieve consensus when needed. A successful outcome was determined by baseline GOSLON ratings of 3, 4, or 5 improving to post-intervention ratings of 1 to 2, and unsuccessful outcomes were defined as GOSLON ratings that remained a 3 or higher. Additional medical study variables included cleft type and the number of prior cleft-related surgeries. Sociodemographic variables included sex, age, ethnicity, type of insurance (public or private), caregiver language, and Hollingshead socioeconomic status (SES) based on caregivers’ marital status, education, and occupation. 32
At each time point, participants’ caregivers completed the Child Behavior Checklist (CBCL; age <18 years) or Adult Behavior Checklist (ABCL; age >18 years) in English or Spanish with a research assistant available if needed.33,34 The checklists had 113-123 items with 3 composite scales of Externalizing, Internalizing, and Total Problems with national age-based measure norms using T-scores (M = 50 ± 10) and a clinical cutoff of ≥ 60. The Child/Adult Behavior Checklists (C/ABCL) also have Syndrome and DSM-Oriented scales with a fixed minimum score of 50 interpreted by the borderline clinical cutoff of ≥ 65. For this study, the scales reported for the C/ABCL were: Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Thought Problems, Attention Problems, Rule Breaking Behavior, Depressive Problems, Anxiety Problems, and ADHD Problems. The reported scales only on the CBCL were: Social Problems, Oppositional Defiant, and Conduct Problems. The scales only on the ABCL that were reported included: Intrusive, Avoidant Personality, and Antisocial Personality.
At each time point, participants completed the Youth Quality of Life—Facial Differences (YQOL-FD) privately with a research assistant available if needed.35,36 The YQOL-FD has 30 Perceptual items about how participants felt daily about the impact of their facial difference, rated from 0 (“not at all”) to 10 (“a great deal” or “completely”), such as feeling frustrated with or judged by their appearance or feeling their facial difference has helped them accept others for who they are and become stronger. Items were converted to a 0 to 100 scale, and means were calculated for the 5 Perceptual Scales: Positive Consequences (5 items), Coping (4 items), Negative Consequences (6 items), Negative Self-Image (5 items), and Stigma (10 items). Higher QoL is reflected in higher Positive Consequences and Coping scores, and conversely with lower scores on the Negative Consequences, Negative Self-Image, and Stigma scales. Self-identified “Mild Severity” of facial difference means from the YQOL-FD measure group norms were used for sample comparisons. The means for those in the norm sample who self-identified as “Marked Severe” in their facial difference were used for clinical cutoff scores for the negative Perceptual scales: Negative Consequences ≥ 38, Negative Self-image ≥ 54, and Stigma ≥ 46. As there were no differences in the norm sample based on severity for Positive Consequences or Coping scales, clinical cutoff scores were not calculated for the positive scales. The original internal reliability ranged from 0.71 to 0.90. In this sample, Cronbach's alphas were acceptable: Positive Consequences α = 0.74, Coping α = 0.76, Negative Consequences α = 0.73, Negative Self-Image α = 0.79, and Stigma α = 0.91.
Analyses
Participant characteristics were summarized with descriptive statistics and were compared across time points with analysis of variance (ANOVA) and chi-square to identify any differences in the sample characteristics over time. The measure scales’ means, standard deviations, and cutoffs were summarized and compared to norm means with t-tests at each time point with Cohen's d for effect size. ANOVAs were run for the scales at treatment completion (Time 3) and at a year post-treatment (Time 4), comparing protraction to surgery and successful to unsuccessful treatment outcome with eta2 for effect size. Paired t-tests were used to compare measure means across consecutive time points as well as from baseline (Time 1) to a year post-treatment (Time 4). Pearson correlations described associations between scales at each time point. Based on Cohen, effect size using Cohen's d was interpreted as small (0.20), medium (0.50), or large (0.80); effect size using eta2 was interpreted as small (0.01), medium (0.06), or large (0.14); and Pearson correlations were interpreted as small (0.10), medium (0.30), or large (0.50). 37 Significance was set as 2-tailed or 2-sided P < .05. Analyses were completed in IBM SPSS Statistics (Version 28). 38
Results
Participant Characteristics
There were 114 participants who completed baseline measures at Time 1, 96 participants at maximal correction at Time 2, and 95 at treatment completion at Time 3 (attrition rate of 17%). Of participants who completed treatment, 68% (n = 64) then completed measures a year later at Time 4. Other than expected increase in age over time, the only difference in sample characteristics across time points was a lower proportion of participants with bilateral CLP at Time 3, Χ2 = 6.19, P = .01. There were fewer caregivers than participants who completed measures at each time point: Time 1 (n = 97), Time 2 (n = 79), Time 3 (n = 82), and Time 4 (n = 47). Of those participants who completed treatment, 58% underwent protraction, and 42% had orthognathic surgery. Baseline GOSLON ratings were 3 (11.9%), 4 (42.4%), or 5 (29.7%) with no significant difference between treatment groups, Χ2 = 1.88, P = .391. Post-treatment GOSLON ratings were 2 (62.1%), 3 (7.4%), 4 (11.6%), or 5 (13.7%). The total sample success rate was 69.5% with a significantly higher success for surgery (92%) compared to protraction (51%), Χ2 = 17.27, P < .001.
