
Abstract
Objective
To analyze publication trends and descriptive patterns in PubMed-indexed literature on craniofacial cleft reconstruction from 2000 to 2025.
Design
Bibliometric analysis.
Setting
PubMed database.
Patients/Participants
Fifty-seven records were screened by title and abstract, and 41 articles met the eligibility criteria.
Interventions
None.
Main Outcome Measure(s)
Annual publication trend and distribution of journals, study types, reconstructive themes, and follow-up patterns.
Results
The included literature was limited in volume and unevenly distributed across the study period. The earliest included article was published in 2003, and the highest annual output was observed in 2014 with 5 publications. Most studies were case reports, case series, or single-center retrospective experiences. Journal of Craniofacial Surgery was the most frequent publication venue, followed by Cleft Palate-Craniofacial Journal and Journal of Cranio-Maxillofacial Surgery. Recurrent themes included Tessier cleft subtypes, orbital and eyelid reconstruction, nasal and alar reconstruction, midfacial correction, and staged long-term management.
Conclusions
PubMed-indexed literature on craniofacial cleft reconstruction from 2000 to 2025 was limited and heterogeneous and was dominated by descriptive surgical reporting. The field remains driven largely by institution-specific experience, highlighting the need for standardized outcome reporting and longer structured follow-up.
Introduction
Cleft lip and palate are among the most common congenital anomalies affecting the orofacial region and require coordinated multidisciplinary care across surgical and allied specialties. 1 Craniofacial clefts represent a rarer and more complex group of deformities, and their classification and anatomic interpretation have been strongly shaped by Tessier-based concepts and neuroembryologic understanding. 2
Bibliometric analysis is a useful method for evaluating the structure and evolution of a scientific field. Recent methodological papers have described practical workflows for performing bibliometric studies using database-derived records and dedicated software platforms such as Biblioshiny, Bibliometrix, and VOSviewer.3,4
Within cleft and related maxillofacial literature, bibliometric studies have already been used to examine influential publications, regional publication trends, and research development over time.5-7 These studies show that bibliometric methods can identify patterns in authorship, institutional productivity, citation impact, and thematic focus.
At the same time, reconstructive care in cleft and craniofacial surgery spans multiple domains, including alveolar cleft grafting, multidisciplinary management, and Tessier craniofacial cleft reconstruction.8-10 Despite this breadth, the literature specifically related to craniofacial cleft reconstruction has not been synthesized bibliometrically in a focused manner.
The present study was therefore designed to perform a bibliometric analysis of the literature on craniofacial cleft reconstruction published from 2000 to 2025. The objectives were to evaluate publication trends over time and describe the distribution of journals, study types, reconstructive themes, anatomic focus, and reported follow-up patterns within this field.3,4
Methods
Study Design
This study was designed as a bibliometric analysis of published literature on craniofacial cleft reconstruction. Bibliometric methods were selected because they permit quantitative evaluation of publication output and descriptive patterns within a defined literature set.3,4
Data Source
The bibliographic dataset for this study was obtained from PubMed. PubMed was selected as the data source because it provides structured bibliographic records for biomedical literature and has been used in published bibliometric workflows employing Biblioshiny and VOSviewer. 3
Search Strategy
The PubMed database was searched for articles published between January 1, 2000, and December 31, 2025. The final search strategy used was as follows: (('Tessier cleft’ [Title/Abstract] OR ‘Tessier clefts’ [Title/Abstract] OR ‘craniofacial cleft’ [Title/Abstract] OR ‘craniofacial clefts’ [Title/Abstract]) AND (reconstruction [Title/Abstract] OR reconstructive [Title/Abstract] OR repair [Title/Abstract] OR surgical [Title/Abstract] OR management [Title/Abstract])) NOT (‘cleft lip’ [Title/Abstract] OR ‘cleft palate’ [Title/Abstract] OR ‘cleft lip and palate’ [Title/Abstract] OR syndrome [Title/Abstract] OR syndromic [Title/Abstract] OR embryology [Title/Abstract] OR genetic [Title/Abstract] OR genetics [Title/Abstract] OR tooth [Title/Abstract] OR dental [Title/Abstract] OR pregnancy [Title/Abstract] OR encephalocele [Title/Abstract]). Filters were applied for English language, human studies, and the 2000 to 2025 publication period. This search yielded 57 records for screening.
