
Abstract
Objective
To describe temporal trends in hospital admissions for cleft lip and/or palate (CL/P) repair in Brazil, assess the COVID-19 pandemic impact, examine racial and demographic disparities in length of hospital stay (LOS), and identify regional efficiency patterns.
Design
Retrospective ecological study using nationwide hospital admission data.
Setting
Brazilian Unified Health System (SUS), covering public sector inpatient procedures. Participants: 98,998 hospital admissions for CL/P surgical repair from 2008 to 2024.
Interventions
None (observational analysis of primary/secondary surgical repairs). Main Outcome Measures: Annual admission volumes and trends (annual percent change via Prais–Winsten regression); LOS by race/color (Kruskal–Wallis test); state-level clustering (K-means) based on volume, sex distribution, and mean LOS.
Results
Male predominance (ratio 1.36:1); 70% repairs under age 5. Stable volumes until 33% decline in 2020, with incomplete recovery. Significant racial disparities in LOS (p = .0007), longer among Brown (Parda) and Indigenous children. Heterogeneous state trends; four clusters identified, with São Paulo high-volume/moderate-stay vs. northern low-volume/prolonged-stay.
Conclusions
Brazil has robust CL/P surgical capacity, but racial and profound regional disparities persist, compromising equity and efficiency. Targeted investment in northern regions, decentralized expertise, and standardized protocols are needed to reduce inequities.
Keywords
Introduction
Cleft lip and/or palate (CL/P) constitute the most common congenital craniofacial malformation, with a reported prevalence in Brazil ranging from approximately 0.52 to 1.36 per 1000 live births depending on regional detection rates.1,2 Globally, the incidence is estimated at around 1 in 700 live births, requiring a series of coordinated multidisciplinary interventions throughout childhood and adolescence. 3 Primary surgical repair, cheiloplasty typically between 3 and 6 months and palatoplasty between 9 and 18 months, remains essential for restoring orofacial function, enabling adequate feeding, preventing recurrent otitis media, and facilitating normal speech development.7-9 Delays beyond these optimal windows are associated with increased risks of speech and language impairments, as well as higher rates of middle ear complications.10-12
Although surgical techniques for CL/P repair are well-established and extensively documented, far less attention has been devoted to systemic factors influencing the efficiency and equity of care delivery at a national scale. In a geographically expansive and socioeconomically diverse nation such as Brazil, demographic disparities related to race/color and pronounced regional variations in healthcare infrastructure may substantially affect access to timely intervention, hospital resource utilization, and treatment outcomes. These inequities remain inadequately characterized in comprehensive, long-term nationwide studies.
Brazil is the largest and most populous country in South America, with a population of approximately 215 million according to the 2022 National Census conducted by the Instituto Brasileiro de Geografia e Estatística (IBGE). Racially, the population self-declares as approximately 43% White (Branca), 43% Brown (Parda), 10% Black (Preta), 2.5% Indigenous (Indígena), and 0.5% Asian (Amarela), following the official Brazilian racial self-classification system adopted across all public data collection platforms, including the health system. Socioeconomically, the southern and southeastern regions, encompassing states such as São Paulo, Santa Catarina, and Rio Grande do Sul, concentrate the majority of the country's gross domestic product, specialized healthcare infrastructure, and tertiary referral centers. In stark contrast, the northern and northeastern regions, particularly states within and bordering the Amazon basin such as Amazonas, Pará, Roraima, and Amapá, are characterized by lower Human Development Index scores, sparse healthcare facilities, large indigenous and riverine communities, and significant geographic barriers that impose substantial challenges to access to specialized surgical services. These structural and demographic disparities directly shape the patterns of CL/P care delivery examined in this study.
The present ecological study addresses this knowledge gap by analyzing 18 years of hospital admission data for CL/P surgical repair in Brazil. The objective of this study was to describe temporal trends in hospital admissions for CL/P repair in Brazil, examine the impact of the COVID-19 pandemic across specific timeframes (pre-pandemic: 2008–2019; pandemic: 2020–2021; and recovery: 2022–2024), and identify regional patterns of healthcare utilization. In this context, length of hospital stay (LOS) is employed as a proxy for healthcare journey complexity, reflecting clinical, logistical, and socioeconomic factors that influence surgical care delivery.
Methods
This retrospective nationwide ecological study analyzed hospital admissions for CL/P repair in Brazil over an 18-year period from 2008 to 2024. The data were sourced from the Hospital Information System of the Brazilian Unified Health System (SIH/SUS), a publicly accessible database managed by the Brazilian Ministry of Health through the DATASUS platform. This system captures all inpatient admissions financed by the public health sector, which provides coverage to approximately 80% of the Brazilian population.