As seen in Table 1, participants had a mean age of 14.8 ± 2.9 at baseline. Most participants were male (57%) and identified as Latino (67.5%), Asian American (15.8%), or White/European American (13.2%). The majority were in the lowest 2 Hollingshead SES groups (57%) and had public insurance (62.3%). Household size ranged from 2 to 15 with an average of 4.7 ± 1.8 people. Participants were born with left (52.6%) or right (23.7%) unilateral CLP or bilateral CLP (21.9%). They had completed an average of 5.1 ± 2.0 prior cleft-related surgeries (range 2-11).
Participant Characteristics (N = 114).
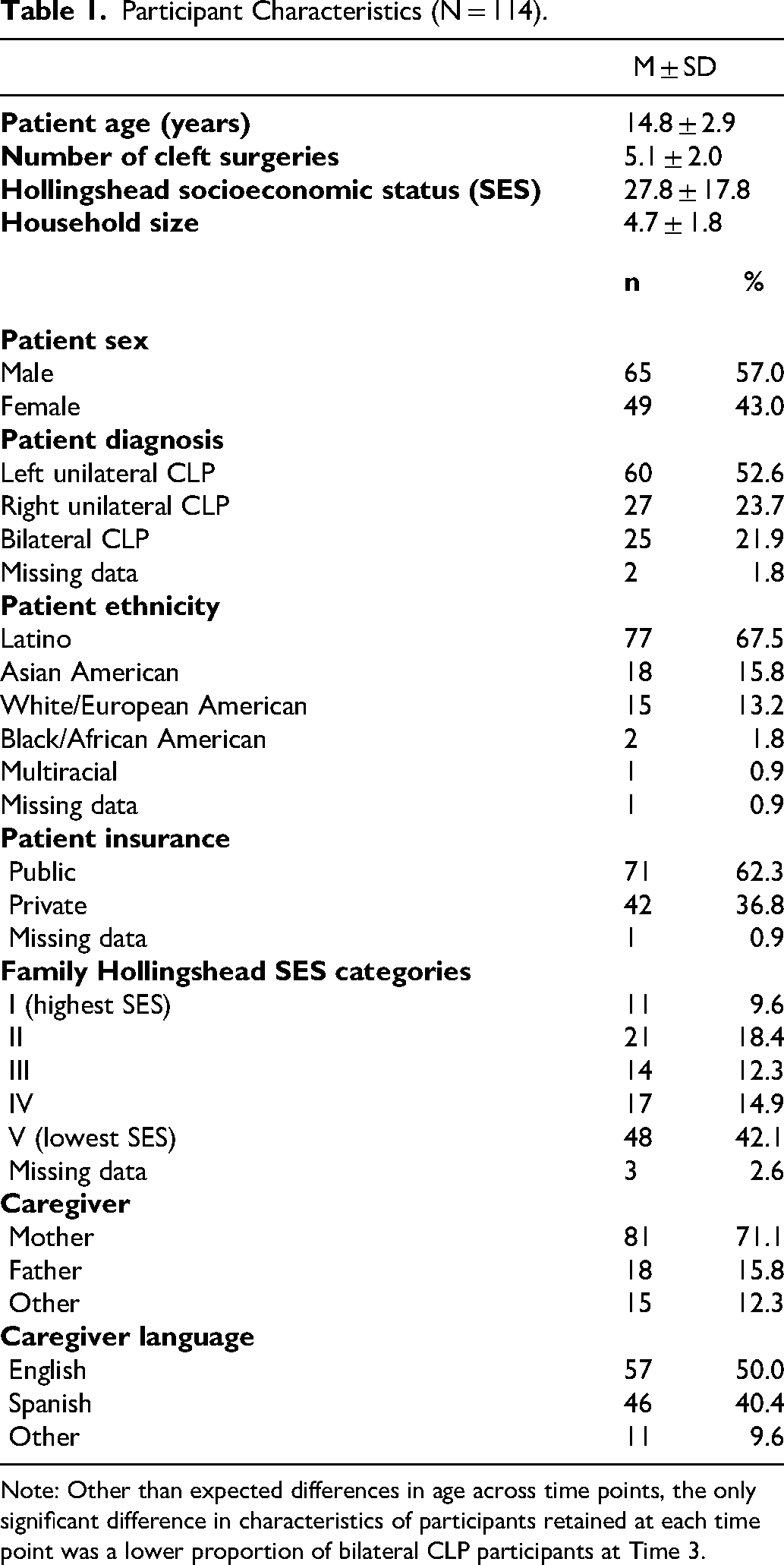
Note: Other than expected differences in age across time points, the only significant difference in characteristics of participants retained at each time point was a lower proportion of bilateral CLP participants at Time 3.