Eligibility Criteria
Publications were considered eligible if they addressed craniofacial clefts or Tessier clefts and focused on reconstruction, surgical repair, or clinical management. Articles were excluded if they dealt primarily with cleft lip, cleft palate, cleft lip and palate, syndromic conditions, embryology, genetics, dental or tooth-related topics, pregnancy-related topics, or encephalocele, in keeping with the predefined PubMed exclusion terms. Only English-language human studies published between 2000 and 2025 were included.
Study Selection
The retrieved records were screened by title and abstract for relevance to the study objective. Articles that met the predefined eligibility criteria were included in the bibliometric dataset, whereas records that were clearly outside the scope of craniofacial cleft reconstruction were excluded. After title and abstract screening, 41 articles were included in the final bibliometric dataset.
Data Extraction and Bibliometric Analysis
Bibliographic information was extracted from the included PubMed records for descriptive bibliometric evaluation. The analysis examined publication output and the distribution of journals, study types, reconstructive themes, and follow-up patterns within the dataset. Methodological guidance for bibliometric analysis and the use of Biblioshiny/Bibliometrix and VOSviewer was drawn from published bibliometric workflow papers.3,4 Extracted clinical and methodological characteristics were tabulated descriptively, including study design, level of evidence, cleft/fissure type, anatomic focus, treatment approach, staging, follow-up reporting, and outcome domains (Figures 1 and 2).