Cases were identified by selecting records where the principal diagnosis corresponded to cleft palate, cleft lip, or cleft lip and palate, according to the International Classification of Diseases, 10th Revision codes. The analysis focused on admissions involving primary or secondary surgical repairs, such as cheiloplasty and palatoplasty, as registered in the authorization for hospital admission forms. Only inpatient procedures were included, as the dataset does not encompass outpatient interventions.
Within the SIH/SUS, hospital admissions are registered through the Autorização de Internação Hospitalar (AIH — Hospital Admission Authorization form), which captures not only the primary ICD-10 diagnostic code but also the procedimento (procedure code) corresponding to the specific intervention authorized for reimbursement by the public system. Case identification in this study was based on the intersection of ICD-10 diagnostic codes for CL/P (Q35–Q37) and procedure codes corresponding to primary or secondary surgical repairs, specifically cheiloplasty and palatoplasty, as listed in the SIGTAP (Sistema de Gerenciamento da Tabela de Procedimentos, the national procedure classification system used by SUS). This dual-filter approach substantially reduces the inclusion of non-surgical admissions, such as pre-operative assessments or admissions for feeding difficulties or failure to thrive, as these would be authorized and reimbursed under different procedure categories within the system. While it is not possible to entirely exclude atypical billing practices, the potential for misclassification is expected to be minimal and consistent across states and time periods, and therefore unlikely to systematically bias regional or temporal comparisons.
For each admission, information was extracted regarding the year of occurrence, the federative unit corresponding to one of the 26 states or the Federal District, patient sex categorized as male or female, self-declared race or color classified into White, Black, Brown (Parda), Asian (Yellow), or Indigenous, age grouped into categories of less than 1 year, 1 to 4 years, 5 to 9 years, and 10 to 14 years, and LOS measured in days. Records with missing values in core variables were retained for aggregated analyses, with such missing data accounting for approximately 2.2% of entries related to sex and length of stay.
To ensure clarity for a broad audience, the Prais–Winsten regression was selected to analyze temporal trends because it corrects for autocorrelation, ensuring that year-over-year fluctuations do not bias the long-term trend results. K-means clustering was utilized to group states with similar care profiles (volume and LOS), facilitating the identification of regional service disparities.
Given the ecological nature of this study, hospital admissions were analyzed as an aggregate proxy for the total surgical burden of CL/P in the public system. While the SIH/SUS database utilizes ICD-10 codes that may encompass different primary and secondary procedures (eg, cheiloplasty and palatoplasty) under broader administrative categories, this approach allows for a comprehensive assessment of nationwide healthcare utilization and regional capacity, rather than individual clinical outcomes.
Descriptive statistics were first computed to summarize the total number of admissions and their distribution across sex, race/color, age groups, and federative units. Annual admission counts were aggregated to examine temporal patterns over the study period.
To evaluate temporal trends, a regression model specifically designed for time series data was applied to the annualized admission counts after logarithmic transformation to stabilize variance and linearize trends. This approach allowed estimation of the annual percent change while adjusting for potential autocorrelation in sequential observations. The analysis was conducted both at the national level and individually for each federative unit.
Differences in the LOS according to race/color were assessed using a non-parametric test suitable for comparing multiple independent groups, with follow-up pairwise comparisons performed when the overall test indicated significance. Differences between sexes were evaluated using a non-parametric test for 2 independent samples.
States were grouped into clusters based on patterns of total admissions by sex, mean length of stay, and overall case volume. A partitioning clustering algorithm was employed after standardizing the features to ensure equal weighting, with the optimal number of clusters determined through visual inspection of inertia reduction and silhouette coefficients.
Hospital efficiency was approximated through the mean length of stay and the cumulative inpatient days calculated per admission. States were ranked according to mean length of stay, where shorter durations suggested greater efficiency. Total inpatient days were derived by multiplying admission counts by corresponding mean stays for each state and year.
All statistical procedures were carried out using Python version 3.12 with libraries dedicated to data manipulation, numerical computing, scientific statistics, econometric modeling, and machine learning. A significance level of 0.05 was adopted for hypothesis testing.
Since the study relied exclusively on anonymized and aggregated data available in the public domain, no individual informed consent was necessary. The research adhered to Brazilian regulatory guidelines for studies involving secondary public health data.
Results
Over the 18-year study period, a total of 98,998 hospital admissions for CL/P repair were recorded within the Brazilian Unified Health System. Of these, 57,114 involved male patients and 41,884 female patients, yielding a male-to-female ratio of 1.36:1. Repairs were predominantly performed in early childhood, with 29,165 admissions (29.5%) occurring in infants under 1 year of age and 39,643 (40.0%) in children aged 1–4 years, accounting for nearly 70% of all procedures in children younger than 5 years.