When comparing baseline functioning on both measures between the 2 treatment groups, there were no differences by parent report and only one difference by self-report for higher Positive Consequences mean scores for the older surgery group (66.1 ± 22.1) than the younger protraction group (54.0 ± 23.3), F = 7.96, P = .006, eta2 = 0.06.
Norm Comparisons and Cutoff Rates
Across all time points, caregivers reported significantly lower Internalizing, Externalizing, and Total Problem scores than national norms with small to large effect sizes (d = −0.22 to −0.93), as shown in Table 2 and Supplemental Figure 1. The proportion of participants above the clinical cutoff was lowest for Externalizing (4%-7%), with relatively more participants above the cutoff for Internalizing (10%-17%). Means and clinical cutoffs for Syndrome and DSM Oriented scales are shown in Supplemental Table 1 with a similar pattern of means close to the minimum score of 50 and a few participants above the borderline clinical cutoff (0%-13%).
Caregiver-Reported and Self-Reported Scales Compared to Measure Norms and Cutoff Scores.
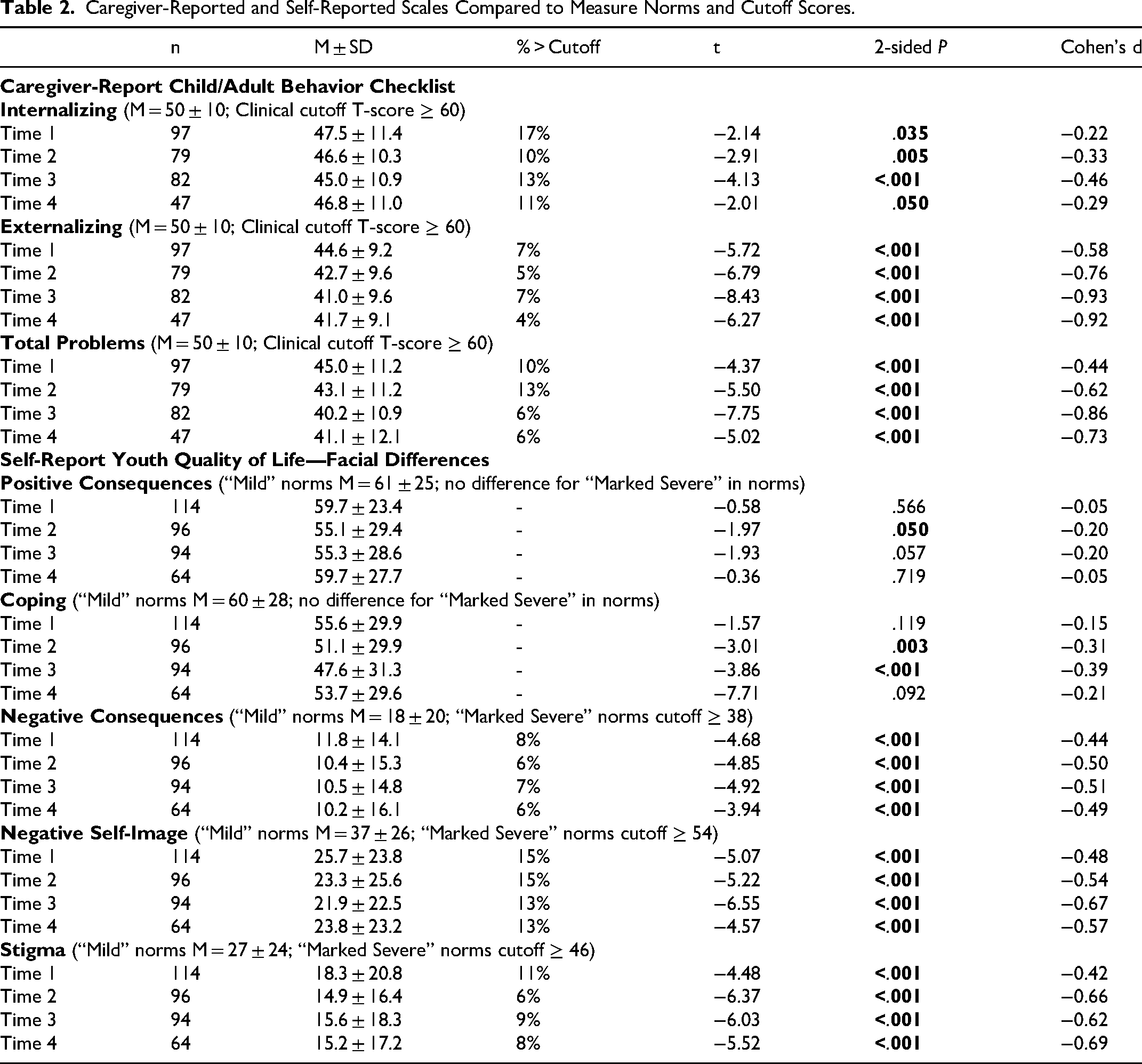
Self-reported functioning (Table 2 and Supplemental Figure 1) had significantly lower negative Perceptual scales across time points than the self-identified “mild” measure norm group with medium effect sizes (d = −0.42 to −0.69), reflecting fewer concerns in these areas. The proportion of participants above the self-identified “severe” measure norm group was highest for Negative Self-Image (13%-15%) with fewer participants reporting concerns for Negative Consequences (6%-8%) and Stigma (6%-11%). There was a significant difference at Time 2 for Positive Consequences from the “mild” norm group, with lower scores and a small effect size (d = −0.20). Coping was significantly lower than the “mild” norm at Time 2 and Time 3 with small effect sizes (d = −0.31 and −0.39, respectively).