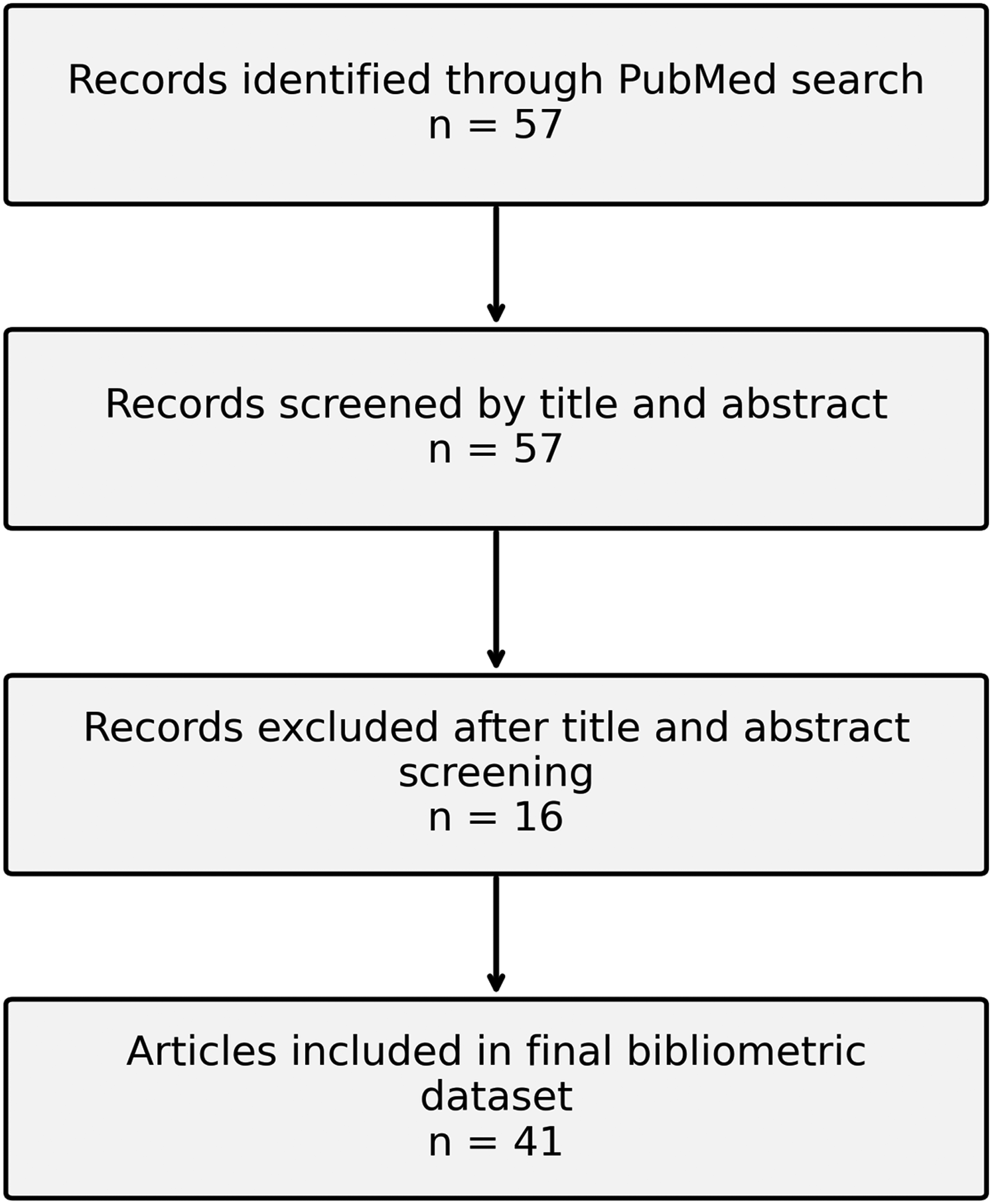
Study selection flow diagram. Flow diagram showing identification and screening of PubMed records for inclusion in the bibliometric dataset. Fifty-seven records were screened by title and abstract, 16 were excluded, and 41 articles were included in the final analysis.
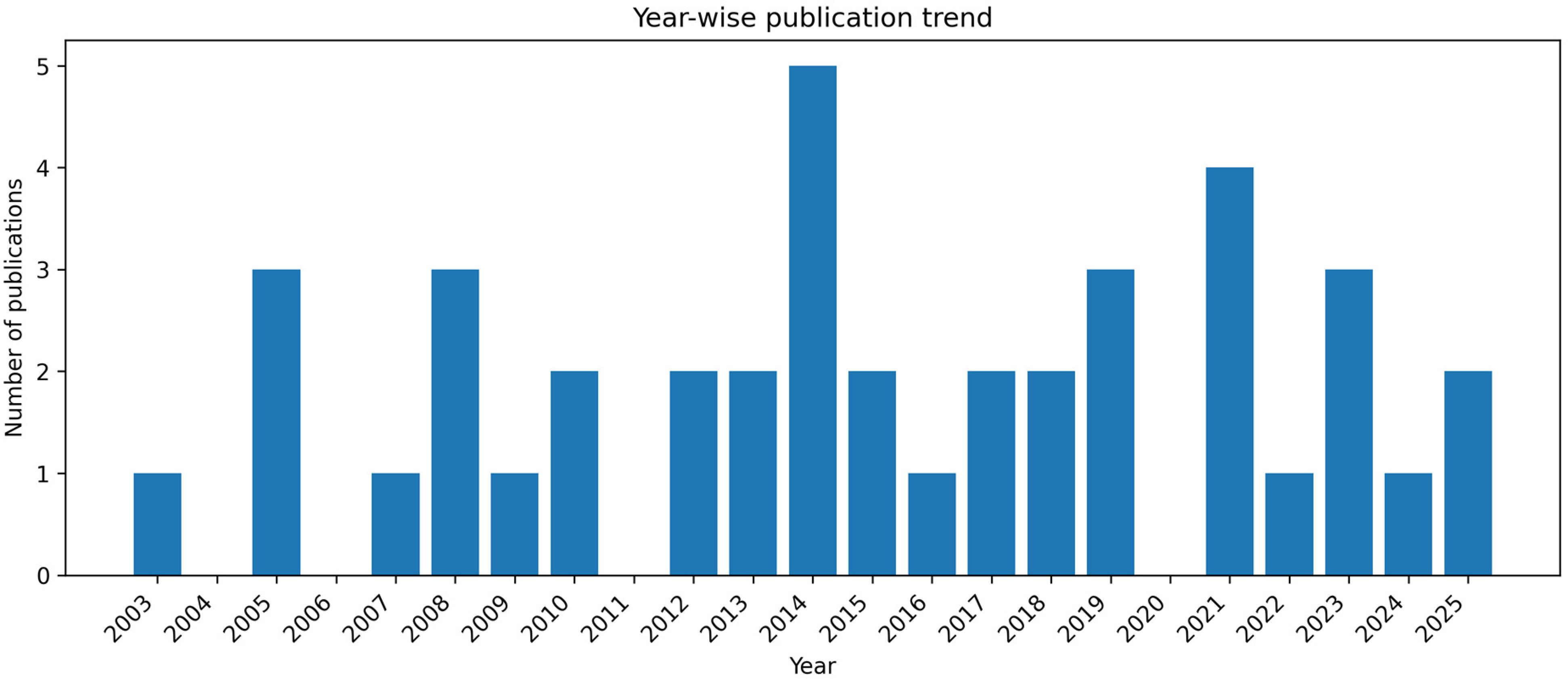
Year-wise publication trend. Annual distribution of included publications on craniofacial cleft reconstruction from 2003 to 2025.
Outcome Measures
The primary outcome measures were the annual publication trend and the distribution of publications across journals. Secondary outcome measures included study types, reconstructive themes, anatomic focus, and patterns of reported follow-up.
Results
The PubMed search yielded 57 records after application of the predefined search strategy and filters. Title and abstract screening resulted in 41 articles being included in the final bibliometric dataset.
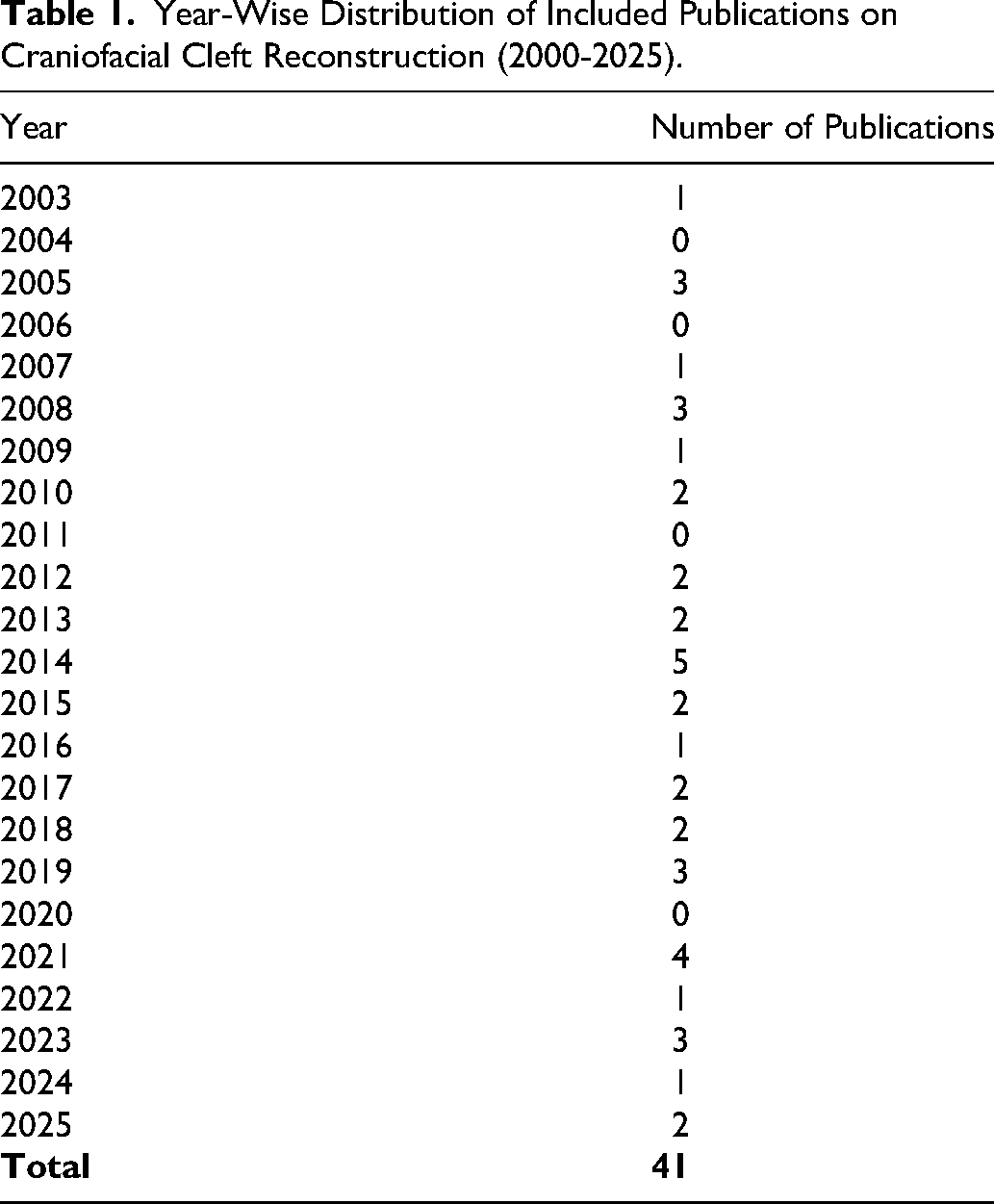
Eligible publications were distributed unevenly across the study period. The earliest included article was published in 2003, and the highest annual output was observed in 2014 with 5 publications. Smaller peaks were seen in 2005, 2008, 2019, and 2023 with 3 publications each.
The included literature was dominated by descriptive clinical reports, particularly case reports, case series, and single-center surgical experiences, whereas larger cohort analyses were uncommon.
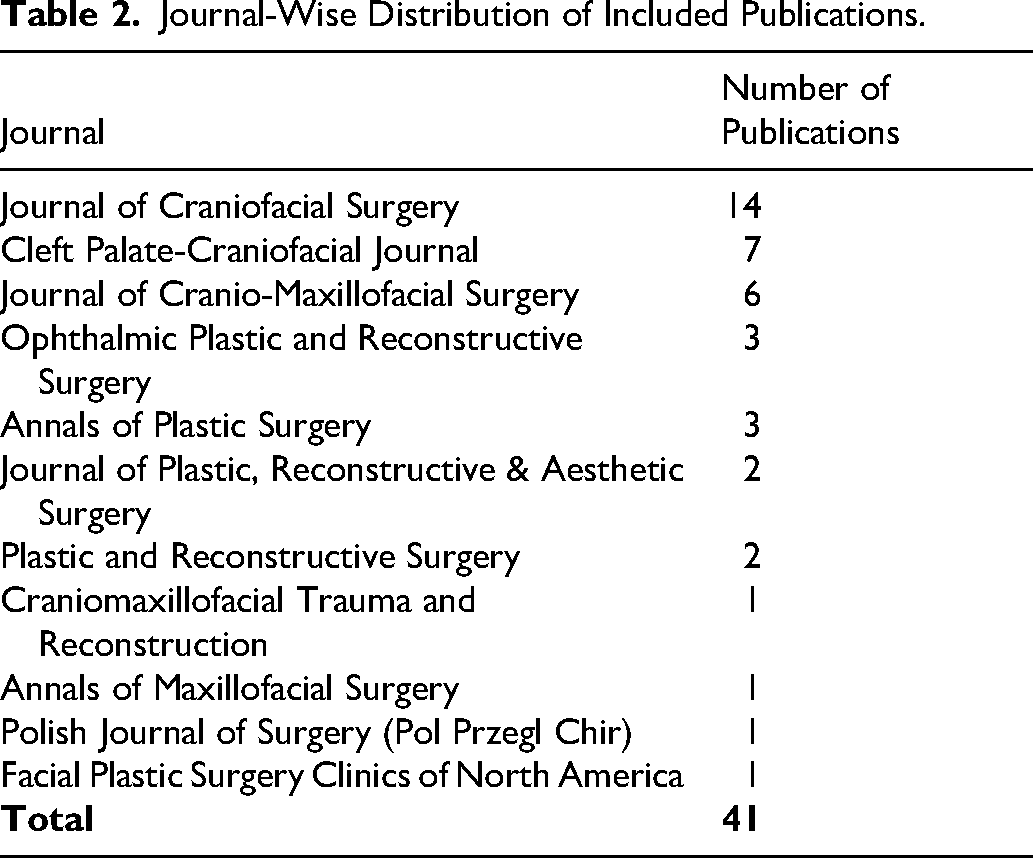