A marked reduction was observed in 2020 (Figure 1), with only 7978 admissions recorded, a 33% decrease compared with the previous year, followed by a gradual but incomplete recovery, reaching 11,926 in 2023 and 11,714 in 2024. The stacked bar component of Figure 1 illustrates the consistent dominance of procedures in younger age groups throughout the period, while the overlaid line and moving average highlight the sharp pandemic-related disruption and subsequent partial rebound.
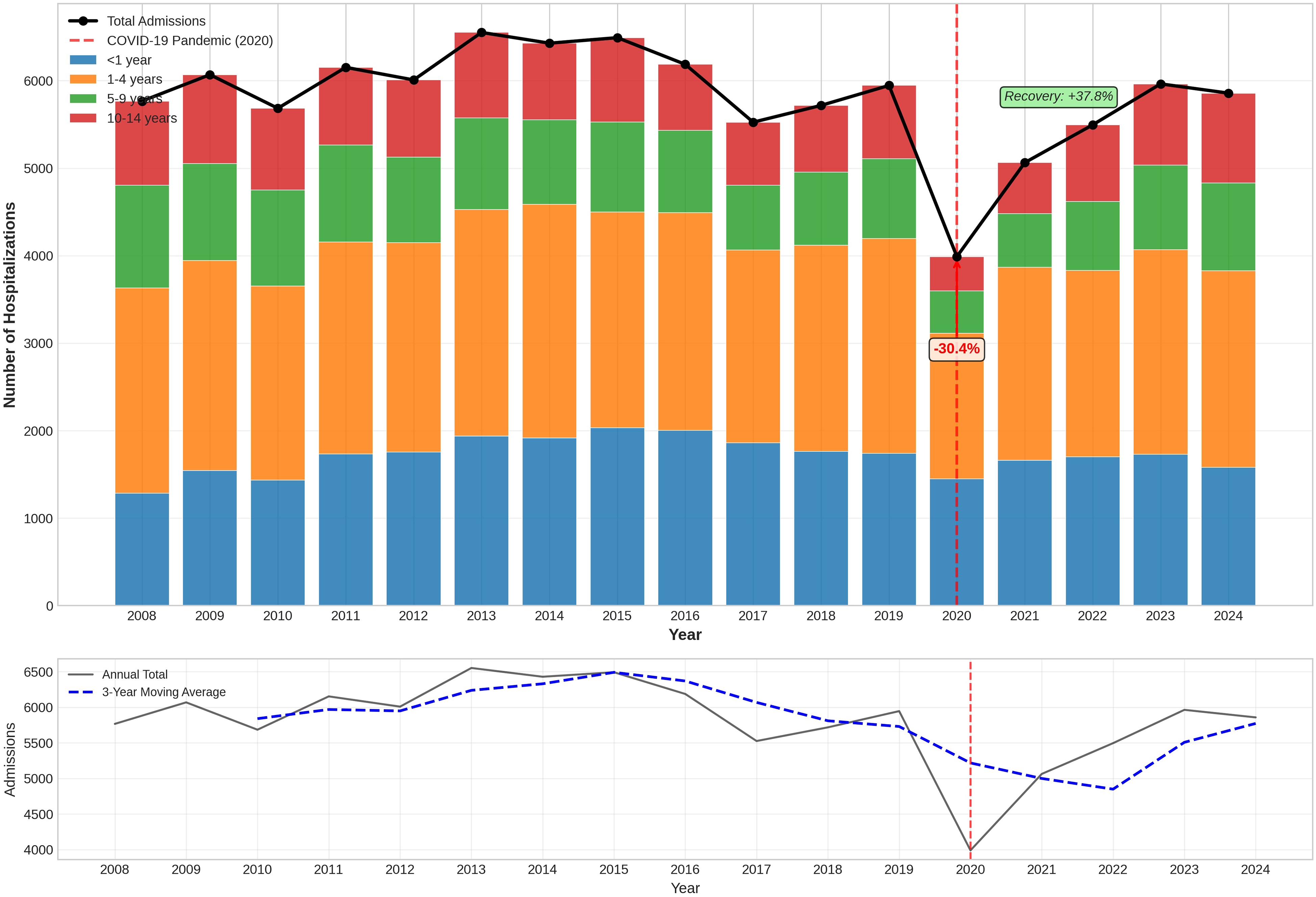
Temporal trends in hospital admissions for cleft lip and/or palate repair in Brazil, 2008–2024. The line graph shows annual admission volumes with a 3-year moving average; the stacked bar chart illustrates distribution by age group (<1 year, 1–4 years, 5–9 years, 10–14 years). A sharp decline is evident in 2020, reflecting the impact of the COVID-19 pandemic, followed by partial recovery.