Changes Over Time
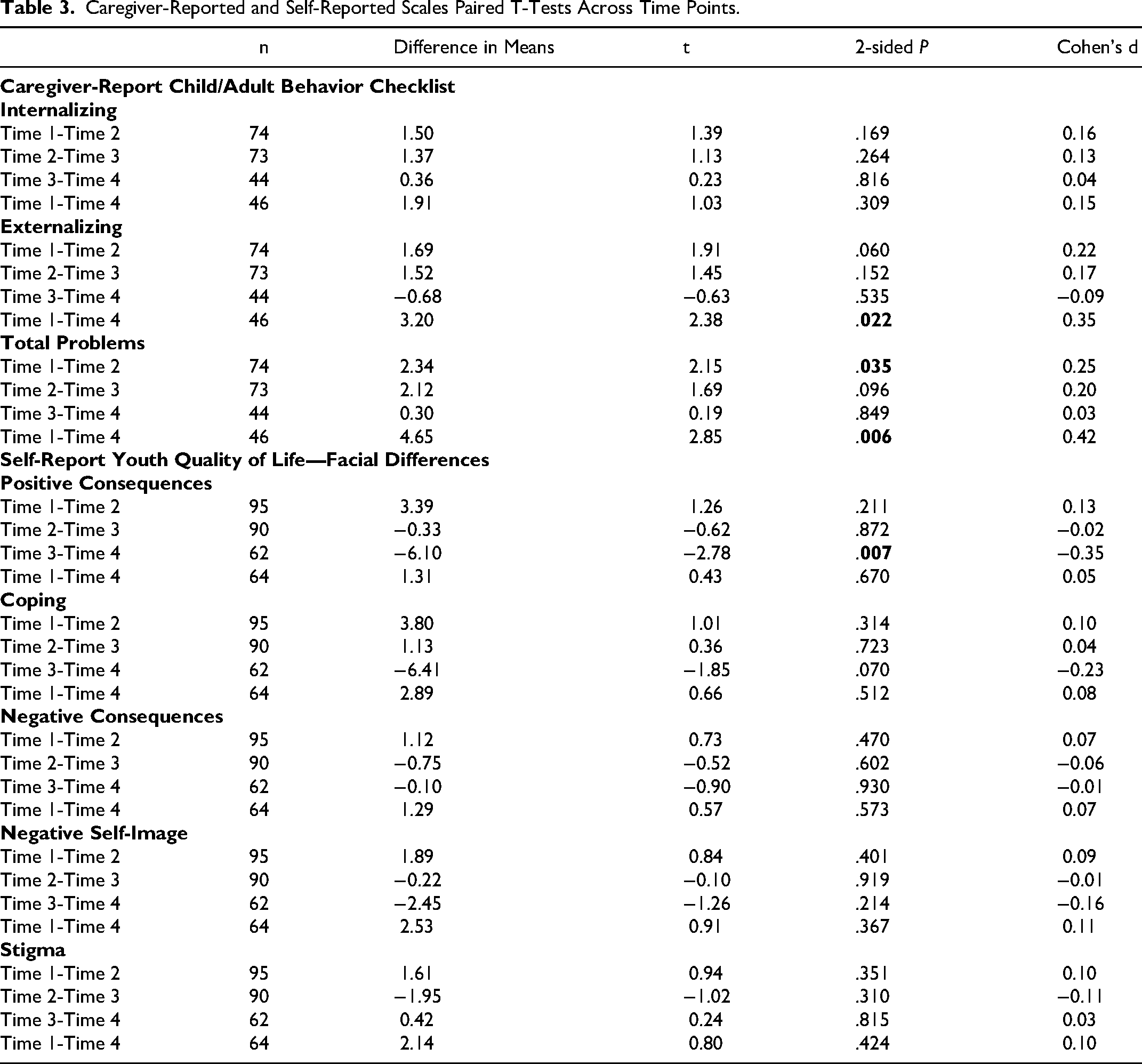
As shown in Table 3, there were a few changes across time. Externalizing and Total Problems significantly decreased by caregiver report from baseline to a year after treatment with a small effect size (d = 0.35 and 0.42, respectively). Total Problems also decreased by caregiver report from Time 1 to Time 2 with a small effect size (d = 0.25). The only significant change based on self-report was an increase in Positive Consequences from finishing treatment at Time 3 to a year later at Time 4 with a small effect size (d = −0.35).
Caregiver-Reported and Self-Reported Scales Paired T-Tests Across Time Points.
Associations Between Caregivers and Self-Reports
Across all time points, there was only one small significant correlation between reports by caregivers and participants. During treatment at Time 2, higher Internalizing was correlated with lower Positive Consequences (r = −0.24, P = .04).
Comparisons Between Types of Treatment and Treatment Outcome
When comparing scores at treatment completion and a year later, there were no differences based on the success of the treatment outcome, and there was only one difference based on the type of treatment, as shown in Supplemental Table 2. At treatment completion, participants who had surgery reported significantly higher Positive Consequences than those who underwent protraction with a medium effect size (eta2 = 0.06). However, this difference was not seen between treatment groups a year after treatment.
Discussion