The publications were dispersed across several specialty journals, with a clear concentration in craniofacial, plastic surgery, and cleft-focused journals. Journal of Craniofacial Surgery was the most frequent publication venue with 14 articles, followed by Cleft Palate-Craniofacial Journal with 7 and Journal of Cranio-Maxillofacial Surgery with 6. Ophthalmic Plastic and Reconstructive Surgery and Annals of Plastic Surgery each contributed 3 articles (Tables 1 and 2).
Year-Wise Distribution of Included Publications on Craniofacial Cleft Reconstruction (2000-2025).
Journal-Wise Distribution of Included Publications.
Anatomically, the included studies addressed a broad range of craniofacial cleft presentations, with repeated attention to Tessier no. 3 and no. 4 clefts, midline clefts, nasal clefts, orbital and eyelid involvement, and lateral facial clefts or macrostomia. Reconstructive themes included local and regional flap-based repair, facial unit repositioning, nasal and alar reconstruction, eyebrow and eyelid reconstruction, bone grafting, distraction-assisted treatment, and staged protocol-based correction. The extracted clinical and methodological characteristics of the included publications are summarized in Table 3.
Extracted Clinical and Methodological Characteristics of Included Craniofacial Cleft Reconstruction Publications.
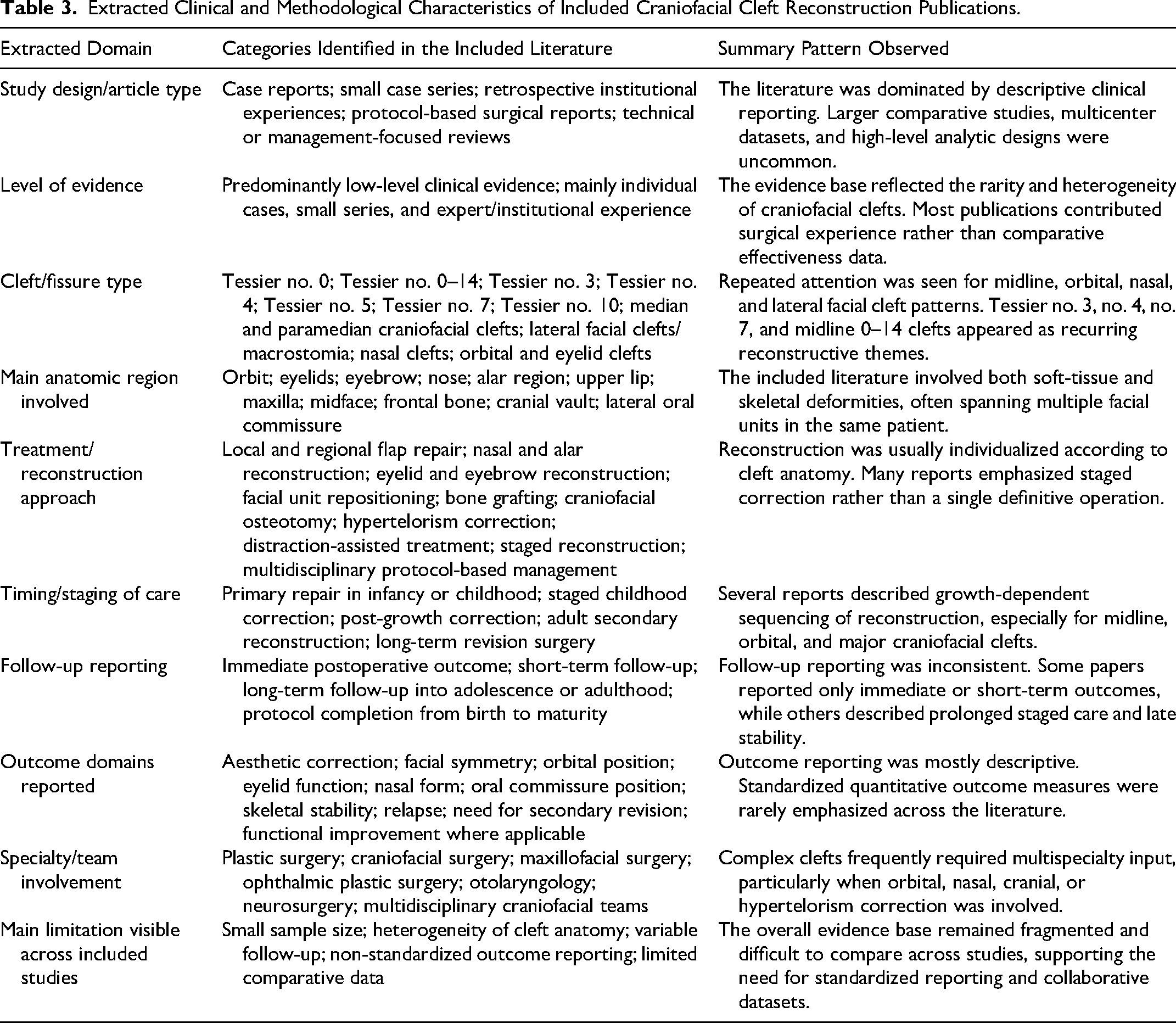
Follow-up reporting was variable across the included studies. Some publications described only immediate reconstructive outcomes, whereas others reported staged management across childhood or long-term follow-up extending into adolescence or adulthood.
Overall, the bibliometric dataset demonstrated that the published literature on craniofacial cleft reconstruction from 2000 to 2025 was limited in volume, heterogeneous in anatomic focus, and dominated by descriptive surgical reporting.