State-level analysis of temporal trends using annual percent change revealed considerable heterogeneity (Table 1 and Figure 2). Significant increases were noted in several northern and central-western states, including Rondônia (+21.5%) and Amazonas (+16.2%), whereas significant declines occurred in Santa Catarina (−10.2%) and São Paulo (−3.3%). Figure 2 further contextualizes these trends by plotting APC against model fit (R2), demonstrating stronger linear trends in states with the most pronounced changes.
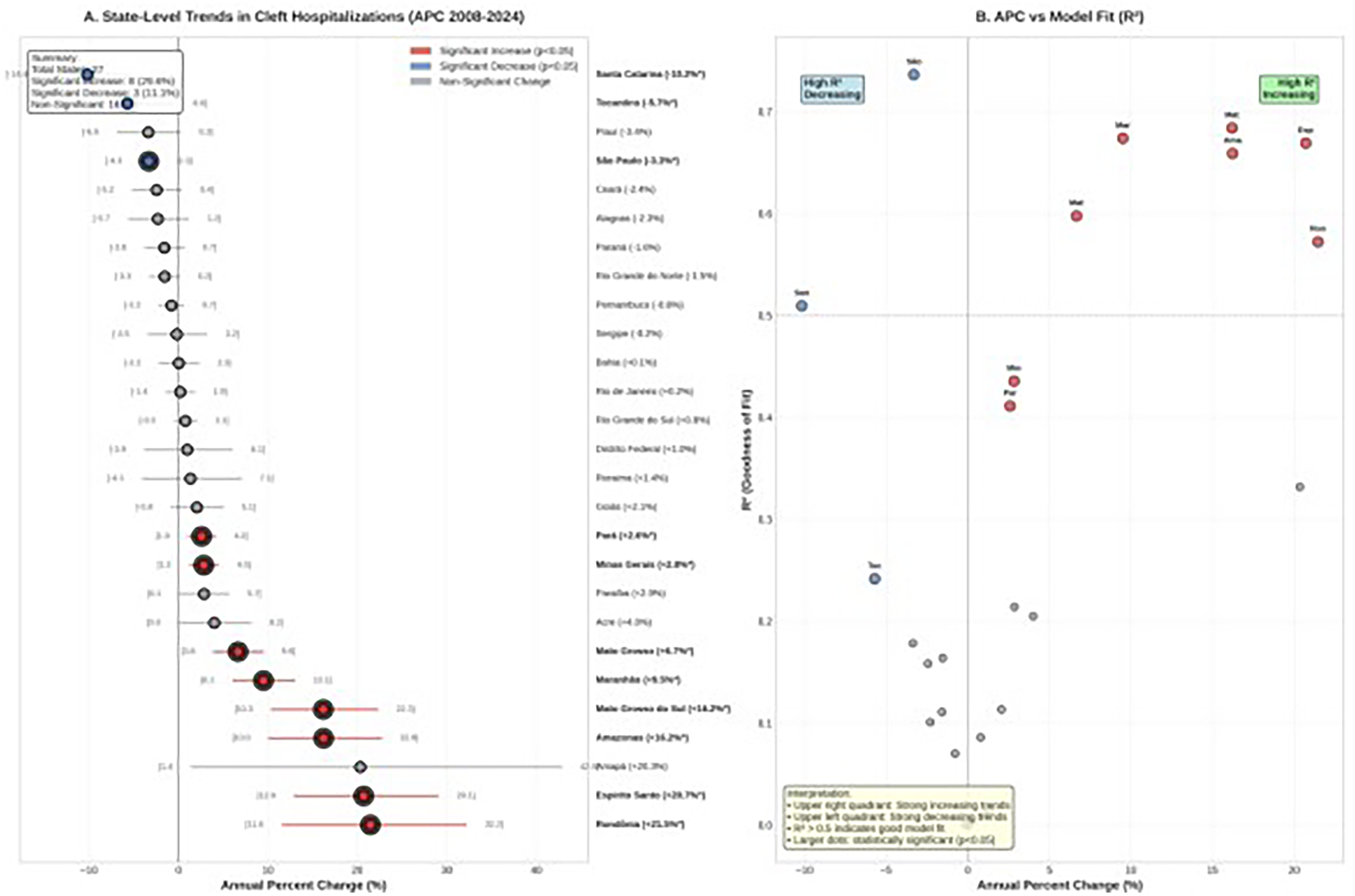
State-level annual percent change (APC) in hospital admissions for cleft lip and/or palate repair in Brazil, 2008–2024. Each point represents one Brazilian state or the Federal District, plotted by APC (x-axis) against model fit (R2, y-axis). Points above the horizontal line indicate statistically significant trends (p < .05); northern states show increasing trends, while southern states show declines.