This longitudinal study found low levels of behavioral concerns reported by caregivers and positive QoL related to having a facial difference from the perspective of individuals with CLP during 2 common interventions for class III malocclusion. As with more recent studies using the C/ABCL scales, this sample had significantly lower behavioral problems than norms with generally large effect sizes.25,26 QoL was high in comparison to the YQOL-FD self-rated “mild” measure norms based on significantly lower negative scales with medium to large effect sizes and few differences for the positive scales. 35 Other studies using the same QoL measure had broadly similar negative scales to this sample; however, the present group of participants had higher positive scales.27,30 Positive adjustment was also seen for this sample using a generic QoL measure and general population measure norms. 39 In the context of ongoing variability related to methodology and setting, these results are consistent with trends of minimal self-reported psychosocial differences compared to peers and growing reports internationally of high health-related QoL that collectively may indicate individuals with a cleft develop resiliency.16,40–49
In this study, neither the type of treatment nor the treatment outcome impacted behavioral ratings or QoL, which might indicate benefits not captured by GOSLON score classifications, as well as positive perceptions formed by participating in any treatment. 50 The one exception was the greater positive consequences at the time of surgery rather than the more gradual shift in the protraction group. The similarity of psychosocial outcomes between treatment options is helpful for providers to be able to include as part of informed consent and shared decision making with patients and their families when planning intervention for class III malocclusion.