Discussion
The present bibliometric analysis identified a relatively small but persistent body of literature on craniofacial cleft reconstruction between 2000 and 2025. The included publications were predominantly descriptive surgical reports, and comparative or higher-level analytic studies were uncommon. This pattern is consistent with the rarity and heterogeneity of craniofacial clefts and also aligns with prior bibliometric observations in cleft-focused and related craniomaxillofacial literature, where research output has been shaped largely by specialized centers, experience-based reporting, and uneven publication volume.5-7
The predominance of descriptive studies in the present dataset is also consistent with the broader evidence structure of cleft and craniofacial surgery. A review of randomized controlled trials has shown that Level I evidence in this field remains limited, with many commonly performed procedures not supported by robust comparative trial data. 11 In rare facial and craniofacial clefts specifically, published experience has often come from institutional series and protocol-based clinical reports rather than large multicenter studies. 12
The clinical breadth of craniofacial cleft reconstruction also helps explain why the literature remains heterogeneous. Reconstructive problems in this field range from alveolar cleft grafting and broader cleft-craniofacial surgical management to the varied anatomic patterns described within Tessier clefts, making uniform comparison across studies inherently difficult.8-10
Rare craniofacial clefts have been described as an underreported group of deformities, and objective long-term evaluation has often been difficult because of their rarity and phenotypic diversity. 13 Bonafos et al. also noted that the published literature in rare craniofacial clefts is sparse and frequently limited to isolated cases or very small series. 14 In a retrospective series of 32 Tessier no. 0 clefts, da Silva Freitas et al. likewise noted a paucity of publications on this malformation and observed that the available literature was largely confined to clinical examination and surgical treatment in small numbers of patients. 15 In an 11-patient series, Fijałkowska and Antoszewski described treatment as multispecialist, multistage, and highly individualized. 16 Monasterio and Taylor similarly argued that standard techniques are difficult to propose for major craniofacial clefts because of the many possible combinations of skeletal and soft-tissue involvement. 17
This need for individualized planning is evident in papers that propose cleft-specific treatment protocols. Woods et al. described an age-based management protocol for Tessier no. 7 clefts, separating infancy, childhood, and post-growth interventions. 18 Golinko et al. reported a four-step primary surgical approach for Tessier no. 3 clefts and anticipated later lip, nose, eyelid, maxillary, orbital, and alveolar revisions. 19 Balaji also emphasized that rare facial Tessier clefts often require more than one operation and do not lend themselves easily to a single universal treatment algorithm. 20