APC in Hospital Admissions for Cleft Lip and/or Palate Repair by Brazilian State, 2008–2024.
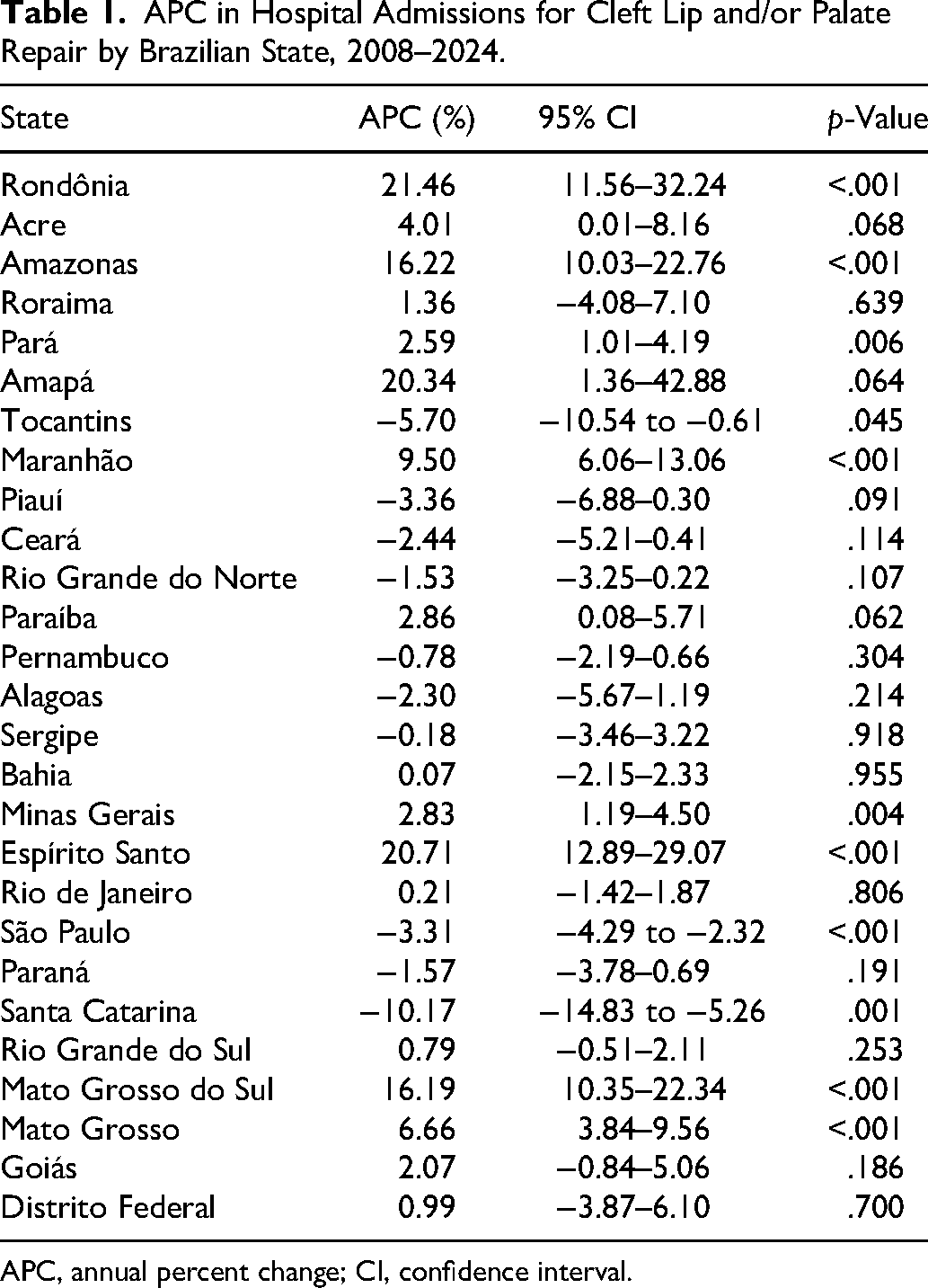
APC, annual percent change; CI, confidence interval.
LOS varied significantly across self-declared racial/color groups (Kruskal–Wallis test, p = .0007). White patients represented the largest absolute volume of cases, whereas Brown (Parda) and Indigenous children showed higher median stays and greater variability (Table 2).