Longitudinal data collection identified improvements seen by caregivers for decreased externalizing and total problems from baseline to a year post-treatment, which may reflect maturation with age in addition to possible treatment benefits. Based on self-report, participants had higher Positive Consequences from treatment completion to a year later. This could be due to greater maturity in how they interpret their cleft-related experiences, as well as the benefit of a year passing without having to cope with active treatment.
Although there were few concerns overall, 10% to 17% of the sample were in the clinical range for internalizing problems and negative self-image, which may be areas to target during universal screening for concerns. Positive behavioral functioning and QoL can be promoted as part of interdisciplinary team care across providers. 51 There was only one association across time points between patients and their caregivers, reinforcing the importance of including both a range of measures and ensuring patients report on their own wellbeing. 52 During treatment at the time of maximal correction, caregivers’ higher ratings of internalizing coincided with lower patient perceptions of positive consequences related to having a cleft. This may reflect a period of relatively greater risk for concerns during class III malocclusion treatment when active engagement with patients would be helpful.53,54 For those individuals who would benefit from greater support, current psychosocial interventions for youth with CLP include Young Persons’ Face IT, building on cognitive behavioral strategies, a model for visible differences within Acceptance and Commitment Therapy, using a trauma-informed focus for care, and peer support groups.55–59
This study addressed gaps in prior research by use of a longitudinal design with both caregiver and self-report during 2 intervention models commonly part of cleft care. However, there were several limitations. As the interventions were determined by age and feasibility, randomization to treatment group was not possible, and there may be variations not captured in the analyses due to the age differences of the treatment groups. 60 Results may not generalize to individuals with a maxillary mandibular cant, as this was an exclusion criterion. While the sample was adequately powered for self-report Time 1 through Time 3 and for caregivers at Time 1 (N = 90 estimated by statistical power of 80% with medium effect size of d = 0.60), decreased sample size at Time 4 for self-report and over time for caregivers may not have had adequate power to identify differences. Proportionally, the only difference in the sample longitudinally was fewer individuals with BCLP at Time 3, which may have impacted negative scores at that time point, as BCLP was associated with lower QoL in this sample. 61 Concordance between caregivers and their children was impacted by differences in measures completed. The benefit of adding to the literature data from an underrepresented, predominantly low SES Latino sample with a large Spanish-speaking group of caregivers is countered by the possibility that there may be cultural-, language-, and SES-related risk and protective factors that do not generalize to other groups.62–64 Finally, both study sites provided comprehensive interdisciplinary team care following the American Cleft Palate Craniofacial Association Parameters for Care that may not be representative of treatment provided in lower-resourced settings. 2
In conclusion, individuals with CLP and their caregivers reported low behavioral concerns with high QoL throughout and after treatment for class III malocclusion without impact of the treatment type or outcome. This sample builds on a growing pattern of positive adjustment reported for youth born with CLP overall with targeted support suggested for a minority of patients experiencing internalizing concerns and negative self-image.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261457188 - Supplemental material for Positive Longitudinal Caregiver Behavioral Ratings and Self-Reported Quality of Life in Youth With Cleft Lip and Palate in Treatment for Class III Malocclusion
Supplemental material, sj-docx-1-cpc-10.1177_10556656261457188 for Positive Longitudinal Caregiver Behavioral Ratings and Self-Reported Quality of Life in Youth With Cleft Lip and Palate in Treatment for Class III Malocclusion by Alexis L. Johns, Julia Zukin, Leia Yen, Amarjit Dass, Barbara Sheller, Hitesh P. Kapadia and Stephen L-K. Yen in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656261457188 - Supplemental material for Positive Longitudinal Caregiver Behavioral Ratings and Self-Reported Quality of Life in Youth With Cleft Lip and Palate in Treatment for Class III Malocclusion
Supplemental material, sj-docx-2-cpc-10.1177_10556656261457188 for Positive Longitudinal Caregiver Behavioral Ratings and Self-Reported Quality of Life in Youth With Cleft Lip and Palate in Treatment for Class III Malocclusion by Alexis L. Johns, Julia Zukin, Leia Yen, Amarjit Dass, Barbara Sheller, Hitesh P. Kapadia and Stephen L-K. Yen in The Cleft Palate Craniofacial Journal
Footnotes
Authors’ Note
Portions of this paper were presented at the 82nd Annual American Cleft Palate-Craniofacial Association Meeting, the 15th International Congress on Cleft Lip/Palate and Related Anomalies, and the 2025 Society of Pediatric Psychology Annual Conference.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Dental and Craniofacial Research (NIDCR) U01 DE022937-01A1 (Protocol #14-045-E).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.