Long-term follow-up is especially important because reconstructive adequacy cannot be judged from the immediate postoperative appearance alone. Toriyama et al. reported stable long-term reconstruction over 7 years in a Tessier no. 10 craniofacial cleft treated with folded vascularized calvarial bone. 21 Afifi et al. described more than a decade of additional reconstruction in an adult with a Tessier no. 5 facial cleft who had already undergone numerous prior procedures. 22 In the protocol series of midline Tessier 0–14 clefts, Pidgeon et al. followed patients from birth to maturity and highlighted the importance of growth-dependent sequencing of correction. 13
Periorbital and midline deformities add another layer of complexity to craniofacial cleft reconstruction. Rüegg et al. managed median and paramedian craniofacial clefts using procedures such as box osteotomy, facial bipartition, canthopexy, and nasal reconstruction according to the underlying deformity pattern. 23 Pittet et al. reported that simultaneous correction of Tessier 0–14 deformity with major hypertelorism, frontal bone defect, and nasal aplasia required repeated operations and neurosurgical participation. 24 Golinko et al. likewise used a coordinated approach involving plastic surgery, otolaryngology, and oculoplastic surgery for Tessier no. 3 repair. 19
Even when skeletal correction is achieved, durability over time remains a concern. In a long-term follow-up study of hypertelorbitism correction, Wan et al. found greater relapse when correction was performed at a younger age. 25 This point is relevant when interpreting reconstructive stability in craniofacial cleft patients who undergo orbital and midfacial correction during growth.