Length of Hospital Stay (Days) by Self-Declared Race/Color.
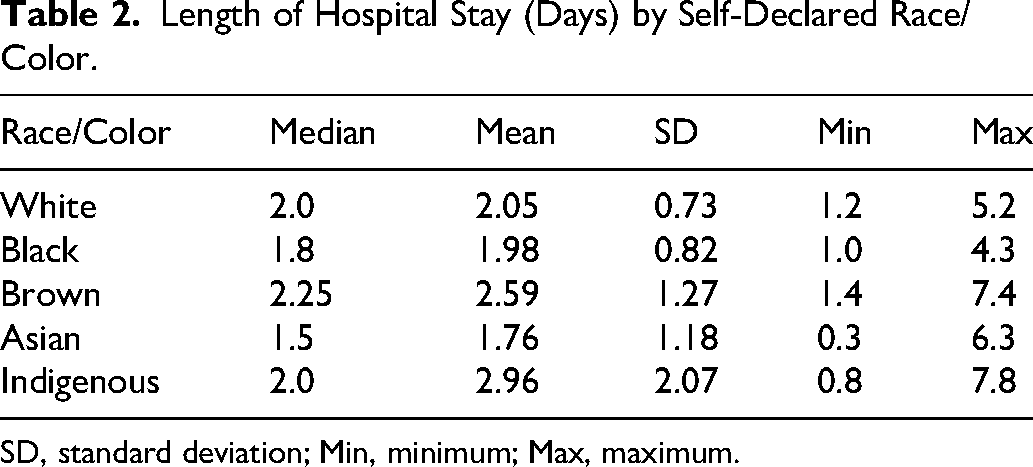
SD, standard deviation; Min, minimum; Max, maximum.
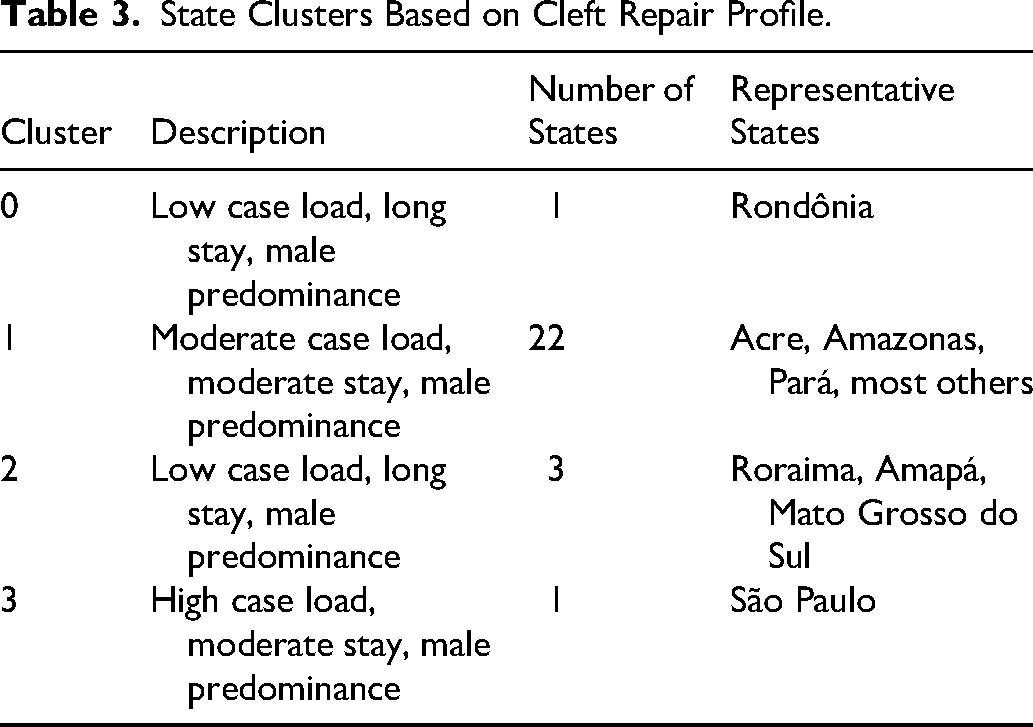
K-means clustering identified four distinct state profiles based on total case volume, sex distribution, and mean length of stay (Table 3 and Figure 3). São Paulo formed a unique cluster characterized by exceptionally high volume and moderate stay duration, while northern and certain isolated states clustered together with low volumes and prolonged stays. The geographic distribution of these clusters is illustrated in Figure 3, which presents a choropleth map of Brazil with states color-coded by cluster designation.
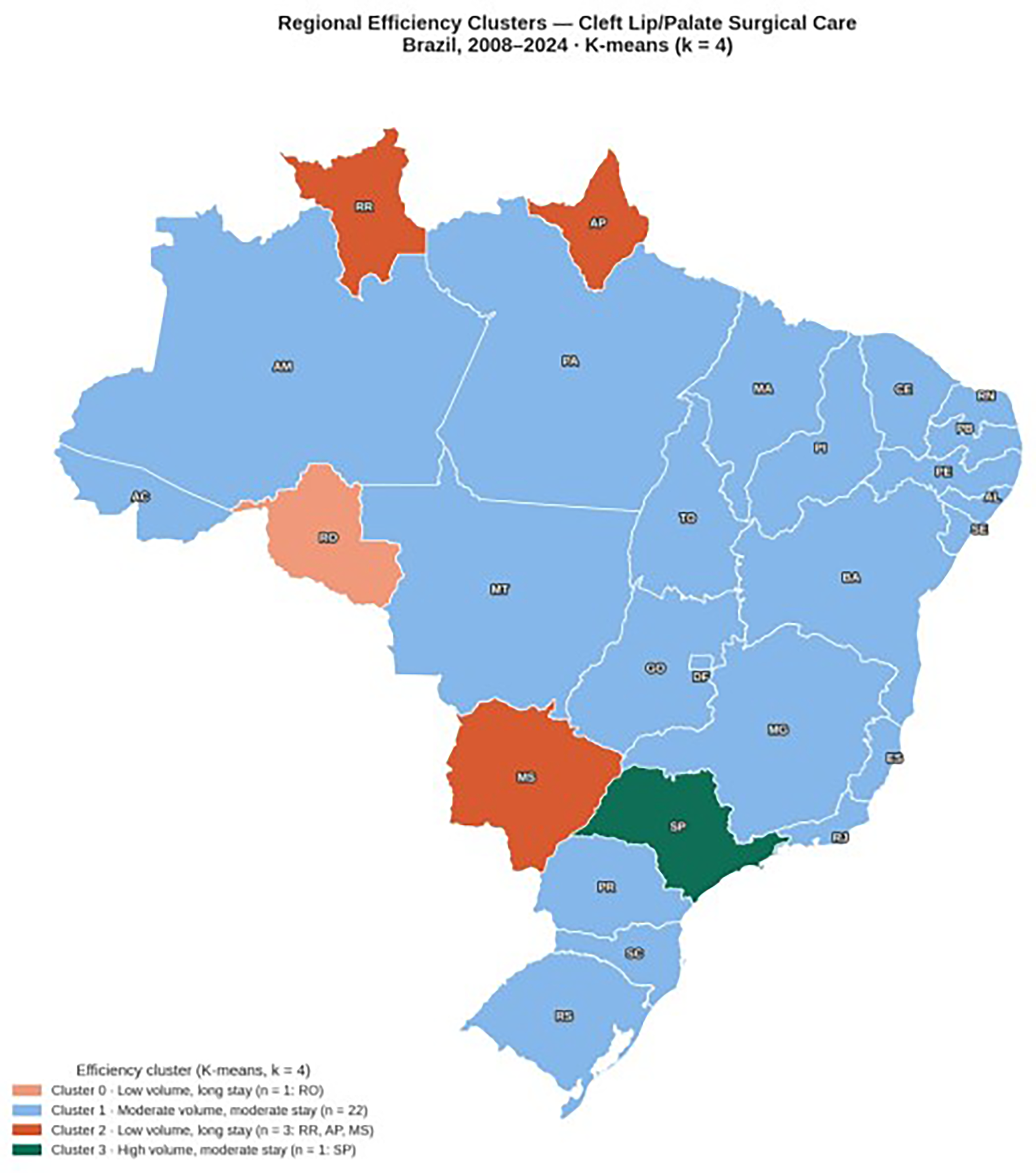
Choropleth map of Brazil illustrating the geographic distribution of regional efficiency clusters identified by K-means analysis (k = 4). States are color-coded by cluster designation: Cluster 0 (low volume, long stay; n = 1: Rondônia); Cluster 1 (moderate volume, moderate stay; n = 22); Cluster 2 (low volume, long stay; n = 3: Roraima, Amapá, Mato Grosso do Sul); Cluster 3 (high volume, moderate stay; n = 1: São Paulo). State abbreviations are labeled within each territory.
State Clusters Based on Cleft Repair Profile.