Against this clinical background, the pattern seen in the present bibliometric dataset becomes easier to understand. A field characterized by rarity, marked anatomic variability, multistage treatment, and prolonged follow-up is more likely to generate case reports, case series, protocol papers, and single-center experiences than large comparative trials. The extracted-characteristics summary further demonstrates that the literature is not only numerically limited but also methodologically heterogeneous, with variable reporting of cleft type, reconstructive approach, staging, follow-up, and outcome domains.
Several limitations of the present study should be acknowledged. The dataset was derived from a single database and was restricted to English-language human studies. Study selection was based on title and abstract screening rather than full-text review of every retrieved record. In addition, the search strategy was intentionally focused on Tessier and craniofacial cleft terminology, so relevant studies using different nomenclature may not have been captured.
Despite these limitations, the present analysis provides a focused overview of how the craniofacial cleft reconstruction literature has developed between 2000 and 2025. The available evidence remains limited in volume and is dominated by descriptive surgical reporting, but it also shows sustained effort by specialized centers to refine reconstructive strategies for these rare deformities. Future work would benefit from standardized outcome reporting, longer structured follow-up, and greater collaboration across centers treating craniofacial clefts.
Footnotes
Ethical Approval
Not applicable for this bibliometric analysis of published literature.
Informed Consent
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study were derived from publicly available PubMed records.