Discussion
This nationwide analysis underscores both the achievements and enduring challenges of surgical care for cleft lip and palate within Brazil's public health system. The observed male predominance aligns with established global patterns, reflecting inherent epidemiological differences across cleft subtypes.3-6 The concentration of repairs in early childhood indicates reasonable adherence to evidence-based timing recommendations, which is critical for minimizing long-term speech and auditory complications.7-12
Temporal stability in annual volumes was disrupted by a sharp decline in 2020, consistent with documented reductions of over 50% in pediatric elective surgery during pandemic peaks, followed by prolonged recovery periods.13,14 Such delays likely contributed to backlog effects, potentially exacerbating functional deficits in affected cohorts.
Racial disparities in LOS were statistically significant, with Brown (Parda) and Indigenous children experiencing longer and more variable durations.15-17 These findings mirror international evidence of delayed or differential care among non-White populations, including lower repair rates and higher complication risks.18-20 The marked under-representation of Black patients further suggests potential gaps in case ascertainment or access, influenced by socioeconomic and geographic barriers.16,17,19
The observed racial disparities in LOS, particularly among Brown (Parda) and Indigenous children, must be interpreted with caution to avoid bias. These findings likely do not stem from biological differences, but rather from structural inequities. Families from these demographic groups often face greater geographic distances from specialized centers, leading to what is termed “social admission”, where hospital stay is prolonged not due to surgical complications, but to ensure patient safety before a long journey back to remote areas with limited local healthcare support. These structural factors are compounded by the regional inequalities documented in this study: states in the North and Northeast, which have lower HDI scores, fewer specialized centers, and larger proportions of Brown and Indigenous populations, consistently show longer stays and lower procedural volumes.
Regional variation proved most pronounced, with São Paulo forming a distinct high-volume, efficient cluster attributable to specialized reference centers exemplified by institutions such as HRAC-USP (“Centrinho”) that leverage economies of scale, standardized protocols, and multidisciplinary expertise to achieve shorter stays.16,17 Conversely, northern states clustered with low volumes and extended hospitalizations, likely reflecting limited local capacity, reliance on distant referrals, and logistical challenges such as family transportation, phenomena akin to “social admission” described in disparity studies.16,17,19
These patterns highlight that, despite substantial national progress facilitated by the SUS, structural inequities continue to impede uniform efficiency and timeliness. High-performing southern and southeastern models offer replicable frameworks, while northern and northeastern regions require targeted strategies to mitigate barriers.
This study is subject to the inherent limitations of ecological designs using secondary administrative data. The reliance on hospital admission forms means that individual-level clinical details, such as specific cleft subtypes or pre-existing comorbidities, were not available for analysis. Furthermore, the system may record repeated admissions for the same patient across different years as separate entries, which reflects total procedural volume but limits our ability to track individual surgical outcomes or complications. Additionally, the geographic scope and procedural heterogeneity inherent to large administrative databases represent constraints that should be considered when interpreting state-level comparisons.
Conclusion
This 18-year nationwide analysis of hospital admissions for CL/P repair in Brazil demonstrates that the Unified Health System has established a robust framework for delivering essential surgical care to affected children, with nearly 99,000 procedures performed over the study period and a substantial proportion occurring in early childhood. The findings confirm expected demographic patterns, including male predominance and concentration of primary repairs in the first years of life, while revealing relative temporal stability interrupted by the profound impact of the COVID-19 pandemic.
However, the results also expose persistent and profound inequities. Significant racial disparities in LOS, coupled with the under-representation of Black patients, point to barriers that disproportionately affect marginalized populations. Even more striking are the regional inequalities, where high-volume reference centers in the South and Southeast achieve markedly shorter stays through economies of scale and specialized expertise, while northern and isolated states endure prolonged hospitalizations that likely reflect both clinical and social challenges.
These disparities underscore that, despite national progress, access to efficient and timely surgical care remains uneven across Brazil's vast geography and diverse population. To address this, policy efforts should focus on decentralizing models of excellence, such as those observed in São Paulo and Santa Catarina, to the North and Northeast through targeted investment in regional reference centers, surgical training programs, and logistical support for families in remote areas.
Ultimately, achieving equitable outcomes for children with CL/P requires a comprehensive, multidisciplinary approach. While the collaboration between pediatric dentistry and surgery is foundational, global standards emphasize the need for integrated teams including speech therapy, audiology, psychology, and otolaryngology to manage the long-term functional results. Policy efforts should focus on decentralizing excellence from southern hubs to the North and Northeast, utilizing standardized protocols to reduce the social and hospital burden identified in this 18-year analysis.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The aggregated dataset and analysis code supporting the conclusions of this article are available upon request. Individual-level data are not publicly available because they belong to the Brazilian Ministry of Health and are subject to data-use agreements.